


Application of Deep Learning Techniques for Detection of Pneumothorax in Chest Radiographs

Abstract
:1. Introduction
- Various pneumothorax models are also augmented with multiple techniques that are available for download [8].
- A comparison between different parameters of a model.
- A comparison of various implementations of models.
- Metrics (high accuracy, low false positives) that are applicable to the medical imaging sector.
- The potential for transfer learning to other diseases.
2. Related Works
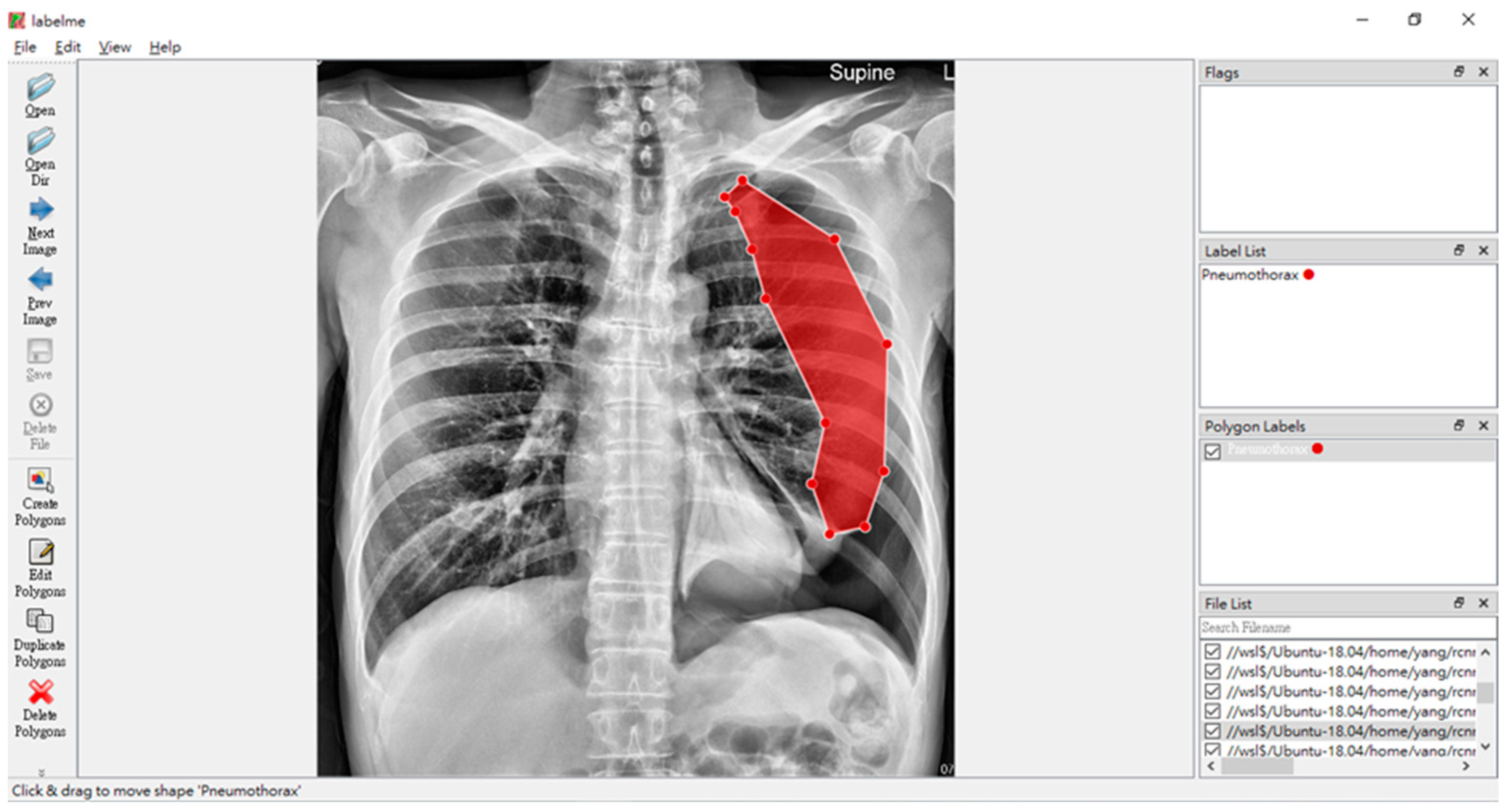
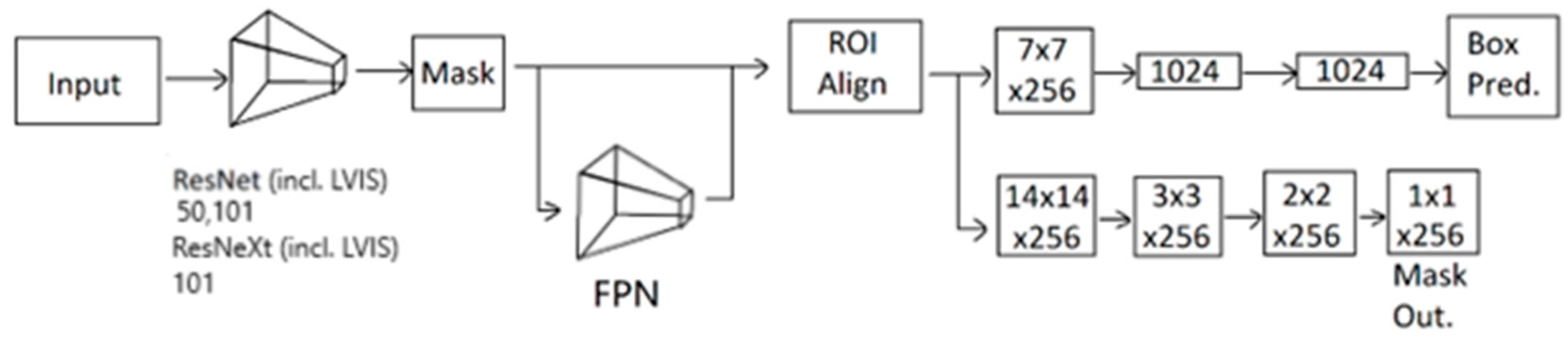
3. Methodology
- Rotation is set to be randomly shifted by 5 degrees.
- Brightness is set to be randomly tuned in a 20% range on the original luminosity of the image.
- Contrast is set to be randomly tuned in a 20% range of the original image.
- Saturation is set to be randomly tuned in a 20% range of the original image.
4. Results
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Noppen, M.; Keukeleire, T. De Pneumothorax. Respiration 2008, 76, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Bintcliffe, O.; Maskell, N. Spontaneous Pneumothorax. BMJ 2014, 348, g2928. [Google Scholar] [CrossRef] [PubMed]
- Novák, K.; Vodicka, J.; Novotný, V. The Importance and Urgency of Pneumothorax. Rozhl. Chir. 1992, 71, 254–263. [Google Scholar] [PubMed]
- Baumann, M.H.; Strange, C.; Heffner, J.E.; Light, R.; Kirby, T.J.; Klein, J.; Luketich, J.D.; Panacek, E.A.; Sahn, S.A. Management of Spontaneous Pneumothorax. Chest 2001, 119, 590–602. [Google Scholar] [CrossRef] [PubMed]
- MacDuff, A.; Arnold, A.; Harvey, J. Management of Spontaneous Pneumothorax: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010, 65, ii18–ii31. [Google Scholar] [CrossRef] [PubMed]
- Kirienko, M.; Sollini, M.; Silvestri, G.; Mognetti, S.; Voulaz, E.; Antunovic, L.; Rossi, A.; Antiga, L.; Chiti, A. Convolutional Neural Networks Promising in Lung Cancer T-Parameter Assessment on Baseline FDG-PET/CT. Contrast Media Amp Mol. Imaging 2018, 2018, 1382309. [Google Scholar] [CrossRef] [PubMed]
- Velez-Cubian, F.O.; Rodriguez, K.L.; Thau, M.R.; Moodie, C.C.; Garrett, J.R.; Fontaine, J.P.; Toloza, E.M. Efficacy of Lymph Node Dissection during Robotic-Assisted Lobectomy for Non-Small Cell Lung Cancer: Retrospective Review of 159 Consecutive Cases. J. Thorac. Dis. 2016, 8, 2454. [Google Scholar] [CrossRef] [PubMed]
- Xiang-Yann, L. Release Model Xiangyann/Pneumothorax Model. 2023. Available online: https://github.com/xiangyann/PneumothoraxModel2023/releases/latest (accessed on 16 August 2023).
- He, K.; Gkioxari, G.; Dollar, P.; Girshick, R. Mask R-CNN. In Proceedings of the IEEE International Conference on Computer Vision (ICCV), Venice, Italy, 22–29 October 2017. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 26 June–1 July 2016; IEEE: Piscataway, NJ, USA, 2016. [Google Scholar]
- Ishfaq, M.; Shah, S.Z.A.; Ahmad, I.; Rahman, Z. Multinomial Classification of NLRP3 Inhibitory Compounds Based on Large Scale Machine Learning Approaches. Mol Divers 2023. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Diggans, J.; Pankratz, D.; Huang, J.; Pagan, M.; Sindy, N.; Tom, E.; Anderson, J.; Choi, Y.; Lynch, D.; et al. Classification of Usual Interstitial Pneumonia in Patients with Interstitial Lung Disease: Assessment of a Machine Learning Approach Using High-Dimensional Transcriptional Data. Lancet Respir. Med. 2015, 3, 473–482. [Google Scholar] [CrossRef]
- Ramalho, G.; Rebouças Filho, P.; Medeiros, F.; Cortez, P. Lung Disease Detection Using Feature Extraction and Extreme Learning Machine. Rev. Bras. Eng. Biomédica 2014, 30, 207–214. [Google Scholar] [CrossRef]
- Poreva, A.; Karplyuk, Y.; Vaityshyn, V. Machine Learning Techniques Application for Lung Diseases Diagnosis. In Proceedings of the 2017 5th IEEE Workshop on Advances in Information, Electronic and Electrical Engineering (AIEEE), Riga, Latvia, 24–25 November 2017; pp. 1–5. [Google Scholar]
- Wild, C.P.; Weiderpass, E.; Stewart, B.W. World Cancer Report. The International Agency for Research on Cancer (IARC): Lyon, France, 2020; Volume 454. [Google Scholar]
- SEER Brain and Other Nervous System Cancer—Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/brain.html (accessed on 7 May 2023).
- Sharma, K.; Kaur, A.; Gujral, S. Brain Tumor Detection Based on Machine Learning Algorithms. Int. J. Comput. Appl. 2014, 103, 7–11. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Raza, M.; Saba, T.; Anjum, M.A. Brain Tumor Detection Using Statistical and Machine Learning Method. Comput. Methods Programs Biomed. 2019, 177, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Hemanth, G.; Janardhan, M.; Sujihelen, L. Design and Implementing Brain Tumor Detection Using Machine Learning Approach. In Proceedings of the 2019 3rd International Conference on Trends in Electronics and Informatics (ICOEI), Tirunelveli, India, 23–25 April 2019; IEEE: Piscataway, NJ, USA; pp. 1289–1294. [Google Scholar]
- Aamir, M.; Rahman, Z.; Abro, W.A.; Bhatti, U.A.; Dayo, Z.A.; Ishfaq, M. Brain Tumor Classification Utilizing Deep Features Derived from High-Quality Regions in MRI Images. Biomed. Signal Process. Control 2023, 85, 104988. [Google Scholar] [CrossRef]
- Girshick, R.; Donahue, J.; Darrell, T.; Malik, J. Rich Feature Hierarchies for Accurate Object Detection and Semantic Segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Columbus, OH, USA, 23–28 June 2014. [Google Scholar]
- Girshick, R. Fast R-CNN. In Proceedings of the IEEE International Conference on Computer Vision (ICCV), Santiago, Chile, 7–13 December 2015. [Google Scholar]
- Ren, S.; He, K.; Girshick, R.; Sun, J. Faster R-CNN: Towards Real-Time Object Detection with Region Proposal Networks. In Proceedings of the Advances in Neural Information Processing Systems, Montreal, QC, Canada, 7–12 December 2015; Cortes, C., Lawrence, N., Lee, D., Sugiyama, M., Garnett, R., Eds.; Curran Associates, Inc.: Newyork, NY, USA, 2015; Volume 28. [Google Scholar]
- Russell, B.; Torralba, A.; Murphy, K.; Freeman, W. LabelMe: A Database and Web-Based Tool for Image Annotation. Int. J. Comput. Vis. 2008, 77, 157–173. [Google Scholar] [CrossRef]
- Wu, Y.; Kirillov, A.; Massa, F.; Lo, W.-Y.; Girshick, R. Detectron2. Available online: https://github.com/facebookresearch/detectron2 (accessed on 16 March 2023).
- Xie, S.; Girshick, R.; Dollár, P.; Tu, Z.; He, K. Aggregated Residual Transformations for Deep Neural Networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017. [Google Scholar]
- Lin, T.-Y.; Dollar, P.; Girshick, R.; He, K.; Hariharan, B.; Belongie, S. Feature Pyramid Networks for Object Detection. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 936–944. [Google Scholar]
- Lin, T.-Y.; Maire, M.; Belongie, S.; Hays, J.; Perona, P.; Ramanan, D.; Dollár, P.; Zitnick, C.L. Microsoft COCO: Common Objects in Context. In Proceedings of the Computer Vision–ECCV 2014: 13th European Conference, Zurich, Switzerland, 6–12 September 2014; pp. 740–755. [Google Scholar]
- Gupta, A.; Dollár, P.; Girshick, R. LVIS: A Dataset for Large Vocabulary Instance Segmentation. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Long Beach, CA, USA, 15–20 June 2019. [Google Scholar]
- Facebook AI Research Detectron2/MODEL_ZOO.Md at Main Facebookresearch/Detectron2. Available online: https://github.com/facebookresearch/detectron2/blob/main/MODEL_ZOO.md (accessed on 13 August 2023).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Configuration Candidate | Iterations | Learning Rate | Weight Decay | Decay Steps | False Positive (%) | False Negative (%) | Accuracy (%) | AP (%) | AP50 (%) | AP75 (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| 22-0710 | 37,500 | 0.1 | 0.005 | 1 k, 2 k, 5 k, 10 k, 15 k, 20 k, 30 k | 3.16 | 9.41 | 87.43 | 48.15 | 81.89 | 46.17 |
| 23-1518 | 500,00 | 0.1 | 0.005 | 1 k, 2 k, 5 k, 10 k, 15 k, 20 k, 30 k | 3.11 | 11.24 | 85.65 | 47.55 | 81.06 | 45.98 |
| 23-2251 | 50,000 | 0.1 | 0.005 | 500, 10 k, 20 k, 30 k, 35 k, 40 k, 45 k | 2.97 | 11.68 | 85.35 | 43.25 | 78.90 | 43.05 |
| 24-1814 | 50,000 | 0.01 | 0.005 | 5 k, 10 k, 15 k, 20 k, 25 k, 30 k, 35 k, 40 k, 45 k | 3.29 | 16.18 | 80.53 | 43.67 | 78.71 | 41.99 |
| 26-1501 | 100,000 | 0.001 | 0.0001 | 25 k, 40 k, 50 k, 60 k, 70 k, 80 k, 85 k, 90 k, 95 k | 1.09 | 3.68 | 95.23 | 46.82 | 76.61 | 50.46 |
| Transfer Learning Model | False Positive (%) | False Negative (%) | Accuracy (%) | AP (%) | AP50 (%) | AP75 (%) |
|---|---|---|---|---|---|---|
| ResNet50 (COCO) | 1.33 | 4.38 | 94.29 | 48.76 | 80.34 | 53.35 |
| ResNet101 (COCO) | 1.09 | 3.68 | 95.23 | 46.82 | 76.61 | 50.46 |
| ResNeXt101 (COCO) | 0.88 | 3.44 | 95.68 | 44.61 | 78.95 | 49.20 |
| ResNet50 (LVIS) | 1.47 | 5.91 | 92.62 | 49.26 | 84.20 | 53.45 |
| ResNet101 (LVIS) | 1.12 | 4.99 | 93.89 | 51.57 | 79.46 | 61.40 |
| ResNeXt101 (LVIS) | 1.05 | 3.40 | 95.55 | 49.50 | 82.20 | 50.79 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deng, L.Y.; Lim, X.-Y.; Luo, T.-Y.; Lee, M.-H.; Lin, T.-C. Application of Deep Learning Techniques for Detection of Pneumothorax in Chest Radiographs. Sensors 2023, 23, 7369. https://doi.org/10.3390/s23177369
Deng LY, Lim X-Y, Luo T-Y, Lee M-H, Lin T-C. Application of Deep Learning Techniques for Detection of Pneumothorax in Chest Radiographs. Sensors. 2023; 23(17):7369. https://doi.org/10.3390/s23177369
Chicago/Turabian StyleDeng, Lawrence Y., Xiang-Yann Lim, Tang-Yun Luo, Ming-Hsun Lee, and Tzu-Ching Lin. 2023. "Application of Deep Learning Techniques for Detection of Pneumothorax in Chest Radiographs" Sensors 23, no. 17: 7369. https://doi.org/10.3390/s23177369