
Fall Recognition Based on an IMU Wearable Device and Fall Verification through a Smart Speaker and the IoT
 ,
,
Abstract
:1. Introduction
- (1)
- We develop a chest-worn wearable device with the integrated operation of an IMU sensor and a precision barometric altimeter.
- (2)
- Based on the chest-worn device, we can determine the direction of the fall, such as falling forward, falling backward, falling to the left, or falling to the right.
- (3)
- We also can determine the intensity of a fall generated from the various behavior states such as standing, sitting, and walking.
- (4)
- With the aid of smart speakers and the IoT, false alarms can be reduced by directly asking the fallen person for further confirmation.
- (5)
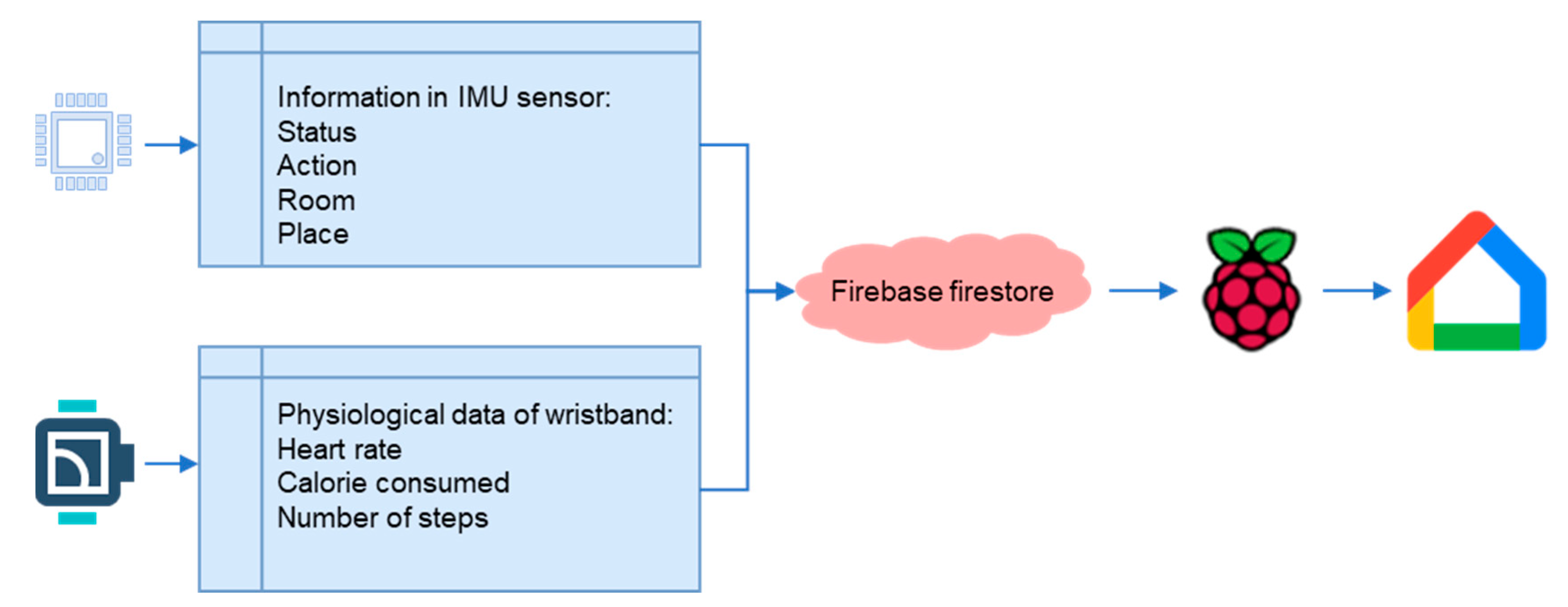
- We provide a smart wristband for sharing important physiological information to the chest-worn device and cloud every second to know if the health condition gets worse after a fall event.
2. Related Work
3. Development Environment and Method
3.1. Development Environment of Falling Recognition
3.2. Development Environment of Falling Verification
- (1)
- bNode modules:
- (2)
- Smart wristband:
- (3)
- Chest-worn IMU sensors:
- (4)
- Raspberry Pi:
- (5)
- Google Home nest mini:

3.3. Active Push Broadcast
3.4. Methods
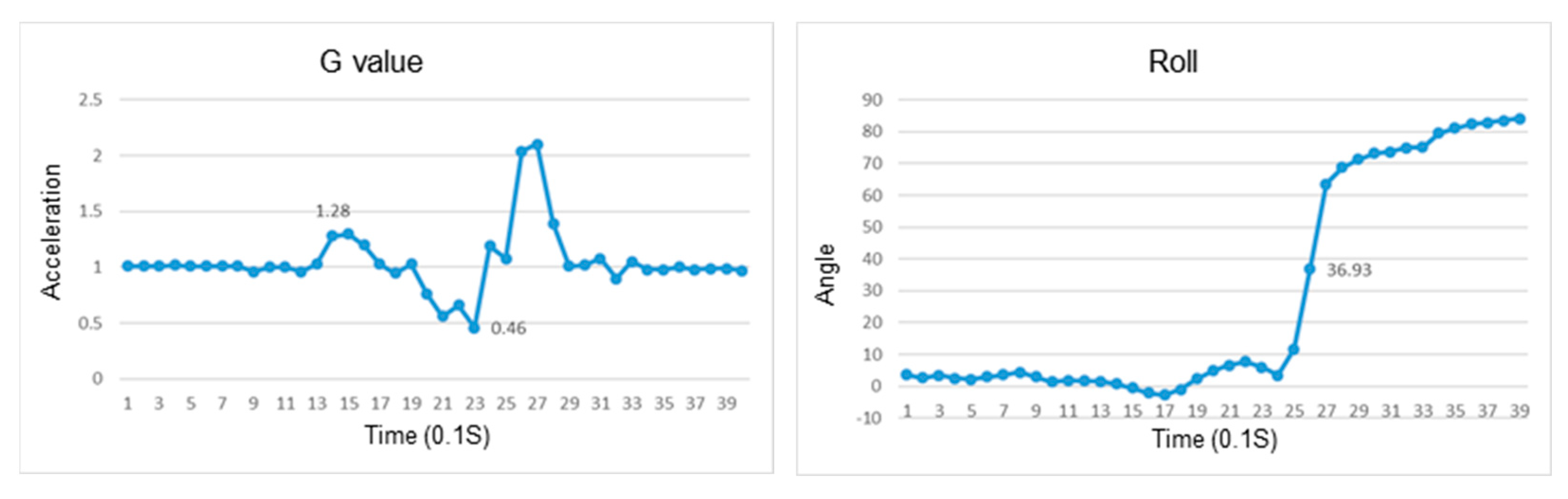
3.5. The Principle of Fall Detection
3.6. Experimental Method
3.7. Experiment Procedure
- (A)
- Falling backward:
- (B) Falling forward:
- (C) Falling leftward and rightward:


4. The Experiment of Recognition of Falls for Various Postures
4.1. Recognition of Falls
4.2. Recognition of a Fall While Sitting
4.3. Recognition of a Fall While Standing
4.4. Recognition of a Fall While Standing Up
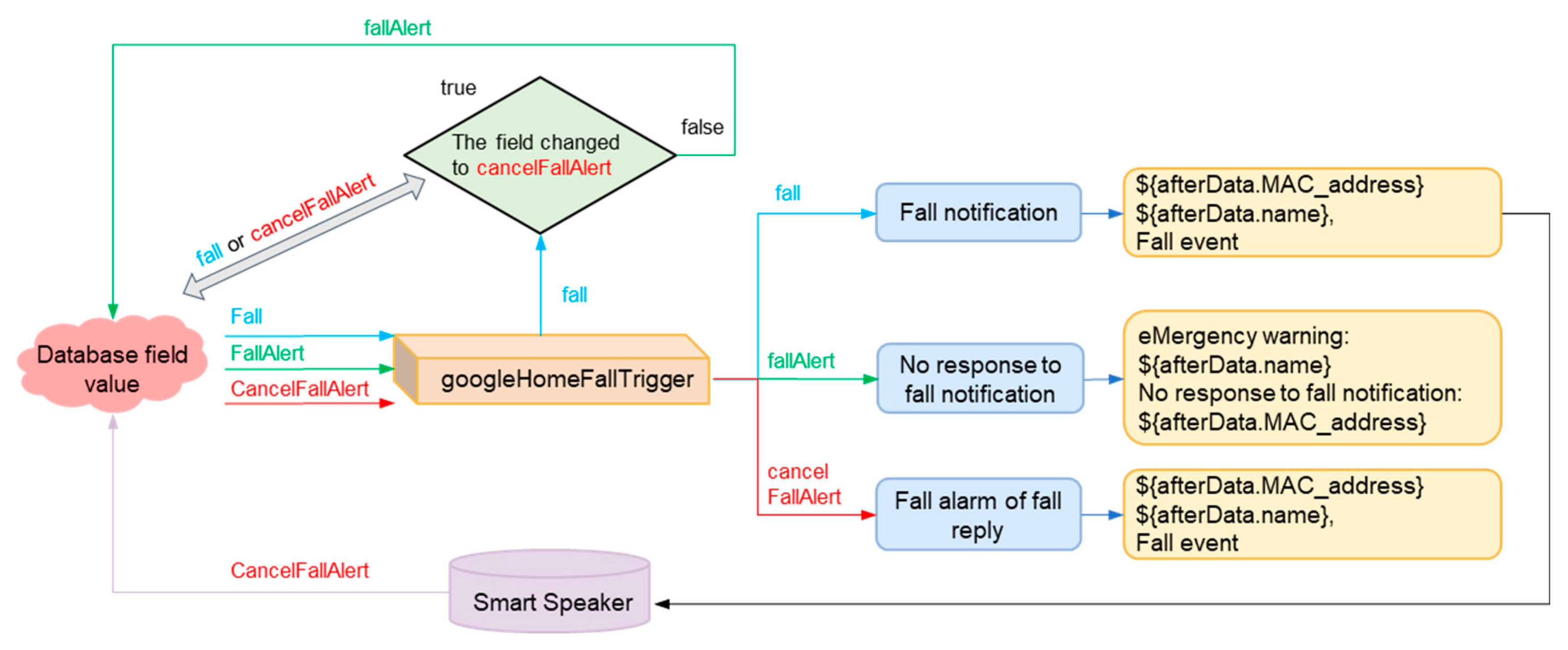
4.5. Falling Verification
5. Discussion
- (1)
- In order to ensure accurate fall detection, the wearable device is attached to the user’s skin near the sternum of the chest with the adhesive. Medical adhesives are widely used in the medical field. Although the adhesive of the device is a medical type, it is still possible to be allergic to the materials in these adhesives. Thus, it is necessary to select a suitable adhesive individually.
- (2)
- The wearable device uses a 150 mAH lithium-ion rechargeable battery, which needs to be charged every day. In order to ensure fall detection is performed 24 h a day, it is necessary to provide two chest-worn wearable devices, which can be used alternatively while the battery is charging.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Step Safely: Strategies for Preventing and Managing Falls Across the Life-Course; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Vieira, E.R.; Palmer, R.C.; Chaves, P.H. Prevention of falls in older people living in the community. BMJ 2016, 353, i1419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dionyssiotis, Y.; Dontas, I.A.; Economopoulos, D.; Lyritis, G.P. Rehabilitation after falls and fractures. J. Musculoskelet. Neuronal Interact. 2008, 8, 244–250. [Google Scholar] [PubMed]
- Schacht, E.; Richy, F.; Reginster, J. The therapeutic effects of alfacalcidol on bone strength, muscle metabolism and prevention of falls and fractures. J. Musculoskelet. Neuronal Interact. 2005, 5, 273–284. [Google Scholar] [PubMed]
- Hanssens, L.; Reginster, J.Y. Relevance of bone mineral density, bone. Musculoskelet. Neuronal Interact. 2003, 3, 189–193. [Google Scholar]
- Taylor, M.E.; Delbaere, K.; Lord, S.R.; Mikolaizak, A.S.; Close, J.C. Physical impairments in cognitively impaired older people: Implications for risk of falls. Int. Psychogeriatr. 2013, 25, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Kurata, S.; Yamamoto, E.; Makino, K.; Kanamori, M. Impact of fall-related behaviors as risk factors for falls among the elderly patients with dementia in a geriatric facility in Japan. Am. J. Alzheimers Dis. Other Demen. 2012, 27, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.S.; Thackeray, A.; Duncan, R.P.; Cavanaugh, J.T.; Ellis, T.D.; Earhart, G.M.; Ford, M.P.; Foreman, K.B.; Dibble, L.E. Two-year trajectory of fall risk in people with Parkinson disease: A latent class analysis. Arch Phys. Med. Rehabil. 2016, 97, 372–379. [Google Scholar] [CrossRef] [Green Version]
- Allen, N.E.; Schwarzel, A.K.; Canning, C.G. Recurrent falls in Parkinson’s disease: A systematic review. Parkinsons Dis. 2013, 2013, 906274. [Google Scholar] [CrossRef] [Green Version]
- Hiorth, Y.; Laresn, J.P.; Lode, K.; Tysnes, O.B.; Godfrey, A.; Lord, S.; Rochester, L.; Pedersen, K.F. Impact of falls on physical activity in people with Parkinson’s disease. J. Parkinsons Dis. 2016, 6, 175–182. [Google Scholar] [CrossRef]
- Jansen, S.; Bhangu, J.; de Rooij, S.; Daams, J.; Kenny, R.A.; van der Velde, N. The Association of Cardiovascular Disorders and Falls:A Systematic Review. J. Am. Med. Dir. Assoc. 2016, 17, 193–199. [Google Scholar] [CrossRef]
- Bhangu, J.; King-Kallimanis, B.L.; Donoghue, O.A.; Carroll, L.; Kenny, R.A. Falls, non-accidental falls and syncope in community-dwelling adults aged 50 years and older:Implications for cardiovascular assessment. PLoS ONE 2017, 12, e0180997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalgaard, F.; Pallisgaard, J.L.; Numé, A.K.; Lindhardt, T.B.; Gislason, G.H.; Torp-Pedersen, C.; Ruwald, M.H. Rate or Rhythm Control in Older Atrial Fibrillation Patients:Risk of Fall-Related Injuries and Syncope. J. Am. Geriatr. Soc. 2019, 67, 2023–2030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliott, S.; Painter, J.; Hudson, S. Living Alone and Fall Risk Factors in Community-Dwelling Middle Age and Older Adults. J. Community Health 2009, 34, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Pathinarupothi, R.K.; Durga, P.; Rangan, E.S. IoT-Based Smart Edge for Global Health: Remote Monitoring With Severity Detection and Alerts Transmission. IEEE Internet Things J. 2019, 6, 2449–2462. [Google Scholar] [CrossRef]
- Taramasco, C.; Rodenas, T.; Martinez, F.; Fuentes, P.; Munoz, R.; Olivares, R.; de Albuquerque, V.H.C. A Novel Monitoring System for Fall Detection in Older People. IEEE Access 2018, 6, 43563–43574. [Google Scholar]
- Liu, S.W.; Obermeyer, Z.; Chang, Y.; Shankar, K.N. Frequency of ED revisits and death among older adults after a fall. Am. J. Emerg. Med. 2015, 33, 1012–1018. [Google Scholar] [CrossRef] [Green Version]
- Davis, J.C.; Robertson, M.C.; Ashe, M.C.; Liu-Ambrose, T.; Khan, K.M.; Marra, C.A. International comparison of cost of falls in older adults living in the community: A systematic review. Osteoporosis Int. 2010, 21, 1295–1306. [Google Scholar] [CrossRef]
- Sahlin, Y. Occurrence of fractures in a defined population:a 1-year study. Injury 1990, 21, 158–160. [Google Scholar] [CrossRef]
- Harvey, L.A.; Close, J.C. Traumatic brain injury in older adults: Characteristics, causes and consequences. Injury 2012, 43, 1821–1826. [Google Scholar] [CrossRef]
- Bouras, T.; Stranjalis, G.; Korfias, S.; Andrianakis, I.; Pitaridis, M.; Sakas, D.E. Head injury mortality in a geriatric population: Differentiating an “edge” age group with better potential for benefit than older poor-prognosis patients. J. Neurotrauma 2007, 24, 1355–1361. [Google Scholar] [CrossRef]
- Saari, P.; Heikkinen, E.; Sakari-Rantala, R.; Rantanen, T. Fall-related injuries among initially 75- and 80-year old people during a 10-year follow-up. Arch. Gerontol. Geriatr. 2007, 45, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Thompson, H.J.; McCormick, W.C.; Kagan, S.H. Traumatic brain injury in older adults: Epidemiology, outcomes, and future implications. J. Am. Geriatr. Soc. 2006, 54, 1590–1595. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.; Stevens, J.; Sarmiento, K.; Wald, M. Fall-related traumatic brain injury deaths and hospitalizations among older adults—United States, 2005. J. Safety Res. 2008, 39, 269–272. [Google Scholar] [CrossRef] [PubMed]
- Watson, W.L.; Mitchell, R. Conflicting trends in fall-related injury hospitalisations among older people: Variations by injury type. Osteoporos. Int. 2011, 22, 2623–2631. [Google Scholar] [CrossRef]
- Korhonen, N.; Niemi, S.; Parkkari, J.; Sievänen, H.; Kannus, P. Incidence of fall-related traumatic brain injuries among older Finnish adults between 1970 and 2011. JAMA 2013, 309, 1891–1892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crenshaw, J.R.; Bernhardt, K.A.; Achenbach, S.J.; Atkinson, E.J.; Khosla, S.; Kaufman, K.R.; Amin, S. The circumstances, orientations, and impact locations of falls in community-dwelling older women. Arch. Gerontol. Geriatr. 2017, 73, 240–247. [Google Scholar] [CrossRef]
- Schonnop, R.; Yang, Y.; Feldman, F.; Robinson, E.; Loughin, M.; Robinovitch, S.N. Prevalence of and factors associated with head impact during falls in older adults in long-term care. CMAJ 2013, 185, E803–E810. [Google Scholar] [CrossRef] [Green Version]
- Auvinet, E.; Multon, F.; Saint-Arnaud, A.; Rousseau, J.; Meunier, J. Fall detection with multiple cameras: An occlusion-resistant method based on 3-D silhouette vertical distribution. IEEE Trans. Inf. Technol. Biomed. 2011, 15, 290–300. [Google Scholar] [CrossRef]
- Feng, G.; Mai, J.; Ban, Z.; Guo, X.; Wang, G. Floor pressure imaging for fall detection with fiber-optic sensors. IEEE Pervasive Comput. 2016, 15, 40–47. [Google Scholar] [CrossRef]
- Maheshwari, S.; Tiwari, A. Ubiquitous fall detection through wireless channel state information. CoCoNet. 2015, 2, 1–9. [Google Scholar]
- Li, Y.; Ho, K.C.; Popescu, M. A microphone array system for automatic fall detection. IEEE Trans. Biomed. Eng. 2012, 59, 1291–1301. [Google Scholar] [PubMed]
- Sinnapolu, G.; Alawneh, S. Integrating wearables with cloud-based communication for health monitoring and emergency assistance. Internet. Things 2018, 1–2, 40–54. [Google Scholar] [CrossRef]
- Nguyen Gia, T.; Sarker, V.K.; Tcarenko, I.; Rahmani, A.M.; Westerlund, T.; Liljeberg, P.; Tenhunen, H. Energy efficient wearable sensor node for IoT-based fall detection systems. Microprocess. Microsyst. 2018, 56, 34–46. [Google Scholar] [CrossRef]
- Feng, P.; Yu, M.; Naqvi, S.M.; Chambers, J.A. Deep learning for posture analysis in fall detection. In Proceedings of the 2014 19th International Conference on Digital Signal Processing, Hong Kong, China, 20–23 August 2014; pp. 12–17. [Google Scholar]
- Yoo, S.; Oh, D. An artificial neural network–based fall detection. Int. J. Eng. Bus. Manag. 2018, 10, 1847979018787905. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, C.; Huang, C.; Liu, K.; Chu, W.; Chan, C. A machine learning approach to fall detection algorithm using wearable sensor. In Proceedings of the 2016 International Conference on Advanced Materials for Science and Engineering (ICAMSE), Chiang Mai, Thailand, 12–13 November 2016; pp. 707–710. [Google Scholar]
- Khojasteh, S.; Villar, J.; Chira, C.; González, V.; de la Cal, E. Improving fall detection using an on-wrist wearable accelerometer. Sensors 2018, 18, 1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, T.; Gu, Y.; Chen, Y.; Xiao, Y.; Wang, J. A mobile cloud collaboration fall detection system based on ensemble learning. arXiv 2019, arXiv:1907.04788. [Google Scholar]
- Saleh, M.; Jeannés, R.L.B. Elderly fall detection using wearable sensors: A low cost highly accurate algorithm. IEEE Sens. J. 2019, 19, 3156–3164. [Google Scholar] [CrossRef]
- Putra, I.; Brusey, J.; Gaura, E.; Vesilo, R. An event-triggered machine learning approach for accelerometer-based fall detection. Sensors 2017, 18, 20. [Google Scholar] [CrossRef] [Green Version]
- Zitouni, M.; Pan, Q.; Brulin, D.; Campo, E. Design of a smart sole with advanced fall detection algorithm. J. Sens. Technol. 2019, 9, 71. [Google Scholar] [CrossRef] [Green Version]
- Scheurer, S.; Koch, J.; Kucera, M.; Bryn, H.; Bärtschi, M.; Meerstetter, T.; Nef, T.; Urwyler, P. Optimization and technical validation of the AIDE-MOI fall detection algorithm in a real-life setting with older adults. Sensors 2019, 19, 1357. [Google Scholar] [CrossRef] [Green Version]
- Aziz, O.; Klenk, J.; Schwickert, L.; Chiari, L.; Becker, C.; Park, E.J.; Mori, G.; Robinovitch, S.N. Validation of accuracy of SVM-based fall detection system using real-world fall and non-fall datasets. PLoS ONE 2017, 12, e0180318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kangas, M.; Korpelainen, R.; Vikman, I.; Nyberg, L.; Jämsä, T. Sensitivity and false alarm rate of a fall sensor in long-term fall detection in the elderly. Gerontology 2015, 61, 61–68. [Google Scholar] [CrossRef]
- Lipsitz, L.A.; Tchalla, A.E.; Iloputaife, I.; Gagnon, M.; Dole, K.; Su, Z.Z.; Klickstein, L. Evaluation of an automated falls detection device in nursing home residents. J. Am. Geriatr. Soc. 2016, 64, 365–368. [Google Scholar] [CrossRef]
- Ren, L.; Peng, Y. Research of Fall Detection and Fall Prevention Technologies: A Systematic Review. IEEE Access 2019, 7, 77702–77722. [Google Scholar] [CrossRef]
- Kelly Joseph, M. Dead Reckoning Based Initialization of Position and Heading Using Discrete Position Indicators US9175963 (B2). U.S. Patent No. 9,175,963, 3 November 2015. [Google Scholar]
- Huang, J.H.; Wang, L.C.; Chang, C.J. Architectures and Deployment Strategies for Wireless Mesh Networks. In Wireless Mesh Networks; Hossain, E., Leung, K., Eds.; Springer: Boston, MA, USA, 2008. [Google Scholar]
- Lin, H.-C.; Chen, M.-J.; Huang, J.-T. An IoT-based Smart Healthcare System using Location-based Mesh Network and Big Data Analytics. J. Ambient. Intell. Smart Environ. 2022, 14, 483–509. [Google Scholar] [CrossRef]
- Berglund, M.E.; Duvall, J.; Dunne, L.E. A survey of the historical scope and current trends of wearable technology applications. In Proceedings of the International Symposium on Wearable Computers, Heidelberg, Germany, 12–16 September 2016; IEEE Computer Society: New York, NY, USA, 2016; pp. 40–43. [Google Scholar]
- Gao, L.; Bourke, A.K.; Nelson, J. Evaluation of accelerometer based multi-sensor versus single-sensor activity recognition systems. Med. Eng. Phys. 2014, 36, 779–785. [Google Scholar] [CrossRef]
- Awais, M.; Palmerini, L.; Chiari, L. Physical activity classification using body-worn inertial sensors in a multi-sensor setup. In Proceedings of the 2016 IEEE 2nd International Forum on Research and Technologies for Society and Industry Leveraging a Better Tomorrow, Bologna, Italy, 7–9 September 2016. [Google Scholar]
- Gjoreski, H.; Rashkovska, A.; Kozina, S.; Lustrek, M.; Gams, M. Telehealth using ECG sensor and accelerometer. In Proceedings of the 2014 37th International Convention on Information and Communication Technology, Electronics and Microelectronics (MIPRO), Opatija, Croatia, 26–30 May 2014; pp. 270–274. [Google Scholar]
- Zhang, J.H.; Macfarlane, D.J.; Sobko, T. Feasibility of a Chest-worn accelerometer for physical activity measurement. J. Sci. Med. Sport. 2016, 19, 1015–1019. [Google Scholar] [CrossRef] [Green Version]
- D’Mello, Y.; Skoric, J.; Xu, S.; Akhras, M.; Roche, P.J.; Lortie, M.A.; Gagnon, S.; Plant, D.V. Autocorrelated Differential Algorithm for Real-Time Seismocardiography Analysis. IEEE Sens. J. 2019, 19, 5127–5514. [Google Scholar] [CrossRef]
- Yu, S.; Liu, S. A novel adaptive recursive least squares filter to remove the motion artifact in seismocardiography. Sensors 2020, 20, 1596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, C.; Uchiyama, H.; Thomas, D.; Shimada, A.; Taniguchi, R.I. Indoor Positioning System Based on Chest-Mounted IMU. Sensors 2019, 19, 420. [Google Scholar] [CrossRef] [Green Version]
- Wu, F.; Zhao, H.; Zhao, Y.; Zhong, H. Development of a wearable-sensor-based fall detection system. Int. J. Telemed. Appl. 2015, 2015, 576364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, A.; Ma, X.; He, Y.; Luo, J. Highly portable, sensor-based system for human fall monitoring. Sensors 2017, 17, 2096. [Google Scholar] [CrossRef] [PubMed] [Green Version]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bosch Sensortec | BMX055 Accelerometer | BMX055 Gyroscope | BMX055 Magnetometer | BMP280 Barometer |
|---|---|---|---|---|
| Operating range | ±4 g | ±1000 °/s | ±1300 µT(x,y) ±2500 µT(z) | 300 to 1100 hPa |
| Sensitivity | 512 LSB/g | 32.8 LSB/°/sec | 3.3 LSB/µT | 6 LSB/Pa |
| Accuracy | - | - | ±2.5 degree | ±1 hPa/±1 m/±1 °C |
| Interface type | I2C, SPI | I2C, SPI | I2C, SPI | I2C, SPI |
| Operating supply voltage (V) | 1.2 to 3.6 | 1.2 to 3.6 | 1.2 to 3.6 | 1.71 to 3.6 |
| Resolution (bit) | 12 | 16 | 16 | 16 to 20 |
| Sample rate (Hz) | 100 | 100 | 100 | 100 |
| Current consumption (mA) | 0.13 | 5 | 0.8/4.9 | 0.0042 |
| Operation case | All | Walking and falling (standing up and sitting down) | Walking and falling (standing up and sitting down) | Walking |
| Using time (h) | 24 | 2 | 2 | 2 |
| Power consumption (mAh) | 3.12 | 10 | 1.6/9.8 | 0.0084 |
| Category | A | B | C |
|---|---|---|---|
| Type of fall | A fall while sitting down | A fall while standing | A fall while standing up |
| Sensitivity | 94% | 96% | 95% |
| Specificity | 95% | 97% | 95% |
| Accuracy | 95% | 96% | 95% |
| Ref | Sample Size (Persons) | Wearable Sensor (Type, Number, Location) | Methodology | Result |
|---|---|---|---|---|
| 59 | 3 | 1 accelerometer | Quaternion algorithm using sum acceleration and rotation angle data | Sensitivity: 97.1%, Specificity: 98.3%. Accuracy: N/A |
| Waist | ||||
| 60 | 15 | 1 accelerometer 1 gyroscope 1 magnetometer | An algorithm based on acceleration and the angle of yaw, pitch, and roll, which is run on a smartphone | Sensitivity: 100% Specificity: 91.1% (shoulder) 100% (waist) 78.5% (foot) Accuracy: 100% |
| Shoulder Waist Foot | ||||
| Our work | 12 | 1 accelerometer, 1 gyroscope 1 magnetometer | Gradient descent algorithm based on the vector sum of acceleration and barometer record | Sensitivity: 94–96% Specificity: 95–97% Accuracy: 95–96% |
| Sense4CareSTAT-ON | Lifeline AutoAlert | Apple Watch (Ultra 49 mm) | This Work | |
|---|---|---|---|---|
| Detection sensor | three-axis accelerometer | three-axis accelerometer/ barometer | nine-axis accelerometer/barometer | nine-axis accelerometer/barometer |
| Sampling rate (Hz) | 40 | N/A | N/A | 100 |
| Size (mm)/ weight (g) | 90 × 62.5 × 21.2/ 86 | 90 × 45 × 18/ 56 | 49 × 44 × 14.4/ 61 | 34 × 34 × 15/ 15 |
| Battery (mAh) | 1200 | 2000 | 542 | 150 |
| Average current (mA) | 4.1 ± 4.2 | N/A | N/A | 4.5 ±1.2 |
| Battery life | 8 h/day for 7 days = 56 h | 5 days | Battery went from 100% down to 18% during 12 h | Continuous for 24 h |
| Installation location | Waist | Around the neck | Wrist | Chest |
| Fixation method | A belt | Pendants | A strap | Adhesives and necklace |
| Fall detection | Yes | Yes | Yes | Yes |
| Direction of the fall | No | No | No | Yes |
| Force of the fall | No | No | No | Yes |
| Posture before the fall | No | No | No | Yes |
| Movement and posture | For Parkinson’s disease | No | No | Yes |
| Combination with a smart speaker | No | Yes | Medical Guardian Mini Guardian (two-way speaker function, optional) | Yes |
| Combination with a physiological wristband | No | No | Has a physiological wristband function | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, H.-C.; Chen, M.-J.; Lee, C.-H.; Kung, L.-C.; Huang, J.-T. Fall Recognition Based on an IMU Wearable Device and Fall Verification through a Smart Speaker and the IoT. Sensors 2023, 23, 5472. https://doi.org/10.3390/s23125472
Lin H-C, Chen M-J, Lee C-H, Kung L-C, Huang J-T. Fall Recognition Based on an IMU Wearable Device and Fall Verification through a Smart Speaker and the IoT. Sensors. 2023; 23(12):5472. https://doi.org/10.3390/s23125472
Chicago/Turabian StyleLin, Hsin-Chang, Ming-Jen Chen, Chao-Hsiung Lee, Lu-Chih Kung, and Jung-Tang Huang. 2023. "Fall Recognition Based on an IMU Wearable Device and Fall Verification through a Smart Speaker and the IoT" Sensors 23, no. 12: 5472. https://doi.org/10.3390/s23125472