
A Novel Methodology for the Synchronous Collection and Multimodal Visualization of Continuous Neurocardiovascular and Neuromuscular Physiological Data in Adults with Long COVID

 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
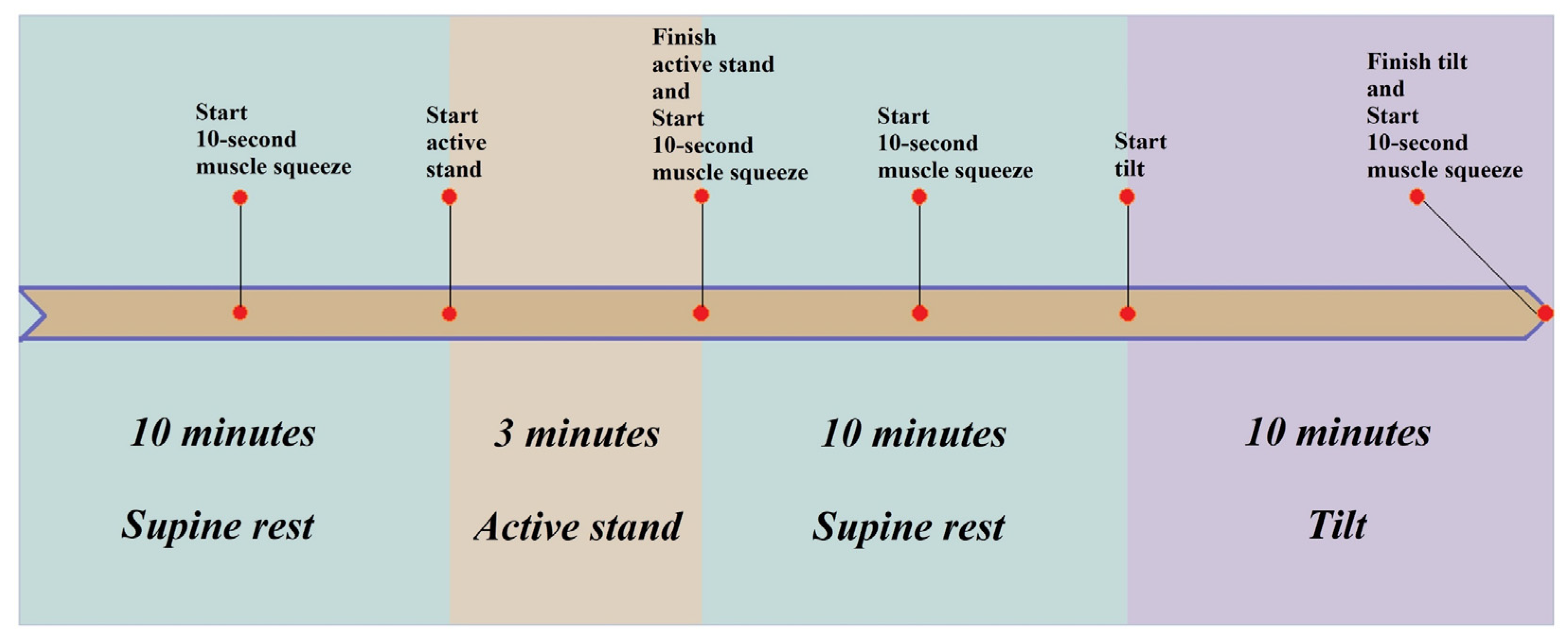
2.1. Assessment Protocol
2.1.1. Active Stand
2.1.2. Head-Up Tilt
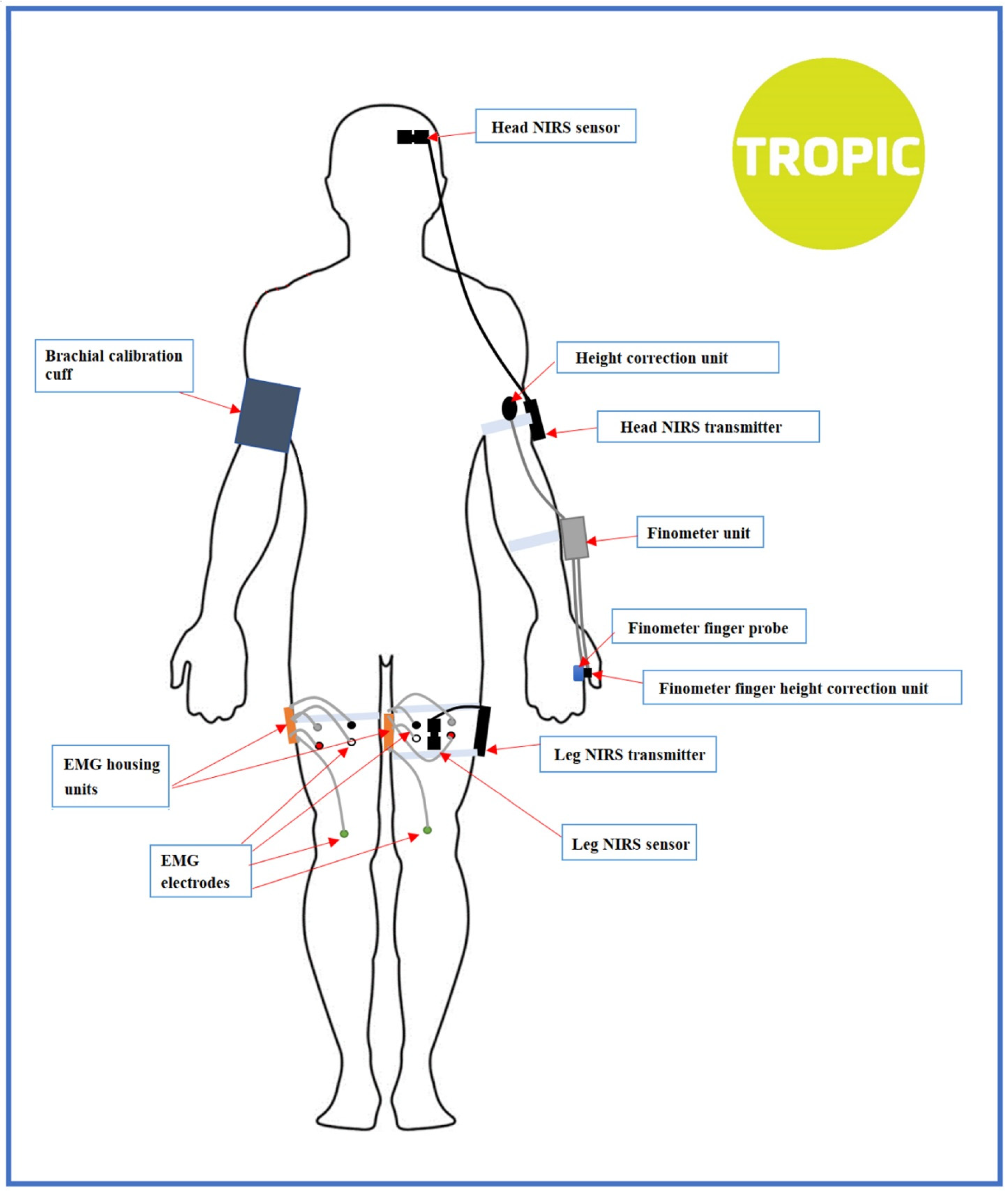
2.2. Instrumentation
2.2.1. Finapres® NOVA
2.2.2. NIRS
2.2.3. Surface EMG
2.3. Data Management
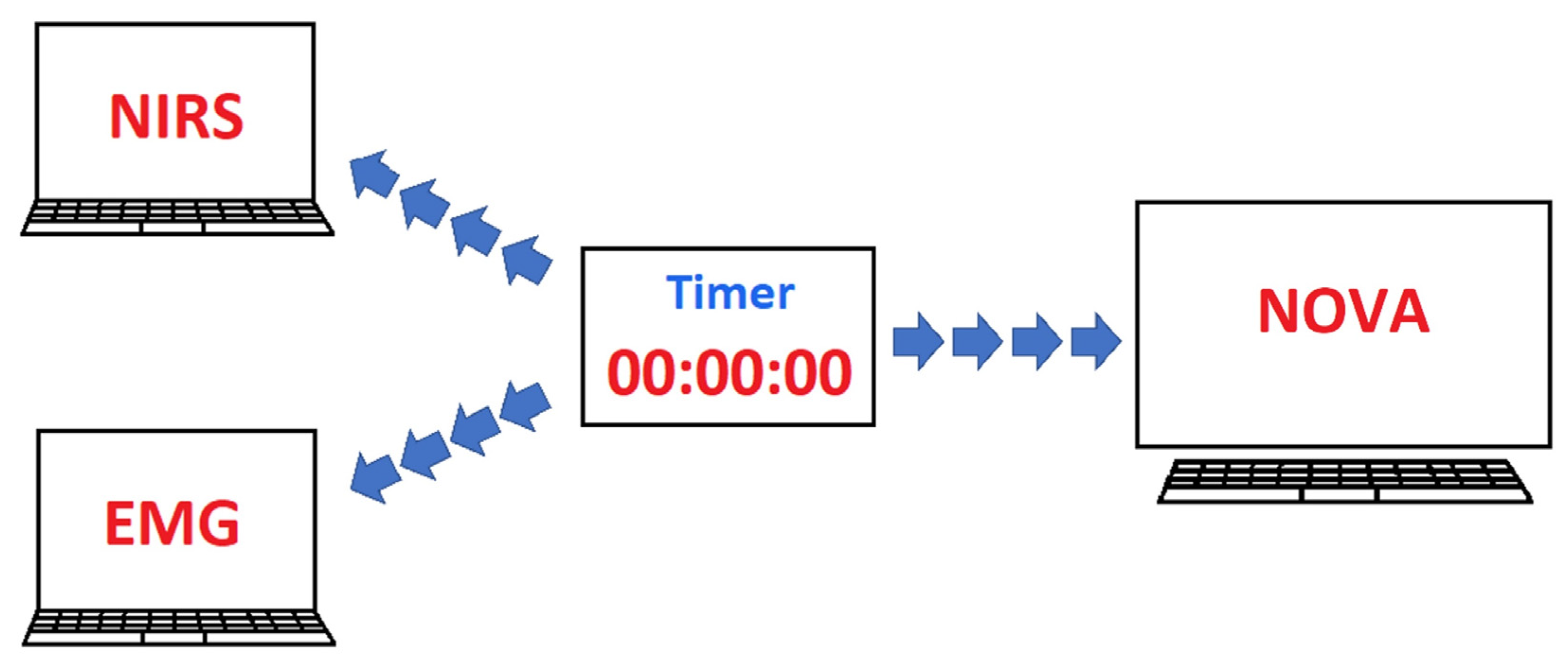
2.3.1. Data Collection
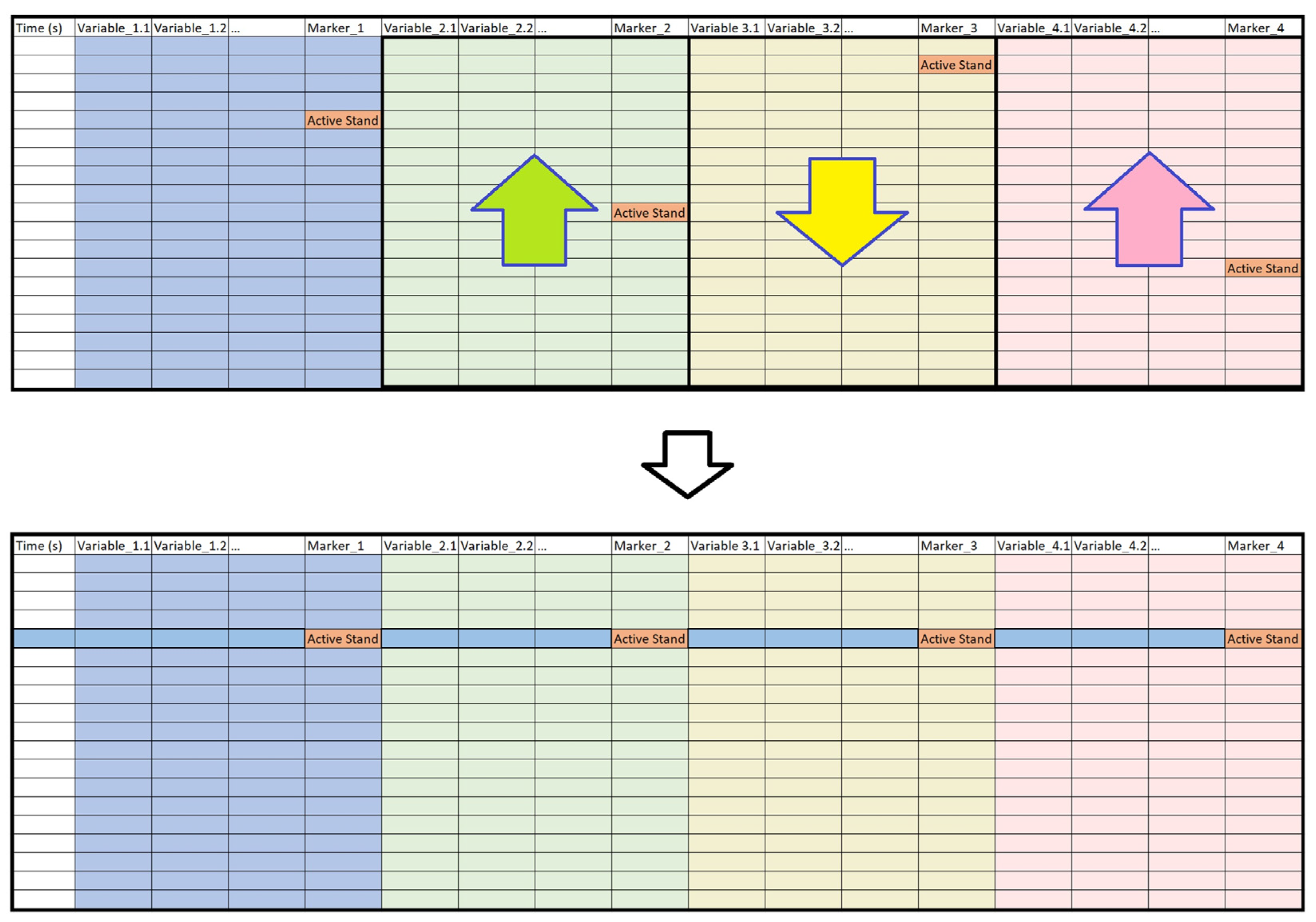
2.3.2. Data Processing
Data Merging
Three-Stage Data Syncing
2.3.3. Visualization for Comparative Studies
3. Results
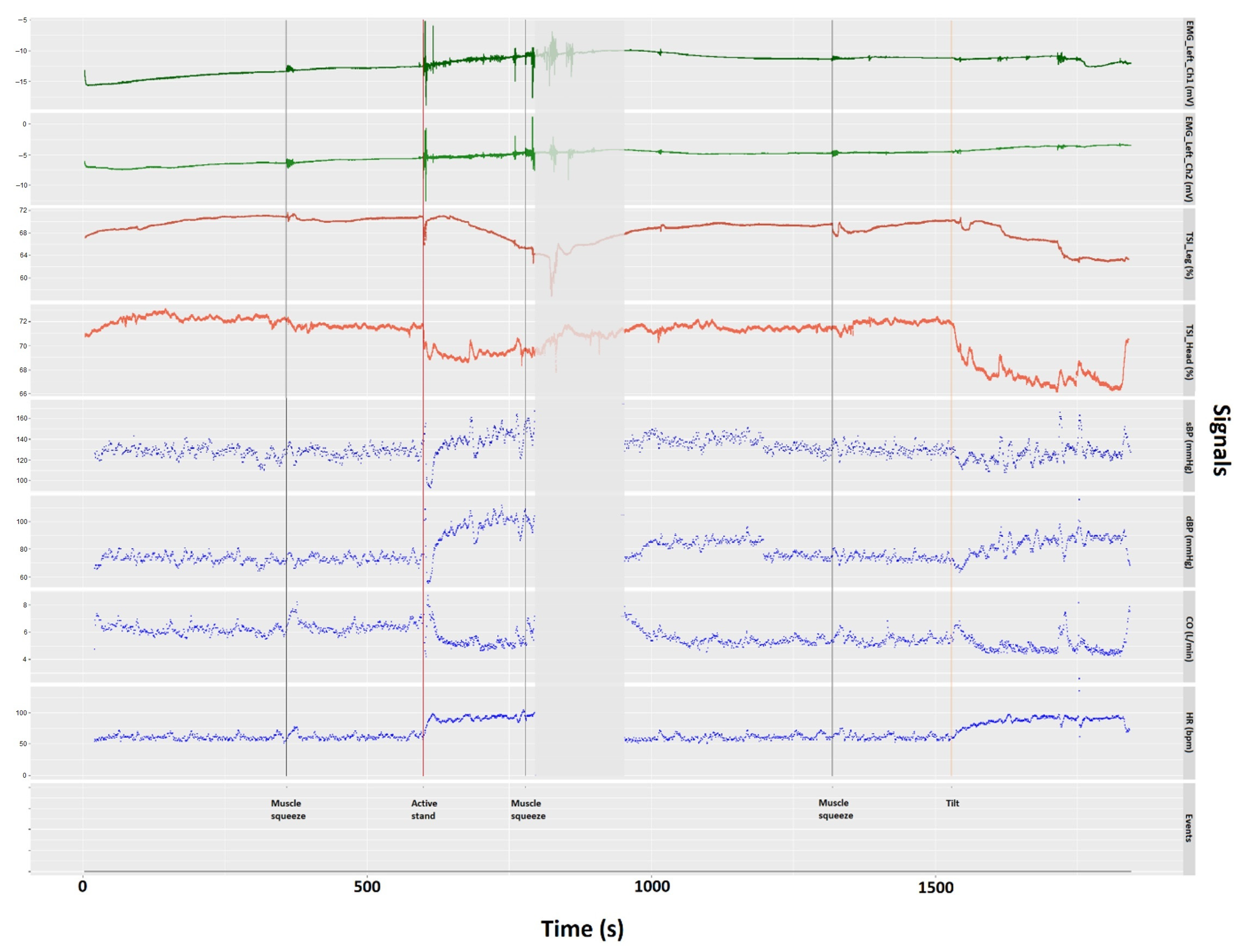
3.1. Assessment Visualization
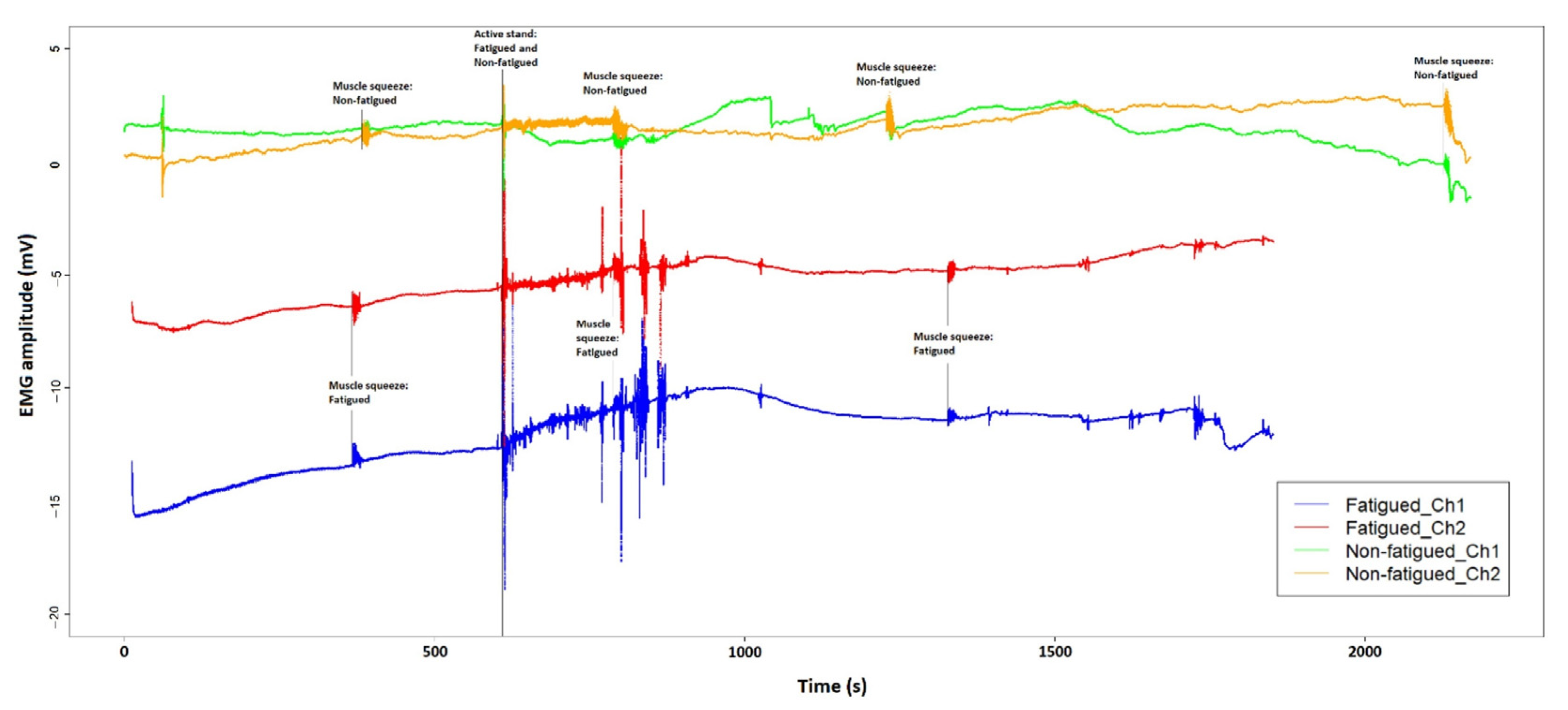
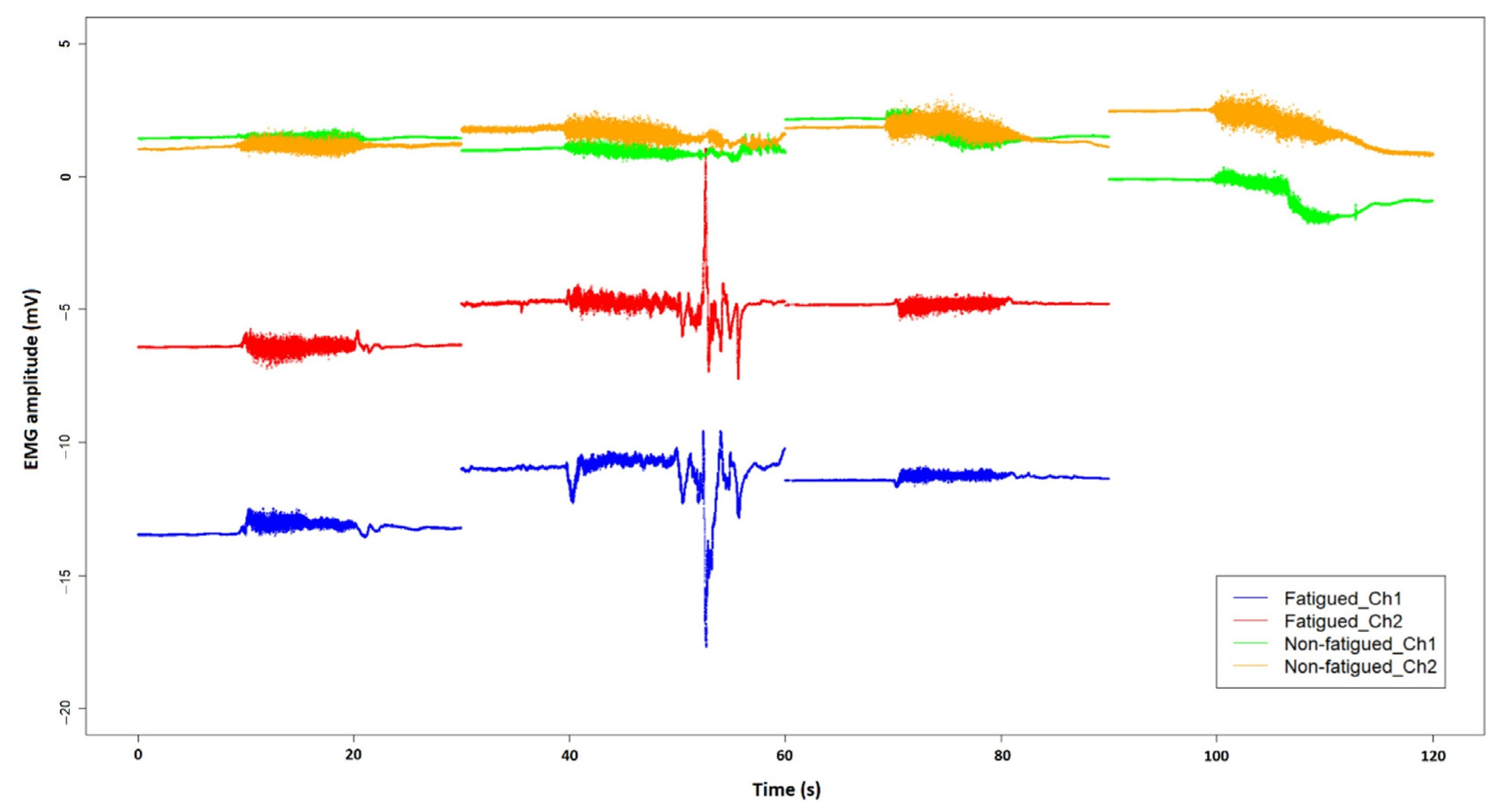
3.2. EMG Comparison
4. Discussion
4.1. Raw Data Visualization for NCVI/NMFI Assessment
4.2. Data Syncing
4.3. EMG Sampling Frequency
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| OI | Orthostatic Intolerance |
| NCVI | Neurocardiovascular Instability |
| NMFI | Neuromuscular Function Impairment |
| NIRS | Near-Infrared Spectroscopy |
| EMG | Electromyography |
| O2Hb | Oxygenated Hemoglobin |
| HHb | Deoxygenated Hemoglobin |
| TSI | Tissue Saturation Index |
| SBP | Systolic Blood Pressure |
| DBP | Diastolic Blood Pressure |
| CO | Cardiac Output |
| BLE | Bluetooth Low Energy |
References
- WHO Coronavirus (COVID-19) Dashboard. 2022. Available online: https://covid19.who.int/ (accessed on 7 January 2022).
- Ares-Blanco, S.; Astier-Peña, M.P.; Gómez-Bravo, R.; Fernández-García, M.; Bueno-Ortiz, J.M. The role of primary care during COVID-19 pandemic: A European overview. Aten Primaria 2021, 53, 102134. [Google Scholar] [CrossRef] [PubMed]
- Lavie, G.; Weinstein, O.; Segal, Y.; Davidson, E. Adapting to change: Clalit’s response to the COVID-19 pandemic. Isr. J. Health Policy Res. 2021, 10, 68. [Google Scholar] [CrossRef] [PubMed]
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing Covid-19 vaccines at pandemic speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef] [PubMed]
- Jennings, G.; Monaghan, A.; Xue, F.; Mockler, D.; Romero-Ortuño, R. A Systematic Review of Persistent Symptoms and Residual Abnormal Functioning following Acute COVID-19: Ongoing Symptomatic Phase vs. Post-COVID-19 Syndrome. J. Clin. Med. 2021, 10, 5913. [Google Scholar] [CrossRef]
- Maiese, A.; Frati, P.; Del Duca, F.; Santoro, P.; Manetti, A.C.; La Russa, R.; Di Paolo, M.; Turillazzi, E.; Fineschi, V. Myocardial pathology in COVID-19-associated cardiac injury: A systematic review. Diagnostics 2021, 11, 1647. [Google Scholar] [CrossRef]
- Monaghan, A.; Jennings, G.; Xue, F.; Byrne, L.; Duggan, E.; Romero-Ortuno, R. Orthostatic intolerance in adults with long COVID was not associated with postural orthostatic tachycardia syndrome. Front. Physiol.-Auton. Neurosci. 2021, in press. [Google Scholar]
- Dani, M.; Dirksen, A.; Taraborrelli, P.; Torocastro, M.; Panagopoulos, D.; Sutton, R.; Lim, P.B. Autonomic dysfunction in ‘long COVID’: Rationale, physiology and management strategies. Clin. Med. 2021, 21, e63–e67. [Google Scholar] [CrossRef]
- Shouman, K.; Vanichkachorn, G.; Cheshire, W.P.; Suarez, M.D.; Shelly, S.; Lamotte, G.J.; Sandroni, P.; Benarroch, E.E.; Berini, S.E.; Cutsforth-Gregory, J.K.; et al. Autonomic dysfunction following COVID-19 infection: An early experience. Clin. Auton. Res. 2021, 31, 385–394. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef]
- Paliwal, V.K.; Garg, R.K.; Gupta, A.; Tejan, N. Neuromuscular presentations in patients with COVID-19. Neurol. Sci. 2020, 41, 3039–3056. [Google Scholar] [CrossRef]
- Guidon, A.C.; Amato, A.A. COVID-19 and neuromuscular disorders. Neurology 2020, 94, 959–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Callaghan, S.; Kenny, R.A. Neurocardiovascular Instability and Cognition. Yale J. Biol. Med. 2016, 89, 59–71. [Google Scholar] [PubMed]
- Collins, O.; Kenny, R.A. Is neurocardiovascular instability a risk factor for cognitive decline and/or dementia? The science to date. Rev. Clin. Gerontol. 2007, 17, 153–160. [Google Scholar] [CrossRef]
- Finucane, C.; van Wijnen, V.K.; Fan, C.W.; Soraghan, C.; Byrne, L.; Westerhof, B.E.; Freeman, R.; Fedorowski, A.; Harms, M.P.M.; Wieling, W.; et al. A practical guide to active stand testing and analysis using continuous beat-to-beat non-invasive blood pressure monitoring. Clin. Auton. Res. 2019, 29, 427–441. [Google Scholar] [CrossRef] [PubMed]
- Metzler, M.; Duerr, S.; Granata, R.; Krismer, F.; Robertson, D.; Wenning, G.K. Neurogenic orthostatic hypotension: Pathophysiology, evaluation, and management. J. Neurol. 2013, 260, 2212–2219. [Google Scholar] [CrossRef] [Green Version]
- Tansey, E.A.; Montgomery, L.E.A.; Quinn, J.G.; Roe, S.M.; Johnson, C.D. Understanding basic vein physiology and venous blood pressure through simple physical assessments. Adv. Physiol. Educ. 2019, 43, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Stewart, J.M. Mechanisms of sympathetic regulation in orthostatic intolerance. J. Appl. Physiol. 2012, 113, 1659–1668. [Google Scholar] [CrossRef] [Green Version]
- Biaggioni, I.; Shibao, C.A.; Diedrich, A.; Muldowney, J.A.S.; Laffer, C.L.; Jordan, J. Blood Pressure Management in Afferent Baroreflex Failure: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 74, 2939–2947. [Google Scholar] [CrossRef]
- Grubb, B. Neurocardiogenic syncope and related disorders of orthostatic intolerance. Circulation 2005, 111, 2997–3006. [Google Scholar] [CrossRef] [Green Version]
- Masterson, M.M.; Morgan, A.L.; Multer, C.E.; Cipriani, D. The role of lower leg muscle activity in blood pressure maintenance of older adults. Clin. Kinesiol. 2006, 60, 8–17. [Google Scholar]
- Garg, A.; Xu, D.; Blaber, A.P. Statistical validation of wavelet transform coherence method to assess the transfer of calf muscle activation to blood pressure during quiet standing. Biomed. Eng. Online 2013, 12, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, D.; Verma, A.K.; Garg, A.; Bruner, M.; Fazel-Rezai, R.; Blaber, A.P.; Tavakolian, K. Significant role of the cardiopostural interaction in blood pressure regulation during standing. Am. J. Physiol. Heart Circ. Physiol. 2017, 313, H568–H577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Technology Assisted Solutions for the Recognition of Objective Physiological Indicators of Post-Coronavirus-19 Fatigue (TROPIC). Available online: https://clinicaltrials.gov/ct2/show/NCT05027724 (accessed on 7 January 2022).
- Frith, J. Diagnosing orthostatic hypotension: A narrative review of the evidence. Br. Med. Bull. 2015, 2015. 115, 123–134. [Google Scholar] [CrossRef] [Green Version]
- Fessel, J.; Robertson, D. Orthostatic hypertension: When pressor reflexes overcompensate. Nat. Clin. Pract. Nephrol. 2006, 2, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Fedorowski, A. Postural orthostatic tachycardia syndrome: Clinical presentation, aetiology and management. J. Intern. Med. 2019, 285, 352–366. [Google Scholar] [CrossRef] [PubMed]
- Brignole, M.; Moya, A.; de Lange, F.J.; Deharo, J.C.; Elliott, P.M.; Fanciulli, A.; Feorowski, A.; Furlan, R.; Kenny, R.A.; Martin, A.; et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef]
- Wesseling, K.H. Finger arterial pressure measurement with Finapres. Z. Kardiol. 1996, 85, 38–44. [Google Scholar] [PubMed]
- Teodorovich, N.; Swissa, M. Tilt table test today—State of the art. World J. Cardiol. 2016, 8, 277–282. [Google Scholar] [CrossRef]
- Aponte-Becerra, L.; Novak, P. Tilt Test: A Review. J. Clin. Neurophysiol. 2021, 38, 279–286. [Google Scholar] [CrossRef]
- Ferrari, M.; Quaresima, V. A brief review on the history of human functional near-infrared spectroscopy (fNIRS) development and fields of application. Neuroimage 2012, 63, 921–935. [Google Scholar] [CrossRef]
- Scholkmann, F.; Kleiser, S.; Metz, A.J.; Zimmermann, R.; Mata Pavia, J.; Wolf, U.; Wolf, M. A review on continuous wave functional near-infrared spectroscopy and imaging instrumentation and methodology. Neuroimage 2014, 85, 6–27. [Google Scholar] [CrossRef] [PubMed]
- Cortese, L.; Zanoletti, M.; Karadeniz, U.; Pagliazzi, M.; Yaqub, M.A.; Busch, D.R.; Mesquida, J.; Durduran, T. Performance Assessment of a Commercial Continuous-Wave Near-Infrared Spectroscopy Tissue Oximeter for Suitability for Use in an International, Multi-Center Clinical Trial. Sensors 2021, 21, 6957. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.; Tgavalekos, K.; Sassaroli, A.; Blaney, G.; Fantini, S. Quantitative measurements of cerebral blood flow with near-infrared spectroscopy. Biomed. Opt. Express 2019, 10, 2117–2134. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, M.; Muthalib, M.; Quaresima, V. The use of near-infrared spectroscopy in understanding skeletal muscle physiology: Recent developments. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2011, 369, 4577–4590. [Google Scholar] [CrossRef]
- Bunce, S.C.; Izzetoglu, M.; Izzetoglu, K.; Onaral, B.; Pourrezaei, K. Functional near-infrared spectroscopy. IEEE Eng. Med. Biol. Mag. 2006, 25, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Boas, D.A.; Elwell, C.E.; Ferrari, M.; Taga, G. Twenty years of functional near-infrared spectroscopy: Introduction for the special issue. Neuroimage 2014, 85, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Sanni, A.A.; McCully, K.K. Interpretation of Near-Infrared Spectroscopy (NIRS) Signals in Skeletal Muscle. J. Funct. Morphol. Kinesiol. 2019, 4, 28. [Google Scholar] [CrossRef] [Green Version]
- Hesford, C.M.; Laing, S.J.; Cardinale, M.; Cooper, C.E. Asymmetry of quadriceps muscle oxygenation during elite short-track speed skating. Med. Sci. Sports Exerc. 2012, 44, 501–508. [Google Scholar] [CrossRef]
- Tsuji, M.; duPlessis, A.; Taylor, G.; Crocker, R.; Volpe, J.J. Near infrared spectroscopy detects cerebral ischemia during hypotension in piglets. Pediatr. Res. 1998, 44, 591–595. [Google Scholar] [CrossRef] [Green Version]
- Newman, L.; Nolan, H.; Carey, D.; Reilly, R.B.; Kenny, R.A. Age and sex differences in frontal lobe cerebral oxygenation in older adults-Normative values using novel, scalable technology: Findings from the Irish Longitudinal Study on Ageing (TILDA). Arch. Gerontol. Geriatr. 2020, 87, 103988. [Google Scholar] [CrossRef]
- Elamvazuthi, I.; Zulkifli, Z.; Ali, Z.; Khan, M.K.A.A.; Parasuraman, S.; Balaji, M.; Chandrasekaran, M. Development of Electromyography Signal Signature for Forearm Muscle. Procedia Comput. Sci. 2015, 76, 229–234. [Google Scholar] [CrossRef] [Green Version]
- Merletti, R.; Lo Conte, L.R. Surface EMG signal processing during isometric contractions. J. Electromyogr. Kinesiol. 1997, 7, 241–250. [Google Scholar] [CrossRef]
- Raez, M.B.; Hussain, M.S.; Mohd-Yasin, F. Techniques of EMG signal analysis: Detection, processing, classification and applications. Biol. Proced. Online 2006, 8, 11–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merletti, R.; Cerone, G.L. Tutorial. Surface EMG detection, conditioning and pre-processing: Best practices. J. Electromyogr. Kinesiol. 2020, 54, 102440. [Google Scholar] [CrossRef] [PubMed]
- Klasser, G.D.; Okeson, J. The clinical usefulness of surface electromyography in the diagnosis and treatment of temporomandibular disorders. J. Am. Dent. Assoc. 2006, 137, 763–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, A.S.; Gavião, M.B.; Derossi, M.; Gameiro, G.H. Electromyographic activity and thickness of masticatory muscles in children with unilateral posterior crossbite. Clin. Anat. 2009, 22, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Cecílio, F.A.; Regalo, S.C.; Palinkas, M.; Issa, J.P.; Siéssere, S.; Hallak, J.E.; Machado-de-Sausa, J.P.; Semprini, M. Ageing and surface EMG activity patterns of masticatory muscles. J. Oral Rehabil. 2010, 37, 248–255. [Google Scholar] [CrossRef]
- Vigotsky, A.D.; Halperin, I.; Lehman, G.J.; Trajano, G.S.; Vieira, T.M. Interpreting Signal Amplitudes in Surface Electromyography Studies in Sport and Rehabilitation Sciences. Front. Physiol. 2017, 8, 985. [Google Scholar] [CrossRef] [Green Version]
- Felici, F.; Del Vecchio, A. Surface Electromyography: What Limits Its Use in Exercise and Sport Physiology? Front. Neurol. 2020, 11, 578504. [Google Scholar] [CrossRef]
- McManus, L.; De Vito, G.; Lowery, M.M. Analysis and Biophysics of Surface EMG for Physiotherapists and Kinesiologists: Toward a Common Language With Rehabilitation Engineers. Front. Neurol. 2020, 11, 576729. [Google Scholar] [CrossRef]
- Mano, T. Muscle Sympathetic Nerve Activity in Blood Pressure Control Against Gravitational Stress. J. Cardiovasc. Pharmacol. 2001, 38, S7–S11. [Google Scholar] [CrossRef] [PubMed]
- Ray, C.A.; Rea, R.F.; Clary, M.P.; Mark, A.L. Muscle sympathetic nerve responses to static leg exercise. J. Appl. Physiol. 1992, 73, 1523–1529. [Google Scholar] [CrossRef] [PubMed]
- De Luca, C.J.; Gilmore, L.D.; Kuznetsov, M.; Roy, S.H. Filtering the surface EMG signal: Movement artifact and baseline noise contamination. J. Biomech. 2010, 43, 1573–1579. [Google Scholar] [CrossRef] [PubMed]
- Afsharipour, B.; Soedirdjo, S.; Merletti, R. Two-dimensional surface EMG: The effects of electrode size, interelectrode distance and image truncation. Biomed. Signal Processing Control. 2019, 49, 298–307. [Google Scholar] [CrossRef]
- Chowdhury, R.H.; Reaz, M.B.; Ali, M.A.; Bakar, A.A.; Chellappan, K.; Chang, T.G. Surface electromyography signal processing and classification techniques. Sensors 2013, 13, 12431–12466. [Google Scholar] [CrossRef]
- Hodges, P.W.; Richardson, C.A. Relationship between limb movement speed and associated contraction of the trunk muscles. Ergonomics 1997, 40, 1220–1230. [Google Scholar] [CrossRef]
- Di Fabio, R.P. Reliability of computerized surface electromyography for determining the onset of muscle activity. Phys. Ther. 1987, 67, 43–48. [Google Scholar] [CrossRef] [Green Version]
- Mathiassen, S.E.; Winkel, J.; Hägg, G.M. Normalization of surface EMG amplitude from the upper trapezius muscle in ergonomic studies—A review. J. Electromyogr. Kinesiol. 1995, 5, 197–226. [Google Scholar] [CrossRef]
- Erdelyi, A.; Sihvonen, T.; Helin, P.; Hänninen, O. Shoulder strain in keyboard workers and its alleviation by arm supports. Int. Arch. Occup. Environ. Health 1988, 60, 119–124. [Google Scholar] [CrossRef]
- Granström, B.; Kvarnström, S.; Tiefenbacher, F. Electromyography as an aid in the prevention of excessive shoulder strain. Appl. Ergon. 1985, 16, 49–54. [Google Scholar] [CrossRef]
- Sardu, C.; De Lucia, C.; Wallner, M.; Santulli, G. Diabetes Mellitus and Its Cardiovascular Complications: New Insights into an Old Disease. J. Diabetes Res. 2019, 2019, 1905194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trierweiler, H.; Kisielewicz, G.; Jonasson, T.H.; Petterle, R.R.; Moreira, C.A.; Borba, V.Z.C. Sarcopenia: A chronic complication of type 2 diabetes mellitus. Diabetol. Metab. Syndr. 2018, 10, 25. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zhu, X.; Wu, G.; Ding, W. Data Mining with Big Data. Knowledge and Data Engineering. IEEE Trans. Knowl. Data Eng. 2014, 26, 97–107. [Google Scholar]
- Tammen, H.; Hess, R. Data Preprocessing, Visualization, and Statistical Analyses of Nontargeted Peptidomics Data from MALDI-MS. Methods Mol. Biol. 2018, 1719, 187–196. [Google Scholar]
- Chang, J.-R.; Chen, Y.-S.; Lin, C.-K.; Cheng, M.-F. Advanced Data Mining of SSD Quality Based on FP-Growth Data Analysis. Appl. Sci. 2021, 11, 1715. [Google Scholar] [CrossRef]
- Zhiyi, T.; Zhicheng, C.; Yuequan, B.; Hui, L. Convolutional neural network-based data anomaly detection method using multiple information for structural health monitoring. Struct. Control. Health Monit. 2018, 26, e2296. [Google Scholar]
- García, S.; Ramírez-Gallego, S.; Luengo, J.; Benítez, J.M.; Herrera, F. Big data preprocessing: Methods and prospects. Big Data Anal. 2016, 1, 9. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.; Huang, Q.; Li, Z.; Liu, K.; Hu, F. Big Data and cloud computing: Innovation opportunities and challenges. Int. J. Digit. Earth 2016, 10, 13–53. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Gupta, A. Dealing with Noise Problem in Machine Learning Data-sets: A Systematic Review. Procedia Comput. Sci. 2019, 161, 466–474. [Google Scholar] [CrossRef]
- Schutte, A.E.; Huisman, H.W.; van Rooyen, J.M.; Malan, N.T.; Schutte, R. Validation of the Finometer device for measurement of blood pressure in black women. J. Hum. Hypertens. 2004, 18, 79–84. [Google Scholar] [CrossRef] [Green Version]
- Hakim, K.; Mole, J.; Mahajan, R. Comparison of blood pressure (BP) measurements using arm cuff and finometry during induction of anaesthesia: 3AP1–8. Eur. J. Anaesthesiol. EJA 2010, 27, 45. [Google Scholar] [CrossRef]
- Carlson, D.J.; Dieberg, G.; McFarlane, J.R.; Smart, N.A. Blood pressure measurements in research: Suitability of auscultatory, beat-to-beat, and ambulatory blood pressure measurements. Blood Press Monit. 2019, 24, 18–23. [Google Scholar] [CrossRef] [PubMed]
- González-Cañete, F.J.; Casilari, E. Consumption Analysis of Smartphone based Fall Detection Systems with Multiple External Wireless Sensors. Sensors 2020, 20, 622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tipparaju, V.V.; Mallires, K.R.; Wang, D.; Tsow, F.; Xian, X. Mitigation of Data Packet Loss in Bluetooth Low Energy-Based Wearable Healthcare Ecosystem. Biosensors 2021, 11, 350. [Google Scholar] [CrossRef]
- Tosi, J.; Taffoni, F.; Santacatterina, M.; Sannino, R.; Formica, D. Performance Evaluation of Bluetooth Low Energy: A Systematic Review. Sensors 2017, 17, 2898. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.; Wu, F.; Qiu, C.; Redouté, J.M.; Yuce, M.R. A Rigid-Flex Wearable Health Monitoring Sensor Patch for IoT-Connected Healthcare Applications. IEEE Internet Things J. 2020, 7, 6932–6945. [Google Scholar] [CrossRef]
- Bravo-Zanoguera, M.; Cuevas-Gonzalez, D.; Reyna, M.A.; Garcia-Vazquez, J.P.; Avitia, R.L. Fabricating a Portable ECG Device Using AD823X Analog Front-End Microchips and Open-Source Development Validation. Sensors 2020, 20, 5962. [Google Scholar] [CrossRef]
- Bulić, P.; Kojek, G.; Biasizzo, A. Data Transmission Efficiency in Bluetooth Low Energy Versions. Sensors 2019, 19, 3746. [Google Scholar] [CrossRef] [Green Version]
- Larivière, C.; Delisle, A.; Plamondon, A. Plamondon, The effect of sampling frequency on EMG measures of occupational mechanical exposure. J. Electromyogr. Kinesiol. 2005, 15, 200–209. [Google Scholar] [CrossRef]
- Chu, J.U.; Moon, I.; Mun, M.S. A real-time EMG pattern recognition system based on linear-nonlinear feature projection for a multifunction myoelectric hand. IEEE Trans. Biomed. Eng. 2006, 53, 2232–2239. [Google Scholar]
- Phinyomark, A.; Nuidod, A.; Phukpattaranont, P.; Limsakul, C. Feature Extraction and Reduction of Wavelet Transform Coefficients for EMG Pattern Classification. Electron. Electr. Eng. 2012, 122, 27–32. [Google Scholar] [CrossRef] [Green Version]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xue, F.; Monaghan, A.; Jennings, G.; Byrne, L.; Foran, T.; Duggan, E.; Romero-Ortuno, R. A Novel Methodology for the Synchronous Collection and Multimodal Visualization of Continuous Neurocardiovascular and Neuromuscular Physiological Data in Adults with Long COVID. Sensors 2022, 22, 1758. https://doi.org/10.3390/s22051758
Xue F, Monaghan A, Jennings G, Byrne L, Foran T, Duggan E, Romero-Ortuno R. A Novel Methodology for the Synchronous Collection and Multimodal Visualization of Continuous Neurocardiovascular and Neuromuscular Physiological Data in Adults with Long COVID. Sensors. 2022; 22(5):1758. https://doi.org/10.3390/s22051758
Chicago/Turabian StyleXue, Feng, Ann Monaghan, Glenn Jennings, Lisa Byrne, Tim Foran, Eoin Duggan, and Roman Romero-Ortuno. 2022. "A Novel Methodology for the Synchronous Collection and Multimodal Visualization of Continuous Neurocardiovascular and Neuromuscular Physiological Data in Adults with Long COVID" Sensors 22, no. 5: 1758. https://doi.org/10.3390/s22051758