
Effects of ECG Data Length on Heart Rate Variability among Young Healthy Adults



Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Experimental Protocol
2.3. Data Preprocessing
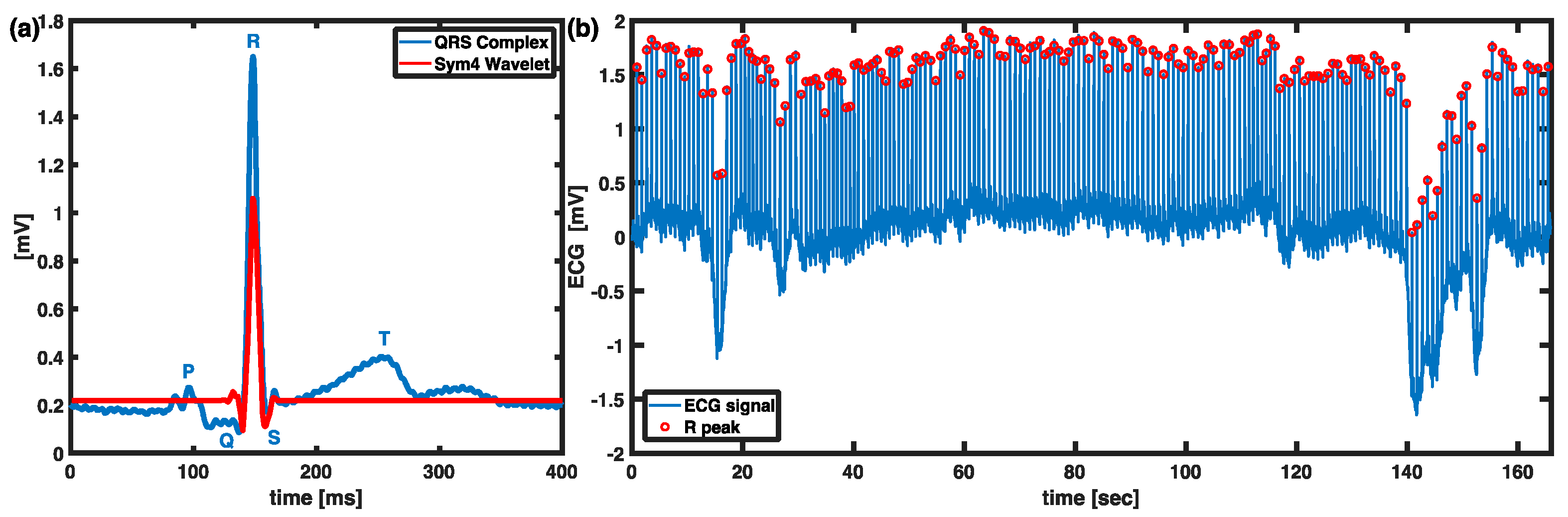
2.4. Extraction of R Peaks Using Wavelet Analysis
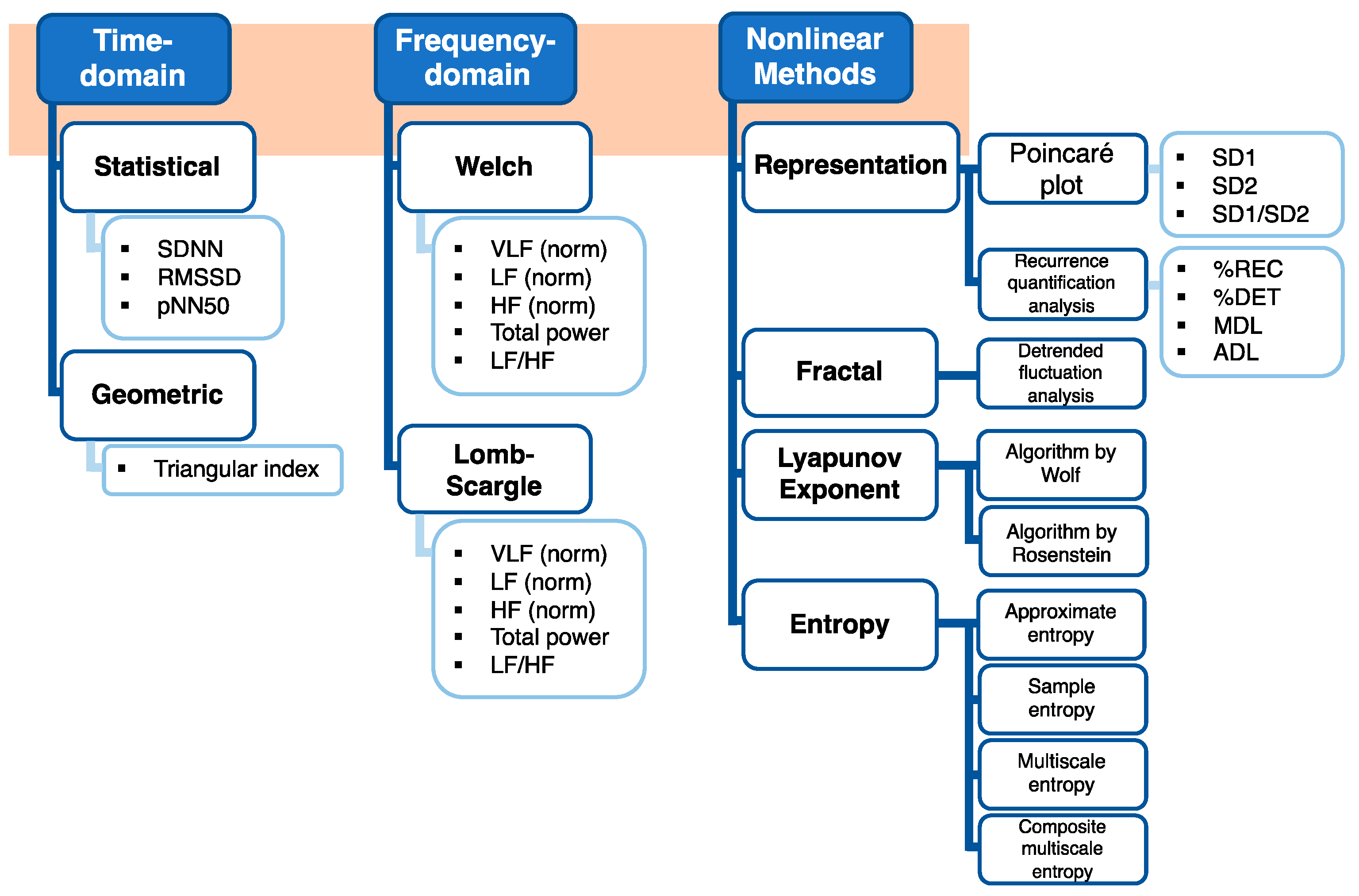
2.5. Time-Domain Analysis
2.6. Frequency-Domain Analysis
2.7. Nonlinear Methods
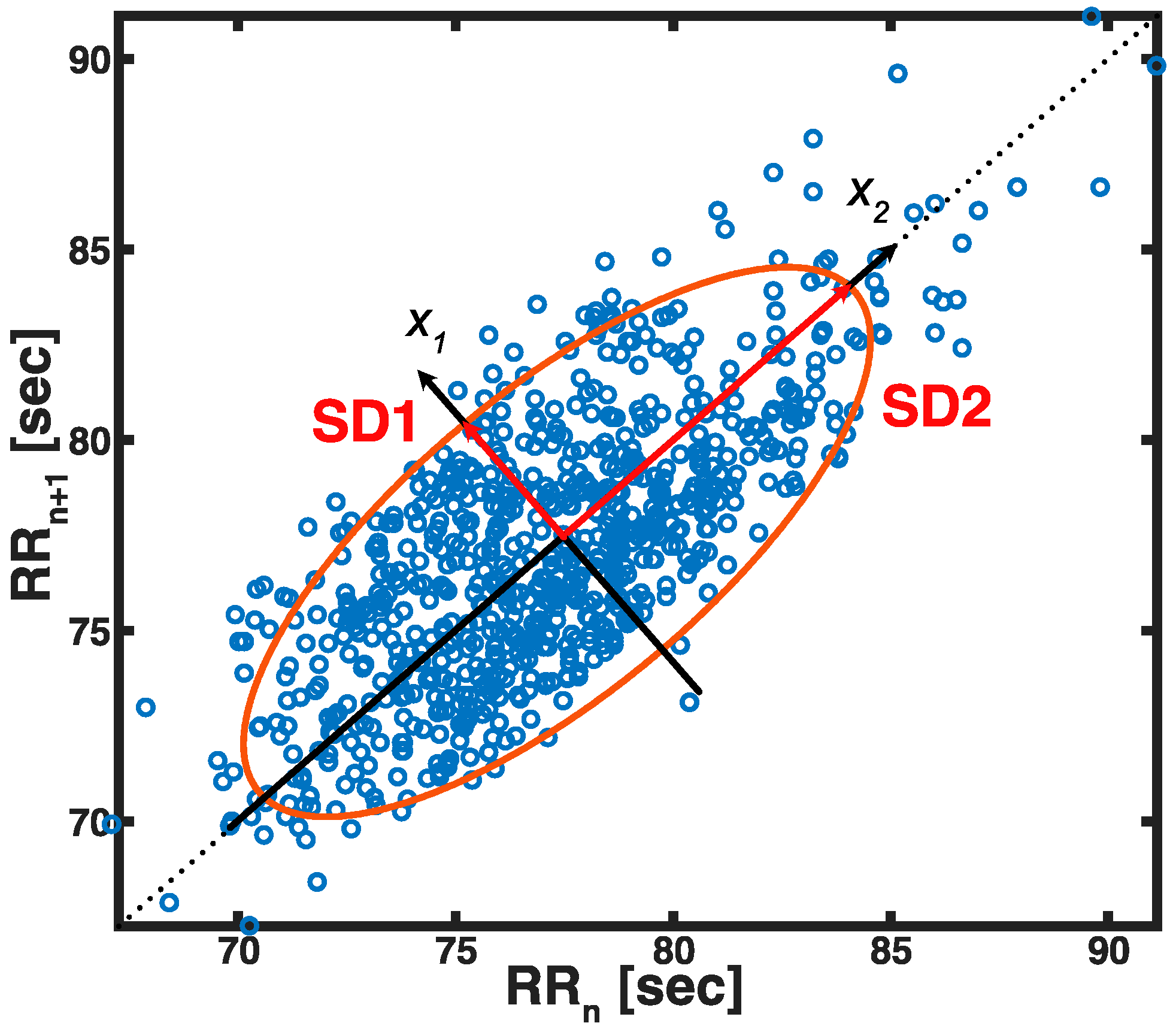
2.7.1. Poincaré Plot
2.7.2. Approximate Entropy
2.7.3. Sample Entropy
2.7.4. Multiscale Entropy
2.7.5. Detrended Fluctuation Analysis
2.7.6. Recurrence Quantification Analysis
2.7.7. Lyapunov Exponent
2.8. Statistical Analysis
3. Results
3.1. Time-Domain HRV
3.2. Frequency-Domain HRV
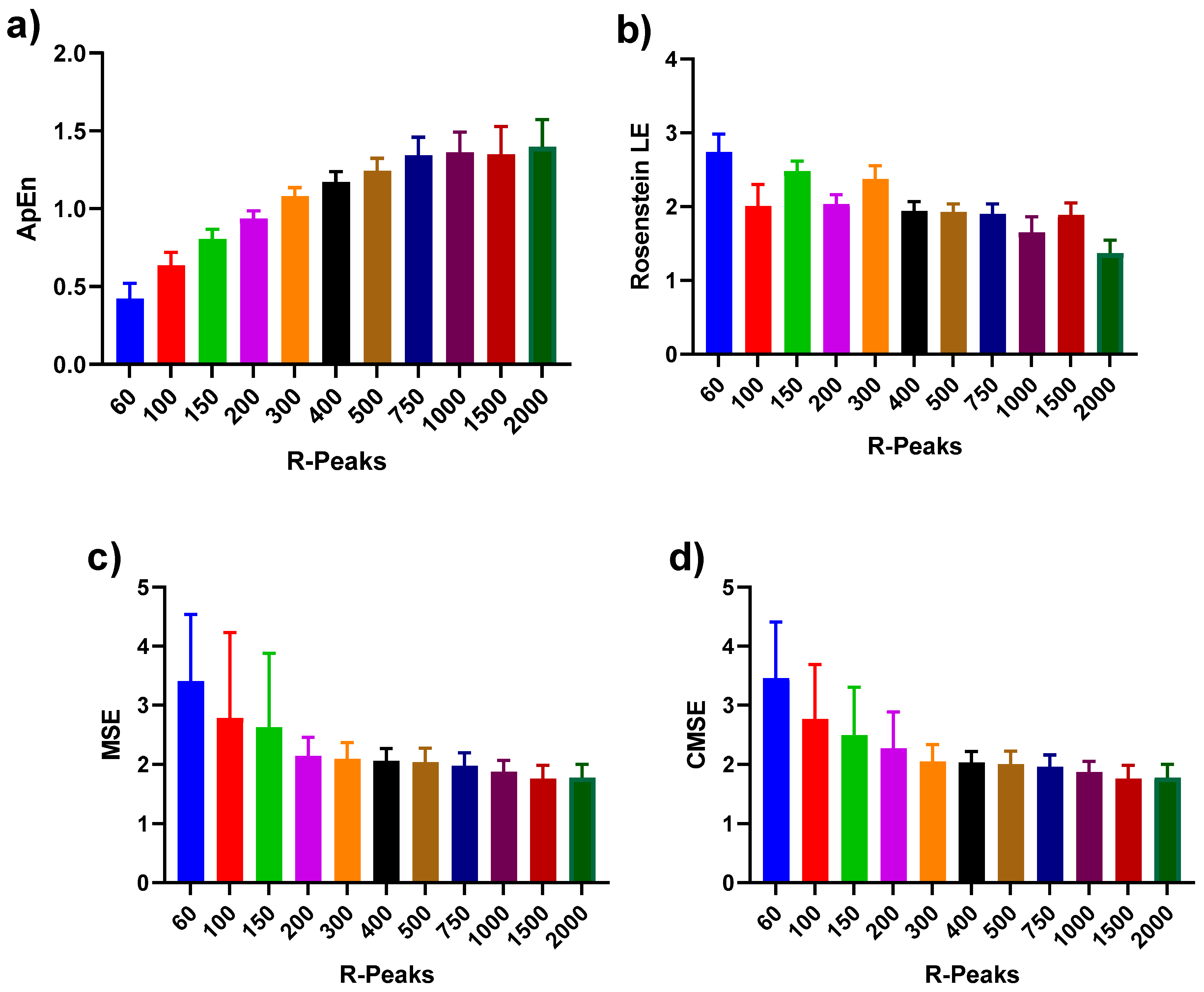
3.3. Nonlinear HRV
4. Discussion
4.1. Use of HRV Measures in Pathology Differentiation
4.2. Importance of Short Data Sets and R-R Intervals
4.3. Linear ECG Variability Measures
4.4. Frequency-Domain Analysis
4.5. Nonlinear Variability Analysis
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malpas, S.C.; Whiteside, E.A.; Maling, T.J. Heart Rate Variability and Cardiac Autonomic Function in Men with Chronic Alcohol Dependence. Heart 1991, 65, 84–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kudat, H.; Akkaya, V.; Sozen, A.; Salman, S.; Demirel, S.; Ozcan, M.; Atilgan, D.; Yilmaz, M.; Guven, O. Heart Rate Variability in Diabetes Patients. J. Int. Med. Res. 2006, 34, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Stein, P.K.; Reddy, A. Non-Linear Heart Rate Variability and Risk Stratification in Cardiovascular Disease. Indian Pacing Electrophysiol. J. 2005, 5, 210–220. [Google Scholar]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The Relationship of Autonomic Imbalance, Heart Rate Variability and Cardiovascular Disease Risk Factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef]
- Sajadieh, A. Increased Heart Rate and Reduced Heart-Rate Variability Are Associated with Subclinical Inflammation in Middle-Aged and Elderly Subjects with No Apparent Heart Disease. Eur. Heart J. 2004, 25, 363–370. [Google Scholar] [CrossRef]
- Lampert, R.; Bremner, J.D.; Su, S.; Miller, A.; Lee, F.; Cheema, F.; Goldberg, J.; Vaccarino, V. Decreased Heart Rate Variability Is Associated with Higher Levels of Inflammation in Middle-Aged Men. Am. Heart J. 2008, 156, 759.e1–759.e7. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.P.; Koenig, J.; Carnevali, L.; Sgoifo, A.; Jarczok, M.N.; Sternberg, E.M.; Thayer, J.F. Heart Rate Variability and Inflammation: A Meta-Analysis of Human Studies. Brain Behav. Immun. 2019, 80, 219–226. [Google Scholar] [CrossRef]
- Zahorska-Markiewicz, B.; Kuagowska, E.; Kucio, C.; Klin, M. Heart Rate Variability in Obesity. Int. J. Obes. Relat. Metab. Disord. 1993, 17, 21–23. [Google Scholar]
- Gorman, J.M.; Sloan, R.P. Heart Rate Variability in Depressive and Anxiety Disorders. Am. Heart J. 2000, 140, S77–S83. [Google Scholar] [CrossRef]
- Chalmers, J.A.; Quintana, D.S.; Abbott, M.J.-A.; Kemp, A.H. Anxiety Disorders Are Associated with Reduced Heart Rate Variability: A Meta-Analysis. Front. Psychiatry 2014, 5, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart Rate Variability: Standards of Measurement, Physiological Interpretation, and Clinical Use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Henriques, T.; Ribeiro, M.; Teixeira, A.; Castro, L.; Antunes, L.; Costa-Santos, C. Nonlinear Methods Most Applied to Heart-Rate Time Series: A Review. Entropy 2020, 22, 309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhea, C.K.; Silver, T.A.; Hong, S.L.; Ryu, J.H.; Studenka, B.E.; Hughes, C.M.L.; Haddad, J.M. Noise and Complexity in Human Postural Control: Interpreting the Different Estimations of Entropy. PLoS ONE 2011, 6, e17696. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Singh, M.; Banga, V.K. Sample Entropy Based HRV: Effect of ECG Sampling Frequency. Biomed. Sci. Eng. 2014, 2, 68–72. [Google Scholar] [CrossRef]
- McCamley, J.; Denton, W.; Arnold, A.; Raffalt, P.; Yentes, J. On the Calculation of Sample Entropy Using Continuous and Discrete Human Gait Data. Entropy 2018, 20, 764. [Google Scholar] [CrossRef] [Green Version]
- Raffalt, P.C.; McCamley, J.; Denton, W.; Yentes, J.M. Sampling Frequency Influences Sample Entropy of Kinematics during Walking. Med. Biol. Eng. Comput. 2019, 57, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Ramdani, S.; Bouchara, F.; Lagarde, J. Influence of Noise on the Sample Entropy Algorithm. Chaos 2009, 19, 013123. [Google Scholar] [CrossRef]
- Casaleggio, A.; Braiotta, S. Estimation of Lyapunov Exponents of ECG Time Series—The Influence of Parameters. Chaos Solitons Fractals 1997, 8, 1591–1599. [Google Scholar] [CrossRef]
- Xinnian, C.; Solomon, I.C.; Chon, K.H. Comparison of the Use of Approximate Entropy and Sample Entropy: Applications to Neural Respiratory Signal. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006; pp. 4212–4215. [Google Scholar]
- Kaffashi, F.; Foglyano, R.; Wilson, C.G.; Loparo, K.A. The Effect of Time Delay on Approximate & Sample Entropy Calculations. Phys. D Nonlinear Phenom. 2008, 237, 3069–3074. [Google Scholar] [CrossRef]
- Singh, B.; Singh, D. Effect of Threshold Value r on Multiscale Entropy Based Heart Rate Variability. Cardiovasc. Eng. Tech. 2012, 3, 211–216. [Google Scholar] [CrossRef]
- Estrada, L.; Torres, A.; Sarlabous, L.; Jané, R. Influence of Parameter Selection in Fixed Sample Entropy of Surface Diaphragm Electromyography for Estimating Respiratory Activity. Entropy 2017, 19, 460. [Google Scholar] [CrossRef]
- Stergious, N. Nonlinear Analysis for Human Movement Variability, 1st ed.; CRC Press: Boca Raton, FL, USA, 2018; ISBN 978-1-315-36237-3. [Google Scholar]
- Yokus, M.A.; Jur, J.S. Fabric-Based Wearable Dry Electrodes for Body Surface Biopotential Recording. IEEE Trans. Biomed. Eng. 2016, 63, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Arquilla, K.; Webb, A.; Anderson, A. Textile Electrocardiogram (ECG) Electrodes for Wearable Health Monitoring. Sensors 2020, 20, 1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crosby, J. Development of a Flexible Printed Paper-Based Battery; Western Michigan University: Kalamazoo, MI, USA, 2020. [Google Scholar]
- Smith, A.-L.; Owen, H.; Reynolds, K.J. Heart Rate Variability Indices for Very Short-Term (30 Beat) Analysis. Part 1: Survey and Toolbox. J. Clin. Monit. Comput. 2013, 27, 569–576. [Google Scholar] [CrossRef]
- Munoz, M.L.; van Roon, A.; Riese, H.; Thio, C.; Oostenbroek, E.; Westrik, I.; de Geus, E.J.C.; Gansevoort, R.; Lefrandt, J.; Nolte, I.M.; et al. Validity of (Ultra-)Short Recordings for Heart Rate Variability Measurements. PLoS ONE 2015, 10, e0138921. [Google Scholar] [CrossRef] [Green Version]
- Thong, T.; Li, K.; McNames, J.; Aboy, M.; Goldstein, B. Accuracy of Ultra-Short Heart Rate Variability Measures. In Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (IEEE Cat. No.03CH37439), Cancun, Mexico, 17–21 September 2003; pp. 2424–2427. [Google Scholar]
- Salahuddin, L.; Cho, J.; Jeong, M.G.; Kim, D. Ultra Short Term Analysis of Heart Rate Variability for Monitoring Mental Stress in Mobile Settings. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; pp. 4656–4659. [Google Scholar]
- Nussinovitch, U.; Elishkevitz, K.P.; Katz, K.; Nussinovitch, M.; Segev, S.; Volovitz, B.; Nussinovitch, N. Reliability of Ultra-Short ECG Indices for Heart Rate Variability: Ultra-Short HRV Reliability. Ann. Noninvasive Electrocardiol. 2011, 16, 117–122. [Google Scholar] [CrossRef]
- Choi, W.-J.; Lee, B.-C.; Jeong, K.-S.; Lee, Y.-J. Minimum Measurement Time Affecting the Reliability of the Heart Rate Variability Analysis. Korean J. Health Promot. 2017, 17, 269. [Google Scholar] [CrossRef] [Green Version]
- Graff, B.; Graff, G.; Kaczkowska, A. Entropy Measures of Heart Rate Variability for Short ECG Datasets in Patients with Congestive Heart Failure. Acta Phys. Pol. B Proc. Suppl. 2012, 5, 153. [Google Scholar] [CrossRef]
- Singh, M.; Singh, B.; Singh, G. Optimal RR-Interval Data Length for Entropy Based Heart Rate Variability Analysis. IJCA 2015, 123, 39–42. [Google Scholar] [CrossRef]
- Lee, D.-Y.; Choi, Y.-S. Multiscale Distribution Entropy Analysis of Short-Term Heart Rate Variability. Entropy 2018, 20, 952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welch, P. The Use of Fast Fourier Transform for the Estimation of Power Spectra: A Method Based on Time Averaging over Short, Modified Periodograms. IEEE Trans. Audio Electroacoust. 1967, 15, 70–73. [Google Scholar] [CrossRef] [Green Version]
- Lomb, N.R. Least-Squares Frequency Analysis of Unequally Spaced Data. Astrophys. Space Sci. 1976, 39, 447–462. [Google Scholar] [CrossRef]
- Estévez, M.; Machado, C.; Leisman, G.; Estévez-Hernández, T.; Arias-Morales, A.; Machado, A.; Montes-Brown, J. Spectral Analysis of Heart Rate Variability. Int. J. Disabil. Hum. Dev. 2016, 15, 5–17. [Google Scholar] [CrossRef] [Green Version]
- Press, W.H.; Flannery, B.P.; Teukolsky, A.A.; Vetterling, W.T. Numerical Recipes in C: The Art of Scientific Computing, 2nd ed.; Cambridge University Press: New York, NY, USA, 1992; ISBN 978-0-521-43108-8. [Google Scholar]
- Moody, G.B. Spectral Analysis of Heart Rate without Resampling. In Proceedings of the Proceedings of Computers in Cardiology Conference, London, UK, 5–8 September 1993; pp. 715–718. [Google Scholar]
- Fonseca, D.S.; Netto, A.D.; Ferreira, R.B.; de Sa, A.M.F.L.M. Lomb-Scargle Periodogram Applied to Heart Rate Variability Study. In Proceedings of the 2013 ISSNIP Biosignals and Biorobotics Conference: Biosignals and Robotics for Better and Safer Living (BRC), Rio de Janerio, Brazil, 18–20 February 2013; pp. 1–4. [Google Scholar]
- Marciano, F.; Migaux, M.L.; Acanfora, D.; Furgi, G.; Rengo, F. Quantification of Poincare’ Maps for the Evaluation of Heart Rate Variability. In Proceedings of the Computers in Cardiology 1994, Bethesda, MD, USA, 25–28 September 1994; pp. 577–580. [Google Scholar]
- Tulppo, M.P.; Makikallio, T.H.; Takala, T.E.; Seppanen, T.; Huikuri, H.V. Quantitative Beat-to-Beat Analysis of Heart Rate Dynamics during Exercise. Am. J. Physiol. Heart Circ. Physiol. 1996, 271, H244–H252. [Google Scholar] [CrossRef] [PubMed]
- D’Addio, G.; Acanfora, D.; Pinna, G.; Maestri, R.; Furgi, G.; Picone, C.; Rengo, F. Reproducibility of Short- and Long-Term Poincare Plot Parameters Compared with Frequency-Domain HRV Indexes in Congestive Heart Failure. In Proceedings of the Computers in Cardiology (Cat. No.98CH36292), Cleveland, OH, USA, 13–16 September 1998; Volume 25, pp. 381–384. [Google Scholar]
- Kamen, P.W.; Krum, H.; Tonkin, A.M. Poincaré Plot of Heart Rate Variability Allows Quantitative Display of Parasympathetic Nervous Activity in Humans. Clin. Sci. 1996, 91, 201–208. [Google Scholar] [CrossRef] [Green Version]
- Brennan, M.; Palaniswami, M.; Kamen, P. New Insights into the Relationship between Poincare Plot Geometry and Linear Measures of Heart Rate Variability. In Proceedings of the 2001 Conference Proceedings of the 23rd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Istanbul, Turkey, 25–28 October 2001; Volume 1, pp. 526–529. [Google Scholar]
- Pincus, S.M. Approximate Entropy as a Measure of System Complexity. Proc. Natl. Acad. Sci. USA 1991, 88, 2297–2301. [Google Scholar] [CrossRef] [Green Version]
- Pincus, S. Approximate Entropy (ApEn) as a Complexity Measure. Chaos 1995, 5, 110–117. [Google Scholar] [CrossRef]
- Eckmann, J.-P.; Ruelle, D. Ergodic theory of chaos and strange attractors. In The Theory of Chaotic Attractors; Hunt, B.R., Li, T.-Y., Kennedy, J.A., Nusse, H.E., Eds.; Springer: New York, NY, USA, 1985; pp. 273–312. ISBN 978-1-4419-2330-1. [Google Scholar]
- Pincus, S.M.; Cummins, T.R.; Haddad, G.G. Heart Rate Control in Normal and Aborted-SIDS Infants. Am. J. Physiol. Regul. Integr. Comp. Physiol. 1993, 264, R638–R646. [Google Scholar] [CrossRef]
- Richman, J.S.; Moorman, J.R. Physiological Time-Series Analysis Using Approximate Entropy and Sample Entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yentes, J.M.; Hunt, N.; Schmid, K.K.; Kaipust, J.P.; McGrath, D.; Stergiou, N. The Appropriate Use of Approximate Entropy and Sample Entropy with Short Data Sets. Ann. Biomed. Eng. 2013, 41, 349–365. [Google Scholar] [CrossRef]
- Montesinos, L.; Castaldo, R.; Pecchia, L. On the Use of Approximate Entropy and Sample Entropy with Centre of Pressure Time-Series. J. NeuroEng. Rehabil. 2018, 15, 116. [Google Scholar] [CrossRef] [Green Version]
- Costa, M.; Goldberger, A.L.; Peng, C.-K. Multiscale Entropy Analysis of Complex Physiologic Time Series. Phys. Rev. Lett. 2002, 89, 068102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, M.; Goldberger, A.L.; Peng, C.-K. Multiscale Entropy Analysis of Biological Signals. Phys. Rev. E 2005, 71, 021906. [Google Scholar] [CrossRef] [Green Version]
- Faes, L.; Porta, A.; Javorka, M.; Nollo, G. Efficient Computation of Multiscale Entropy over Short Biomedical Time Series Based on Linear State-Space Models. Complexity 2017, 2017, 1–13. [Google Scholar] [CrossRef]
- Amoud, H.; Snoussi, H.; Hewson, D.; Doussot, M.; Duchene, J. Intrinsic Mode Entropy for Nonlinear Discriminant Analysis. IEEE Signal Process. Lett. 2007, 14, 297–300. [Google Scholar] [CrossRef]
- Valencia, J.F.; Porta, A.; Vallverdu, M.; Claria, F.; Baranowski, R.; Orlowska-Baranowska, E.; Caminal, P. Refined Multiscale Entropy: Application to 24-h Holter Recordings of Heart Period Variability in Healthy and Aortic Stenosis Subjects. IEEE Trans. Biomed. Eng. 2009, 56, 2202–2213. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-D.; Wu, C.-W.; Lin, S.-G.; Wang, C.-C.; Lee, K.-Y. Time Series Analysis Using Composite Multiscale Entropy. Entropy 2013, 15, 1069–1084. [Google Scholar] [CrossRef] [Green Version]
- Humeau-Heurtier, A. The Multiscale Entropy Algorithm and Its Variants: A Review. Entropy 2015, 17, 3110–3123. [Google Scholar] [CrossRef] [Green Version]
- Peng, C.-K.; Havlin, S.; Stanley, H.E.; Goldberger, A.L. Quantification of Scaling Exponents and Crossover Phenomena in Nonstationary Heartbeat Time Series. Chaos 1995, 5, 82–87. [Google Scholar] [CrossRef]
- Zbilut, J.P.; Webber, C.L. Embeddings and Delays as Derived from Quantification of Recurrence Plots. Phys. Lett. A 1992, 171, 199–203. [Google Scholar] [CrossRef]
- Webber, C.L.; Zbilut, J.P. Dynamical Assessment of Physiological Systems and States Using Recurrence Plot Strategies. J. Appl. Physiol. 1994, 76, 965–973. [Google Scholar] [CrossRef] [PubMed]
- Trulla, L.L.; Giuliani, A.; Zbilut, J.P.; Webber, C.L. Recurrence Quantification Analysis of the Logistic Equation with Transients. Phys. Lett. A 1996, 223, 255–260. [Google Scholar] [CrossRef]
- Eckmann, J.-P.; Oliffson, S.K.; David, R. Recurrence plots of dynamical systems. In World Scientific Series on Nonlinear Science Series A; World Scientific Publishing Company: Singapore, 1995; pp. 441–446. ISBN 1793-1010. [Google Scholar]
- Takens, F. Detecting strange attractors in turbulence. In Dynamical Systems and Turbulence, Warwick 1980; Rand, D., Young, L.-S., Eds.; Lecture Notes in Mathematics; Springer: Berlin/Heidelberg, Germany, 1981; Volume 898, pp. 366–381. ISBN 978-3-540-11171-9. [Google Scholar]
- Gao, J.; Cai, H. On the Structures and Quantification of Recurrence Plots. Phys. Lett. A 2000, 270, 75–87. [Google Scholar] [CrossRef]
- Kennel, M.B.; Brown, R.; Abarbanel, H.D.I. Determining Embedding Dimension for Phase-Space Reconstruction Using a Geometrical Construction. Phys. Rev. A 1992, 45, 3403–3411. [Google Scholar] [CrossRef] [Green Version]
- Marwan, N.; Carmenromano, M.; Thiel, M.; Kurths, J. Recurrence Plots for the Analysis of Complex Systems. Phys. Rep. 2007, 438, 237–329. [Google Scholar] [CrossRef]
- Wallot, S. Recurrence Quantification Analysis of Processes and Products of Discourse: A Tutorial in R. Discourse Process. 2017, 54, 382–405. [Google Scholar] [CrossRef] [Green Version]
- Wolf, A.; Swift, J.B.; Swinney, H.L.; Vastano, J.A. Determining Lyapunov Exponents from a Time Series. Phys. D Nonlinear Phenom. 1985, 16, 285–317. [Google Scholar] [CrossRef] [Green Version]
- Rosenstein, M.T.; Collins, J.J.; De Luca, C.J. A Practical Method for Calculating Largest Lyapunov Exponents from Small Data Sets. Phys. D Nonlinear Phenom. 1993, 65, 117–134. [Google Scholar] [CrossRef]
- Zulli, R.; Nicosia, F.; Borroni, B.; Agosti, C.; Prometti, P.; Donati, P.; Vecchi, M.; Romanelli, G.; Grassi, V.; Padovani, A. QT Dispersion and Heart Rate Variability Abnormalities in Alzheimer’s Disease and in Mild Cognitive Impairment: Cardiovascular abnormalities in alzheimer’s disease and MCI. J. Am. Geriatr. Soc. 2005, 53, 2135–2139. [Google Scholar] [CrossRef]
- Giubilei, F.; Strano, S.; Imbimbo, B.P.; Tisei, P.; Calcagnini, G.; Lino, S.; Frontoni, M.; Santini, M.; Fieschi, C. Cardiac Autonomic Dysfunction in Patients with Alzheimer Disease: Possible Pathogenetic Mechanisms. Alzheimer Dis. Assoc. Disord. 1998, 12, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Ke, J.-Q.; Shao, S.-M.; Zheng, Y.-Y.; Fu, F.-W.; Zheng, G.-Q.; Liu, C.-F. Sympathetic Skin Response and Heart Rate Variability in Predicting Autonomic Disorders in Patients with Parkinson Disease. Medicine 2017, 96, e6523. [Google Scholar] [CrossRef]
- Kallio, M.; Suominen, K.; Bianchi, A.M.; Mäkikallio, T.; Haapaniemi, T.; Astafiev, S.; Sotaniemi, K.A.; Myllylä, V.V.; Tolonen, U. Comparison of Heart Rate Variability Analysis Methods in Patients with Parkinson’s Disease. Med. Biol. Eng. Comput. 2002, 40, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Valappil, R.A.; Black, J.E.; Broderick, M.J.; Carrillo, O.; Frenette, E.; Sullivan, S.S.; Goldman, S.M.; Tanner, C.M.; Langston, J.W. Exploring the Electrocardiogram as a Potential Tool to Screen for Premotor Parkinson’s Disease. Mov. Disord. 2010, 25, 2296–2303. [Google Scholar] [CrossRef]
- Javorka, M.; Trunkvalterova, Z.; Tonhajzerova, I.; Javorkova, J.; Javorka, K.; Baumert, M. Short-Term Heart Rate Complexity Is Reduced in Patients with Type 1 Diabetes Mellitus. Clin. Neurophysiol. 2008, 119, 1071–1081. [Google Scholar] [CrossRef] [PubMed]
- Mussalo, H.; Vanninen, E.; Ikäheimo, R.; Laitinen, T.; Laakso, M.; Länsimies, E.; Hartikainen, J. Heart Rate Variability and Its Determinants in Patients with Severe or Mild Essential Hypertension: HRV and Its Determinants in Severe and Mild Hypertension. Clin. Physiol. 2001, 21, 594–604. [Google Scholar] [CrossRef]
- Kumar, M.S.; Singh, A.; Jaryal, A.K.; Ranjan, P.; Deepak, K.K.; Sharma, S.; Lakshmy, R.; Pandey, R.M.; Vikram, N.K. Cardiovascular Autonomic Dysfunction in Patients of Nonalcoholic Fatty Liver Disease. Int. J. Hepatol. 2016, 2016, 1–8. [Google Scholar] [CrossRef]
- Nguyen Phuc Thu, T.; Hernández, A.I.; Costet, N.; Patural, H.; Pichot, V.; Carrault, G.; Beuchée, A. Improving Methodology in Heart Rate Variability Analysis for the Premature Infants: Impact of the Time Length. PLoS ONE 2019, 14, e0220692. [Google Scholar] [CrossRef] [Green Version]
- McNames, J.; Aboy, M. Reliability and Accuracy of Heart Rate Variability Metrics versus ECG Segment Duration. Med. Biol. Eng. Comput. 2006, 44, 747–756. [Google Scholar] [CrossRef]
- Baek, H.J.; Cho, C.-H.; Cho, J.; Woo, J.-M. Reliability of Ultra-Short-Term Analysis as a Surrogate of Standard 5-Min Analysis of Heart Rate Variability. Telemed. e-Health 2015, 21, 404–414. [Google Scholar] [CrossRef]
- Li, L.; Liu, C.; Liu, C.; Zhang, Q.; Li, B. Physiological Signal Variability Analysis Based on the Largest Lyapunov Exponent. In Proceedings of the 2009 2nd International Conference on Biomedical Engineering and Informatics, Tianjin, China, 17–19 October 2009; pp. 1–5. [Google Scholar]
- Signorini, M.G.; Cerutti, S. Lyapunov Exponents Calculated from Heart Rate Variability Time Series. In Proceedings of the 16th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Baltimore, MD, USA, 3–6 November 1994; pp. 119–120. [Google Scholar]
- Lin, G.-H.; Chang, Y.-H.; Lin, K.-P. Comparison of Heart Rate Variability Measured by ECG in Different Signal Lengths. J. Med. Biol. Eng. 2005, 25, 67–71. [Google Scholar]
- Mayya, S.; Jilla, V.; Tiwari, V.N.; Nayak, M.M.; Narayanan, R. Continuous Monitoring of Stress on Smartphone Using Heart Rate Variability. In Proceedings of the 2015 IEEE 15th International Conference on Bioinformatics and Bioengineering (BIBE), Belgrade, Serbia, 2–4 November 2015; pp. 1–5. [Google Scholar]
- Pereira, T.; Almeida, P.R.; Cunha, J.P.S.; Aguiar, A. Heart Rate Variability Metrics for Fine-Grained Stress Level Assessment. Comput. Methods Programs Biomed. 2017, 148, 71–80. [Google Scholar] [CrossRef]
- Gao, J.B.; Hu, J.; Tung, W.W.; Cao, Y.H. Distinguishing Chaos from Noise by Scale-Dependent Lyapunov Exponent. Phys. Rev. E 2006, 74, 066204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, J.; Cao, Y.; Tung, W.-W.; Hu, J. Multiscale Analysis of Complex Time Series: Integration of Chaos and Random Fractal Theory, and Beyong; John Wiley & Sons: Hoboken, NJ, USA, 2007; ISBN 978-0-471-65470-4. [Google Scholar]
- Hu, J.; Gao, J.; Tung, W. Characterizing Heart Rate Variability by Scale-Dependent Lyapunov Exponent. Chaos 2009, 19, 028506. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Length (R Peaks) | Time Delay | Embedding Dimension |
|---|---|---|
| 60 | 2 | 2 |
| 100 | 3 | 2 |
| 150 | 2 | 3 |
| 200 | 3 | 3 |
| 300 | 2 | 3 |
| 400 | 3 | 4 |
| 500 | 3 | 4 |
| 750 | 3 | 4 |
| 1000 | 4 | 4 |
| 1500 | 3 | 4 |
| 2000 | 5 | 5 |
| Length | 60 | 100 | 150 | 200 | 300 | 400 | 500 | 750 | 1000 | 1500 |
|---|---|---|---|---|---|---|---|---|---|---|
| Time-domain HRV | ||||||||||
| Geometric measure | ||||||||||
| Triangular index | 0.000 | 0.002 | 0.004 | 0.004 | 0.005 | 0.008 | 0.017 | 0.048 | 0.148 | 0.800 |
| Statistical measure | ||||||||||
| SDNN | 0.016 | 0.056 | 0.056 | 0.069 | 0.056 | 0.062 | 0.104 | 0.094 | 0.265 | 0.946 |
| RMSSD | 0.982 | 0.804 | 0.667 | 0.734 | 0.734 | 0.701 | 0.701 | 0.635 | 0.769 | 1.000 |
| pNN50 | 0.946 | 0.909 | 0.730 | 0.872 | 0.836 | 0.765 | 0.909 | 0.836 | 0.909 | 0.982 |
| Frequency-domain HRV | ||||||||||
| Welch’s periodogram | ||||||||||
| VLF | 0.000 | 0.002 | 0.002 | 0.002 | 0.001 | 0.003 | 0.006 | 0.009 | 0.104 | 0.734 |
| LF | 0.035 | 0.050 | 0.104 | 0.056 | 0.044 | 0.048 | 0.044 | 0.044 | 0.210 | 0.839 |
| HF | 0.603 | 0.804 | 0.910 | 0.839 | 0.874 | 0.910 | 0.874 | 0.946 | 0.982 | 0.982 |
| Total power | 0.016 | 0.039 | 0.050 | 0.050 | 0.044 | 0.035 | 0.057 | 0.050 | 0.210 | 0.910 |
| VLF norm | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.001 | 0.005 | 0.009 | 0.103 | 0.646 |
| LF norm | 0.946 | 0.701 | 0.734 | 0.927 | 0.804 | 0.769 | 0.748 | 0.946 | 0.734 | 0.890 |
| HF norm | 0.008 | 0.003 | 0.008 | 0.014 | 0.019 | 0.024 | 0.044 | 0.085 | 0.137 | 0.734 |
| LF/HF | 0.137 | 0.062 | 0.085 | 0.062 | 0.069 | 0.085 | 0.113 | 0.183 | 0.306 | 0.839 |
| Lomb–Scargle’s periodogram | ||||||||||
| VLF | 0.945 | 0.121 | 0.188 | 0.105 | 0.256 | 0.306 | 0.418 | 1.000 | 0.069 | 0.728 |
| LF | 0.000 | 0.000 | 0.006 | 0.004 | 0.013 | 0.050 | 0.188 | 0.188 | 0.798 | 0.694 |
| HF | 0.000 | 0.000 | 0.001 | 0.001 | 0.003 | 0.011 | 0.030 | 0.112 | 0.982 | 0.963 |
| Total power | 0.000 | 0.000 | 0.001 | 0.000 | 0.001 | 0.013 | 0.073 | 0.140 | 0.645 | 0.890 |
| VLF norm | 0.000 | 0.000 | 0.000 | 0.002 | 0.002 | 0.010 | 0.056 | 0.040 | 0.358 | 0.804 |
| LF norm | 0.137 | 0.435 | 0.839 | 0.807 | 1.000 | 0.982 | 0.910 | 0.769 | 0.890 | 0.982 |
| HF norm | 0.027 | 0.077 | 0.048 | 0.062 | 0.081 | 0.094 | 0.178 | 0.198 | 0.511 | 0.818 |
| LF/HF | 0.839 | 0.541 | 0.482 | 0.511 | 0.520 | 0.401 | 0.520 | 0.804 | 0.734 | 0.982 |
| Nonlinear HRV | ||||||||||
| Poincaré plot | ||||||||||
| SD1 | 0.667 | 1.000 | 0.890 | 0.963 | 0.908 | 0.874 | 0.910 | 0.769 | 0.854 | 0.910 |
| SD2 | 0.009 | 0.031 | 0.021 | 0.027 | 0.014 | 0.014 | 0.031 | 0.044 | 0.198 | 0.910 |
| SD1/SD2 | 0.004 | 0.002 | 0.008 | 0.011 | 0.009 | 0.014 | 0.039 | 0.085 | 0.150 | 0.667 |
| Entropy | ||||||||||
| SampEn | 0.046 | 0.009 | 0.006 | 0.007 | 0.035 | 0.021 | 0.031 | 0.077 | 0.329 | 0.734 |
| ApEn | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.011 | 0.541 | 0.701 | 0.511 |
| MSE | 0.005 | 0.125 | 0.012 | 0.003 | 0.002 | 0.003 | 0.007 | 0.035 | 0.164 | 0.839 |
| CMSE | 0.000 | 0.002 | 0.007 | 0.002 | 0.009 | 0.004 | 0.009 | 0.062 | 0.164 | 0.839 |
| Fractal | ||||||||||
| DFA | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.002 | 0.000 | 0.002 | 0.667 |
| Lyapunov exponent | ||||||||||
| Wolf | 0.000 | 0.000 | 0.000 | 0.035 | 0.000 | 0.001 | 0.069 | 0.085 | 0.002 | 0.701 |
| Rosenstein | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.002 | 0.000 |
| Length (s) | 60 | 100 | 150 | 200 | 300 | 400 | 500 | 600 |
|---|---|---|---|---|---|---|---|---|
| %REC | 0.910 | 0.910 | 1.000 | 0.946 | 1.000 | 0.874 | 0.946 | 0.982 |
| %DET | 1.000 | 0.982 | 0.946 | 1.000 | 1.000 | 0.946 | 1.000 | 0.946 |
| MDL | 0.982 | 0.769 | 0.839 | 0.982 | 0.804 | 1.000 | 1.000 | 0.982 |
| ADL | 0.701 | 0.910 | 0.982 | 0.982 | 0.946 | 0.946 | 0.982 | 0.946 |
| HRV Parameters | Recommended Minimum Data Length (R Peaks) |
|---|---|
| Time-domain HRV | |
| Geometric measure | |
| Triangular index | 1000 |
| Statistical measure | |
| SDNN | 100 |
| RMSSD | 60 |
| pNN50 | 60 |
| Frequency-domain HRV | |
| Welch’s periodogram | |
| VLF | 1000 |
| LF | 1000 |
| HF | 60 |
| Total power | 1000 |
| VLF norm | 1000 |
| LF norm | 60 |
| HF norm | 750 |
| LF/HF | 60 |
| Lomb–Scargle’s periodogram | |
| VLF | 60 |
| LF | 500 |
| HF | 1000 |
| Total power | 500 |
| VLF norm | 1000 |
| LF norm | 60 |
| HF norm | 500 |
| LF/HF | 60 |
| Nonlinear HRV | |
| Poincaré plot | |
| SD1 | 60 |
| SD2 | 1000 |
| SD1/SD2 | 1000 |
| Entropy | |
| SampEn | 1000 |
| ApEn | 1000 |
| MSE | 1000 |
| CMSE | 1000 |
| Fractal | |
| DFA | 1500 |
| Lyapunov exponent | |
| Wolf | 1500 |
| Rosenstein | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, E.-F.; Khine, M.; Lockhart, T.; Soangra, R. Effects of ECG Data Length on Heart Rate Variability among Young Healthy Adults. Sensors 2021, 21, 6286. https://doi.org/10.3390/s21186286
Chou E-F, Khine M, Lockhart T, Soangra R. Effects of ECG Data Length on Heart Rate Variability among Young Healthy Adults. Sensors. 2021; 21(18):6286. https://doi.org/10.3390/s21186286
Chicago/Turabian StyleChou, En-Fan, Michelle Khine, Thurmon Lockhart, and Rahul Soangra. 2021. "Effects of ECG Data Length on Heart Rate Variability among Young Healthy Adults" Sensors 21, no. 18: 6286. https://doi.org/10.3390/s21186286