
Test-Retest Reliability of Acoustic Emission Sensing of the Knee during Physical Tasks

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Protocol
2.2. Data Processing
2.3. Statistical Analysis
3. Results
3.1. Inter-Day Test-Retest Reliability
3.2. Intrasession Reliability
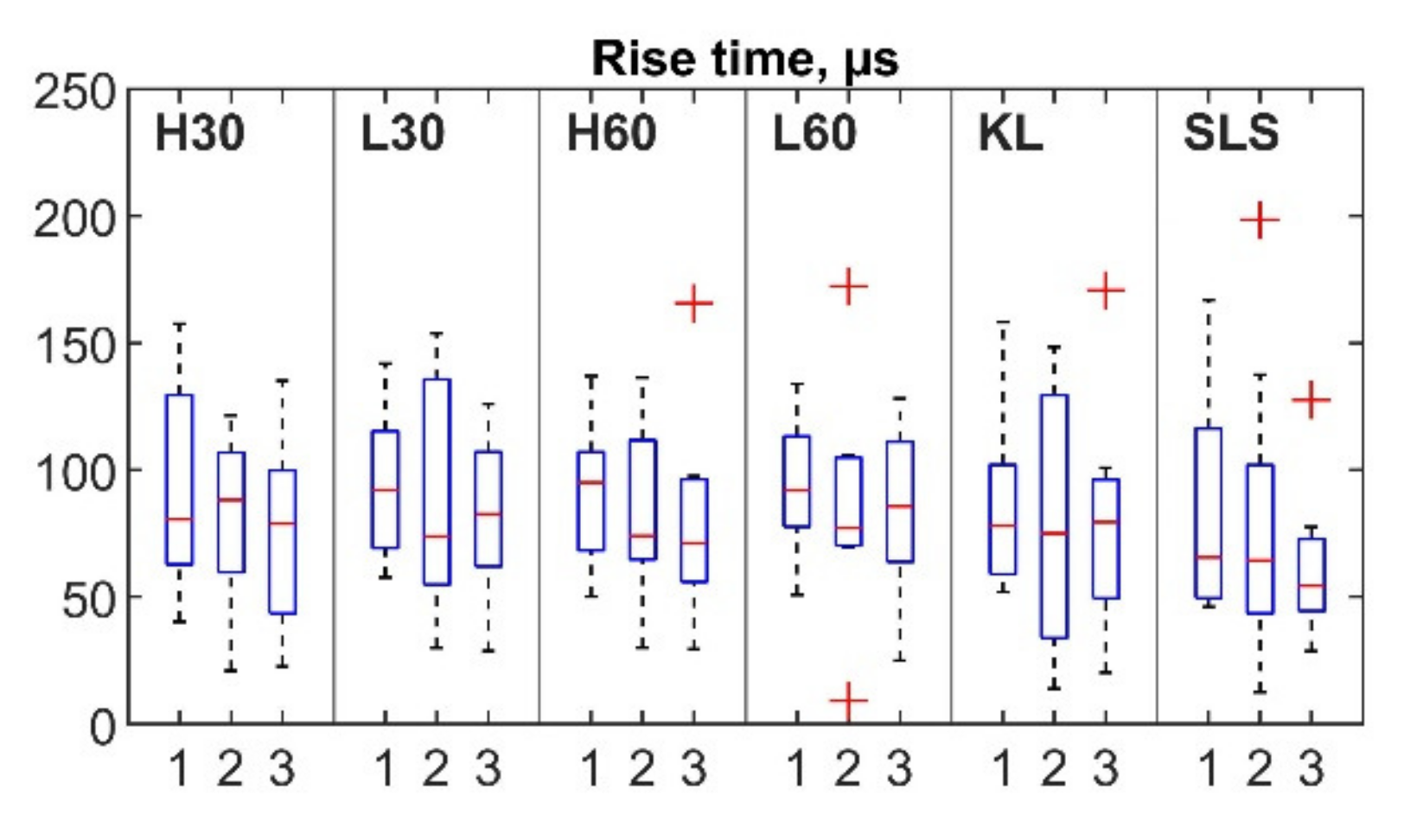
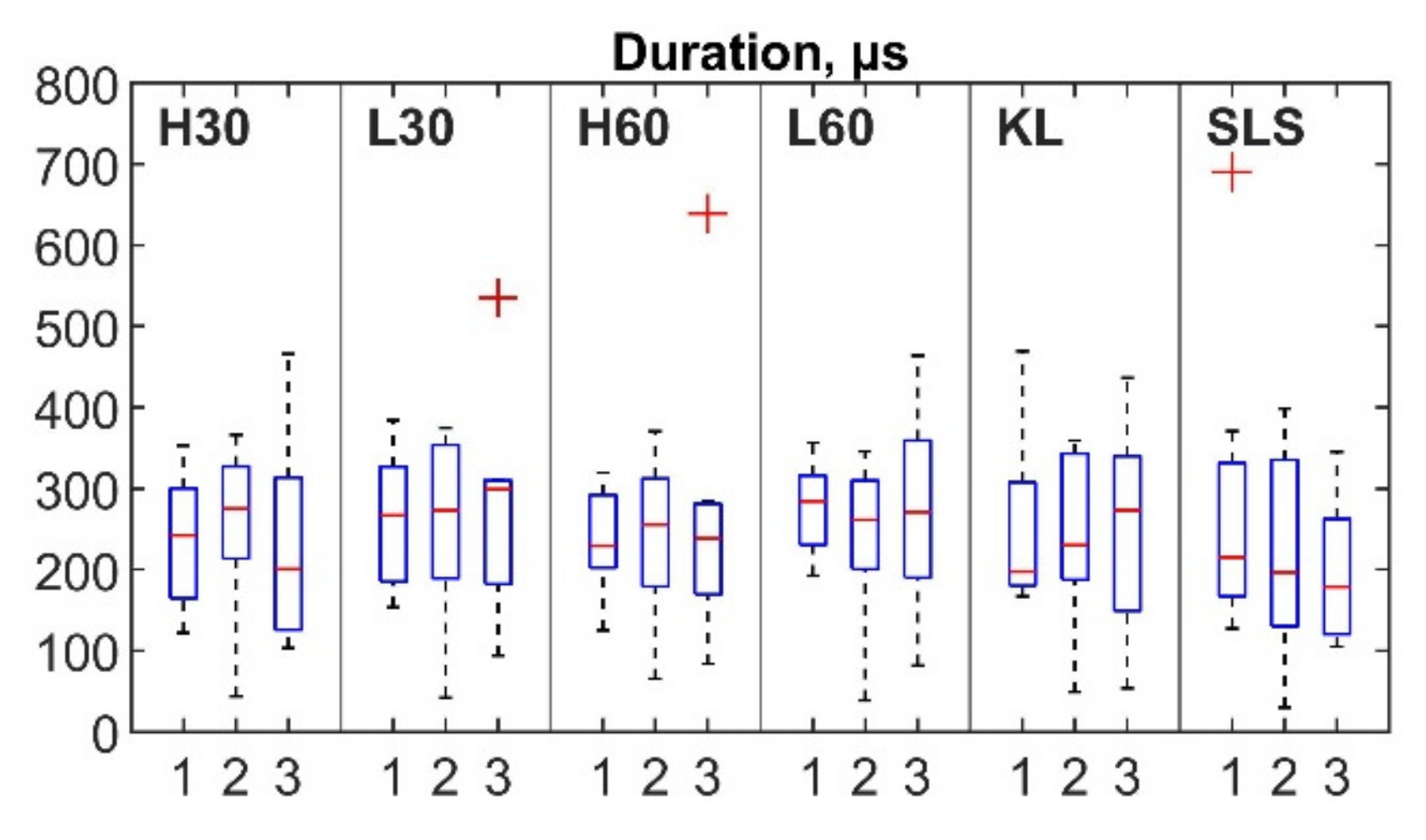
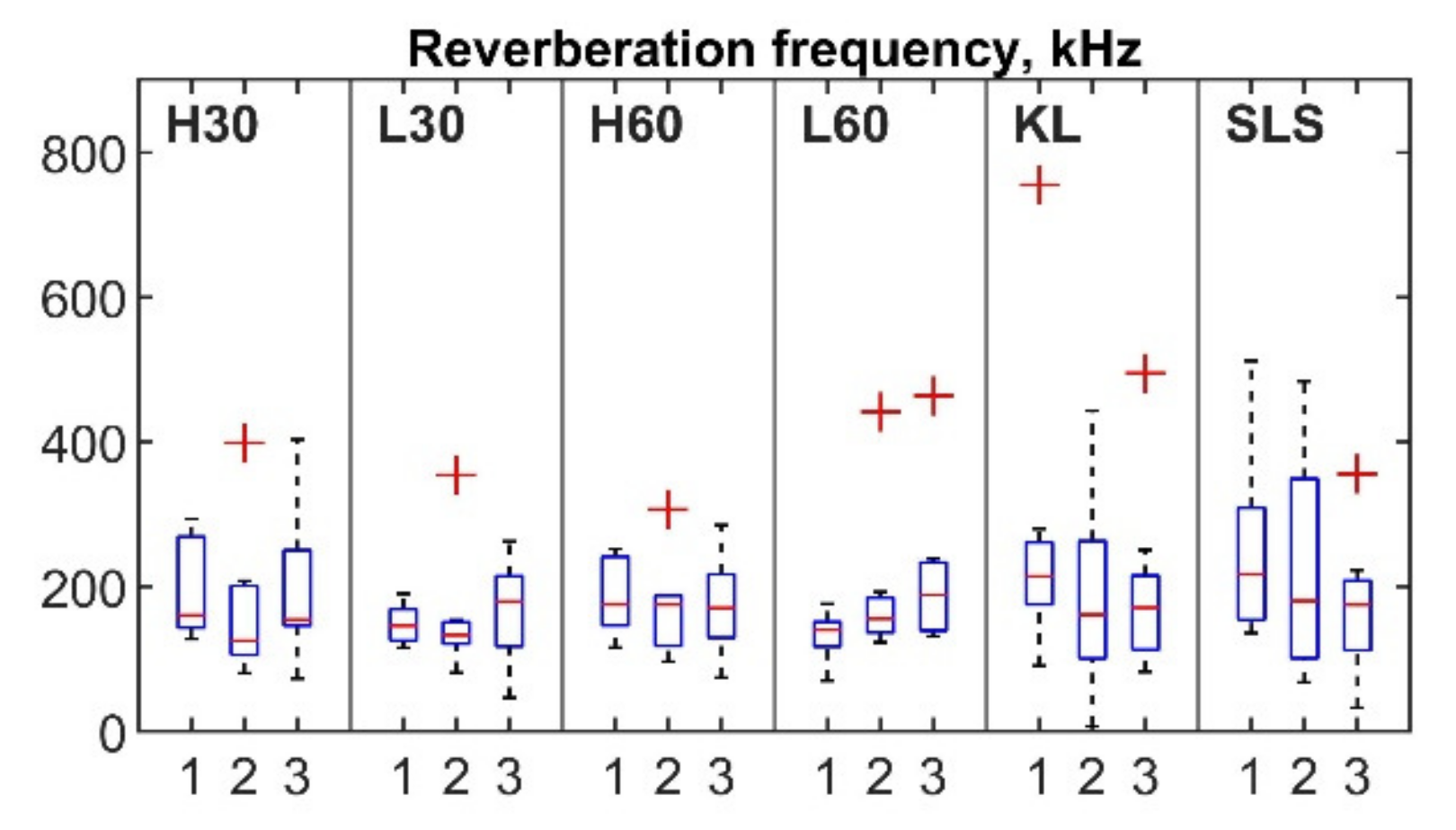
3.3. AE Events Parameters
4. Discussion
4.1. Reliability of Knee AE Monitoring
4.2. Limitations of the Present Study and Future Work
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exercise 1 | ICC | LOWER Bound (95% CI) | Upper Bound (95% CI) | CV1 | CV2 | CV3 |
|---|---|---|---|---|---|---|
| Counts: mean value | ||||||
| L30 | 0.383 | 0 | 0.867 | 0.342 | 0.333 | 0.715 |
| H30 | 0.752 | 0.167 | 0.946 | 0.378 | 0.576 | 0.679 |
| L60 | 0.532 | 0 | 0.897 | 0.239 | 0.675 | 0.838 |
| H60 | 0.581 | 0 | 0.910 | 0.313 | 0.527 | 0.969 |
| KL | 0 | 0 | 0.326 | 0.615 | 0.410 | 0.454 |
| SLS | 0.474 | 0 | 0.884 | 0.828 | 0.550 | 0.563 |
| Amplitude (dB): mean value | ||||||
| L30 | 0.309 | 0 | 0.860 | 0.024 | 0.034 | 0.060 |
| H30 | 0.783 | 0.213 | 0.954 | 0.028 | 0.037 | 0.029 |
| L60 | 0.128 | 0 | 0.826 | 0.015 | 0.023 | 0.058 |
| H60 | 0.256 | 0 | 0.846 | 0.022 | 0.031 | 0.072 |
| KL | 0 | 0 | 0.608 | 0.046 | 0.036 | 0.040 |
| SLS | 0.532 | 0 | 0.899 | 0.127 | 0.051 | 0.070 |
| Counts to peak: mean value | ||||||
| L30 | 0.495 | 0 | 0.892 | 0.301 | 0.409 | 0.604 |
| H30 | 0 | 0 | 0.657 | 0.380 | 0.386 | 0.557 |
| L60 | 0.532 | 0 | 0.897 | 0.215 | 0.685 | 0.777 |
| H60 | 0.656 | 0 | 0.926 | 0.290 | 0.432 | 0.827 |
| KL | 0 | 0 | 0 | 0.543 | 0.413 | 0.487 |
| SLS | 0.323 | 0 | 0.855 | 0.532 | 0.458 | 0.381 |
| Signal Strength (pV-s): mean value | ||||||
| L30 | 0.770 | 0.191 | 0.951 | 0.403 | 0.506 | 0.580 |
| H30 | 0 | 0 | 0.762 | 0.337 | 0.450 | 0.608 |
| L60 | 0.684 | 0 | 0.933 | 0.273 | 0.488 | 0.529 |
| H60 | 0.539 | 0 | 0.904 | 0.301 | 0.456 | 1.020 |
| KL | 0 | 0 | 0.613 | 0.556 | 0.501 | 0.727 |
| SLS | 0.084 | 0 | 0.799 | 2.370 | 0.735 | 0.486 |
| Absolute Energy (attoJoules): mean value | ||||||
| L30 | 0.741 | 0.165 | 0.943 | 1.747 | 0.640 | 1.227 |
| H30 | 0.734 | 0.158 | 0.941 | 0.349 | 0.803 | 2.560 |
| L60 | 0 | 0 | 0.528 | 0.798 | 0.745 | 0.626 |
| H60 | 0.409 | 0 | 0.875 | 1.173 | 1.009 | 1.438 |
| KL | 0 | 0 | 0.570 | 1.281 | 0.659 | 1.276 |
| SLS | 0.001 | 0 | 0.781 | 2.722 | 0.944 | 0.575 |
| Average Frequency (kHz): mean value | ||||||
| L30 | 0.555 | 0 | 0.907 | 0.179 | 0.781 | 0.426 |
| H30 | 0.720 | 0.112 | 0.938 | 0.319 | 0.691 | 0.522 |
| L60 | 0.674 | 0.024 | 0.926 | 0.216 | 0.693 | 0.575 |
| H60 | 0.766 | 0.152 | 0.950 | 0.277 | 0.463 | 0.426 |
| KL | 0.036 | 0 | 0.798 | 0.940 | 0.844 | 0.913 |
| SLS | 0 | 0 | 0.694 | 0.606 | 0.659 | 0.728 |
References
- Murphy, L.; Schwartz, T.A.; Helmick, C.G.; Renner, J.B.; Tudor, G.; Koch, G.; Dragomir, A.; Kalsbeek, W.D.; Luta, G.; Jordan, J.M. Lifetime risk of symptomatic knee osteoarthritis. Arthritis Care Res. Off. J. Am. Coll. Rheumatol. 2008, 59, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- Culliford, D.J.; Maskell, J.; Kiran, A.; Judge, A.; Javaid, M.K.; Cooper, C.; Arden, N.K. The lifetime risk of total hip and knee arthroplasty: Results from the UK general practice research database. Osteoarthr. Cartil. 2012, 20, 519–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulkarni, K.; Karssiens, T.; Kumar, V.; Pandit, H. Obesity and osteoarthritis. Maturitas 2016, 89, 22–28. [Google Scholar] [CrossRef]
- Kremers, H.M.; Larson, D.R.; Crowson, C.S.; Kremers, W.K.; Washington, R.E.; Steiner, C.A.; Jiranek, W.A.; Berry, D.J. Prevalence of total hip and knee replacement in the United States. J. Bone Jt. Surg.-Am. Vol. 2014, 97, 1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, J.A.; Yu, S.; Chen, L.; Cleveland, J.D. Rates of total joint replacement in the United States: Future projections to 2020-2040 using the national inpatient sample. J. Rheumatol. 2019, 46, 1134–1140. [Google Scholar] [CrossRef]
- Price, A.J.; Alvand, A.; Troelsen, A.; Katz, J.N.; Hooper, G.; Gray, A.; Carr, A.; Beard, D. Knee replacement. Lancet 2018, 392, 1672–1682. [Google Scholar] [CrossRef]
- Zhang, H.; Zhou, Y. Concept verification of a Remote Automatic Scoring System for Evaluating Knee Function after Total Knee Arthroplasty. J. Knee Surg. 2020, 34, 464–470. [Google Scholar] [CrossRef]
- Ramkumar, P.N.; Haeberle, H.S.; Ramanathan, D.; Cantrell, W.A.; Navarro, S.M.; Mont, M.A.; Bloomfield, M.; Patterson, B.M. Remote Patient Monitoring Using Mobile Health for Total Knee Arthroplasty: Validation of a Wearable and Machine Learning–Based Surveillance Platform. J. Arthroplast. 2019, 34, 2253–2259. [Google Scholar] [CrossRef]
- Guk, K.; Han, G.; Lim, J.; Jeong, K.; Kang, T.; Lim, E.-K.; Jung, J. Evolution of Wearable Devices with Real-Time Disease Monitoring for Personalized Healthcare. Nanomaterials 2019, 9, 813. [Google Scholar] [CrossRef] [Green Version]
- Khokhlova, L.; Komaris, D.S.; Tedesco, S.; O’Flynn, B. Assessment of hip and knee joints and implants using acoustic emission monitoring: A scoping review. IEEE Sens. J. 2020, 21, 14379–14388. [Google Scholar] [CrossRef]
- PAC. PCI-2 Based AE System User’s Manual Rev 3 Associated with: AEWIN for PCI-2 Software Part #: 6301-7001 Version 1.30 or Higher; Physical Acoustics Corporation: Princeton Junction, NJ, USA, 2007. [Google Scholar]
- Wells, J.G.; Rawlings, R.D. Acoustic emission and mechanical properties of trabecular bone. Biomaterials 1985, 6, 218–224. [Google Scholar] [CrossRef]
- Browne, M.; Barrett, D.; Balabanis, A.; Rowland, C. Passive monitoring of knee joint condition using acoustic emission. In Orthopaedic Proceedings; The British Editorial Society of Bone & Joint Surgery: London, UK, 2016; Volume 98, p. 54. [Google Scholar]
- Khan, T.I.; Yoho, H. Integrity analysis of knee joint by acoustic emission technique. J. Multimodal User Interfaces 2016, 10, 319–324. [Google Scholar] [CrossRef]
- Spain, L.; Rajoub, B.; Schlüter, D.; Waterton, J.; Bowes, M.; Shark, L.-K.; Diggle, P.; Goodacre, J. Biomarkers for knee osteoarthritis: New technologies, new paradigms. Int. J. Clin. Rheumtol. 2015, 10, 287–297. [Google Scholar] [CrossRef] [Green Version]
- Wierzcholski, K. Acoustic emission diagnosis for human joint cartilage diseases. Acta Bioeng. Biomech./Wrocław Univ. Technol. 2015, 17, 139–148. [Google Scholar]
- Schluter, D.K.; Spain, L.; Quan, W.; Southworth, H.; Platt, N.; Mercer, J.; Shark, L.-K.; Waterton, J.C.; Bowes, M.; Diggle, P.J.; et al. Use of acoustic emission to identify novel candidate biomarkers for knee osteoarthritis (OA). PLoS ONE 2019, 14, e0223711. [Google Scholar] [CrossRef] [Green Version]
- Hersek, S.; Pouyan, M.B.; Teague, C.N.; Sawka, M.N.; Millard-Stafford, M.L.; Kogler, G.F.; Wolkoff, P.; Inan, O.T. Acoustical Emission Analysis by Unsupervised Graph Mining: A Novel Biomarker of Knee Health Status. IEEE Trans. Biomed. Eng. 2018, 65, 1291–1300. [Google Scholar] [CrossRef]
- Whittingslow, D.C.; Jeong, H.-K.K.; Ganti, V.G.; Kirkpatrick, N.J.; Kogler, G.F.; Inan, O.T. Acoustic Emissions as a Non-invasive Biomarker of the Structural Health of the Knee. Ann. Biomed. Eng. 2020, 48, 225–235. [Google Scholar] [CrossRef]
- Unnþórsson, R. Hit Detection and Determination in AE Bursts; InTech: London, UK, 2013. [Google Scholar] [CrossRef] [Green Version]
- Kalo, K.; Niederer, D.; Sus, R.; Sohrabi, K.; Gross, V.; Vogt, L. Reliability of Vibroarthrography to Assess Knee Joint Sounds in Motion. Sensors 2020, 20, 1998. [Google Scholar] [CrossRef] [Green Version]
- Hochman, D.M.; Gharehbaghi, S.; Whittingslow, D.C.; Inan, O.T. A Pilot Study to Assess the Reliability of Sensing Joint Acoustic Emissions of the Wrist. Sensors 2020, 20, 4240. [Google Scholar] [CrossRef]
- Kottner, J.; Audigé, L.; Brorson, S.; Donner, A.; Gajewski, B.J.; Hróbjartsson, A.; Roberts, C.; Shoukri, M.; Streiner, D.L. Guidelines for Reporting Reliability and Agreement Studies (GRRAS) were proposed. J. Clin. Epidemiol. 2011, 64, 96–106. [Google Scholar] [CrossRef]
- Walter, S.D.; Eliasziw, M.; Donner, A. Sample size and optimal designs for reliability studies. Stat. Med. 1998, 17, 101–110. [Google Scholar] [CrossRef]
- PK15I-150 kHz AE Sensor with Low-Power Integral Preamp, by Physical Acoustics. Available online: https://www.physicalacoustics.com/by-product/sensors/PK15I-150-kHz-AE-Sensor-with-Low-Power-Integral-Preamp (accessed on 6 April 2021).
- Nano30-Miniature Acoustic Emission Sensor with Integral Coaxial Cable, by Physical Acoustics. Available online: https://www.physicalacoustics.com/by-product/nano30-150-750-khz-miniature-ae-sensor-with-integral-coaxial-cable/ (accessed on 2 September 2022).
- Khokhlova, L.; Komaris, D.S.; Tedesco, S.; O’Flynn, B. Motion Artifact Resistant Mounting of Acoustic Emission Sensors for Knee Joint Monitoring. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 1–5 November 2021; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2021; pp. 7300–7303. [Google Scholar] [CrossRef]
- Shark, L.-K.; Chen, H.; Goodacre, J. Discovering differences in acoustic emission between healthy and osteoarthritic knees using a four-phase model of sit-stand-sit movements. Open Med. Inform. J. 2010, 4, 116–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luan, L.; Bousie, J.; Pranata, A.; Adams, R.; Han, J. Stationary cycling exercise for knee osteoarthritis: A systematic review and meta-analysis. Clin. Rehabil. 2021, 35, 522–533. [Google Scholar] [CrossRef] [PubMed]
- Mistry, J.B.; Elmallah, R.D.K.; Bhave, A.; Chughtai, M.; Cherian, J.J.; McGinn, T.; Harwin, S.F.; Mont, M.A. Rehabilitative Guidelines after Total Knee Arthroplasty: A Review. J. Knee Surg. 2016, 29, 201–217. [Google Scholar] [CrossRef] [PubMed]
- NHS The Royal Orthopaedic Hospital Exercises for Osteoarthritis of the Knee Your Rehabilitation Programme. Available online: www.roh.nhs.uk (accessed on 4 November 2022).
- Teague, C.N.; Hersek, S.; Toreyin, H.; Millard-Stafford, M.L.; Jones, M.L.; Kogler, G.F.; Sawka, M.N.; Inan, O.T. Novel methods for sensing acoustical emissions from the knee for wearable joint health assessment. IEEE Trans. Biomed. Eng. 2016, 63, 1581–1590. [Google Scholar] [CrossRef] [PubMed]
- USB Node DLL DRIVER & LabVIEW VI’ s Software User’ s Manual; Physical Acoustics Corporation: Princeton Junction, NJ, USA, 2016.
- Qin, S.; Nelson, L.; McLeod, L.; Eremenco, S.; Coons, S.J. Assessing test–retest reliability of patient-reported outcome measures using intraclass correlation coefficients: Recommendations for selecting and documenting the analytical formula. Qual. Life Res. 2019, 28, 1029–1033. [Google Scholar] [CrossRef] [Green Version]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155. [Google Scholar] [CrossRef] [Green Version]
- Liljequist, D.; Elfving, B.; Roaldsen, K.S. Intraclass correlation–A discussion and demonstration of basic features. PLoS ONE 2019, 14, e0219854. [Google Scholar] [CrossRef] [Green Version]
- Bartko, J.J. On various intraclass correlation reliability coefficients. Psychol. Bull. 1976, 83, 762–765. [Google Scholar] [CrossRef]









| Parameter | Definition | Measurement Unit |
|---|---|---|
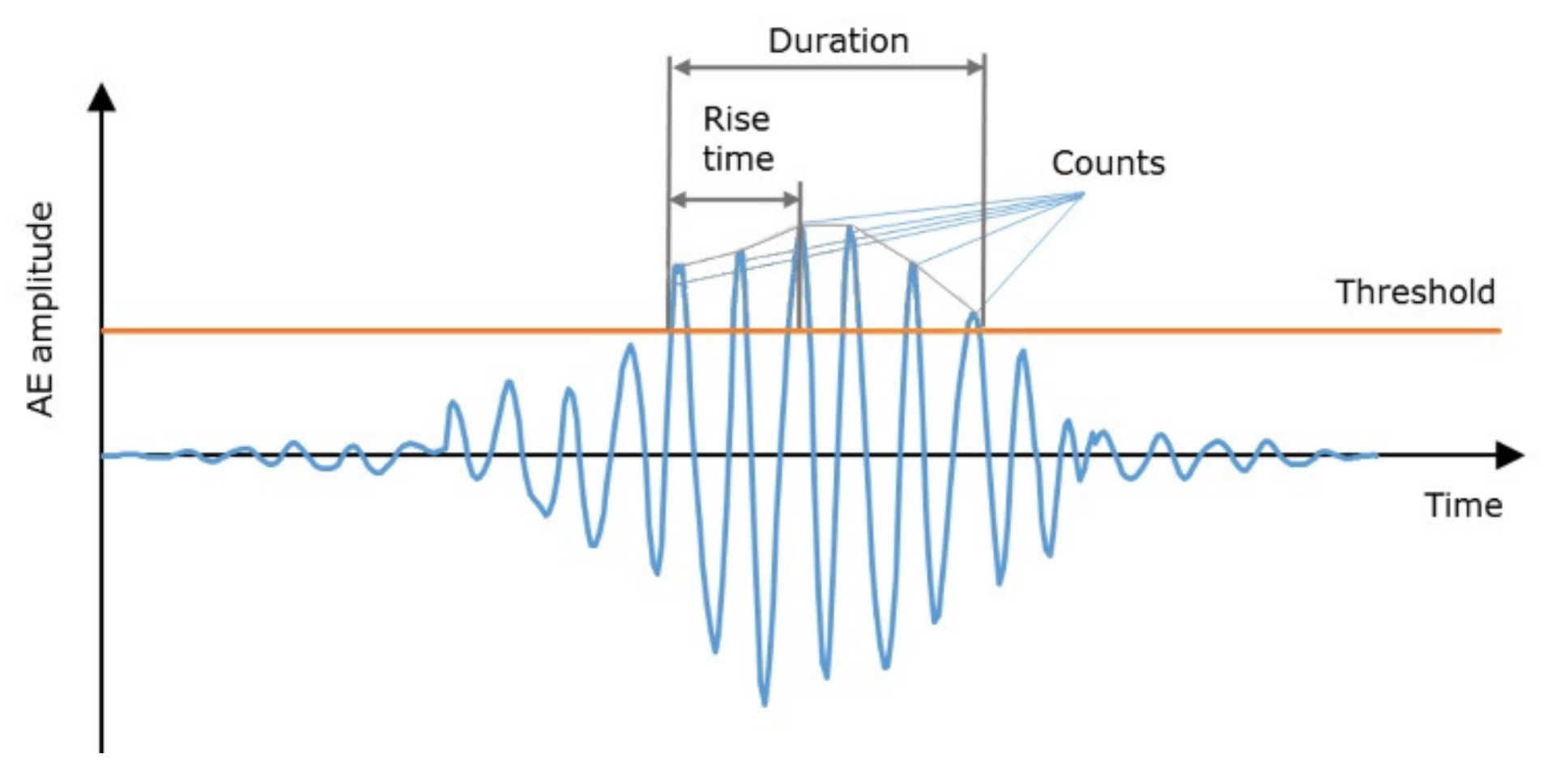
| Hits number | Number of the detected AE hits | - |
| Rise time | Time between detected AE hit start and its peak amplitude | µs |
| Counts | Number of an AE signal excursions over the threshold in one hit | - |
| Duration | Time from the first threshold crossing of the hit to the last | µs |
| Amplitude | Maximum AE signal excursion during a hit | dB |
| Counts to peak | Number of an AE signal excursions over the threshold between AE hit start and its peak amplitude | - |
| Signal strength | Integral of the rectified voltage signal over the duration of an AE hit | pV-s |
| Absolute (true) energy | Integral of the squared voltage signal divided by the reference resistance over the duration of an AE hit | attoJoules |
| Average frequency 1 | Average frequency over the entire AE hit | kHz |
| Reverberation frequency 1 | Average frequency of AE hit after the peak | kHz |
| Exercise 1 | ICC | Lower Bound (95% CI) | Upper Bound (95% CI) | CV1 | CV2 | CV3 |
|---|---|---|---|---|---|---|
| Hits per repetition: mean value | ||||||
| L30 | 0.771 | 0.205 | 0.951 | 1.093 | 1.069 | 1.137 |
| H30 | 0.694 | 0 | 0.934 | 1.120 | 0.773 | 0.992 |
| L60 | 0.901 | 0.681 | 0.978 | 1.015 | 0.798 | 0.980 |
| H60 | 0.765 | 0.163 | 0.950 | 0.861 | 0.528 | 0.919 |
| KL | 0.381 | 0 | 0.866 | 0.843 | 0.784 | 1.298 |
| SLS | 0.716 | 0 | 0.940 | 0.926 | 0.811 | 0.544 |
| Rise time (µs): mean value | ||||||
| L30 | 0.828 | 0.422 | 0.963 | 0.326 | 0.523 | 0.389 |
| H30 | 0.844 | 0.503 | 0.965 | 0.441 | 0.417 | 0.510 |
| L60 | 0.538 | 0 | 0.903 | 0.292 | 0.533 | 0.402 |
| H60 | 0.785 | 0.267 | 0.954 | 0.307 | 0.409 | 0.514 |
| KL | 0.073 | 0 | 0.790 | 0.417 | 0.658 | 0.562 |
| SLS | 0.200 | 0 | 0.832 | 0.706 | 0.763 | 0.487 |
| Duration (µs): mean value | ||||||
| L30 | 0.810 | 0.332 | 0.959 | 0.319 | 0.454 | 0.482 |
| H30 | 0.794 | 0.279 | 0.956 | 0.350 | 0.406 | 0.556 |
| L60 | 0.856 | 0.533 | 0.968 | 0.212 | 0.407 | 0.456 |
| H60 | 0.728 | 0.025 | 0.942 | 0.270 | 0.406 | 0.637 |
| KL | 0 | 0 | 0.526 | 0.419 | 0.444 | 0.521 |
| SLS | 0.513 | 0 | 0.893 | 0.563 | 0.581 | 0.444 |
| Reverberation Frequency (kHz): mean value | ||||||
| L30 | 0.712 | 0 | 0.938 | 0.182 | 0.534 | 0.420 |
| H30 | 0.827 | 0.426 | 0.962 | 0.357 | 0.616 | 0.517 |
| L60 | 0.567 | 0 | 0.899 | 0.243 | 0.550 | 0.512 |
| H60 | 0.696 | 0 | 0.935 | 0.280 | 0.387 | 0.384 |
| KL | 0 | 0 | 0.710 | 0.764 | 0.750 | 0.671 |
| SLS | 0.102 | 0 | 0.807 | 0.659 | 0.667 | 0.555 |
| Exercise 1 | ICC | Lower Bound (95% CI) | Upper Bound (95% CI) | CV Range |
|---|---|---|---|---|
| Session 1 | ||||
| L30 | 0.974 | 0.941 | 0.994 | 0.110–0.336 |
| H30 | 0.984 | 0.963 | 0.996 | 0.074–0.347 |
| L60 | 0.984 | 0.963 | 0.996 | 0.065–0.271 |
| H60 | 0.971 | 0.934 | 0.993 | 0.077–0.323 |
| KL | 0.760 | 0.541 | 0.933 | 0.217–1.512 |
| SLS | 0.795 | 0.593 | 0.944 | 0.146–1.532 |
| Session 2 | ||||
| L30 | 0.903 | 0.796 | 0.975 | 0.134–0.371 |
| H30 | 0.942 | 0.872 | 0.986 | 0.097–0.611 |
| L60 | 0.964 | 0.918 | 0.991 | 0.082–0.582 |
| H60 | 0.920 | 0.828 | 0.980 | 0.086–0.601 |
| KL | 0.725 | 0.492 | 0.921 | 0.204 2–0.672 |
| SLS | 0.884 | 0.746 | 0.971 | 0.123–1.088 |
| Session 3 | ||||
| L30 | 0.924 | 0.835 | 0.981 | 0.152–1.593 |
| H30 | 0.949 | 0.887 | 0.987 | 0.089–0.479 |
| L60 | 0.966 | 0.923 | 0.992 | 0.087–0.544 |
| H60 | 0.966 | 0.923 | 0.992 | 0.072–0.708 |
| KL | 0.901 | 0.777 | 0.975 | 0.127–0.943 |
| SLS | 0.600 | 0.343 | 0.872 | 0.247–1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khokhlova, L.; Komaris, D.-S.; Tedesco, S.; O’Flynn, B. Test-Retest Reliability of Acoustic Emission Sensing of the Knee during Physical Tasks. Sensors 2022, 22, 9027. https://doi.org/10.3390/s22239027
Khokhlova L, Komaris D-S, Tedesco S, O’Flynn B. Test-Retest Reliability of Acoustic Emission Sensing of the Knee during Physical Tasks. Sensors. 2022; 22(23):9027. https://doi.org/10.3390/s22239027
Chicago/Turabian StyleKhokhlova, Liudmila, Dimitrios-Sokratis Komaris, Salvatore Tedesco, and Brendan O’Flynn. 2022. "Test-Retest Reliability of Acoustic Emission Sensing of the Knee during Physical Tasks" Sensors 22, no. 23: 9027. https://doi.org/10.3390/s22239027