
Using Artificial Intelligence-Enhanced Sensing and Wearable Technology in Sports Medicine and Performance Optimisation
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
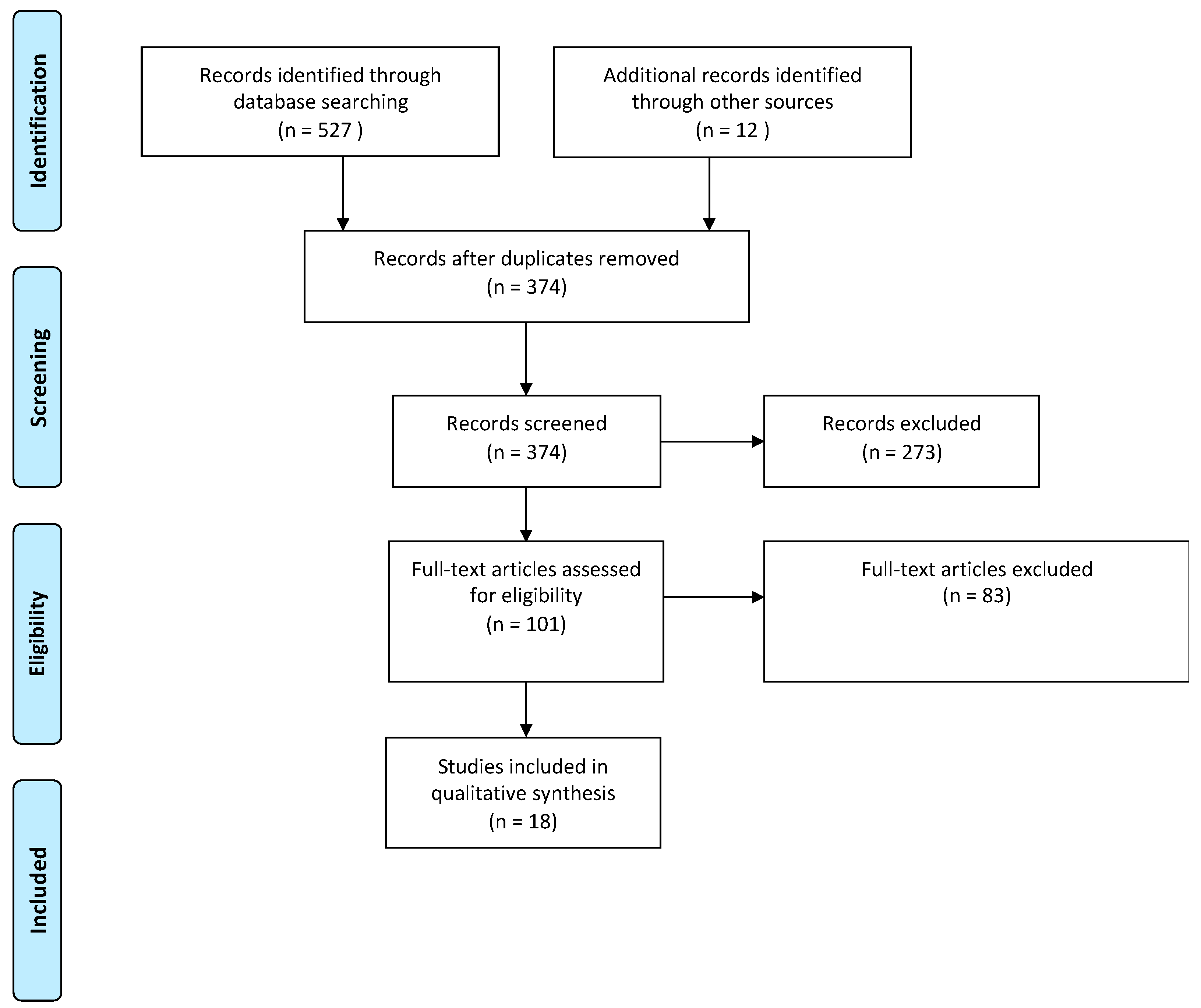
2.1. Literature Search
2.2. Selection and Quality Assessment of Studies
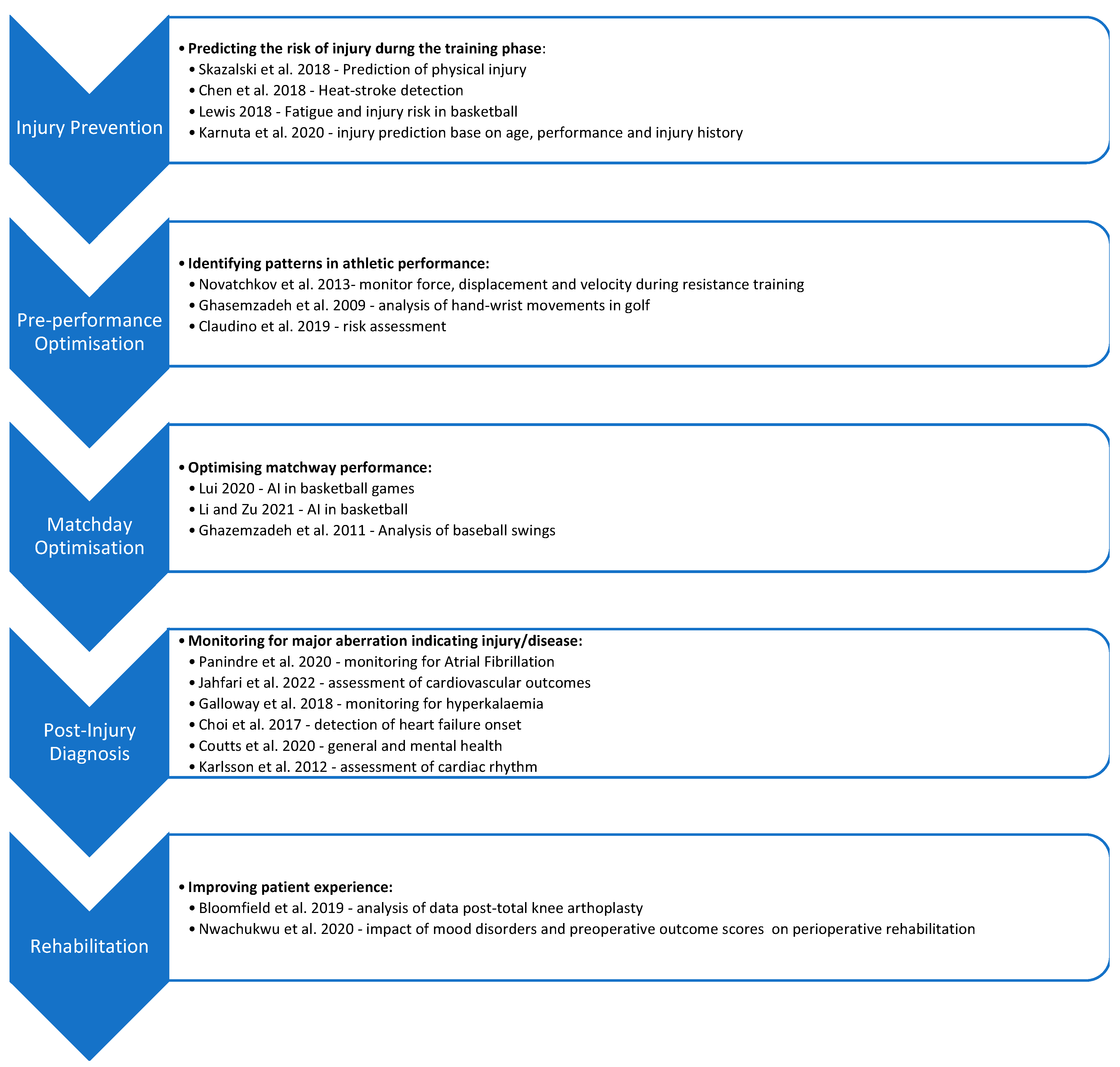
3. Before the Event: Prediction of Athlete’s Injury Risk
4. Before and during the Event: Optimisation of Athletic Performance
5. After the Event: AI-Based Wearable Devices as Diagnostic Systems
6. After the Event: An Opportunity to Improve Patient Experience
7. Challenges and Areas of Future Work
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ometov, A.; Shubina, V.; Klus, L.; Skibińska, J.; Saafi, S.; Pascacio, P.; Flueratoru, L.; Gaibor, D.Q.; Chukhno, N.; Chukhno, O.; et al. A Survey on Wearable Technology: History, State-of-the-Art and Current Challenges. Comput. Netw. 2021, 193, 108074. [Google Scholar] [CrossRef]
- Wearable Technology Market Size, Share & Trends Analysis Report By Product (Wrist-Wear, Eye-Wear & Head-Wear, Foot-Wear, Neck-Wear, Body-Wear), By Application, By Region, And Segment Forecasts, 2021–2028. 2020. Available online: https://www.grandviewresearch.com/industry-analysis/wearable-technology-market (accessed on 6 September 2022).
- Altini, M.; Kinnunen, H. The Promise of Sleep: A Multi-Sensor Approach for Accurate Sleep Stage Detection Using the Oura Ring. Sensors 2021, 21, 4302. [Google Scholar] [CrossRef] [PubMed]
- de Zambotti, M.; Rosas, L.; Colrain, I.M.; Baker, F.C. The Sleep of the Ring: Comparison of the ŌURA Sleep Tracker Against Polysomnography. Behav. Sleep Med. 2019, 17, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Turakhia, M.P.; Desai, M.; Hedlin, H.; Rajmane, A.; Talati, N.; Ferris, T.; Desai, S.; Nag, D.; Patel, M.; Kowey, P.; et al. Rationale and design of a large-scale, app-based study to identify cardiac arrhythmias using a smartwatch: The Apple Heart Study. Am. Heart J. 2018, 207, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Helm, J.M.; Swiergosz, A.M.; Haeberle, H.S.; Karnuta, J.M.; Schaffer, J.L.; Krebs, V.E.; Spitzer, A.I.; Ramkumar, P.N. Machine Learning and Artificial Intelligence: Definitions, Applications, and Future Directions. Curr. Rev. Musculoskelet. Med. 2020, 13, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; Depristo, M.; Chou, K.; Cui, C.; Corrado, G.; Thrun, S.; Dean, J. A guide to deep learning in healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef] [PubMed]
- McKinney, S.M.; Sieniek, M.; Godbole, V.; Godwin, J.; Antropova, N.; Ashrafian, H.; Back, T.; Chesus, M.; Corrado, G.S.; Darzi, A.; et al. International evaluation of an AI system for breast cancer screening. Nature 2020, 577, 89–94. [Google Scholar] [CrossRef]
- Skazalski, C.; Whiteley, R.; Hansen, C.; Bahr, R. A valid and reliable method to measure jump-specific training and competition load in elite volleyball players. Scand. J. Med. Sci. Sports 2018, 28, 1578–1585. [Google Scholar] [CrossRef]
- Chen, S.-T.; Lin, S.-S.; Lan, C.-W.; Hsu, H.-Y. Design and Development of a Wearable Device for Heat Stroke Detection. Sensors 2017, 18, 17. [Google Scholar] [CrossRef]
- Lewis, M. It’s a Hard-Knock Life: Game Load, Fatigue, and Injury Risk in the National Basketball Association. J. Athl. Train. 2018, 53, 503–509. [Google Scholar] [CrossRef] [Green Version]
- Karnuta, J.M.; Luu, B.C.; Haeberle, H.S.; Saluan, P.M.; Frangiamore, S.J.; Stearns, K.L.; Farrow, L.D.; Nwachukwu, B.U.; Verma, N.N.; Makhni, E.C.; et al. Machine Learning Outperforms Regression Analysis to Predict Next-Season Major League Baseball Player Injuries: Epidemiology and Validation of 13,982 Player-Years From Performance and Injury Profile Trends, 2000–2017. Orthop. J. Sports Med. 2020, 8, 2325967120963046. [Google Scholar] [CrossRef] [PubMed]
- Novatchkov, H.; Baca, A. Artificial intelligence in sports on the example of weight training. J. Sports Sci. Med. 2013, 12, 27–37. [Google Scholar] [PubMed]
- Ghasemzadeh, H.; Loseu, V.; Jafari, R. Wearable coach for sport training: A quantitative model to evaluate wrist-rotation in golf. J. Ambient Intell. Smart Environ. 2009, 1, 173–184. [Google Scholar] [CrossRef]
- Bloomfield, R.; Williams, H.A.; Broberg, J.S.; Lanting, B.A.; McIsaac, K.A.; Teeter, M.G. Machine Learning Groups Patients by Early Functional Improvement Likelihood Based on Wearable Sensor Instrumented Preoperative Timed-Up-and-Go Tests. J. Arthroplast. 2019, 34, 2267–2271. [Google Scholar] [CrossRef]
- Coutts, L.V.; Plans, D.; Brown, A.W.; Collomosse, J. Deep learning with wearable based heart rate variability for prediction of mental and general health. J. Biomed. Inform. 2020, 112, 103610. [Google Scholar] [CrossRef]
- Karlsson, M.; Hörnsten, R.; Rydberg, A.; Wiklund, U. Automatic filtering of outliers in RR intervals before analysis of heart rate variability in Holter recordings: A comparison with carefully edited data. Biomed. Eng. Online 2012, 11, 2. [Google Scholar] [CrossRef]
- Claudino, J.G.; de Oliveira Capanema, D.; De Souza, T.V.; Serrão, J.C.; Pereira, A.C.M.; Nassis, G.P. Current Approaches to the Use of Artificial Intelligence for Injury Risk Assessment and Performance Prediction in Team Sports: A Systematic Review. Sports Med. Open 2019, 5, 28. [Google Scholar] [CrossRef]
- Liu, Z. Application of Artificial Intelligence Technology in Basketball Games. IOP Conf. Ser. Mater. Sci. Eng. 2020, 750, 12093. [Google Scholar] [CrossRef]
- Li, B.; Xu, X. Application of Artificial Intelligence in Basketball Sport. J. Educ. Health Sport 2021, 11, 54–67. [Google Scholar] [CrossRef]
- Lapham, A.; Bartlett, R. The use of artificial intelligence in the analysis of sports performance: A review of applications in human gait analysis and future directions for sports biomechanics. J. Sports Sci. 1995, 13, 229–237. [Google Scholar] [CrossRef]
- Panindre, P.; Gandhi, V.; Kumar, S. Comparison of Performance of Artificial Intelligence Algorithms for Real-Time Atrial Fibrillation Detection using Instantaneous Heart Rate. In Proceedings of the 2020 IEEE 17th International Conference on Smart Communities: Improving Quality of Life Using ICT, IoT and AI (HONET), Charlotte, NC, USA, 14–16 December 2020; pp. 168–172. [Google Scholar] [CrossRef]
- Jahfari, A.N.; Tax, D.; Reinders, M.; van der Bilt, I. Machine Learning for Cardiovascular Outcomes From Wearable Data: Systematic Review From a Technology Readiness Level Point of View. JMIR Med. Informatics 2022, 10, e29434. [Google Scholar] [CrossRef] [PubMed]
- Galloway, C.D.; Valys, A.V.; Petterson, F.L.; Gundotra, V.P.; Treiman, D.L.; Albert, D.E.; Dillon, J.J.; Attia, Z.I.; Friedman, P.A. Non-invasive detection of hyperkalemia with a smartphone electrocardiogram and artificial intelligence. J. Am. Coll. Cardiol. 2018, 71, A272. [Google Scholar] [CrossRef]
- Choi, E.; Schuetz, A.; Stewart, W.F.; Sun, J. Using recurrent neural network models for early detection of heart failure onset. J. Am. Med. Inform. Assoc. 2016, 24, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Nwachukwu, B.U.; Beck, E.C.; Lee, E.; Cancienne, J.M.; Waterman, B.R.; Paul, K.; Nho, S.J. Application of Machine Learning for Predicting Clinically Meaningful Outcome After Arthroscopic Femoroacetabular Impingement Surgery. Am. J. Sports Med. 2019, 48, 415–423. [Google Scholar] [CrossRef]
- Ley, C.; Martin, R.K.; Pareek, A.; Groll, A.; Seil, R.; Tischer, T. Machine learning and conventional statistics: Making sense of the differences. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 753–757. [Google Scholar] [CrossRef]
- Bzdok, D. Classical Statistics and Statistical Learning in Imaging Neuroscience. Front. Neurosci. 2017, 11, 543. [Google Scholar] [CrossRef]
- Bzdok, D.; Krzywinski, M.; Altman, N. Machine learning: Supervised methods. Nat. Methods 2018, 15, 5–6. [Google Scholar] [CrossRef]
- Krzywinski, M.; Altman, N. Comparing samples—Part II. Nat. Methods 2014, 11, 355. [Google Scholar] [CrossRef]
- Lever, J.; Krzywinski, M.; Altman, N. Model selection and overfitting. Nat. Methods 2016, 13, 703–704. [Google Scholar] [CrossRef]
- Bzdok, D.; Altman, N.; Krzywinski, M. Statistics versus machine learning. Nat. Methods 2018, 15, 233–234. [Google Scholar] [CrossRef]
- Burke, B.B.; Phillips, G.; Jacobson, A.; Eager, E.; Chahrouri, G.; Mack, C.D. Injuries Cost NFL Teams Over $500 Million In 2019. Orthop. J. Sport Med. 2020, 21, 9. [Google Scholar]
- Uematsu, T.; Sano, A.; Taylor, S.; Picard, R.W. Improving Stress Forecasting Using LSTM Neural Networks. In Proceedings of the 2019 IEEE EMBS International Conference on Biomedical & Health Informatics (BHI), Chicago, IL, USA, 19–22 May 2019. [Google Scholar]
- Rodrigues, A.C.N.; Pereira, A.; Mendes, R.M.S.; Araújo, A.G.; Couceiro, M.S.; Figueiredo, A.J. Using Artificial Intelligence for Pattern Recognition in a Sports Context. Sensors 2020, 20, 3040. [Google Scholar] [CrossRef] [PubMed]
- Noble, J. How Red Bull plans to take AI in F1 to the next level. Motorsport. 15 April 2021.
- Darzi, A. High Quality Care for All: NHS Next Stage Review; Department of Health: London, UK, 2008. [Google Scholar]
- Department of Health. NHS Next Stage Review: A High Quality Workforce. Inquiry. 2008. Available online: https://www.gov.uk/government/publications/high-quality-care-for-all-nhs-next-stage-review-final-report (accessed on 6 September 2022).
- Fontana, M.A.; Lyman, S.; Sarker, G.K.; Padgett, D.E.; MacLean, C.H. Can machine learning algorithms predict which patients will achieve minimally clinically important differences from total joint arthroplasty? Clin. Orthop. Relat. Res. 2019, 477, 1267. [Google Scholar] [CrossRef] [PubMed]
- Paschos, N.K. Editorial Commentary: Artificial Intelligence in Sports Medicine Diagnosis Needs to Improve. Arthrosc. J. Arthrosc. Relat. Surg. 2021, 37, 782–783. [Google Scholar] [CrossRef] [PubMed]
- Wawira Gichoya, J.; McCoy, L.G.; Celi, L.A.; Ghassemi, M. Equity in essence: A call for operationalising fairness in machine learning for healthcare. BMJ Health Care Inform. 2021, 28, e100289. [Google Scholar] [CrossRef]
- Soliño-Fernandez, D.; Ding, A.; Bayro-Kaiser, E.; Ding, E.L. Willingness to adopt wearable devices with behavioral and economic incentives by health insurance wellness programs: Results of a US cross-sectional survey with multiple consumer health vignettes. BMC Public Health 2019, 19, 1649. [Google Scholar] [CrossRef]
- Gao, Y.; Li, H.; Luo, Y. An empirical study of wearable technology acceptance in healthcare. Ind. Manag. Data Syst. 2015, 115, 1704–1723. [Google Scholar] [CrossRef]
- Tran, V.-T.; Riveros, C.; Ravaud, P. Patients’ views of wearable devices and AI in healthcare: Findings from the ComPaRe e-cohort. NPJ Digit. Med. 2019, 2, 53. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Author | Year | Country | Design | Sample Size | Sex (% of Males) | Age | Sport/Activity | Outcome Measures | Sensor | Conclusion |
|---|---|---|---|---|---|---|---|---|---|---|
| Skazalski et al. [9] | 2018 | Qatar | Comparing IMU data with visual observation of jumps | 14 | 100 | Not Specified | Volleyball | 1. Jump Count recorded by IMU device, compared with visual observation 2. Jump height recorded by IMU device and compared with visual observation | Vert Classic (Model #JEM) with Vert Coach Application (version 2.0.6) | Vert device demonstrates excellent accuracy counting volleyball-specific jumps. Vert Device can be used to monitor athlete jump intensity |
| Chen et al. [10] | 2018 | Taiwan | Using a Wearable heat-stroke-detection device (WHDD) to monitor a runner’s physiological information | 1 | 100 | 35 | Running | 1. Galvanic skin response. 2. Heart rate. 3. Body temperature. 4. Ambient temperature. 5. Ambient humidity. 6. Predicted risk of heat stroke. Above measures all recorded during a predertemined running programme | Custom WHDD with GSR, MLX90614 and SHT75 sensors. | WHDD detected the trend in a runner’s physiologcal information in advance of exercise intensity. The WHDD could specifically prevent the occurrence of heat stroke. |
| Lewis [11] | 2018 | USA | Cross sectional study | 627 | 100 | Not specified | Basketball | 1. Injury events. 2. Player fatigue. 3. Performance load (total rebounds and field goal attempts). | Random-effects, multi-level logistic regression model | Higher levels of fatigue and workload led to greater injury risk. With these constant factors, a higher injury risk was associated with greater NBA experience and below average height. |
| Karnuta et al. [12] | 2020 | USA | Descriptive Epidemiology Study | 139,783 | 100 | Not Specified | Baseball | Predictions for future injury risk based on logistic regression and machine learning algorithms. | Logistic regression, random forest, k-nearest neighbours, Naïve Bayers, XGBoost, Top 3 Ensemble. Models were built usnig scikit-learn Python library (Version 0.20.3) and XGBoost (Version 1.0.2) | Advanced machine learning models outperformed logistic regression and demonstrated fair capability of predicting whether a publicy reportable injury was likely to occur. |
| Novatchkov and Baca [13] | 2013 | Austria | Descriptive Study | 15 | 53 | 24.6 | Weight Training | Force displacement parameters measured from a weght leg press machine | Weight leg press machine equipped wht a load cell (PW10A or PW12C3, Hottinger Baldwin) and a rotary encoder (DP18, Altmann). Modelling of signals by multilayer pattern recognition networks based on the Levenberg-Marquardt algorthm. | Computer based feedback frameworks can be used for analysis of performance during workouts. |
| Ghasemzadeh et al. [14] | 2009 | USA | Quantitative analysis of golf swings using BSN | 4 | 75 | 20–35 | Golf | Degrees of wrist rotation during segments of a golf swing | TelosB from Xbow | Body Sensor Networks can provide information on the quality of a golf swing with respect to the angle of the wrist rotation |
| Bloomfield et al. [15] | 2019 | Canada | Cross sectional study | 68 | 34 | 65.6 ± 9.1 | Timed-up-and-go tests | Post-operative recovery | custom wearable system | Wearable sensors during instrument functional tests during clinical visits and using machine learning to parse complex patterns can reveal clinically relevant parameters |
| Coutts et al. [16] | 2020 | UK | Prospective cohort study | 100 in trial 1; 799 Iin trial 2 | 38; 224 | 18–38; 18–69 | Cycling | Heart rate; Perceived Stress Scale; Depression Anxiety Stress Scale; State and Trait Anxiety | Biobeam band; Deep Neural Networks (LSTMs) | Classification accuracy of up to 85% with the current AI model and biosensor. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chidambaram, S.; Maheswaran, Y.; Patel, K.; Sounderajah, V.; Hashimoto, D.A.; Seastedt, K.P.; McGregor, A.H.; Markar, S.R.; Darzi, A. Using Artificial Intelligence-Enhanced Sensing and Wearable Technology in Sports Medicine and Performance Optimisation. Sensors 2022, 22, 6920. https://doi.org/10.3390/s22186920
Chidambaram S, Maheswaran Y, Patel K, Sounderajah V, Hashimoto DA, Seastedt KP, McGregor AH, Markar SR, Darzi A. Using Artificial Intelligence-Enhanced Sensing and Wearable Technology in Sports Medicine and Performance Optimisation. Sensors. 2022; 22(18):6920. https://doi.org/10.3390/s22186920
Chicago/Turabian StyleChidambaram, Swathikan, Yathukulan Maheswaran, Kian Patel, Viknesh Sounderajah, Daniel A. Hashimoto, Kenneth Patrick Seastedt, Alison H. McGregor, Sheraz R. Markar, and Ara Darzi. 2022. "Using Artificial Intelligence-Enhanced Sensing and Wearable Technology in Sports Medicine and Performance Optimisation" Sensors 22, no. 18: 6920. https://doi.org/10.3390/s22186920