
A Comprehensive Analysis of the Validity and Reliability of the Perception Neuron Studio for Upper-Body Motion Capture


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instrumentation
2.3. Experimental Protocol
2.4. Data Preprocessing
2.5. Statistical Analysis
3. Results
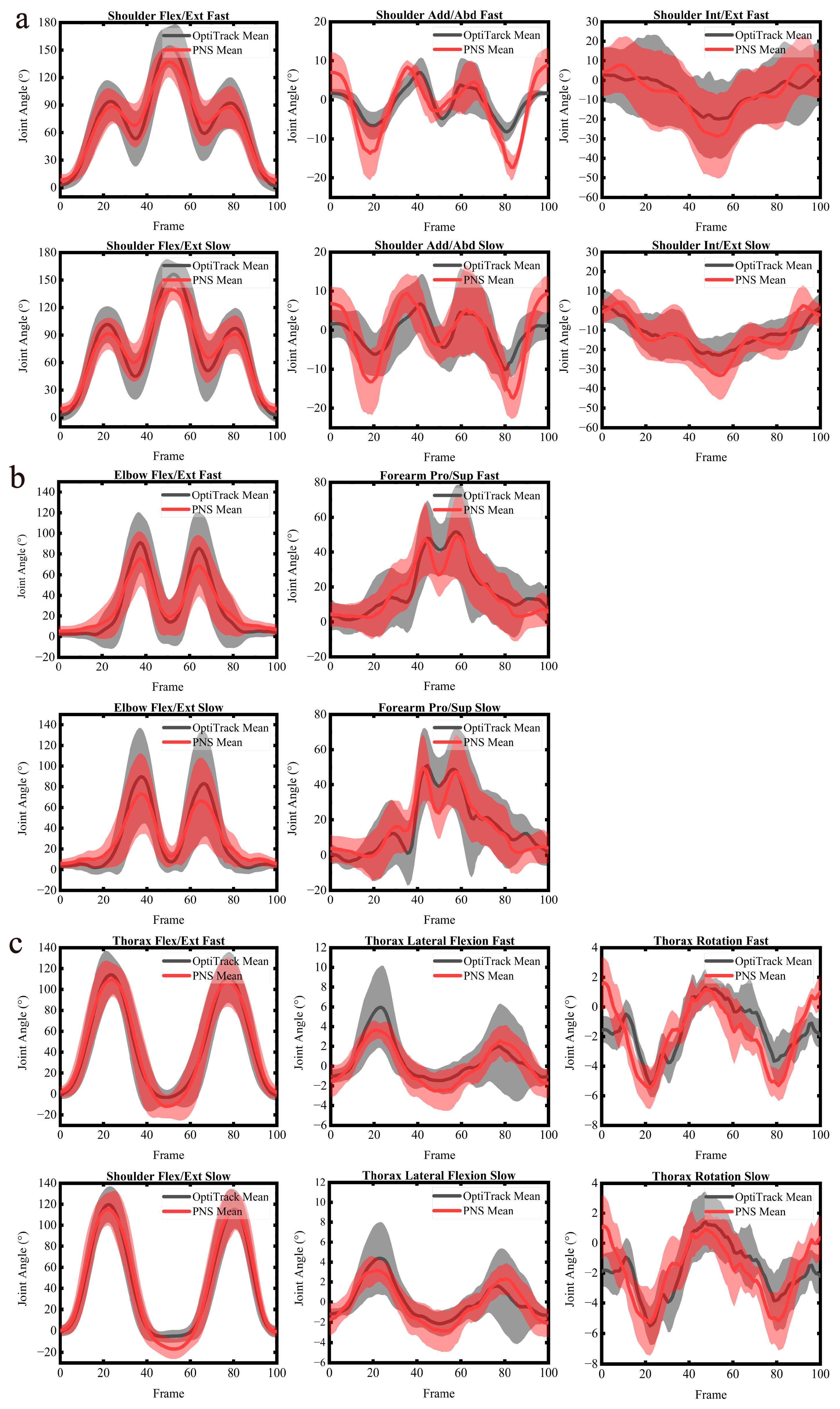
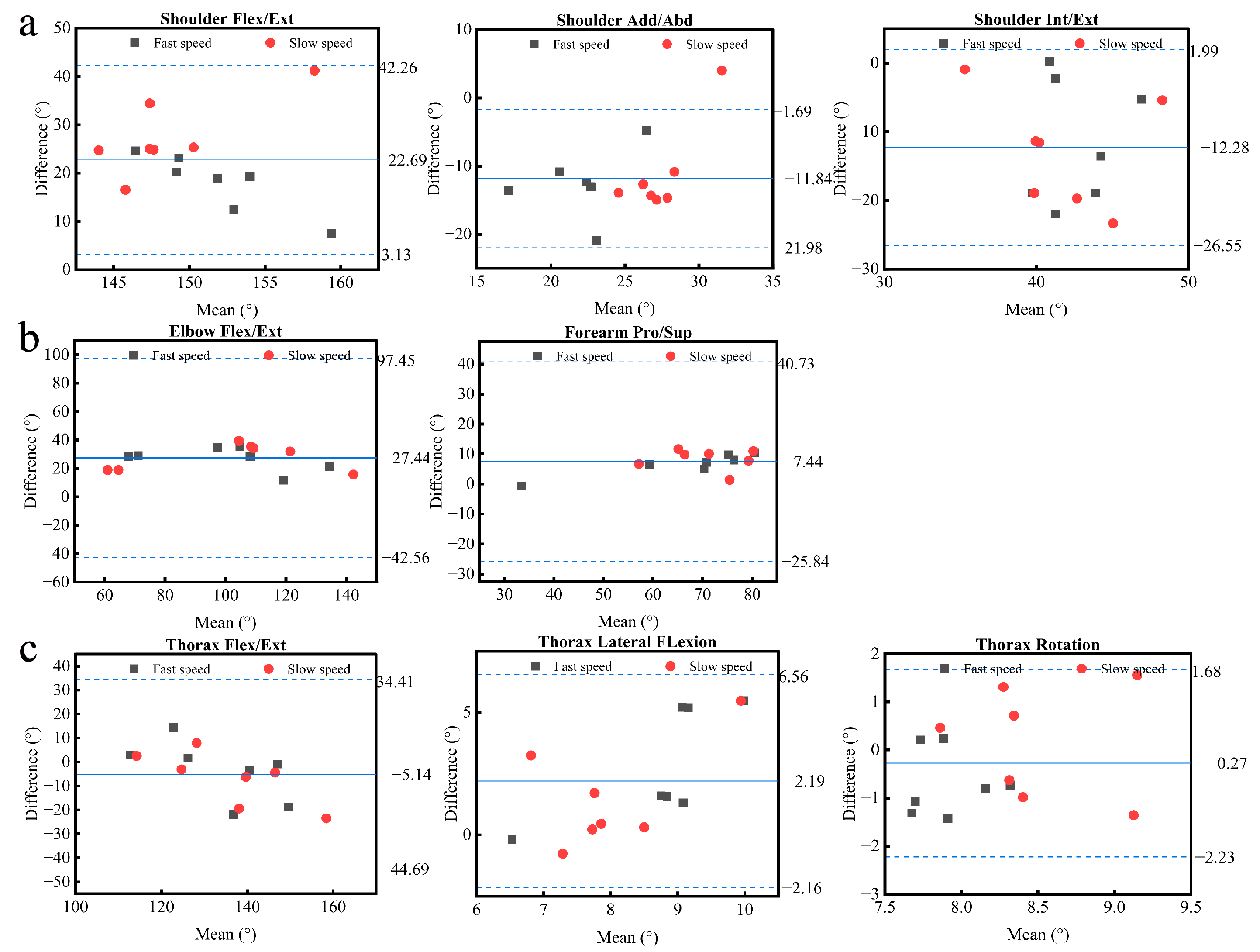
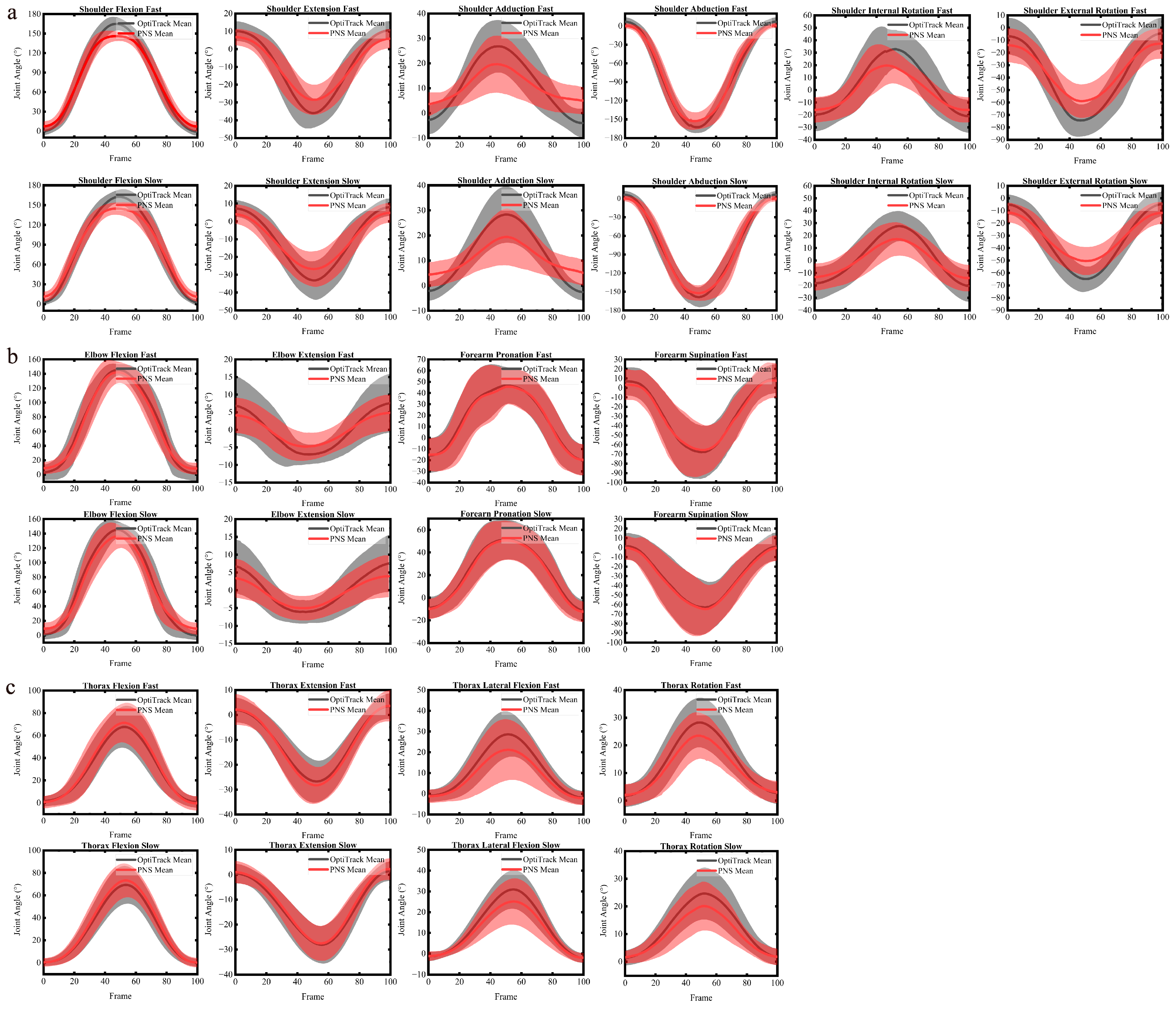
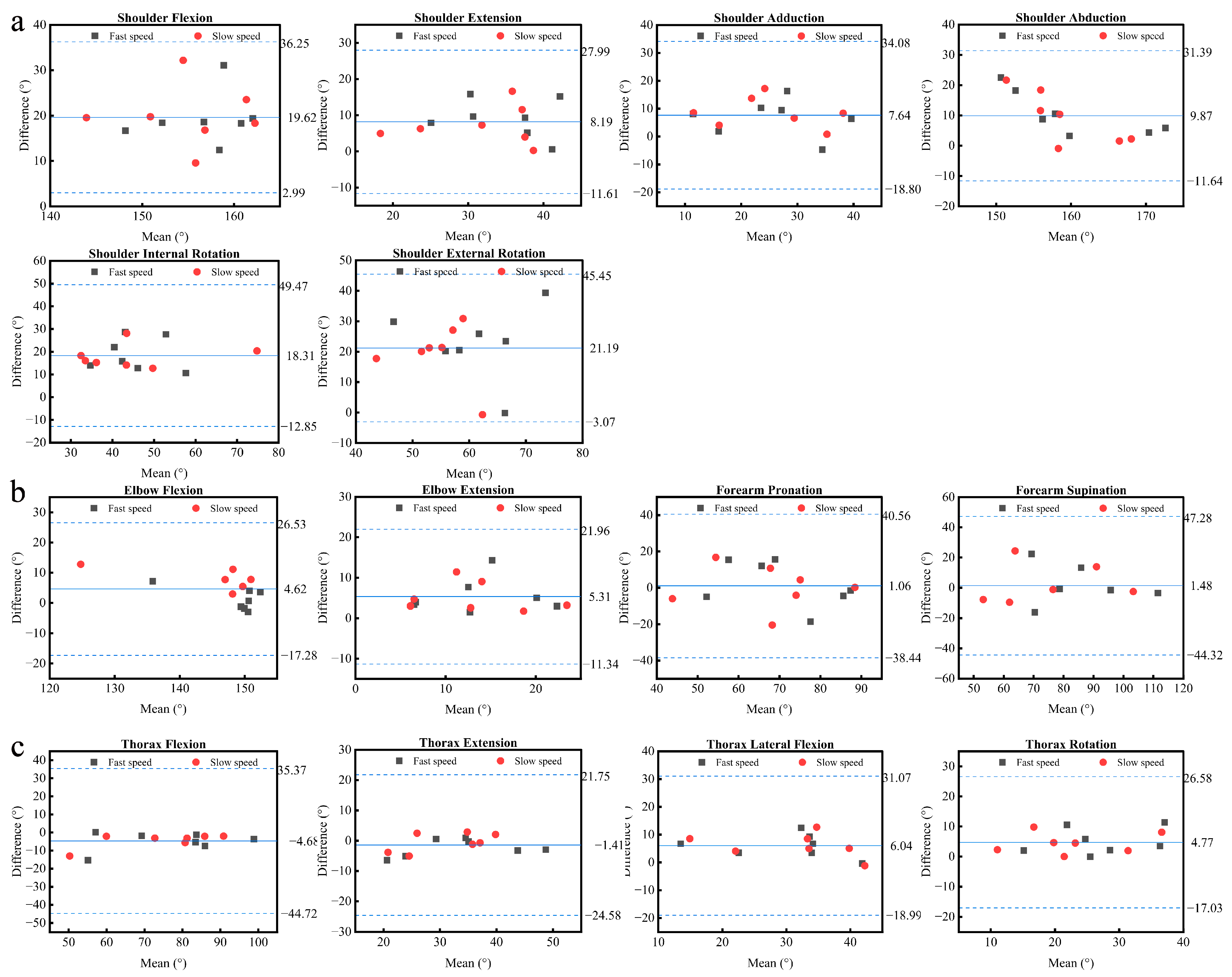
3.1. PNS’ Concurrent Validity in Upper-Body Assessment
3.2. PNS’ Intra- and Intersession Reliability
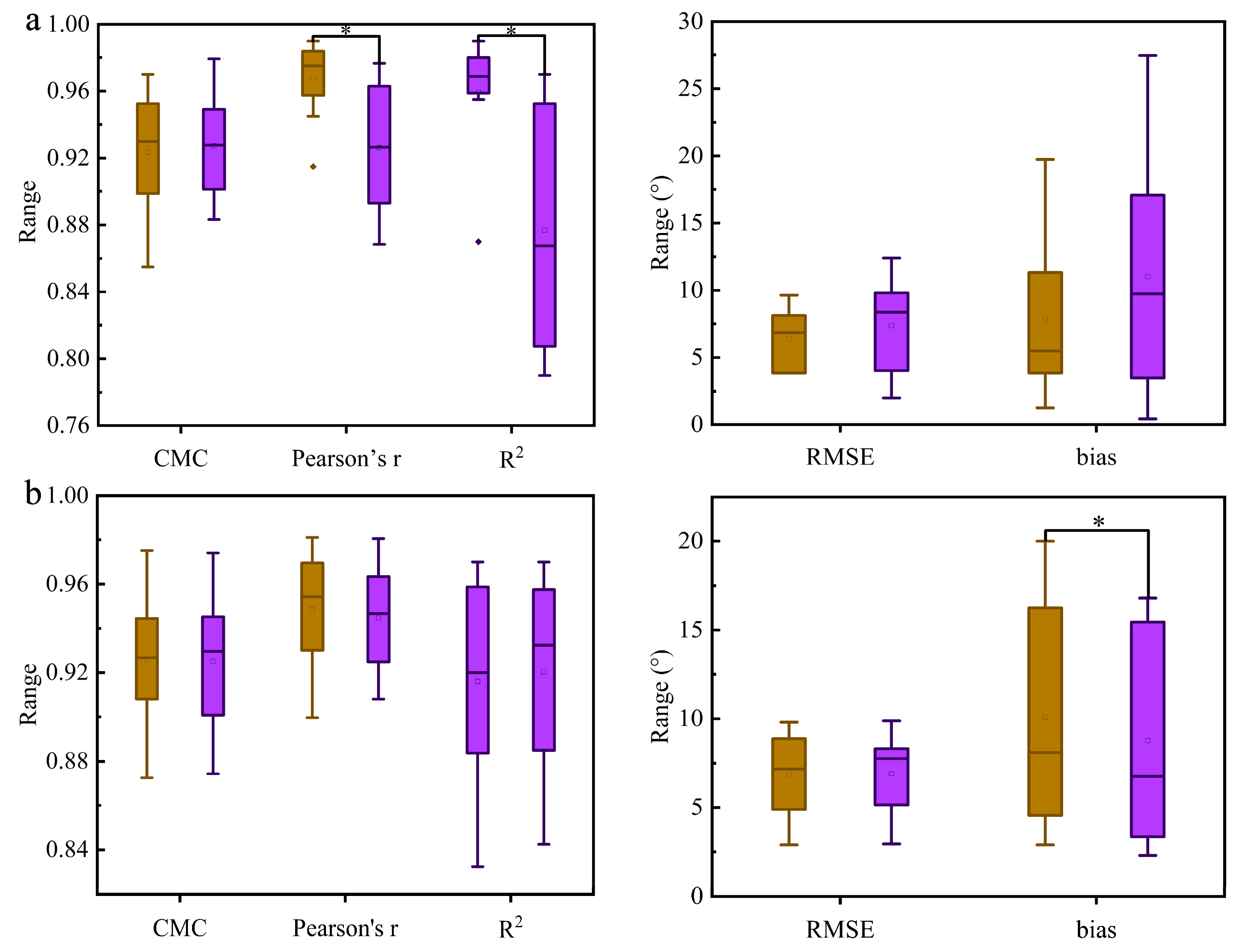
3.3. Task Complexity and Movement Speed Analysis
4. Discussion
4.1. PNS’ Concurrent Validity in Upper-Body Assessment
4.2. PNS’ Intra- and Intersession Reliability
4.3. Task Complexity and Movement Speed Analysis
4.4. Limitation and Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | TEM | SWC0.2 | SWC0.6 | SWC1.2 | MDC95% | |
|---|---|---|---|---|---|---|
| Shoulder | flexion/ extension | 0.77 | 1.14 | 3.41 | 6.81 | 2.13 |
| adduction/ abduction | 1.26 | 1.21 | 3.63 | 7.25 | 3.49 | |
| internal/ external rotation | 2.53 | 1.61 | 4.82 | 9.65 | 7.03 | |
| Elbow | flexion/ extension | 1.85 | 3.05 | 9.16 | 18.31 | 5.12 |
| pronation/ supination | 3.31 | 2.88 | 8.65 | 17.30 | 9.18 | |
| Thorax | flexion/ extension | 1.63 | 2.86 | 8.58 | 17.17 | 4.52 |
| lateral flexion | 1.25 | 0.97 | 2.92 | 5.84 | 3.47 | |
| rotation | 0.48 | 0.78 | 2.34 | 4.68 | 1.34 | |
References
- Nagymáté, G.; Kiss, R.M. Application of OptiTrack motion capture systems in human movement analysis: A systematic literature review. Recent Innov. Mechatron. 2018, 5, 1–9. [Google Scholar] [CrossRef]
- Valevicius, A.M.; Jun, P.Y.; Hebert, J.S.; Vette, A.H. Use of optical motion capture for the analysis of normative upper body kinematics during functional upper limb tasks: A systematic review. J. Electromyogr. Kinesiol. 2018, 40, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Taborri, J.; Keogh, J.; Kos, A.; Santuz, A.; Umek, A.; Urbanczyk, C.; van der Kruk, E.; Rossi, S. Sport biomechanics applications using inertial, force, and EMG sensors: A literature overview. Appl. Bionics Biomech. 2020, 2020, 2041549. [Google Scholar] [CrossRef]
- Sessa, S.; Zecca, M.; Lin, Z.; Bartolomeo, L.; Ishii, H.; Takanishi, A. A methodology for the performance evaluation of inertial measurement units. J. Intell. Robot. Syst. 2013, 71, 143–157. [Google Scholar] [CrossRef]
- Windt, J.; MacDonald, K.; Taylor, D.; Zumbo, B.D.; Sporer, B.C.; Martin, D.T. “To tech or not to tech?” A critical decision-making framework for implementing technology in sport. J. Athl. Train. 2020, 55, 902–910. [Google Scholar] [CrossRef]
- Sperlich, B.; Holmberg, H.-C. Wearable, yes, but able…?: It is time for evidence-based marketing claims! Br. J. Sports Med. 2017, 51, 1240. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, F.; Duval, C.; Jog, M.; Bee, C.; South, A.; Edwards, R.; Boissy, P. Capturing whole-body mobility of patients with Parkinson disease using inertial motion sensors: Expected challenges and rewards. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 5833–5838. [Google Scholar]
- Brice, S.M.; Phillips, E.J.; Millett, E.L.; Hunter, A.; Philippa, B. Comparing inertial measurement units and marker-based biomechanical models during dynamic rotation of the torso. Eur. J. Sport Sci. 2020, 20, 767–775. [Google Scholar] [CrossRef]
- Al-Amri, M.; Nicholas, K.; Button, K.; Sparkes, V.; Sheeran, L.; Davies, J.L. Inertial measurement units for clinical movement analysis: Reliability and concurrent validity. Sensors 2018, 18, 719. [Google Scholar] [CrossRef]
- Chung, W.; Yeung, S.; Chan, W.; Lee, R. Validity of VICON motion analysis system for upper limb kinematic MeasuremeNT–A comparison study with inertial tracking Xsens system. Hong Kong Physiother. J. 2011, 2, 97. [Google Scholar] [CrossRef]
- Sers, R.; Forrester, S.; Moss, E.; Ward, S.; Ma, J.; Zecca, M. Validity of the Perception Neuron inertial motion capture system for upper body motion analysis. Measurement 2020, 149, 107024. [Google Scholar] [CrossRef]
- Choo, C.Z.Y.; Chow, J.Y.; Komar, J. Validation of the Perception Neuron system for full-body motion capture. PLoS ONE 2022, 17, e0262730. [Google Scholar] [CrossRef] [PubMed]
- Shuai, Z.; Dong, A.; Liu, H.; Cui, Y. Reliability and Validity of an Inertial Measurement System to Quantify Lower Extremity Joint Angle in Functional Movements. Sensors 2022, 22, 863. [Google Scholar] [CrossRef] [PubMed]
- Poitras, I.; Dupuis, F.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.J.; Roy, J.-S. Validity and reliability of wearable sensors for joint angle estimation: A systematic review. Sensors 2019, 19, 1555. [Google Scholar] [CrossRef]
- Sama, A.J.; Hillstrom, H.; Daluiski, A.; Wolff, A. Reliability and agreement between two wearable inertial sensor devices for measurement of arm activity during walking and running gait. J. Hand Ther. 2020, 35, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Armitage, M.; Beato, M.; McErlain-Naylor, S.A. Inter-unit reliability of IMU Step metrics using IMeasureU Blue Trident inertial measurement units for running-based team sport tasks. J. Sports Sci. 2021, 39, 1512–1518. [Google Scholar] [CrossRef]
- Washabaugh, E.P.; Kalyanaraman, T.; Adamczyk, P.G.; Claflin, E.S.; Krishnan, C. Validity and repeatability of inertial measurement units for measuring gait parameters. Gait Posture 2017, 55, 87–93. [Google Scholar] [CrossRef]
- Walmsley, C.P.; Williams, S.A.; Grisbrook, T.; Elliott, C.; Imms, C.; Campbell, A. Measurement of upper limb range of motion using wearable sensors: A systematic review. Sports Med.-Open 2018, 4, 53. [Google Scholar] [CrossRef]
- Roetenberg, D.; Luinge, H.J.; Baten, C.T.; Veltink, P.H. Compensation of magnetic disturbances improves inertial and magnetic sensing of human body segment orientation. IEEE Trans. Neural Syst. Rehabil. Eng. 2005, 13, 395–405. [Google Scholar] [CrossRef]
- Camomilla, V.; Bergamini, E.; Fantozzi, S.; Vannozzi, G. Trends supporting the in-field use of wearable inertial sensors for sport performance evaluation: A systematic review. Sensors 2018, 18, 873. [Google Scholar] [CrossRef]
- Hindle, B.R.; Keogh, J.W.; Lorimer, A.V. Inertial-based human motion capture: A technical summary of current processing methodologies for spatiotemporal and kinematic measures. Appl. Bionics Biomech. 2021, 2021, 6628320. [Google Scholar] [CrossRef]
- Noitom. Available online: https://www.noitom.com.cn/ (accessed on 21 April 2022).
- OptiTrack. Available online: https://v21.wiki.optitrack.com/ (accessed on 21 April 2022).
- OpenSim. Available online: https://opensim.stanford.edu/ (accessed on 21 April 2022).
- Bolsterlee, B.; Veeger, H.; van der Helm, F.C. Modelling clavicular and scapular kinematics: From measurement to simulation. Med. Biol. Eng. Comput. 2014, 52, 283–291. [Google Scholar] [CrossRef]
- Maldonado, G.; Souères, P.; Watier, B. Whole-Body Musculo-Skeletal Model V1; [Technical Report] Rapport LAAS n° 18233, LAAS-CNRS. hal-01841355; Université de Toulouse 3 Paul Sabatier: Toulouse, France, 2018. [Google Scholar]
- Plantard, P.; Muller, A.; Pontonnier, C.; Dumont, G.; Shum, H.P.; Multon, F. Inverse dynamics based on occlusion-resistant Kinect data: Is it usable for ergonomics? Int. J. Ind. Ergon. 2017, 61, 71–80. [Google Scholar] [CrossRef]
- Bailey, C.A.; Uchida, T.K.; Nantel, J.; Graham, R.B. Validity and sensitivity of an inertial measurement unit-driven biomechanical model of motor variability for gait. Sensors 2021, 21, 7690. [Google Scholar] [CrossRef] [PubMed]
- Overbergh, T.; Severijns, P.; Beaucage-Gauvreau, E.; Jonkers, I.; Moke, L.; Scheys, L. Development and validation of a modeling workflow for the generation of image-based, subject-specific thoracolumbar models of spinal deformity. J. Biomech. 2020, 110, 109946. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Van der Helm, F.C.; Veeger, H.D.; Makhsous, M.; Van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.R.; McQuade, K.; Wang, X. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef] [PubMed]
- Abdi, H. Multiple correlation coefficient. Encycl. Meas. Stat. 2007, 648, 651. [Google Scholar] [CrossRef]
- Ferrari, A.; Cutti, A.G.; Cappello, A. A new formulation of the coefficient of multiple correlation to assess the similarity of waveforms measured synchronously by different motion analysis protocols. Gait Posture 2010, 31, 540–542. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding bland altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Ribeiro, A.I.; Franchini, E.; Mesquita, P.H.; Junior, P.A.A.; Albuquerque, M.R. Development and reliability of a kick test system for taekwondo athletes. J. Martial Arts Anthropol. 2020, 20, 31–39. [Google Scholar] [CrossRef]
- Wagner, J.M.; Rhodes, J.A.; Patten, C. Reproducibility and minimal detectable change of three-dimensional kinematic analysis of reaching tasks in people with hemiparesis after stroke. Phys. Ther. 2008, 88, 652–663. [Google Scholar] [CrossRef] [PubMed]
- Pasciuto, I.; Ligorio, G.; Bergamini, E.; Vannozzi, G.; Sabatini, A.M.; Cappozzo, A. How angular velocity features and different gyroscope noise types interact and determine orientation estimation accuracy. Sensors 2015, 15, 23983–24001. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Vargas, A.I.; Galán-Mercant, A.; Williams, J.M. The use of inertial sensors system for human motion analysis. Phys. Ther. Rev. 2010, 15, 462–473. [Google Scholar] [CrossRef] [PubMed]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Accuracy and repeatability of single-pose calibration of inertial measurement units for whole-body motion analysis. Gait Posture 2017, 54, 80–86. [Google Scholar] [CrossRef]
- Godwin, A.; Agnew, M.; Stevenson, J. Accuracy of inertial motion sensors in static, quasistatic, and complex dynamic motion. J. Biomech. Eng. 2009, 131, 5. [Google Scholar] [CrossRef]
- Mundt, M.; Wisser, A.; David, S.; Dupré, T.; Quack, V.; Bamer, F.; Tingart, M.; Potthast, W.; Markert, B. The influence of motion tasks on the accuracy of kinematic motion patterns of an IMU-based measurement system. ISBS Proc. Arch. 2017, 35, 245. [Google Scholar]
- Morrow, M.M.; Lowndes, B.; Fortune, E.; Kaufman, K.R.; Hallbeck, M.S. Validation of inertial measurement units for upper body kinematics. J. Appl. Biomech. 2017, 33, 227–232. [Google Scholar] [CrossRef]
- Mavor, M.P.; Ross, G.B.; Clouthier, A.L.; Karakolis, T.; Graham, R.B. Validation of an IMU suit for military-based tasks. Sensors 2020, 20, 4280. [Google Scholar] [CrossRef]
- Ertzgaard, P.; Öhberg, F.; Gerdle, B.; Grip, H. A new way of assessing arm function in activity using kinematic Exposure Variation Analysis and portable inertial sensors–A validity study. Man. Ther. 2016, 21, 241–249. [Google Scholar] [CrossRef]
- Fantozzi, S.; Giovanardi, A.; Magalhães, F.A.; Di Michele, R.; Cortesi, M.; Gatta, G. Assessment of three-dimensional joint kinematics of the upper limb during simulated swimming using wearable inertial-magnetic measurement units. J. Sports Sci. 2016, 34, 1073–1080. [Google Scholar] [CrossRef]
- Kumar, Y.; Yen, S.-C.; Tay, A.; Lee, W.; Gao, F.; Zhao, Z.; Li, J.; Hon, B.; Xu, T.T.-M.; Cheong, A. Wireless wearable range-of-motion sensor system for upper and lower extremity joints: A validation study. Healthc. Technol. Lett. 2015, 2, 12–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mjøsund, H.L.; Boyle, E.; Kjaer, P.; Mieritz, R.M.; Skallgård, T.; Kent, P. Clinically acceptable agreement between the ViMove wireless motion sensor system and the Vicon motion capture system when measuring lumbar region inclination motion in the sagittal and coronal planes. BMC Musculoskelet. Disord. 2017, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Goreham, J.A.; MacLean, K.F.; Ladouceur, M. The validation of a low-cost inertial measurement unit system to quantify simple and complex upper-limb joint angles. J. Biomech. 2022, 134, 111000. [Google Scholar] [CrossRef] [PubMed]
- Hanawa, H.; Hirata, K.; Miyazawa, T.; Sonoo, M.; Kubota, K.; Fujino, T.; Kokubun, T.; Kanemura, N. Validity of inertial measurement units in assessing segment angles and mechanical energies of elderly persons during sit-to-stand motion. In Proceedings of the 2019 58th Annual Conference of the Society of Instrument and Control Engineers of Japan (SICE), Hiroshima, Japan, 10–13 September 2019; pp. 936–940. [Google Scholar]
- Humadi, A.; Nazarahari, M.; Ahmad, R.; Rouhani, H. In-field instrumented ergonomic risk assessment: Inertial measurement units versus Kinect V2. Int. J. Ind. Ergon. 2021, 84, 103147. [Google Scholar] [CrossRef]
- Seel, T.; Raisch, J.; Schauer, T. IMU-based joint angle measurement for gait analysis. Sensors 2014, 14, 6891–6909. [Google Scholar] [CrossRef]
- Teufl, W.; Miezal, M.; Taetz, B.; Fröhlich, M.; Bleser, G. Validity of inertial sensor based 3D joint kinematics of static and dynamic sport and physiotherapy specific movements. PLoS ONE 2019, 14, e0213064. [Google Scholar] [CrossRef]
- Karatsidis, A.; Jung, M.; Schepers, H.M.; Bellusci, G.; de Zee, M.; Veltink, P.H.; Andersen, M.S. Musculoskeletal model-based inverse dynamic analysis under ambulatory conditions using inertial motion capture. Med. Eng. Phys. 2019, 65, 68–77. [Google Scholar] [CrossRef]
- Benoit, D.L.; Damsgaard, M.; Andersen, M.S. Surface marker cluster translation, rotation, scaling and deformation: Their contribution to soft tissue artefact and impact on knee joint kinematics. J. Biomech. 2015, 48, 2124–2129. [Google Scholar] [CrossRef]
- Schiefer, C.; Kraus, T.; Ellegast, R.P.; Ochsmann, E. A technical support tool for joint range of motion determination in functional diagnostics-an inter-rater study. J. Occup. Med. Toxicol. 2015, 10, 16. [Google Scholar] [CrossRef]
- Bouvier, B.; Duprey, S.; Claudon, L.; Dumas, R.; Savescu, A. Upper limb kinematics using inertial and magnetic sensors: Comparison of sensor-to-segment calibrations. Sensors 2015, 15, 18813–18833. [Google Scholar] [CrossRef]
- Nüesch, C.; Roos, E.; Pagenstert, G.; Mündermann, A. Measuring joint kinematics of treadmill walking and running: Comparison between an inertial sensor based system and a camera-based system. J. Biomech. 2017, 57, 32–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, H.; Hou, B.; Lin, Z.; Guo, M. Modeling and compensation of random drift of MEMS gyroscopes based on least squares support vector machine optimized by chaotic particle swarm optimization. Sensors 2017, 17, 2335. [Google Scholar] [CrossRef] [PubMed]
- Xiong, P.; He, K.; Wu, E.Q.; Zhu, L.-M.; Song, A.; Liu, P.X. Human-Exploratory-Procedure-Based Hybrid Measurement Fusion for Material Recognition. IEEE/ASME Trans. Mechatron. 2021, 27, 1093–1104. [Google Scholar] [CrossRef]
- Zheng, W.; Liu, H.; Sun, F. Lifelong visual-tactile cross-modal learning for robotic material perception. IEEE Trans. Neural Netw. Learn. Syst. 2020, 32, 1192–1203. [Google Scholar] [CrossRef]
- Liu, H.; Guo, D.; Zhang, X.; Zhu, W.; Fang, B.; Sun, F. Toward image-to-tactile cross-modal perception for visually impaired people. IEEE Trans. Autom. Sci. Eng. 2020, 18, 521–529. [Google Scholar] [CrossRef]
- Xiong, P.; Liao, J.; Zhou, M.; Song, A.; Liu, P.X. Deeply Supervised Subspace Learning for Cross-Modal Material Perception of Known and Unknown Objects. IEEE Trans. Ind. Inform. 2022, 1–10. [Google Scholar] [CrossRef]




| Variable | Validity | Reliability | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Degree of Validity | CMC | RMSE (°) | Pearson’s r | R2 | LOA (°) | Degree of Reliability | ICC (Intrasession) | ICC (Intersession) | CMC (Intersession) | |||
| Shoulder | flexion | Fast | excellent | 0.99 | 8.8 | 0.99 | 0.99 | 19.3 ± 11.2 | excellent | 0.98 | 0.99 | 0.98 |
| Slow | excellent | 0.98 | 9.2 | 0.99 | 0.99 | 20.0 ± 13.4 | excellent | 0.98 | 0.99 | 0.98 | ||
| extension | Fast | excellent | 0.95 | 4.1 | 0.98 | 0.97 | 9.1 ± 10.6 | excellent | 0.92 | 0.95 | 0.89 | |
| Slow | excellent | 0.96 | 3.4 | 0.98 | 0.97 | 7.3 ± 10.5 | excellent | 0.94 | 0.96 | 0.88 | ||
| adduction | Fast | moderate | 0.73 | 8.4 | 0.84 | 0.75 | 8.5 ± 10.9 | good | 0.81 | 0.84 | 0.75 | |
| Slow | moderate | 0.73 | 7.6 | 0.85 | 0.77 | 6.8 ± 13.1 | good | 0.82 | 0.79 | 0.77 | ||
| abduction | Fast | good | 0.98 | 11.1 | 0.98 | 0.98 | 10.5 ± 14.3 | excellent | 0.98 | 0.98 | 0.98 | |
| Slow | good | 0.98 | 11.4 | 0.99 | 0.98 | 9.3 ± 17.1 | excellent | 0.98 | 0.98 | 0.98 | ||
| internal rotation | Fast | excellent | 0.92 | 9.3 | 0.98 | 0.96 | 18.8 ± 14.4 | excellent | 0.95 | 0.94 | 0.84 | |
| Slow | excellent | 0.90 | 7.4 | 0.98 | 0.97 | 17.8 ± 10.2 | excellent | 0.90 | 0.92 | 0.85 | ||
| external rotation | Fast | excellent | 0.91 | 8.9 | 0.98 | 0.98 | 22.7 ± 23.6 | excellent | 0.96 | 0.96 | 0.91 | |
| Slow | excellent | 0.91 | 8.1 | 0.99 | 0.97 | 19.7 ± 19.7 | excellent | 0.93 | 0.97 | 0.93 | ||
| Elbow | flexion | Fast | excellent | 0.98 | 8.8 | 0.98 | 0.98 | 1.3 ± 7.2 | excellent | 0.97 | 0.97 | 0.94 |
| Slow | excellent | 0.98 | 8.7 | 0.99 | 0.99 | 7.9 ± 6.5 | excellent | 0.98 | 0.97 | 0.95 | ||
| extension | Fast | good | 0.78 | 6.0 | 0.96 | 0.93 | 5.5 ± 8.5 | good | 0.78 | 0.78 | 0.75 | |
| Slow | good | 0.81 | 5.8 | 0.95 | 0.92 | 5.1 ± 7.2 | good | 0.78 | 0.79 | 0.75 | ||
| forearm pronation | Fast | excellent | 0.96 | 7.6 | 0.99 | 0.98 | 1.9 ± 25.2 | good | 0.91 | 0.92 | 0.88 | |
| Slow | excellent | 0.96 | 7.2 | 0.99 | 0.99 | 0.2 ± 23.8 | excellent | 0.91 | 0.94 | 0.87 | ||
| forearm supination | Fast | excellent | 0.95 | 8.6 | 0.97 | 0.95 | 1.9 ± 24.4 | good | 0.83 | 0.81 | 0.83 | |
| Slow | excellent | 0.95 | 7.8 | 0.97 | 0.95 | 1.1 ± 25.8 | good | 0.77 | 0.84 | 0.81 | ||
| Thorax | flexion | Fast | excellent | 0.96 | 4.2 | 0.97 | 0.96 | −4.9 ± 10.2 | good | 0.88 | 0.98 | 0.95 |
| Slow | excellent | 0.96 | 4.3 | 0.97 | 0.96 | −4.4 ± 7.7 | excellent | 0.96 | 0.97 | 0.95 | ||
| extension | Fast | excellent | 0.94 | 3.3 | 0.97 | 0.96 | −2.3 ± 5.5 | excellent | 0.93 | 0.96 | 0.93 | |
| Slow | excellent | 0.94 | 3.6 | 0.97 | 0.97 | −0.4 ± 6.1 | excellent | 0.96 | 0.96 | 0.91 | ||
| lateral flexion | Fast | excellent | 0.94 | 3.6 | 0.99 | 0.99 | 5.9 ± 8.3 | good | 0.95 | 0.97 | 0.94 | |
| Slow | excellent | 0.94 | 4.1 | 0.99 | 0.99 | 6.1 ± 8.6 | excellent | 0.96 | 0.95 | 0.92 | ||
| rotation | Fast | excellent | 0.94 | 3.9 | 0.99 | 0.98 | 5.0 ± 8.6 | good | 0.91 | 0.95 | 0.92 | |
| Slow | excellent | 0.90 | 3.8 | 0.99 | 0.98 | 4.4 ± 6.9 | excellent | 0.93 | 0.94 | 0.86 | ||
| Variable | Validity | Reliability | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Degree of Validity | CMC | RMSE (°) | Pearson’s r | R2 | LOA (°) | Degree of Reliability | ICC (Intrasession) | ICC (Intersession) | CMC (Intersession) | |||
| Shoulder | flexion/ extension | Fast | excellent | 0.98 | 7.5 | 0.98 | 0.96 | 25.9 ± 6.4 | excellent | 0.92 | 0.97 | 0.96 |
| Slow | excellent | 0.98 | 8.8 | 0.97 | 0.96 | 17.9 ± 11.9 | excellent | 0.95 | 0.97 | 0.97 | ||
| adduction/ abduction | Fast | good | 0.89 | 5.0 | 0.88 | 0.80 | −12.6 ± 16.0 | good | 0.87 | 0.87 | 0.88 | |
| Slow | good | 0.89 | 6.8 | 0.90 | 0.81 | −11.3 ± 13.6 | good | 0.86 | 0.86 | 0.84 | ||
| internal/ external rotation | Fast | good | 0.88 | 9.0 | 0.87 | 0.79 | −13.0 ± 15.9 | good | 0.87 | 0.85 | 0.82 | |
| Slow | good | 0.88 | 8.2 | 0.86 | 0.79 | −11.5 ± 17.7 | good | 0.89 | 0.87 | 0.86 | ||
| Elbow | flexion/ extension | Fast | good | 0.95 | 12.3 | 0.97 | 0.95 | 27.8 ± 18.8 | good | 0.86 | 0.92 | 0.89 |
| Slow | good | 0.92 | 12.5 | 0.95 | 0.94 | 27.1 ± 16.1 | excellent | 0.90 | 0.95 | 0.95 | ||
| pronation/ supination | Fast | excellent | 0.91 | 9.3 | 0.89 | 0.81 | 8.3 ± 6.9 | good | 0.90 | 0.88 | 0.84 | |
| Slow | excellent | 0.92 | 9.5 | 0.90 | 0.81 | 6.6 ± 7.2 | good | 0.88 | 0.91 | 0.79 | ||
| Thorax | flexion/ extension | Fast | excellent | 0.96 | 10.0 | 0.97 | 0.97 | −6.2 ± 21.7 | excellent | 0.90 | 0.96 | 0.95 |
| Slow | excellent | 0.96 | 10.4 | 0.97 | 0.97 | −3.7 ± 24.8 | excellent | 0.94 | 0.97 | 0.96 | ||
| lateral flexion | Fast | excellent | 0.91 | 2.2 | 0.91 | 0.84 | 2.5 ± 5.1 | good | 0.89 | 0.93 | 0.87 | |
| Slow | excellent | 0.93 | 2.1 | 0.92 | 0.85 | 1.5 ± 4.2 | excellent | 0.90 | 0.93 | 0.92 | ||
| rotation | Fast | excellent | 0.93 | 1.9 | 0.93 | 0.87 | −0.7 ± 1.3 | good | 0.88 | 0.96 | 0.94 | |
| Slow | excellent | 0.95 | 2.1 | 0.95 | 0.91 | −0.2 ± 2.3 | good | 0.86 | 0.93 | 0.89 | ||
| CMC | Pearson’s r | R2 | RMSE | Bias | |
|---|---|---|---|---|---|
| Task complexities | |||||
| Simple task | 0.92 ± 0.04 | 0.97 ± 0.03 | 0.96 ± 0.04 | 6.38 ± 2.29 | 7.79 ± 6.18 |
| Complex task | 0.93 ± 0.03 | 0.93 ± 0.04 | 0.88 ± 0.07 | 7.35 ± 3.74 | 11.05 ± 9.52 |
| p value | 0.838 | 0.029 | 0.015 | 0.459 | 0.363 |
| Effect size of Cohen’s d | 0.075 | 0.969 | 1.14 | 0.277 | 0.344 |
| Movement speeds | |||||
| Fast speed | 0.93 ± 0.03 | 0.95 ± 0.03 | 0.91 ± 0.05 | 6.82 ± 2.63 | 10.08 ± 6.71 |
| Slow speed | 0.93 ± 0.03 | 0.94 ± 0.02 | 0.92 ± 0.04 | 6.91 ± 2.53 | 8.77 ± 6.33 |
| p value | 0.712 | 0.474 | 0.150 | 0.691 | 0.046 |
| Effect size of Cohen’s d | 0.136 | 0.268 | 0.572 | 0.146 | 0.855 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, Y.; Tao, K.; Chen, Q.; Tian, Y.; Sun, L. A Comprehensive Analysis of the Validity and Reliability of the Perception Neuron Studio for Upper-Body Motion Capture. Sensors 2022, 22, 6954. https://doi.org/10.3390/s22186954
Wu Y, Tao K, Chen Q, Tian Y, Sun L. A Comprehensive Analysis of the Validity and Reliability of the Perception Neuron Studio for Upper-Body Motion Capture. Sensors. 2022; 22(18):6954. https://doi.org/10.3390/s22186954
Chicago/Turabian StyleWu, Yiwei, Kuan Tao, Qi Chen, Yinsheng Tian, and Lixin Sun. 2022. "A Comprehensive Analysis of the Validity and Reliability of the Perception Neuron Studio for Upper-Body Motion Capture" Sensors 22, no. 18: 6954. https://doi.org/10.3390/s22186954