
Wearable Blood Pressure Sensing Based on Transmission Coefficient Scattering for Microstrip Patch Antennas


Abstract
:1. Introduction
2. Background
3. Materials and Methods
3.1. Theoretical Equations
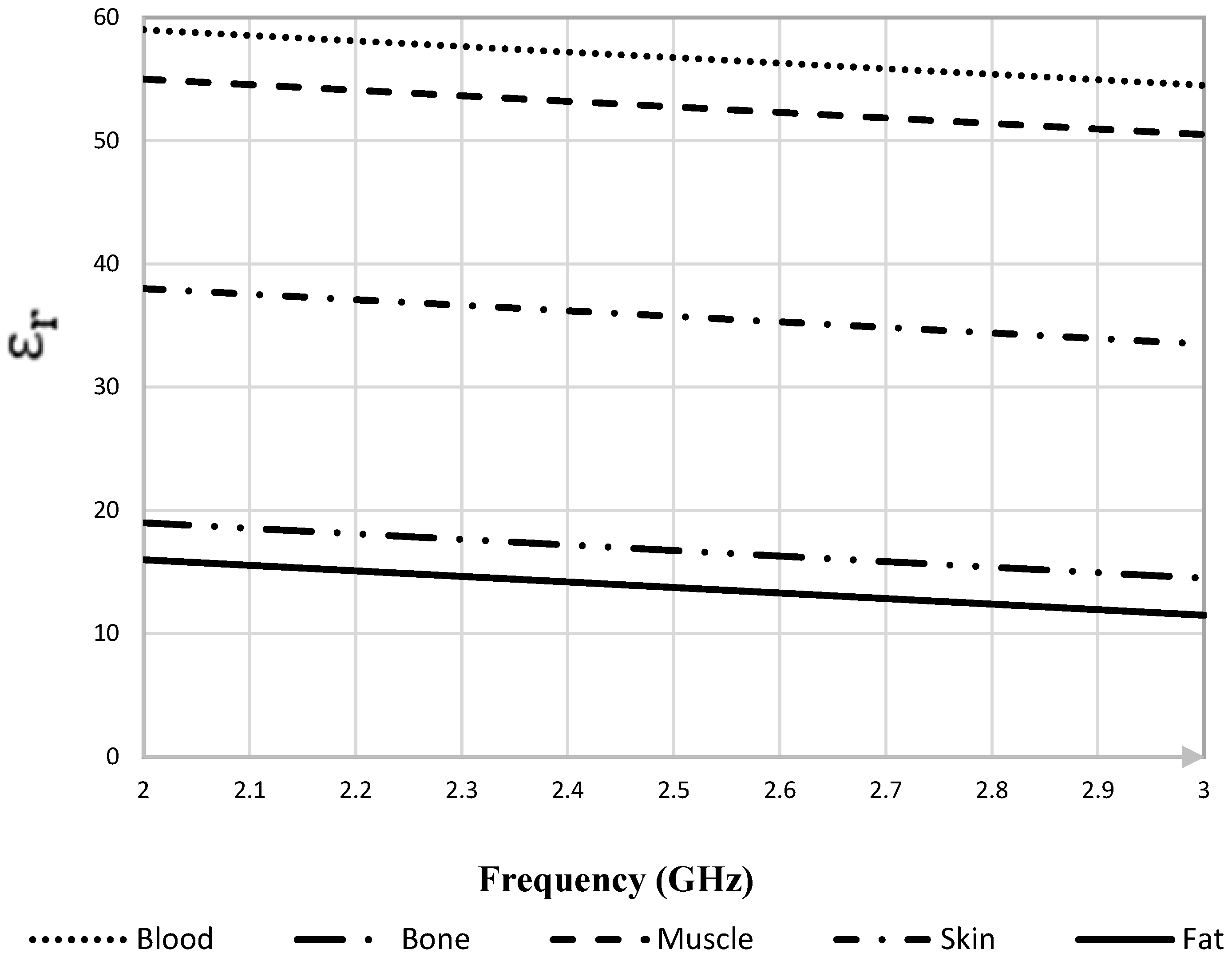
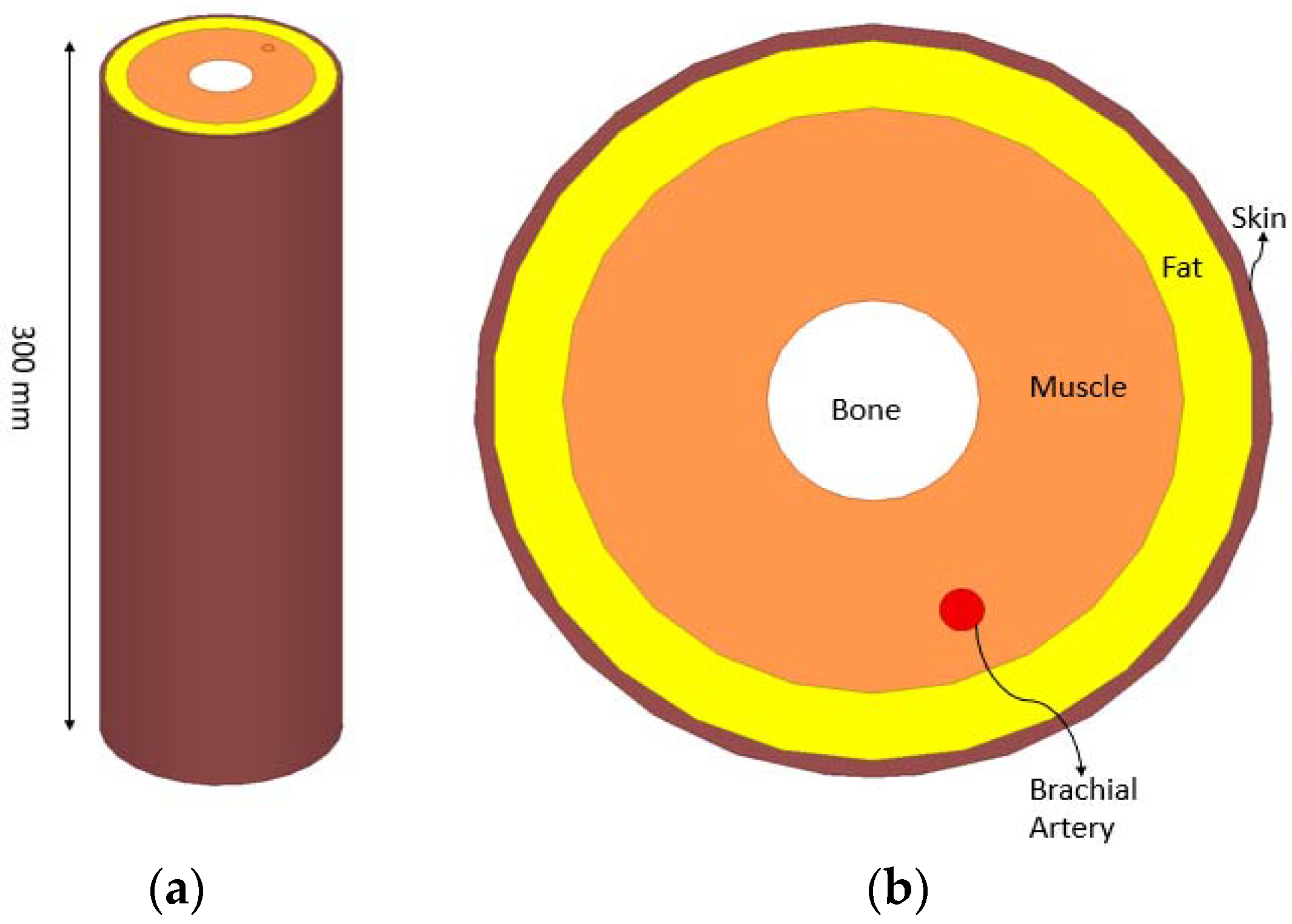
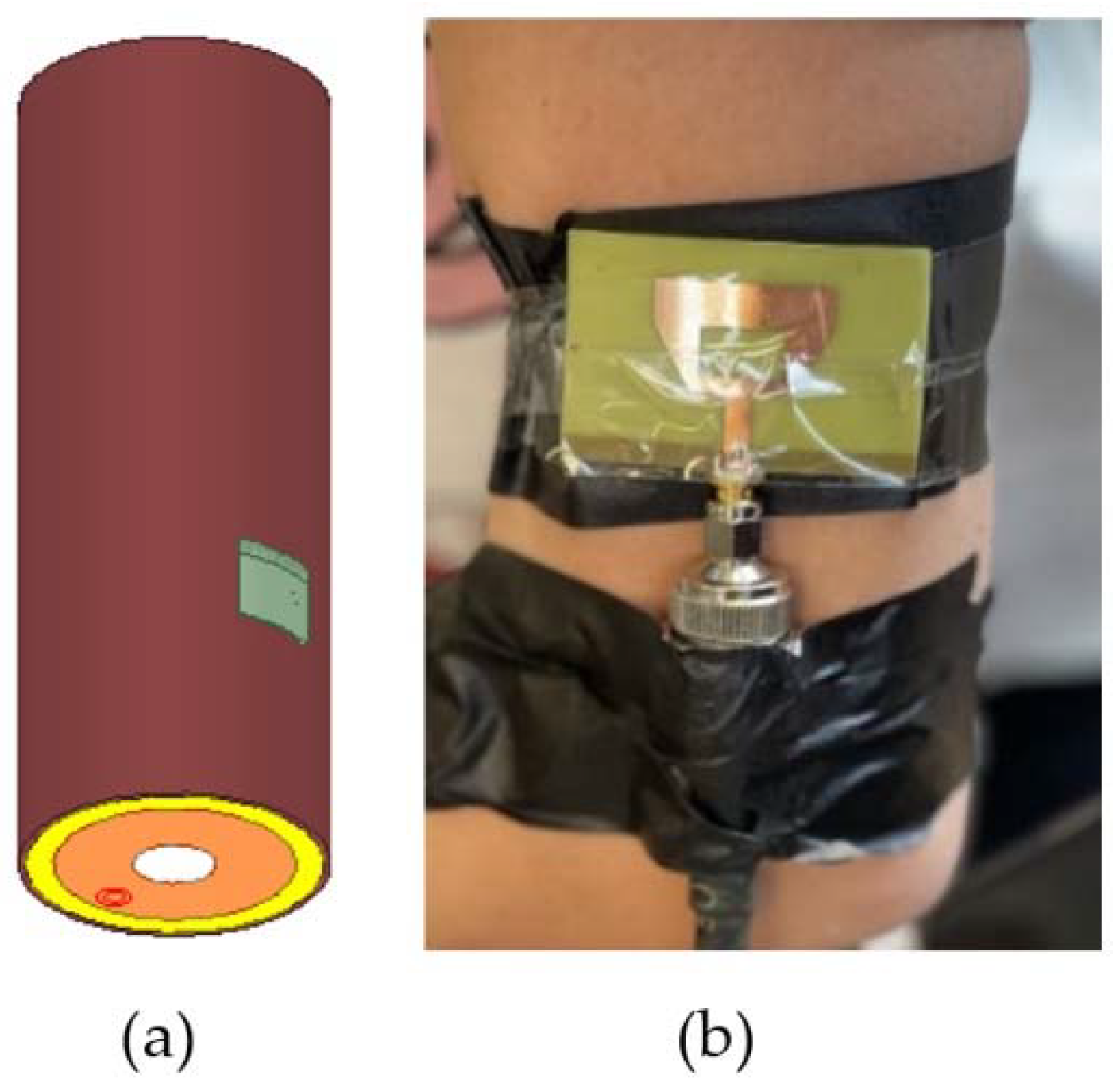
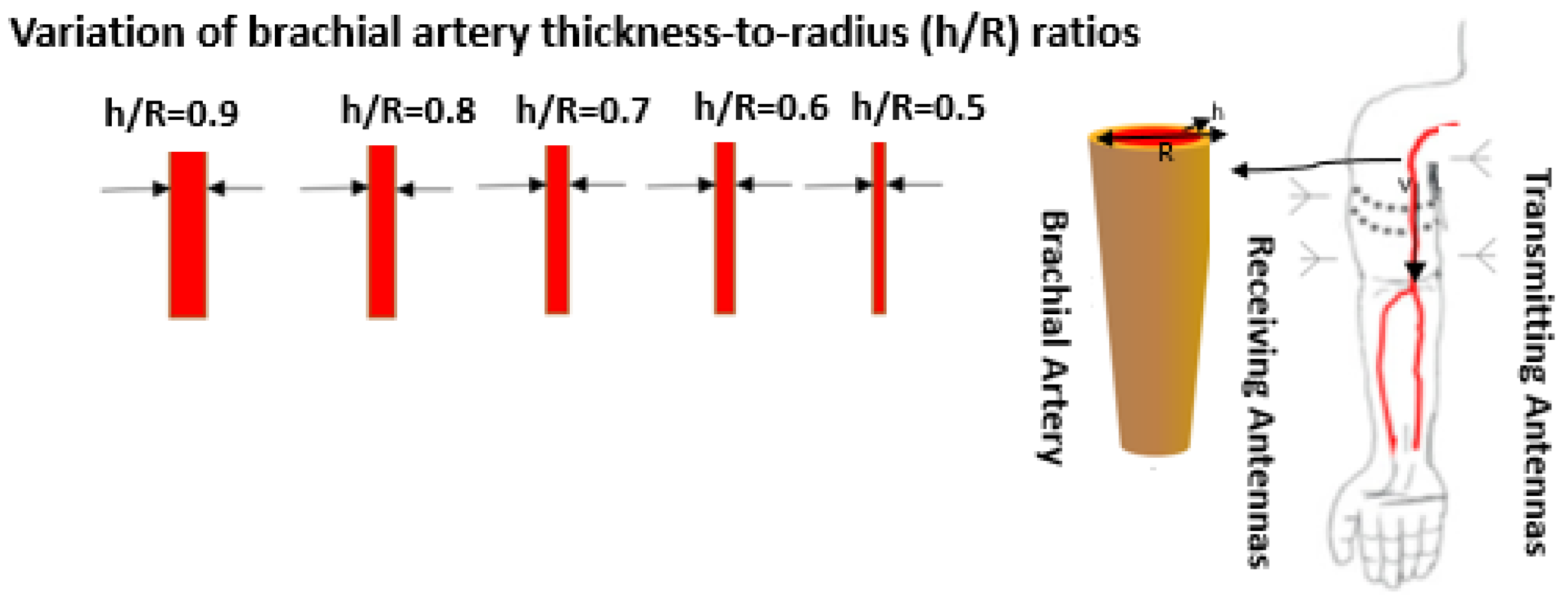
3.2. The Human Arm Model
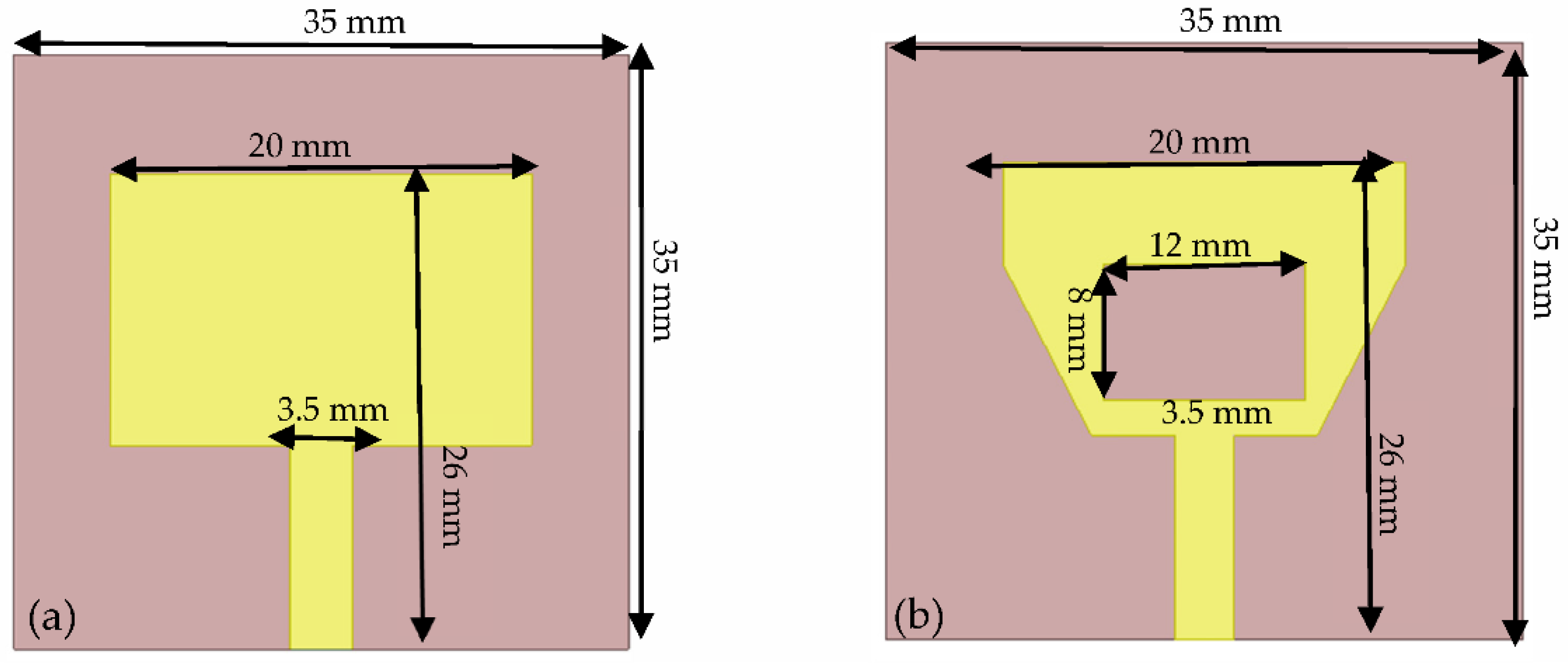
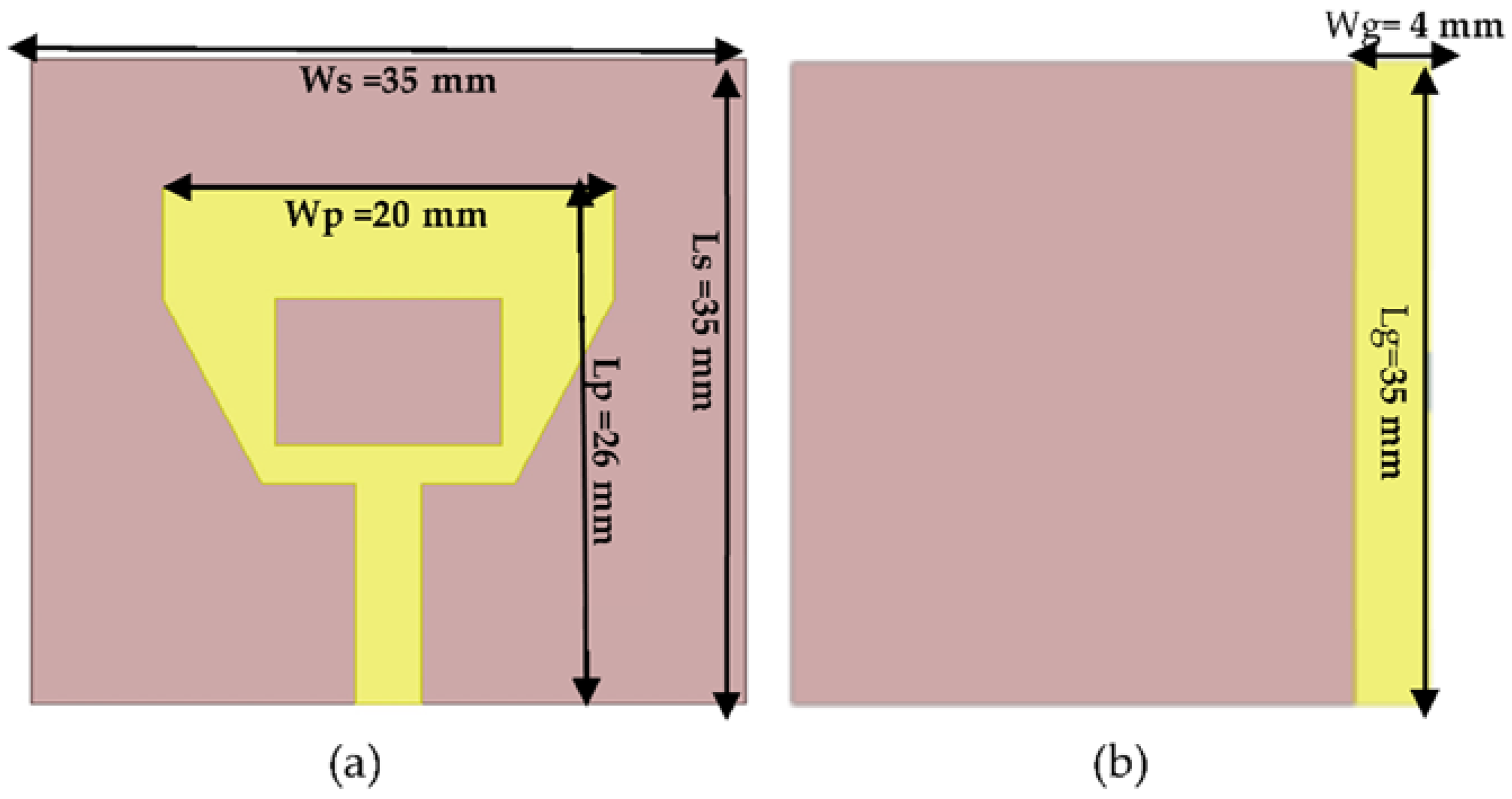
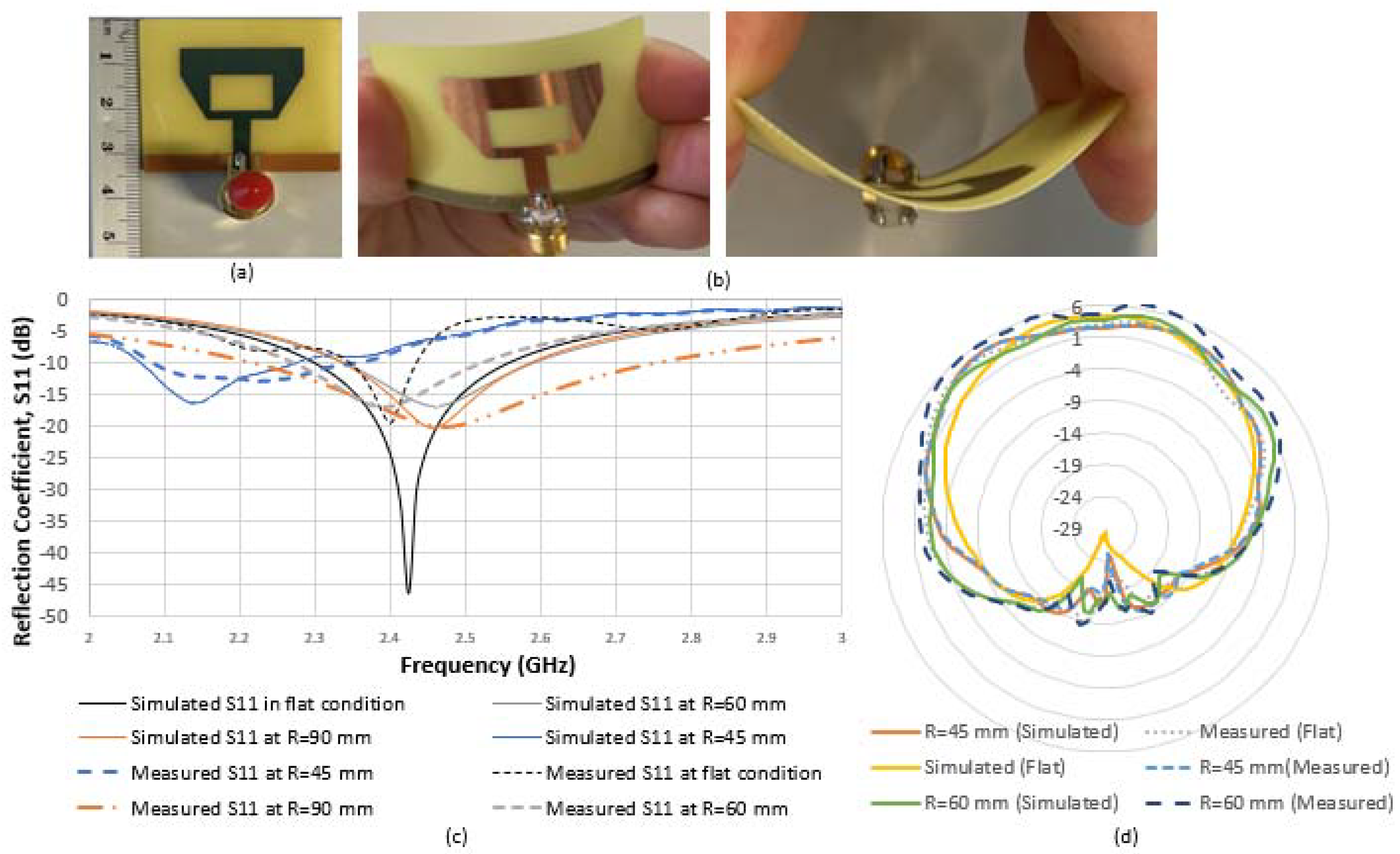
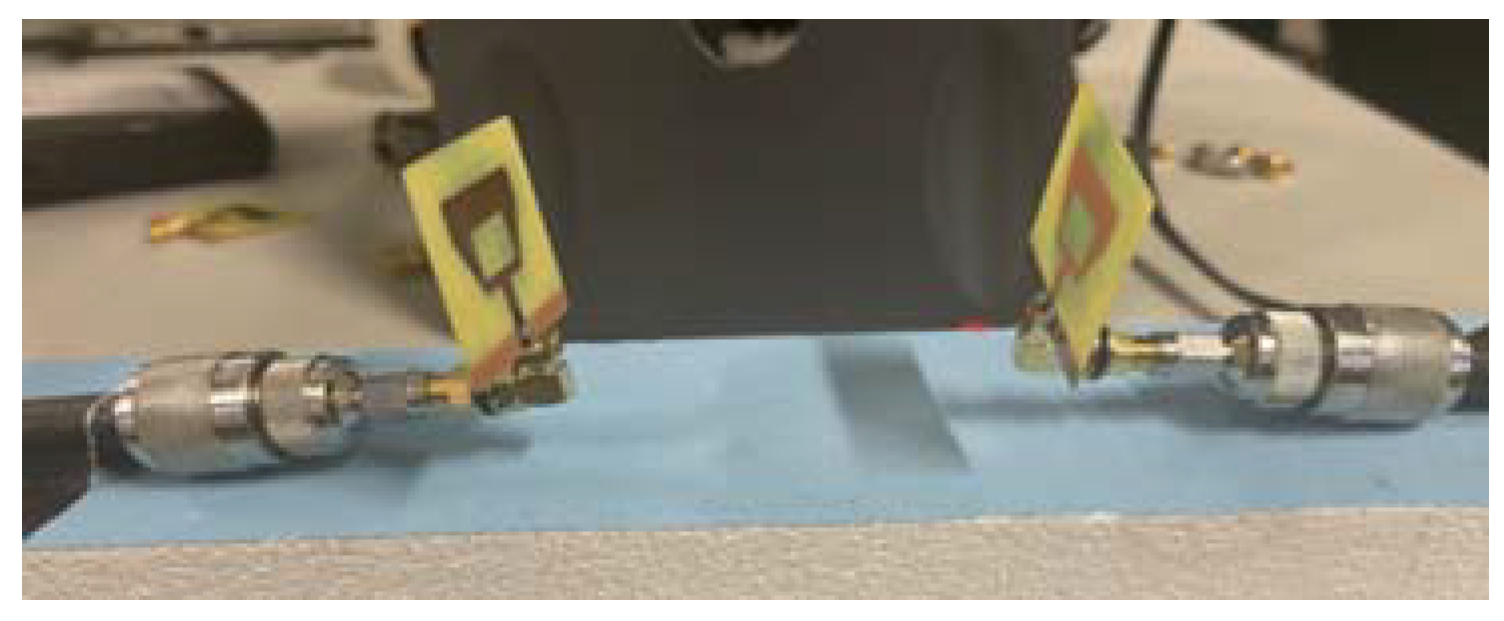
3.3. Design of the Proposed Microstrip Patch Antenna
3.4. The Proposed Blood Pressure Determination Method
4. Results
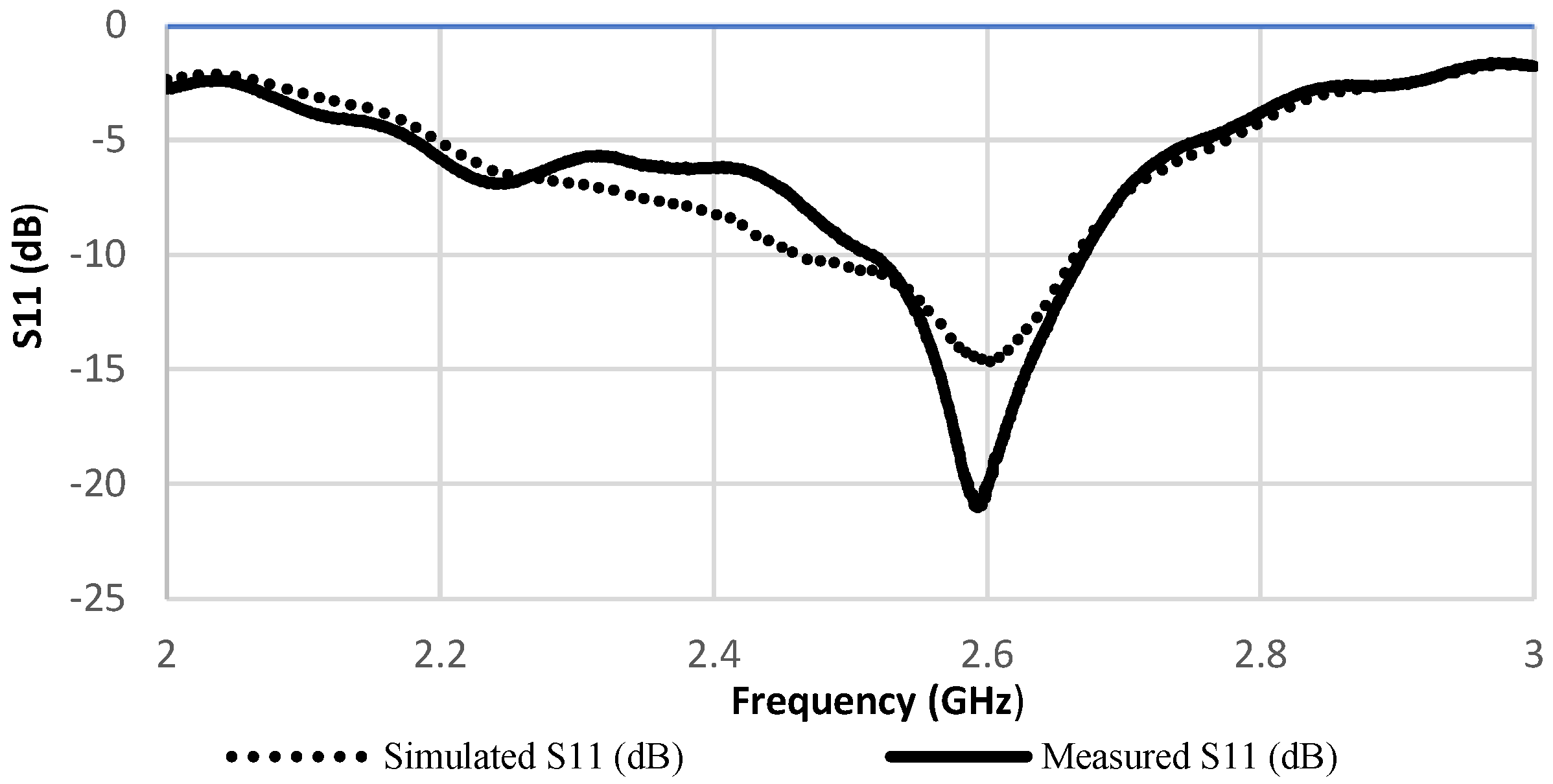
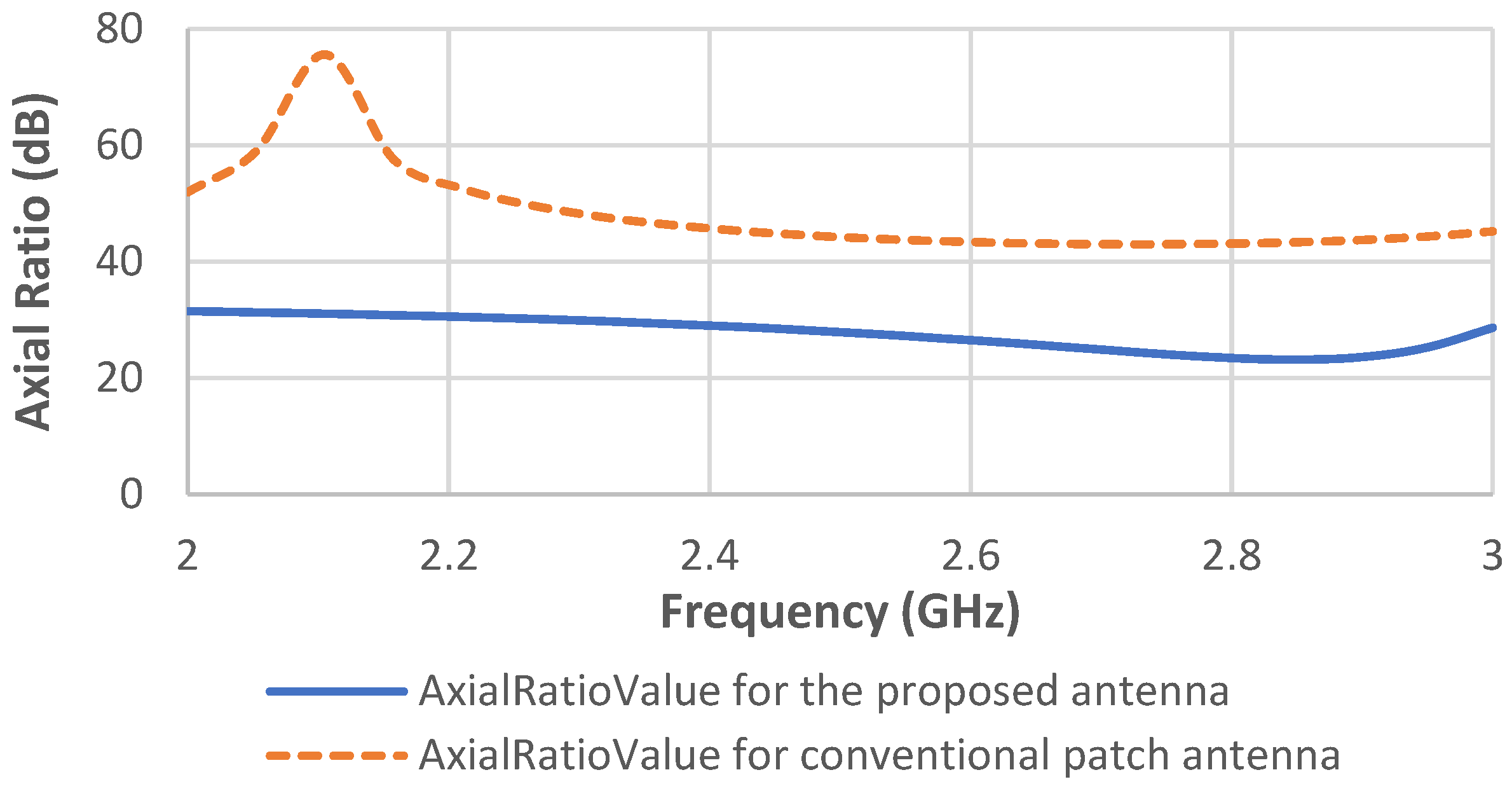
4.1. Transmission Coefficient Scattering Parameters of Antennas
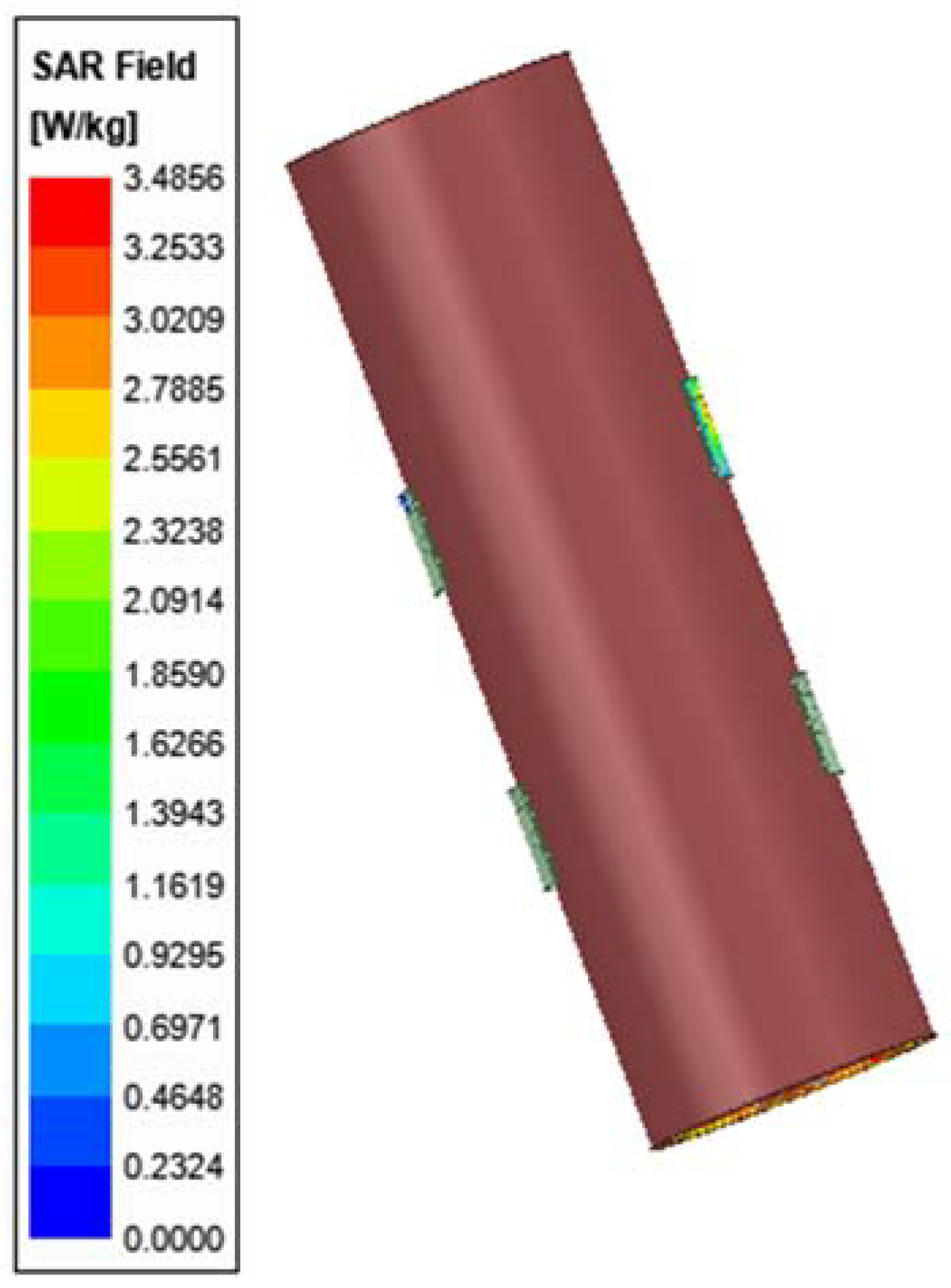
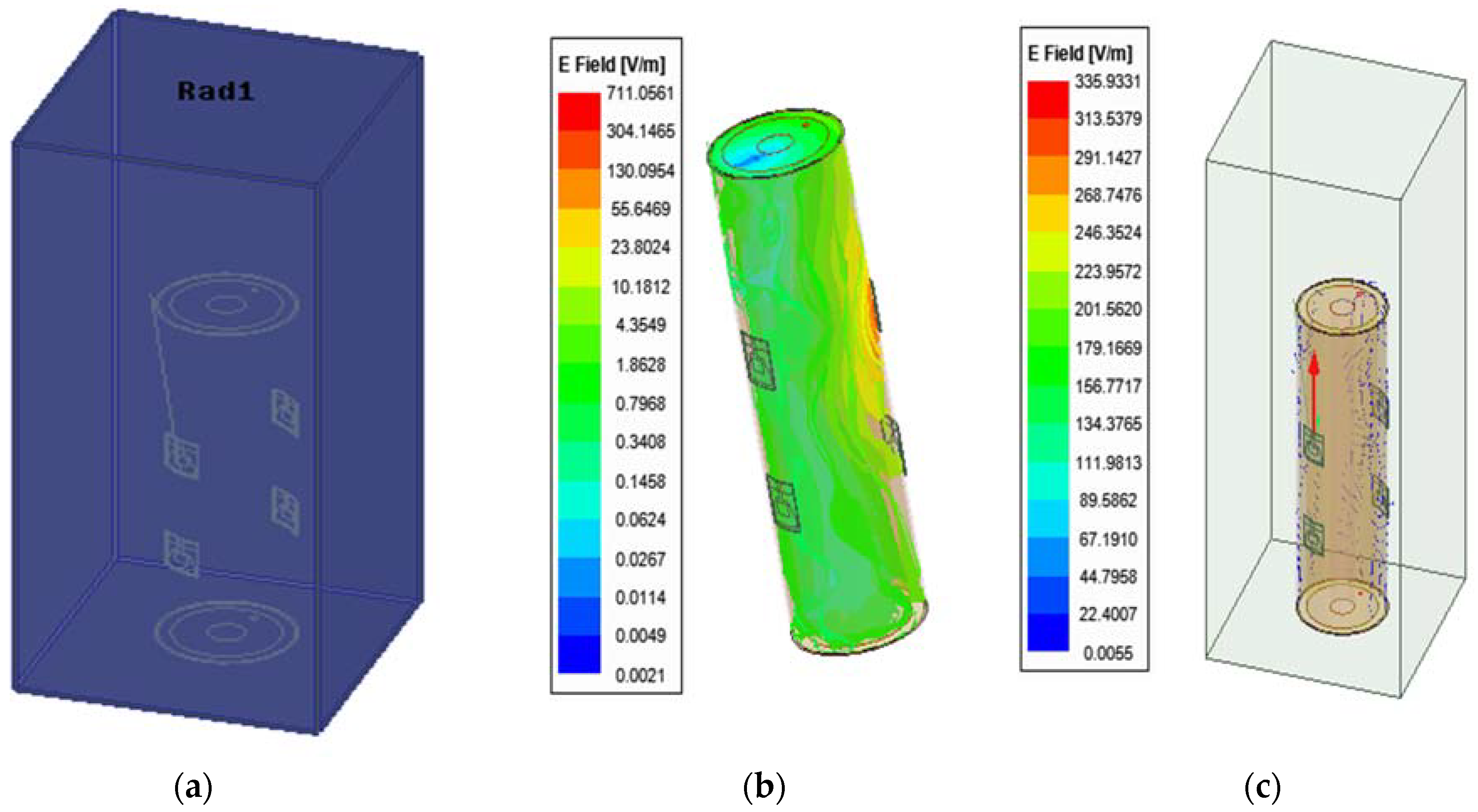
4.2. Electric Field Distribution
4.3. Measuring Transmission Coefficient Scattering Parameter and Computing Blood Pressure
- The time shift delay shown in Figure 14 between the two waveforms of both sensors is used to estimate PTT at different artery thickness to radius coefficients.
- The transmission coefficient waveforms between the two pairs of antennas are noted through three main simulations of brachial artery h/R variation for the same human arm model, as shown in Figure 15.
- 3.
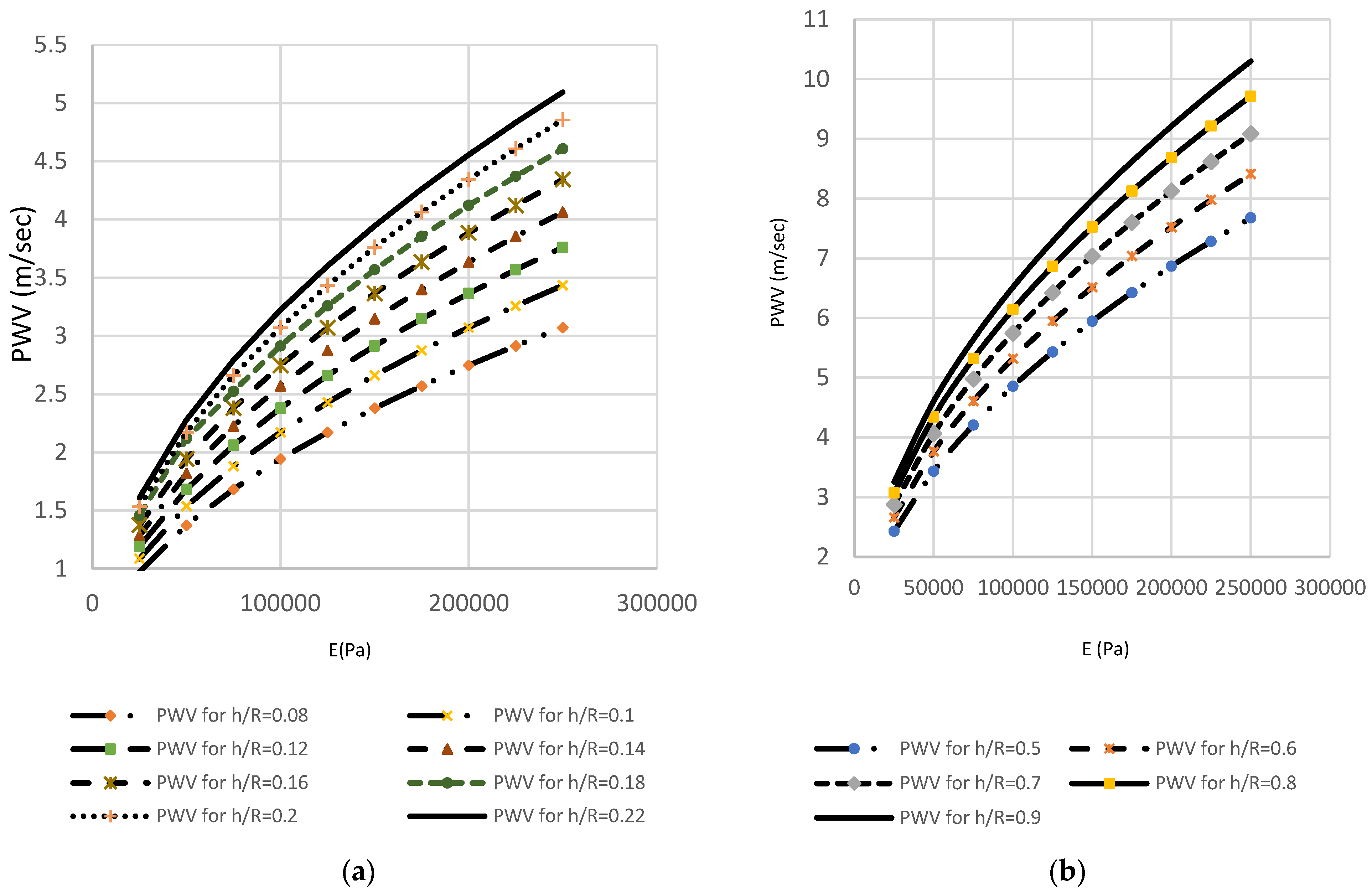
- The distance (L) between the two sensors allows calculation of PWV as shown in Figure 16. After PTT estimates were extracted as the time difference between proximal and distal transmission waveforms between the two pair of sensors presented previously in Figure 8, the Bramwell–Hill formula was applied to compute the PWV from the distance and pulse transit time (PTT) as shown in Figure 11. Pulse transit time is, in turn, estimated by acquiring proximal and distal arterial waveforms from the two sites and then detecting the foot-to-foot time delay between the waveforms [26,27,28,29]. The PWV-PTT relationship is noted in the three different brachial artery h/R ratio changes. The arterial thickness-to-radius ratio varies with the blood vessel volume variation, and thus, arterial BP. The accuracy of BP estimation is affected if the arterial diameter is ignored. Pulse wave velocity can be calculated based on the Bramwell–Hill formula and is therefore indirectly related to arterial distensibility as shown in Figure 16.
- 4.
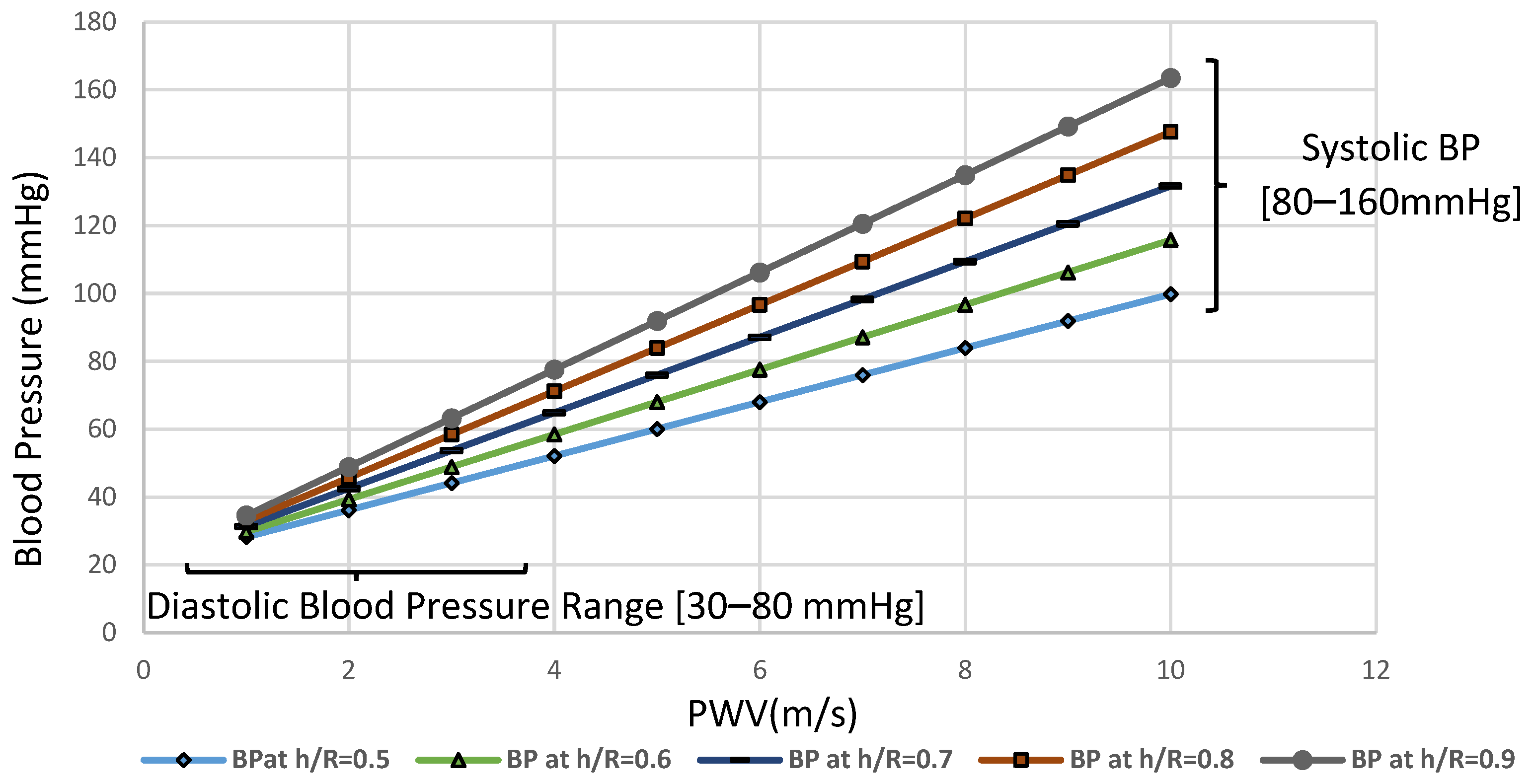
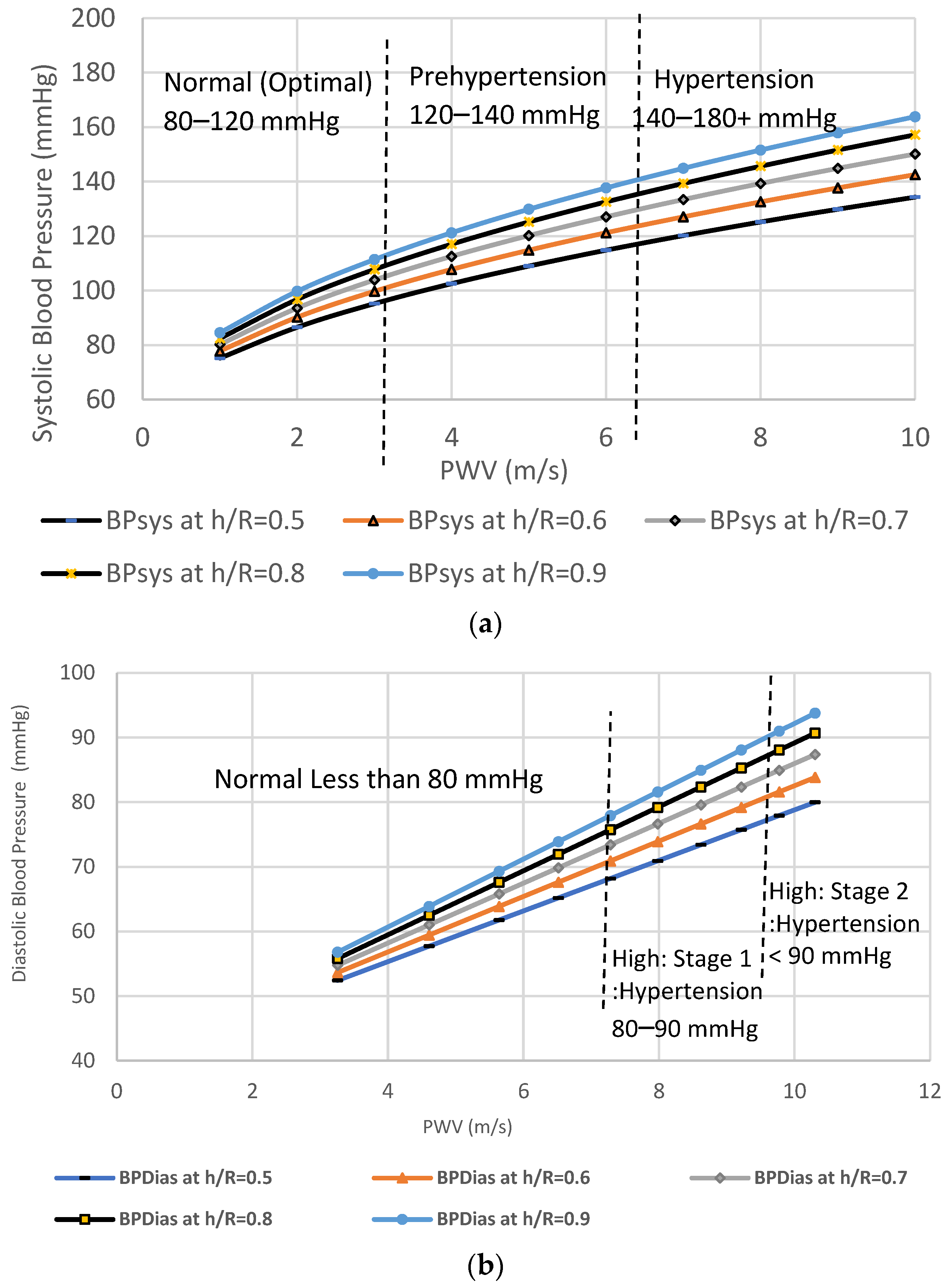
- Arterial distensibility is related to mean arterial pressure through regression analysis that reflect trends in blood pressure over the longer term as well as indicating abrupt changes in arterial systolic and diastolic blood pressures as shown in Figure 17.
- Whilst the PWV and PTT levels were set at normal values. The regression routine is shown in Figure 17 as a red dotted trend line of the mean BP, and it reveals the correlation of the systolic and diastolic blood pressure conditions. However, as the varying brachial artery coefficients increase, there is an increase in blood pressure levels [30,31,32]. For the change in transmission coefficient curves of brachial artery h/R ratio of 0.7, the systolic blood pressure decreased from 120 mmHg to 90 mmHg.
4.4. Comparing the Proposed Method to the Standard MK Model
- The MK model is established to compute the PWV. The PWV depends on the elastic properties of both arteries and blood;
- The arterial strain (E) can be computed from the Hughes Equation (Equation (2)) where the considered blood pressure range lies between 5 kPa to ~20 kPa;
- The h/R of the arteries are dynamic and can change up to 30% with changes in blood pressure;
- Table 6 shows that PWV varies directly with the arterial wall stiffness and is related to the wall thickness and elasticity and inversely related to arterial radius. It has been shown that any change in arterial radius is related to changes in instantaneous blood pressure.
5. Discussion & Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goonasekera, C.D. Current topic: Measurement and interpretation of Blood Pressure. Arch. Dis. Child. 2000, 82, 261–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meidert, A.S.; Saugel, B. Techniques for non-invasive monitoring of arterial blood pressure. Front. Med. 2018, 4, 231. [Google Scholar] [CrossRef] [PubMed]
- Wibmer, T.; Denner, C.; Fischer, C.; Schildge, B.; Rüdiger, S.; Kropf-Sanchen, C.; Rottbauer, W.; Schumann, C. Blood pressure monitoring during exercise: Comparison of pulse transit time and volume clamp methods. Blood Press. 2015, 24, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Hellbrück, H.; Ardelt, G.; Wegerich, P.; Gehring, H. Brachialis pulse Wave measurements with ultra-wide band and continuous wave radar, Photoplethysmography and Ultrasonic Doppler Sensors. Sensors 2020, 21, 165. [Google Scholar] [CrossRef]
- Balanis, C.A. Antenna theory: A review. Proc. IEEE 1992, 80, 7–23. [Google Scholar] [CrossRef]
- Yao, J.; Xu, C.C.; Mears, A.; Jaguan, M.; Tjuatja, S.; Huang, H. Pressure sensing using low-cost microstrip antenna sensor. In Sensors and Smart Structures Technologies for Civil, Mechanical, and Aerospace Systems 2015; International Society for Optics and Photonics: Bellingham, WA, USA, 2015. [Google Scholar]
- Kim, I.; Bhagat, Y.A. Towards development of a Mobile RF Doppler sensor for continuous heart rate variability and blood pressure monitoring. In Proceedings of the 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016. [Google Scholar]
- Wang, R.; Jia, W.; Mao, Z.-H.; Sclabassi, R.J.; Sun, M. Cuff-free blood pressure estimation using pulse transit time and heart rate. In Proceedings of the 12th International Conference on Signal Processing (ICSP), Hangzhou, China, 19–23 October 2014. [Google Scholar]
- Mukkamala, R.; Hahn, J.-O.; Inan, O.T.; Mestha, L.K.; Kim, C.-S.; Toreyin, H.; Kyal, S. Toward ubiquitous blood pressure monitoring via pulse transit time: Theory and practice. IEEE Trans. Biomed. Eng. 2015, 62, 1879–1901. [Google Scholar] [CrossRef] [Green Version]
- Huynh, T.; Jafari, R.; Chung, W.-Y. An accurate bioimpedance measurement system for Blood Pressure monitoring. Sensors 2018, 18, 2095. [Google Scholar] [CrossRef] [Green Version]
- Kathuria, N.; Seet, B.-C. 24 GHz flexible antenna for doppler radar-based human vital signs monitoring. Sensors 2021, 21, 3737. [Google Scholar] [CrossRef]
- Vallejo, M.; Recas, J.; del Valle, P.; Ayala, J. Accurate human tissue characterization for energy-efficient wireless on-body communications. Sensors 2013, 13, 7546–7569. [Google Scholar] [CrossRef]
- TMaruhashi; Soga, J.; Fujimura, N.; Idei, N.; Mikami, S.; Iwamoto, Y.; Iwamoto, A.; Kajikawa, M.; Higashi, Y. Brachial artery diameter as a marker for cardiovascular risk assessment: FMD-J Study. Atherosclerosis 2018, 268, 92–98. [Google Scholar] [CrossRef]
- Fantini, F.; Barletta, G.; Bene, R.D.; Lazzeri, C.; la Villa, G.; Franchi, F. Parallel increase in carotid, brachial and left ventricular cross-sectional areas in arterial hypertension. J. Hum. Hypertens. 1997, 11, 515–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abohmra, A.; Ramani, S.; Sharif, A.; Imran, M.A.; Abbasi, Q.; Ahmad, W. Novel flexible and wearable 2.4 GHz antenna for body-centric applications. In Proceedings of the 2019 IEEE Intl Conf on Dependable, Autonomic and Secure Computing, Intl Conf on Pervasive Intelligence and Computing, Intl Conf on Cloud and Big Data Computing, Intl Conf on Cyber Science and Technology Congress (DASC/PiCom/CBDCom/CyberSciTech), Fukuoka, Japan, 5–8 August 2019. [Google Scholar]
- Klemm, M.; Troester, G. EM energy absorption in the human body tissues due to UWB antennas. Prog. Electromagn. Res. 2006, 62, 261–280. [Google Scholar] [CrossRef] [Green Version]
- Murbach, M.; Neufeld, E.; Capstick, M.; Kainz, W.; Brunner, D.O.; Samaras, T.; Pruessmann, K.P.; Kuster, N. Thermal tissue damage model analyzed for different whole-body SAR and scan durations for standard body coils. Magn. Reson. Med. 2013, 71, 421–431. [Google Scholar] [CrossRef] [PubMed]
- C95.1-2019; IEEE Standard for Safety Levels with Respect to Human Exposure to Electric, Magnetic, and Electromagnetic Fields, 0 Hz to 300 GHz. (n.d.). IEEE: New York, NY, USA, 2019. [CrossRef]
- Ali, I.H.; Hamd, H.I.; Abdalla, A.I. Design and comparison of two types of antennas for SAR calculation in wireless applications. In Proceedings of the 2018 Advances in Science and Engineering Technology International Conferences (ASET), Dubai, Sharjah, Abu Dhabi, United Arab Emirates, 6 February–5 April 2018. [Google Scholar]
- Lin, H.D.; Lee, Y.S.; Chuang, B.N. Using dual-antenna nanosecond pulse near-field sensing technology for non-contact and continuous blood pressure measurement. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012. [Google Scholar]
- Ebrahim, M.P.; Heydari, F.; Wu, T.; Walker, K.; Joe, K.; Redoute, J.-M.; Yuce, M.R. Blood pressure estimation using on-body continuous wave radar and photoplethysmogram in various posture and exercise conditions. Sci. Rep. 2019, 9, 16346. [Google Scholar] [CrossRef] [PubMed]
- Semmler, L.; Weberruß, H.; Baumgartner, L.; Pirzer, R.; Oberhoffer-Fritz, R. Vascular diameter and intima-media thickness to diameter ratio values of the carotid artery in 642 healthy children. Eur. J. Pediatr. 2020, 180, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Chami, H.A.; Keyes, M.J.; Vita, J.A.; Mitchell, G.F.; Larson, M.G.; Fan, S.; Vasan, R.S.; O’Connor, G.T.; Benjamin, E.J.; Gottlieb, D.J. Brachial artery diameter, blood flow and flow-mediated dilation in sleep-disordered breathing. Vasc. Med. 2009, 14, 351–360. [Google Scholar] [CrossRef]
- McEniery, C.M.; Cockcroft, J.R.; Roman, M.J.; Franklin, S.S.; Wilkinson, I.B. Central blood pressure: Current evidence and clinical importance. Eur. Heart J. 2014, 35, 1719–1725. [Google Scholar] [CrossRef] [Green Version]
- Holubkov, R.; Karas, R.H.; Pepine, C.J.; Rickens, C.R.; Reichek, N.; Rogers, W.J.; Sharaf, B.L.; Sopko, G.; Merz, C.N.B.; Kelsey, S.F.; et al. Large brachial artery diameter is associated with angiographic coronary artery disease in women. Am. Heart J. 2002, 143, 802–807. [Google Scholar] [CrossRef]
- Kachuee, M.; Kiani, M.M.; Mohammadzade, H.; Shabany, M. Cuff-less high-accuracy calibration-free blood pressure estimation using Pulse Transit Time. In Proceedings of the 2015 IEEE International Symposium on Circuits and Systems (ISCAS), Lisbon, Portugal, 24–27 May 2015. [Google Scholar]
- Xu, D.; Ryan, K.L.; Rickards, C.A.; Zhang, G.; Convertino, V.A.; Mukkamala, R. Improved pulse transit time estimation by system identification analysis of proximal and distal arterial waveforms. Am. J. Physiol.-Heart Circ. Physiol. 2011, 301, H1389–H1395. [Google Scholar] [CrossRef]
- Gao, M.; Cheng, H.-M.; Sung, S.-H.; Chen, C.-H.; Olivier, N.B.; Mukkamala, R. Estimation of pulse transit time as a function of blood pressure using a nonlinear arterial tube-load model. IEEE Trans. Biomed. Eng. 2017, 64, 1524–1534. [Google Scholar] [CrossRef]
- Ding, X.; Zhang, Y.-T. Pulse Transit Time technique for cuffless unobtrusive blood pressure measurement: From theory to algorithm. Biomed. Eng. Lett. 2019, 9, 37–52. [Google Scholar] [CrossRef] [PubMed]
- Said, M.A.; Eppinga, R.N.; Lipsic, E.; Verweij, N.; van der Harst, P. Relationship of arterial stiffness index and pulse pressure with cardiovascular disease and mortality. J. Am. Heart Assoc. 2018, 7, e007621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCall, C.; Rostosky, R.; Wiard, R.M.; Inan, O.T.; Giovangrandi, L.; Cuttino, C.M.; Kovacs, G.T. Noninvasive pulse transit time measurement for arterial stiffness monitoring in microgravity. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; Volume 4. [Google Scholar]
- Wagenseil, J.E.; Mecham, R.P. Elastin in large artery stiffness and hypertension. J. Cardiovasc. Transl. Res. 2012, 5, 264–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tissues | σ (S/m) | ρ (Kg/m3) | σmec (W/K/m) | |
|---|---|---|---|---|
| Skin | 40.93 | 0.89 | 1100 | 0.293 |
| Fat | 5.34 | 0.08 | 1100 | 0.201 |
| Muscle | 55.19 | 1.49 | 1850 | 0.46 |
| Bones | 12.36 | 0.15 | 1020 | 0.41 |
| Blood | 59.19 | 2.11 | 1000 | 0.505 |
| Parameter | Value (mm) |
|---|---|
| Ls | 35 |
| Ws | 35 |
| Lp | 26 |
| Wp | 20 |
| Lg | 35 |
| Wg | 4 |
| Cylindrical Bend [mm] | S11 [dB] at 2.4 GHz | Bandwidth (GHz) | ||
|---|---|---|---|---|
| Simulated | Measured | Simulated | Measured | |
| R = 0 | −47 | −20 | 0.25 | 0.15 |
| R = 45 | −17 | −13 | 0.2 | 0.25 |
| R = 60 | −17 | −19 | 0.25 | 0.22 |
| R = 75 | −20 | −20 | 0.25 | 0.5 |
| Power (mW) | SAR for 10 g (W/Kg) |
|---|---|
| 1000 | 1.4917 × 103 |
| 800 | 1.1933 × 103 |
| 600 | 25.222 |
| 400 | 16.334 |
| 200 | 10.089 |
| 100 | 5.044 |
| 50 | 3.89 |
| Parameters | Case 1: h/R = 0.5 | Case 2: h/R = 0.7 | Case 3: h/R = 0.9 |
|---|---|---|---|
| PTT (s) | 0.8–1.8 | 0.15–0.75 | 0.1–1.6 |
| PWV (m/s) | 2.7–6.2 | 6.5–11 | 3–13 |
| Mean BP | 60–120 | 50–110 | 50–140 |
| Systolic BP | 80–120 | 100–140 | 100–140 |
| Diastolic BP | 20–60 | 40–80 | 90–130 |
| Pulse Wave Velocity for Different Values of Different h/R Ratios | ||||||||
|---|---|---|---|---|---|---|---|---|
| E(kPa) | h/R = 0.08 | h/R = 0.1 | h/R = 0.12 | h/R = 0.14 | h/R = 0.16 | h/R = 0.18 | h/R = 0.2 | h/R = 0.22 |
| 25 | 0.971 | 1.086 | 1.190 | 1.285 | 1.374 | 1.457 | 1.536 | 1.611 |
| 50 | 1.374 | 1.536 | 1.682 | 1.817 | 1.943 | 2.117 | 2.172 | 2.278 |
| 75 | 1.682 | 1.881 | 2.060 | 2.225 | 2.379 | 2.523 | 2.660 | 2.790 |
| 100 | 1.943 | 2.172 | 2.379 | 2.570 | 2.747 | 2.914 | 3.071 | 3.221 |
| 125 | 2.172 | 2.428 | 2.660 | 2.873 | 3.071 | 3.258 | 3.434 | 3.602 |
| 150 | 2.379 | 2.660 | 2.914 | 3.147 | 3.365 | 3.569 | 3.762 | 3.945 |
| 175 | 2.570 | 2.873 | 3.147 | 3.400 | 3.634 | 3.855 | 4.063 | 4.261 |
| 200 | 2.747 | 3.071 | 3.365 | 3.634 | 3.885 | 4.121 | 4.344 | 4.556 |
| 225 | 2.914 | 3.258 | 3.569 | 3.855 | 4.121 | 4.371 | 4.607 | 4.832 |
| 250 | 3.071 | 3.434 | 3.762 | 4.063 | 4.344 | 4.607 | 4.856 | 5.093 |
| E (KPa) | h/R | PWV for h/R = 0.5 | PWV for h/R = 0.6 | PWV for h/R = 0.7 | PWV for h/R = 0.8 | PWV for h/R = 0.9 |
|---|---|---|---|---|---|---|
| 25 | 0.5 | 2.428 | 2.660 | 2.873 | 3.071 | 3.258 |
| 50 | 0.6 | 3.434 | 3.762 | 4.063 | 4.344 | 4.607 |
| 75 | 0.7 | 4.206 | 4.607 | 4.976 | 5.320 | 5.643 |
| 100 | 0.8 | 4.856 | 5.320 | 5.746 | 6.143 | 6.516 |
| 125 | 0.9 | 5.430 | 5.948 | 6.424 | 6.868 | 7.285 |
| 150 | 5.948 | 6.516 | 7.038 | 7.524 | 7.980 | |
| 175 | 6.424 | 7.038 | 7.602 | 8.126 | 8.619 | |
| 200 | 6.868 | 7.524 | 8.126 | 8.687 | 9.214 | |
| 225 | 7.285 | 7.980 | 8.619 | 9.214 | 9.773 | |
| 250 | 7.679 | 8.412 | 9.086 | 9.713 | 10.302 |
| Parameters | Case 1: h/R = 0.5 | Case 2: h/R = 0.7 | Case 3: h/R = 0.9 | |||
|---|---|---|---|---|---|---|
| Transmission Coefficient-PTT Method | Moens Korteweg Equation | Transmission Coefficient-PTT Method | Moens Korteweg Equations | Transmission Coefficient-PTT Method | Moens Korteweg Equation | |
| PTT (s) | 0.8–1.8 | - | 0.6–1.6 | - | 0.1–1.3 | - |
| PWV (m/s) | 2.7–6.2 | 2.5–7.5 | 6.5–11 | 3–9 | 3–13 | 3.5–10.5 |
| Mean BP | 60–120 | 30–100 | 50–110 | 30–130 | 70–140 | 40–160 |
| SBP | 80–120 | 80–130 | 100–140 | 80–150 | 100–140 | 90–165 |
| DBP | 20–60 | 55–80 | 50–90 | 55–85 | 50–90 | 55–95 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Abbasi, M.K.; Madi, M.; Jelinek, H.F.; Kabalan, K.Y. Wearable Blood Pressure Sensing Based on Transmission Coefficient Scattering for Microstrip Patch Antennas. Sensors 2022, 22, 3996. https://doi.org/10.3390/s22113996
El Abbasi MK, Madi M, Jelinek HF, Kabalan KY. Wearable Blood Pressure Sensing Based on Transmission Coefficient Scattering for Microstrip Patch Antennas. Sensors. 2022; 22(11):3996. https://doi.org/10.3390/s22113996
Chicago/Turabian StyleEl Abbasi, Mona K., Mervat Madi, Herbert F. Jelinek, and Karim Y. Kabalan. 2022. "Wearable Blood Pressure Sensing Based on Transmission Coefficient Scattering for Microstrip Patch Antennas" Sensors 22, no. 11: 3996. https://doi.org/10.3390/s22113996