
Perceptions of and Experiences with Consumer Sleep Technologies That Use Artificial Intelligence


Abstract
:1. Introduction
1.1. Aims
1.2. Significance
1.3. Current Use of Consumer Sleep Technology
1.4. Accuracy of Consumer Sleep Technology
1.5. Known Advantages and Disadvantages of Consumer Sleep Technology
2. Materials and Methods
2.1. Study Design
2.1.1. Consumer Sleep Technologies That Use Artificial Intelligence
Head-Mounted Devices
Tracking Pads
Standalone Mobile Applications
Responsive Devices
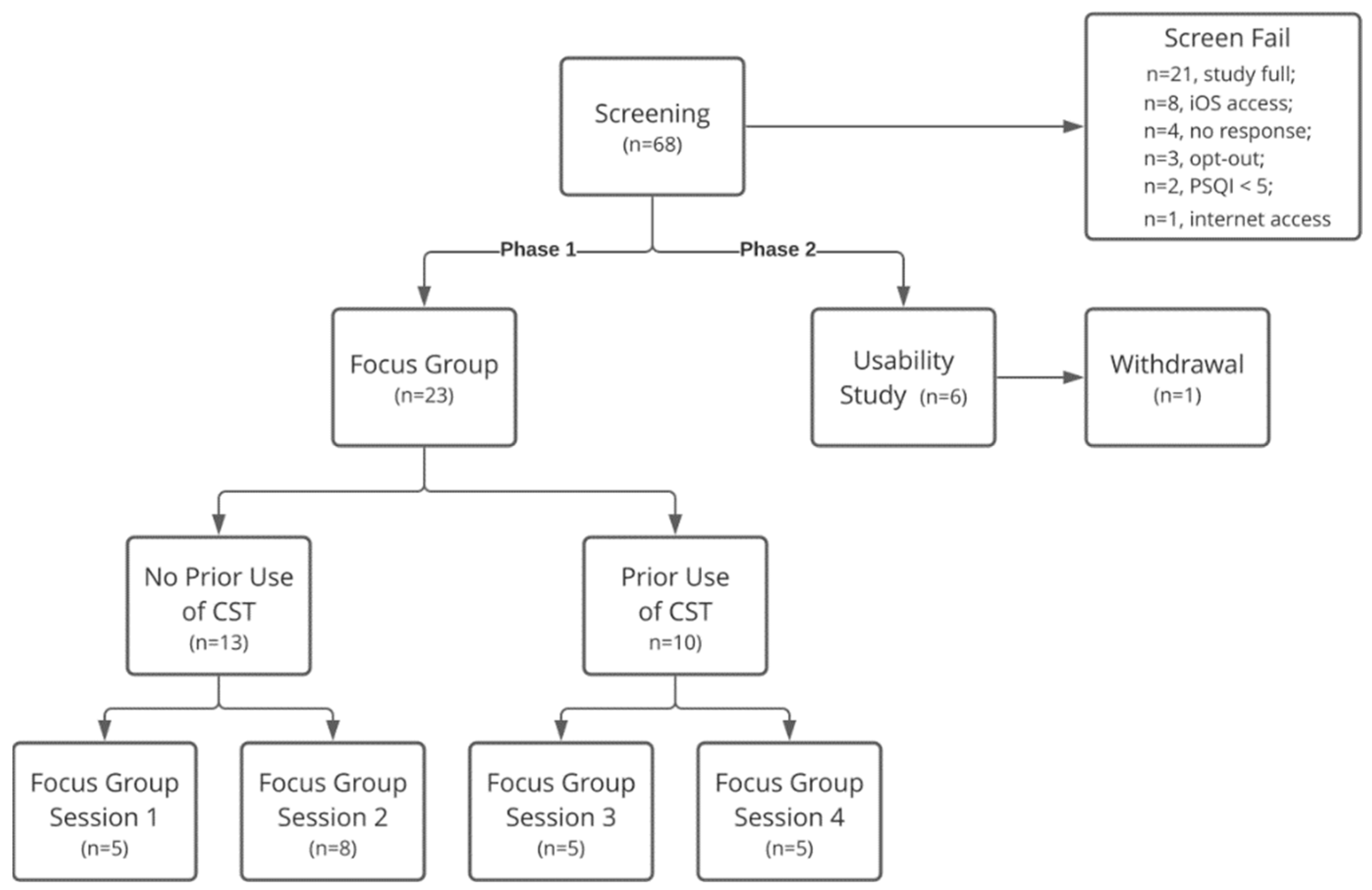
2.1.2. Screening Criteria
2.1.3. Phase 1-Focus Groups
2.1.4. Phase 2-Usability Testing
2.2. Qualitative Content Analysis
3. Results
3.1. Phase 1-Focus Groups
3.1.1. Sample
3.1.2. General Themes
3.1.3. Consumer Priorities
3.1.4. Desires and Suggestions
3.1.5. Comparisons with Habitual Sleep Strategies and Technologies
3.2. Phase 2-Interviews
3.2.1. Sample
3.2.2. General Themes
3.3. Head-Mounted Devices
3.4. Standalone Mobile Applications
3.5. Tracking Pads
4. Discussion
4.1. Design Recommendations
4.1.1. Phase 1-Focus Groups
- Comfort is king, except for participants who prioritize accuracy. Participants preferred non-contact solutions like tracking pads and standalone mobile applications over head-mounted devices.
- Embrace the home sleep setting. Participants were interested in how different environmental factors impacted their sleep and expected apps to incorporate these features to provide actionable feedback rather than just a score.
- Consider integrating with wellness products and strategies that patient-consumers already use. Participants found many of the demonstrated functionalities duplicative and indicated an interest in integrating CSTs+AI with products they already use, such as fitness trackers, smart devices, and personal health apps.
4.1.2. Phase 2-Usability Study
- Participants desired feedback about sleep cycles.
- Other features that participants are interested in are graphs/visuals, interaction from apps, ease of use, aids to help with falling asleep, and alerts of any detected abnormalities.
- Participants also appreciate the ability to personalize CST+AIs.
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| CST | Consumer Sleep Technology |
| CSTs+AI | Consumer Sleep Technologies using Artificial Intelligence |
| HMD | Head-Mounted Device |
| PGHD | Patient-Generated Health Data PSG: Polysomnography |
| PSQI | Pittsburgh Sleep Quality Index SP: Study Participant |
| SP | Study Participant |
Appendix A. Interview Guides
- Have you heard about artificial intelligence?
- How about its applications in healthcare?
- When you hear about artificial intelligence technology being applied to improving sleep what does that bring to mind?
- What sleep technologies have you tried, if any?
- What did you think about these?
- How did AI play a role in this technology?
- If you could design a sleep technology, what would you want the device to do?
- Who do you think would benefit from this technology?
- What differentiates these from other products?
- How would they benefit?
- What features and why?
- What concerns might there be about this technology?
- How could these products be improved?
- Which if any of these technologies do you think you’d be likely to try?
- Why?
- Have you tried any consumer technologies? If so, what kinds?
- Before using the technologies, what were your expectations?
- What would you use sleep technologies for?
- How easy or difficult was it to use each technology?
- What did you enjoy about each technology?
- How do you think these products could be improved?
- What concerns do you have about these technologies?
- How do you think people with sleep disorders can benefit from consumer sleep technologies?
- If you could design a consumer sleep technology, what features would you like it to have?
- If you would continue using any of these technologies, which one(s) and why?
Appendix B

{kind=link}
| Code | Code Definition |
|---|---|
| AWARENESS_OF_AI | to capture the conversation at the beginning of the focus group, related to participants’ awareness of the use of AI in society in general, in healthcare, and in sleep |
| ATTRIBUTE | functions or qualities about a product, device, object, item, or strategy |
| ATTR:Accuracy | information or readings from the product, device, or strategy affected by it falling off, moving around, missing data, lack of trust in the technology, interference by other entities |
| ATTR:Comfort | how it feels on user, if it interferes with sleep or wakes user up |
| ATTR:Cost | direct and indirect costs associated with using or purchasing a device, or seeking medical care, medical insurance, or filling prescriptions for pharmaceuticals or devices |
| ATTR:Ease_of_Use | easy to use interface, able to quickly obtain started, time required to obtain insights from the technology also, related to how the device is charged or powered, gets software updates |
| ATTR:Adhesive | any mention of the adhesive component of a device |
| ATTR:Enhancing_Sleep | related to senses of smell, touch, sound, light |
| ATTR:Feedback | explanations (provides explanations for quality of sleep, patterns in data, or abnormalities in data); summaries (provides summaries of patterns and trends in sleep); recommendations (provides feedbacks, tips, or recommendations for sleep) |
| ATTR:Guided_Meditation | provides guidance on deep breathing, relaxation, or mental wellbeing |
| ATTR:Health_Tracking | feature that helps user track aspects of health including sleep (hours slept or wake/sleep times), fitness, dietary, mental wellness, other (e.g., menstrual cycle) |
| ATTR:Hygiene | how the device can withstand multiple uses or cleaning; cleanliness of the device |
| ATTR:Integration | whether it can be integrated with the consumer’s other technologies or devices (e.g., FitBit or other health tracking apps) |
| ATTR:Need_for_Testing | expressed need for evidence, information, research, or proof about the product |
| ATTR:Personalization | user can decide to customize product, how device is used, or product is customized to the user |
| ATTR:Privacy | whether the information collected by the product will shared with others |
| ATTR:Safety | unintentionally hurting self or others with physical device due to movement; radiation from electronic devices, parts, or components (e.g., Bluetooth) that may cause cancer or other side effects or illnesses |
| ATTR:Utility | usefulness in discussions with doctor, in making treatment decisions, or usefulness in making changes to sleep habits or routines, detection or diagnosis of sleep problems |
| ATTR:Other | does not fit in the list above |
| COMPARISON | When the person discusses the pros/cons between two different products or devices. |
| HEALTH_CONDITIONS | health diagnoses or conditions, such as sleep disorder, anxiety, diabetes, heart conditions, insomnia |
| LOCATION | the physical location or placement of the object, device, or product, or where the product or mobile application’s will be used |
| LOC:DeviceBody | and attached to or on body |
| LOC:DeviceBody:Arm | |
| LOC:DeviceBody:Chest | |
| LOC:DeviceBody:Head | |
| LOC:DeviceBody:Leg | |
| LOC:DeviceNonbody | device NOT attached to nor on body |
| LOC:Place:Clinic | Sleep study centers, and research centers |
| LOC:Place:Home | used in the customer/patient’s primary residence |
| RELATIONSHIPS | a tag used to identify if a participant comments on relationships with other individuals |
| REL:Child | |
| REL:Clinician | physicians, nurses, sleep researchers, etc. |
| REL:Partner | |
| REL:Other | for example parents or pets |
| REL:Self | |
| SENTIMENT | ideally, every utterance mentioning a device will have a sentiment coded with it |
| Negative | |
| NEG:Concern | (-) participant demonstrates worry or anxiety or hesitation about a product or device or feature |
| NEG:Disapproval | (--) participant demonstrates they do not wish to try or use a product or device or feature |
| Neutral | participant may find a product or device or feature acceptable but does not explicitly demonstrate concern or interest |
| Positive | |
| POS:Interest | (+) participant demonstrates curiosity, wanting to know more about a product or device or feature |
| POS:Approval | (++) participant demonstrates they would want to try or use a product or device or feature |
| ST | (sleep therapeutics) a physical item, object, device, or product used in the course of improving sleep |
| ST:Activity_Band | a wrist band, watch, or other device worn on the body to track components of health (separate from the trackers presented in the focus group) |
| ST:App | not related to the sleep apps presented during the focus group. this could include music apps, such as Spotify or Pandora or iTunes, podcast apps |
| ST:CPAP | continuous positive airway pressure therapy and equipment |
| ST:Eye_Mask | fabric covering worn over the eyes during sleep to prevent light-related disturbance |
| ST:Headband | objects worn on or around the head, presented during the focus group |
| ST:Medications | prescribed by a medical professional, over the counter, or recreational |
| ST:Noise_Machine | white noise machines |
| ST:Sleep_Apps | the sleep related apps presented during the focus group |
| ST:Sleep_Pads | the mattress pad presented during the focus group |
| ST:Snoring_Device | Smart Nora device, presented during the focus group |
| ST:Other | mouth guards, video recorders, blue light glasses |
| TEMPORAL | |
| TEMP:CurrentPast | current or prior use of a sleep therapeutic |
| TEMP:Future | envisioned or predicted use of a sleep therapeutic |
References
- Institute of Medicine (US) Committee on Sleep Medicine and Research. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem; Colten, H.R., Altevogt, B.M., Eds.; National Academies Press: Washington, DC, USA, 2006. Available online: http://www.ncbi.nlm.nih.gov/books/NBK19960/ (accessed on 6 June 2021).
- Liu, Y.; Wheaton, A.G.; Chapman, D.P.; Cunningham, T.J.; Lu, H.; Croft, J.B. Prevalence of Healthy Sleep Duration among Adults—United States, 2014. Morb. Mortal. Wkly. Rep. 2016, 65, 137–141. [Google Scholar] [CrossRef] [Green Version]
- Hafner, M.; Stepanek, M.; Taylor, J.; Troxel, W.M.; van Stolk, C. Why Sleep Matters—The Economic Costs of Insufficient Sleep. Rand Health Q. 2017, 6, 11. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5627640/ (accessed on 6 June 2021). [PubMed]
- Khosla, S.; Deak, M.C.; Gault, D.; Goldstein, C.A.; Hwang, D.; Kwon, Y.; O’Hearn, D.; Schutte-Rodin, S.; Yurcheshen, M.; Rosen, I.M.; et al. Consumer Sleep Technology: An American Academy of Sleep Medicine Position Statement. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2018, 14, 877–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, P.-R.T.; Kientz, J.A.; Choe, E.K.; Kay, M.; Landis, C.A.; Watson, N.F. Consumer Sleep Technologies: A Review of the Landscape. J. Clin. Sleep Med. 2015, 11, 1455–1461. [Google Scholar] [CrossRef] [PubMed]
- Consumer Electronics Association. Consumer Awareness and Perceptions of Sleep Technology. Consumer Electronics Association. 2015. Available online: https://web.archive.org/web/20200816231710/https://www.sleepfoundation.org/sites/default/files/2019-02/Consumer-Awareness-and-Perceptions-of-Sleep-Technology.pdf (accessed on 30 June 2020).
- Altini, M.; Kinnunen, H. The Promise of Sleep: A Multi-Sensor Approach for Accurate Sleep Stage Detection Using the Oura Ring. Sensors 2021, 21, 4302. [Google Scholar] [CrossRef] [PubMed]
- de Zambotti, M.; Goldstone, A.; Claudatos, S.; Colrain, I.M.; Baker, F.C. A validation study of Fitbit Charge 2TM compared with polysomnography in adults. Chronobiol. Int. 2018, 35, 465–476. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.K.; Demiris, G.; Lin, S.-Y.; Iribarren, S.J.; Landis, C.A.; Thompson, H.J.; McCurry, S.M.; Heitkemper, M.M.; Ward, T.M. Smartphone Applications to Support Sleep Self-Management: Review and Evaluation. J. Clin. Sleep Med. 2018, 14, 1783–1790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Zambotti, M.; Rosas, L.; Colrain, I.M.; Baker, F.C. The Sleep of the Ring: Comparison of the ŌURA Sleep Tracker against Polysomnography. Behav. Sleep Med. 2019, 17, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Chinoy, E.D.; Cuellar, J.A.; Huwa, K.E.; Jameson, J.T.; Watson, C.H.; Bessman, S.C.; Hirsch, D.A.; Cooper, A.D.; Drummond, S.P.A.; Markwald, R.R. Performance of seven consumer sleep-tracking de-vices compared with polysomnography. Sleep 2021, 44, zsaa291. [Google Scholar] [CrossRef] [PubMed]
- Chinoy, E.D.; Cuellar, J.A.; Jameson, J.T.; Markwald, R.R. Performance of Four Commercial Wearable Sleep-Tracking Devices Tested Under Unrestricted Conditions at Home in Healthy Young Adults. Nat. Sci. Sleep 2022, 14, 493–516. [Google Scholar] [CrossRef] [PubMed]
- De Zambotti, M.; Cellini, N.; Goldstone, A.; Colrain, I.M.; Baker, F.C. Wearable Sleep Technology in Clinical and Research Settings. Med. Sci. Sports Exerc. 2019, 51, 1538–1557. [Google Scholar] [CrossRef] [PubMed]
- Watson, N.F.; Lawlor, C.; Raymann, R.J.E.M. Will Consumer Sleep Technologies Change the Way We Practice Sleep Medicine? J. Clin. Sleep Med. 2019, 15, 159–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aji, M.; Gordon, C.; Peters, D.; Bartlett, D.; Calvo, R.A.; Naqshbandi, K.; Glozier, N. Exploring User Needs and Preferences for Mobile Apps for Sleep Disturbance: Mixed Methods Study. JMIR Ment. Health 2019, 6, e13895. [Google Scholar] [CrossRef] [PubMed]
- Using Sleep Cycle While Sharing a Bed with a Partner. Sleep Cycle. Available online: https://support.sleepcycle.com/hc/en-us/articles/206704569-Using-Sleep-Cycle-While-Sharing-a-Bed-With-a-Partner (accessed on 6 June 2021).
- Buysse, D.J.; Hall, M.L.; Strollo, P.J.; Kamarck, T.W.; Owens, J.; Lee, L.; Reis, S.E.; Matthews, K.A. Relationships Between the Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), and Clinical/Polysomnographic Measures in a Community Sample. J. Clin. Sleep Med. Off. Publ. Am. Acad. Sleep Med. 2008, 4, 563–571. [Google Scholar] [CrossRef] [Green Version]
- Kelly, J.M.; Strecker, R.E.; Bianchi, M.T. Recent Developments in Home Sleep-Monitoring Devices. ISRN Neurol. 2012, 2012, e768794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaudhry, F.F.; Danieletto, M.; Golden, E.; Scelza, J.; Botwin, G.; Shervey, M.; De Freitas, J.K.; Paranjpe, I.; Nadkarni, G.N.; Miotto, R.; et al. Sleep in the Natural Environment: A Pilot Study. Sensors 2020, 20, 1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lordon, R.J.; Mikles, S.P.; Kneale, L.; Evans, H.L.; Munson, S.A.; Backonja, U.; Lober, W.B. How patient-generated health data and patient-reported outcomes affect patient–clinician relationships: A systematic review. Health Inform. J. 2020, 26, 2689–2706. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.T.; Xin, C.; Bindhu, S.; Xu, C.; Sachdeva, J.; Brown, J.L.; Jung, H. Clinician Perspectives and Design Implications in Using Patient-Generated Health Data to Improve Mental Health Practices: Mixed Methods Study. JMIR Form. Res. 2020, 4, e18123. [Google Scholar] [CrossRef] [PubMed]
- Neilsen, J. Why You Only Need to Test with 5 Users. Available online: https://www.nngroup.com/articles/why-you-only-need-to-test-with-5-users/ (accessed on 10 October 2020).

| Consumer Sleep Technology Using AI | Device Name (Vendor) |
|---|---|
| Head-Mounted Devices (HMD) | Beddr (Hancock Medical, Inc., Mountain View, CA, USA) * Dreem Headband (Dreem, Paris, France) Muse S (InteraXon Inc., Toronto, ON, Canada) |
| Tracking Pads | Sleep Analyzer (Withings, Nanterre, France) * Sleep Number (Sleep Number, Minneapolis, MN, USA) ** Smart Bed (Eight Sleep, New York, NY, USA) ** |
| Standalone Mobile Applications | Do I Snore or Grind (SleepScore Labs, Carlsbad, CA, USA) Sleep Cycle (Sleep Cycle AB, Stockholm, Sweden) * Sleeprate (Sleeprate Tel Aviv, Israel) Sleep Score (SleepScore Labs. Carlsbad, CA, USA) |
| Responsive Devices | Smart Nora (Smart Nora, Inc., Toronto, ON, Canada) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, E.; Kearns, W.; Laine, M.; Demiris, G.; Thompson, H.J. Perceptions of and Experiences with Consumer Sleep Technologies That Use Artificial Intelligence. Sensors 2022, 22, 3621. https://doi.org/10.3390/s22103621
Oh E, Kearns W, Laine M, Demiris G, Thompson HJ. Perceptions of and Experiences with Consumer Sleep Technologies That Use Artificial Intelligence. Sensors. 2022; 22(10):3621. https://doi.org/10.3390/s22103621
Chicago/Turabian StyleOh, Esther, William Kearns, Megan Laine, George Demiris, and Hilaire J. Thompson. 2022. "Perceptions of and Experiences with Consumer Sleep Technologies That Use Artificial Intelligence" Sensors 22, no. 10: 3621. https://doi.org/10.3390/s22103621