
Development of a Virtual Reality Simulator for an Intelligent Robotic System Used in Ankle Rehabilitation



Abstract
:1. Introduction
2. Background
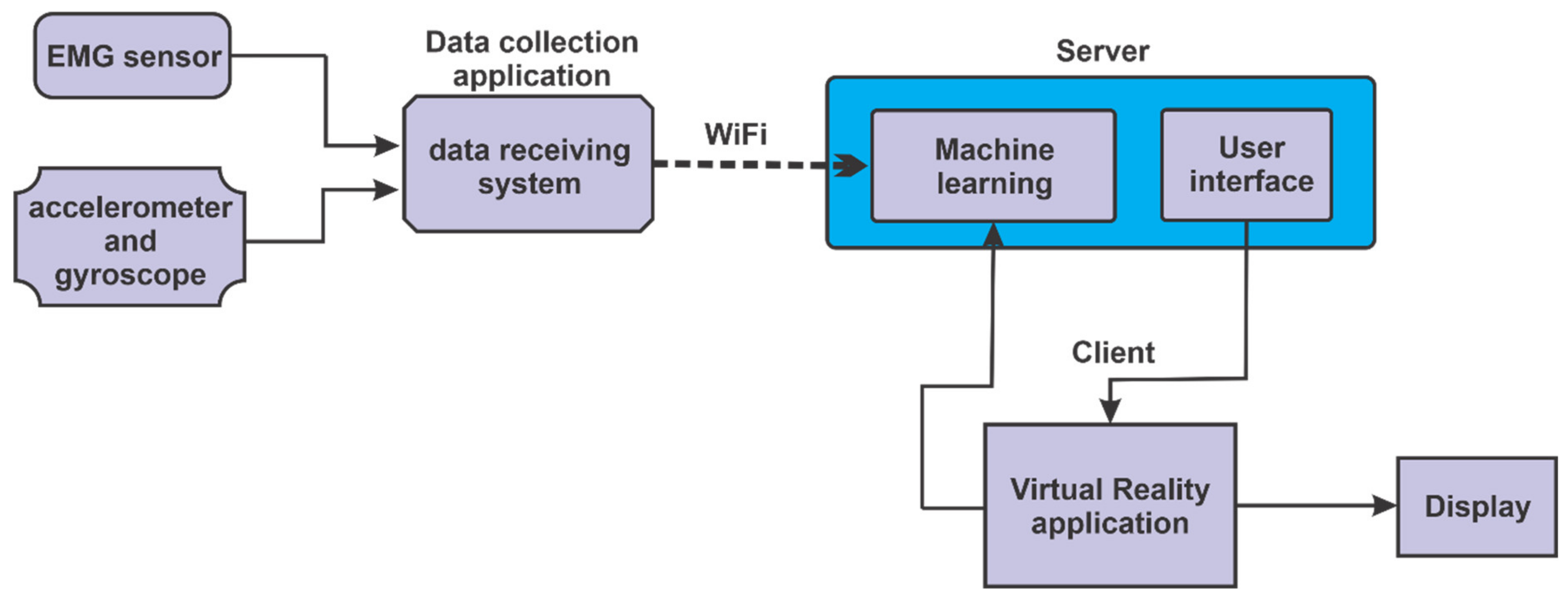
3. Robotic System Architecture
3.1. Components and Connections in the Robotic System
- (1)
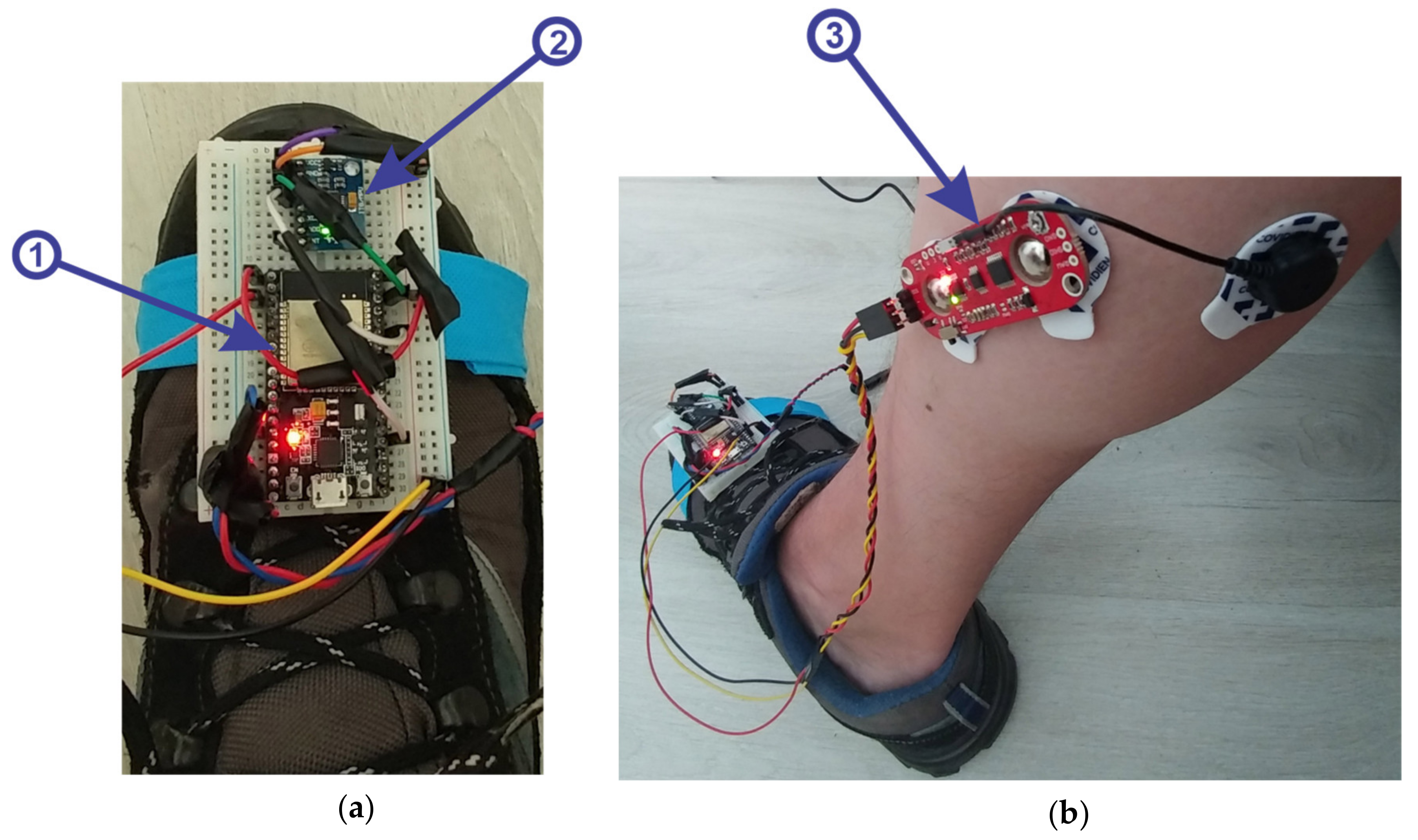
- microcontroller ESP32 (Figure 2a, 1), is a strong development board, containing the following:
- Wi-Fi, Bluetooth and a dual-core processor; frequency: 2.4~2.5 GHz; power supply: 7~3.6 V; size: 18 mm × 25.5 mm × 3.1 mm.
- (2)
- 3-axis accelerometer and gyroscope module, model MPU6050, with the following specifications:
- supply voltage: 3.3–5 V (LDO regulator included); I2C bus voltage: 3.3 V (MAX); current: 5 mA; programmable gyroscope range: ±250, ±500, ±1000, ±2000 o/s; programmable accelerometer range: ±2 g, ±4 g, ±8 g, ±16 g; maximum I2C frequency: 400 kHz.
- (3)
- muscle sensor, MyoWare model with the following specifications:
- single supply, +2.9 V to +5.7 V with polarity reversal protection; two output modes: EMG Envelope and Raw EMG; LED indicators; adjustable gain.

3.2. Description of the Main Components of the Robotic Rehabilitation Structure
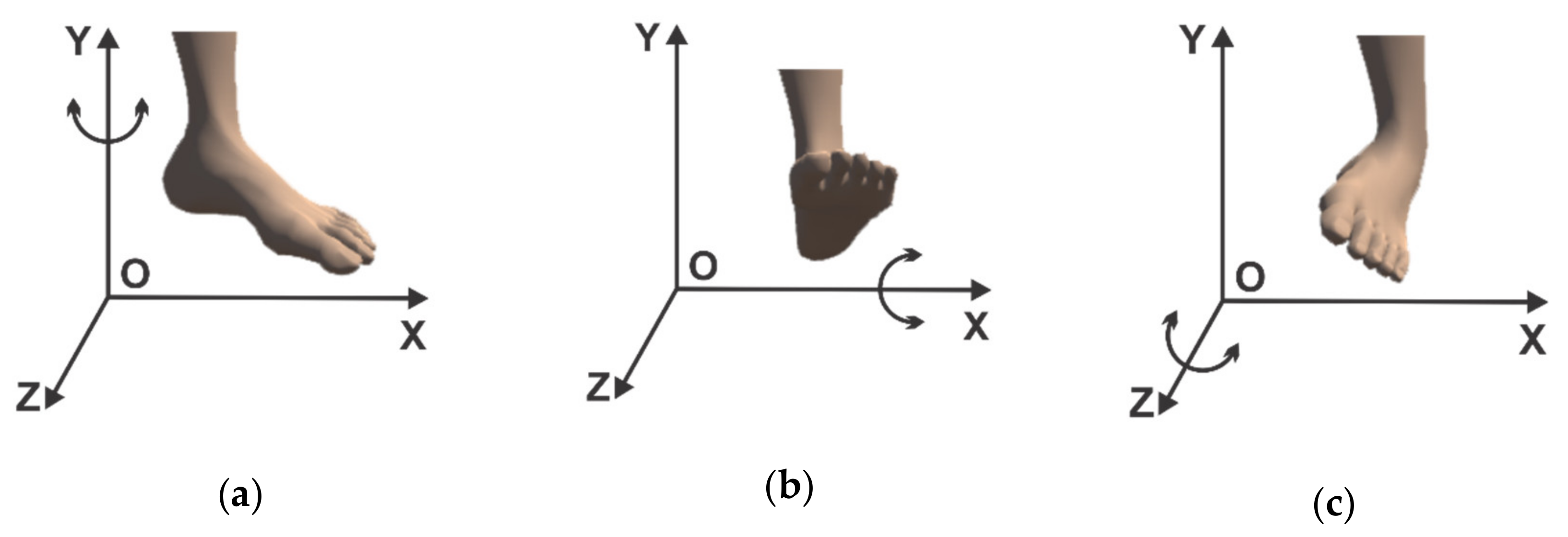
- (1)
- rotation in horizontal plane (parallel to the xOz plane) around the Oy axis (Figure 3a);
- (2)
- rotational motion in vertical plane (parallel to the yOz plane) around the Ox axis (Figure 3b);
- (3)
- the third motion shown consists of a rotation around the Oz axis (in a plane parallel to the xOy plane) (Figure 3c).

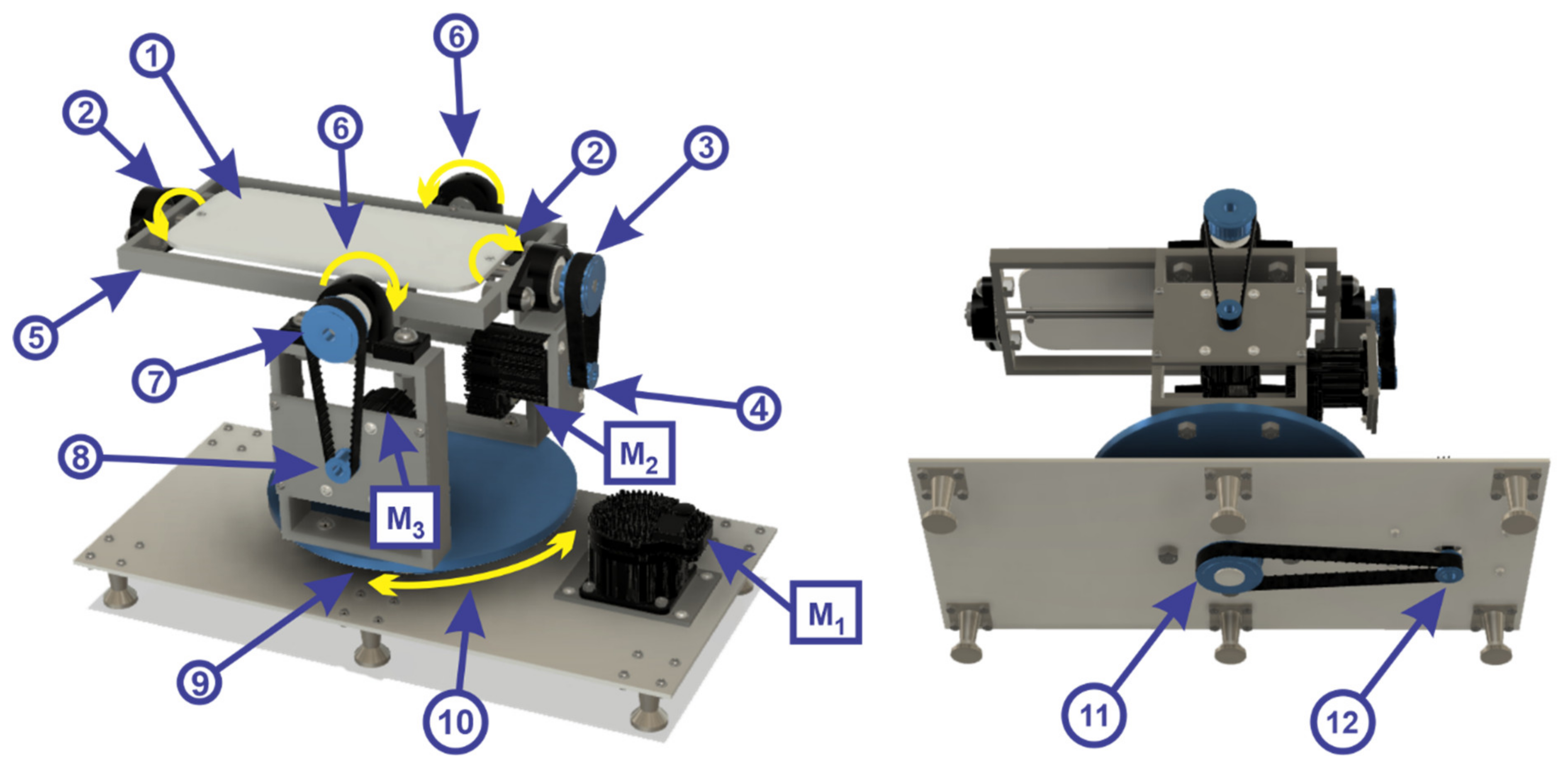
- mobile platform 1 rotates about the Oz axis in a counterclockwise and clockwise direction, by means of a toothed wheel (2);
- toothed wheel (2) is driven by a transmission belt (3) by means of a toothed wheel (4);
- toothed wheel (4) is driven by a servomotor (M2) from TEKNIC, model CPM-SDHP-2311S-ELS;
- the mobile platform 2 (5) rotates vertically plane around the Ox axis in a counterclockwise and clockwise direction (6) by means of a toothed wheel (7);
- toothed wheel (7) is driven by a drive belt by means of a toothed wheel (8) being driven by a servomotor (M3) from TEKNIC, model CPM-SDHP-2311S-ELS;
- the mobile platform 3 (9) make a rotation in horizontal plane (parallel to the xOz plane) around the Oy axis in the counterclockwise and clockwise direction (10) by means of a toothed wheel (11);
- toothed wheel (11) is driven by a transmission belt by means of a toothed wheel (12) being driven by a servomotor (M1) from the company TEKNIC, model CPM SDHP-3411S-ELS.

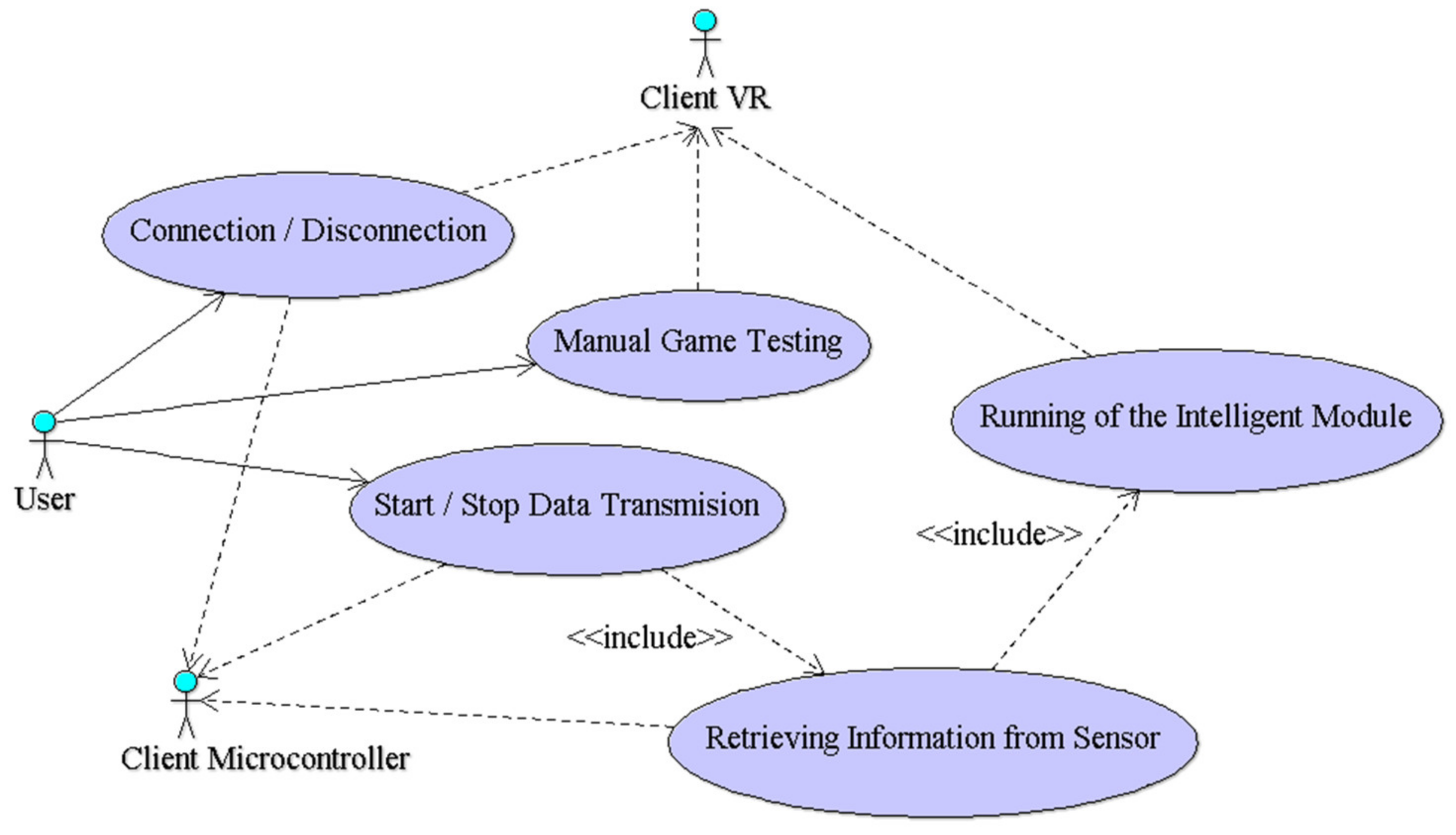
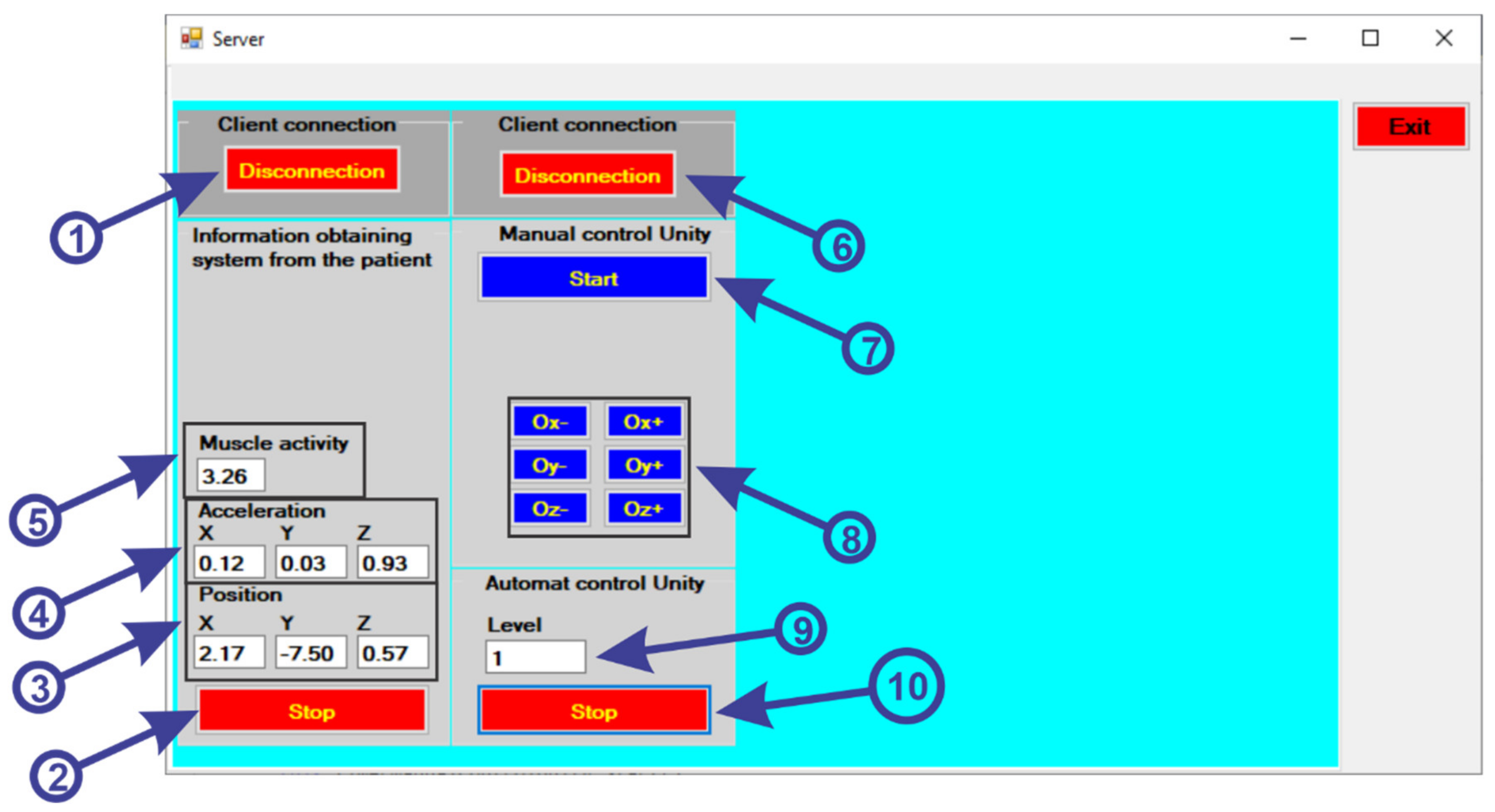
3.3. Description of the Graphical User Interface
- first the “ConnectESP32” button (1) is pressed to make the connection via Wi-Fi connection between the Server application and the Client application located on the ESP32 microcontroller;
- to receive the data from the sensors, we must press the “Start” button (2);
- after pressing the button, the data is collected and displayed from the gyroscope sensor (3) for position, accelerometer (4) to identify the acceleration and the muscle activity sensor (5) to identify the state of muscle tone.
- to make the connection between the server and the client application of the virtual reality application, the “ConnectUnity” button must be pressed (6);
- after the communication has been established, we must press the “Start” button (7) to start the communication for the manual control of the virtual reality application, without including the intelligent module;
- using the following buttons (8), a test of the robotic rehabilitation structure is performed to perform the various exercises, as follows:
- -
- when we press the “Ox−” button a clockwise rotation is made around the Ox axis;
- -
- when we press the “Ox+” button a counterclockwise rotation is made around the Ox axis;
- -
- when we press the “Oy−” button a clockwise rotation is made around the Oy axis;
- -
- when we press the “Oy+” button a counterclockwise rotation is made around the Oy axis;
- -
- when we press the “Oz−” button a clockwise rotation is made around the Oz axis;
- -
- when we press the “Oz+” button a counterclockwise rotation is made around the Oz axis;
- by pressing the “Start” button (10) the virtual reality application is started automatically, the application communicating with the intelligent module to create the range of levels for the virtual reality application (9).

4. Software Application Development
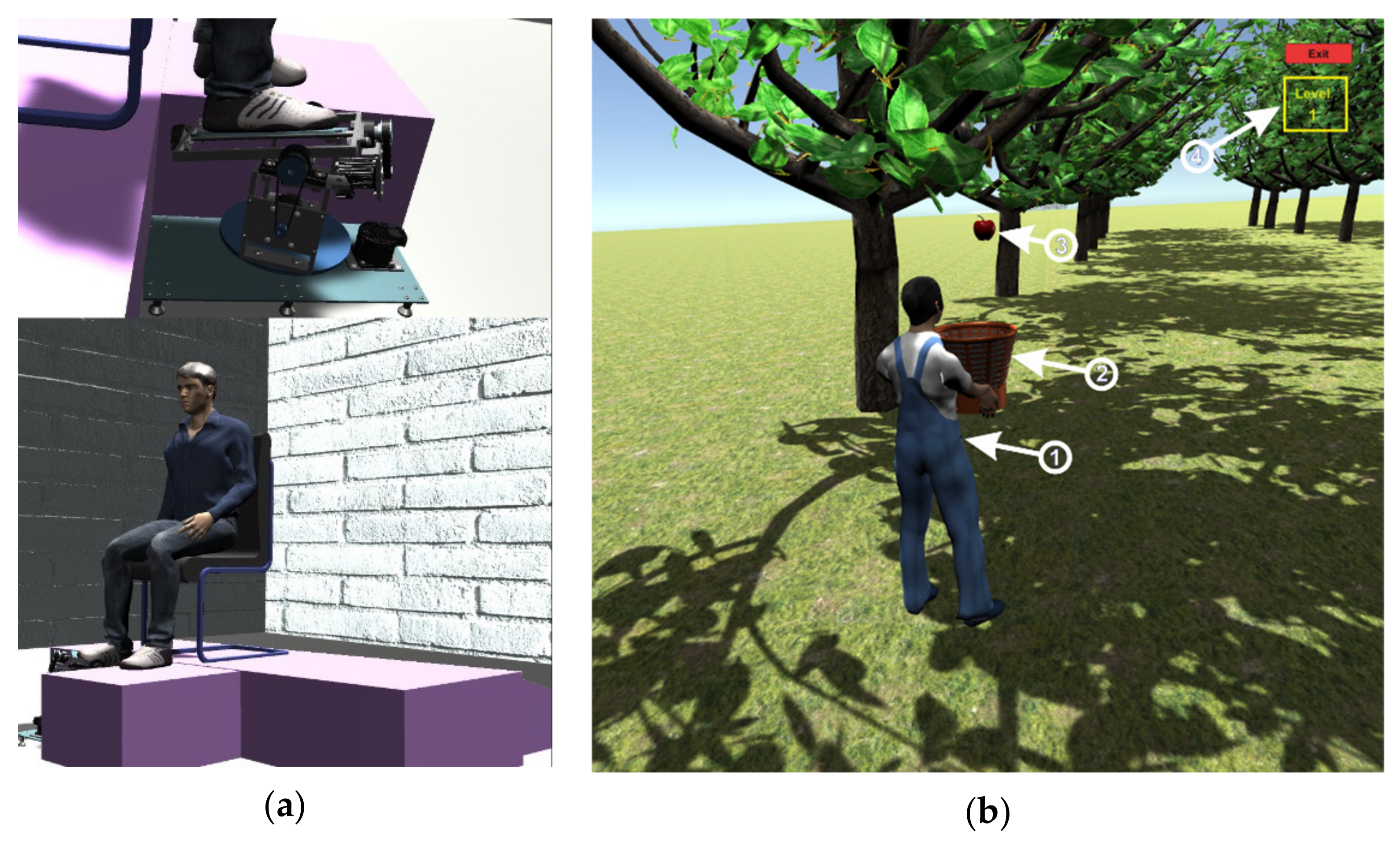
4.1. Description of the Operation of the Virtual Reality Application
- to control the walking of the human virtual character, the patient must make a rotation in vertical plane of the ankle (parallel to the yOz plane) around the Ox axis (Figure 3b). By rotating the ankle around the Ox axis in the counterclockwise direction, the human virtual character goes slowly, and by rotating the ankle around the Ox axis in the clockwise direction, the human virtual character begins to run;
- to direct the human virtual character as it goes left and right, the real human subject must make a rotational movement of the ankle in a horizontal plane (parallel to the xOz plane) around the Oy axis (Figure 3a). When a rotation movement is made in a counterclockwise direction, the human virtual character turns to the left, and when a rotation is made in a clockwise direction, the human virtual character turns to the right;
- in order to make a 180-degree rotation of the human virtual character, the patient must make a rotation of the ankle around the Oz axis (in a plane parallel to the xOy plane) (Figure 3c) in counterclockwise and clockwise direction.

4.2. Intelligent Module Description
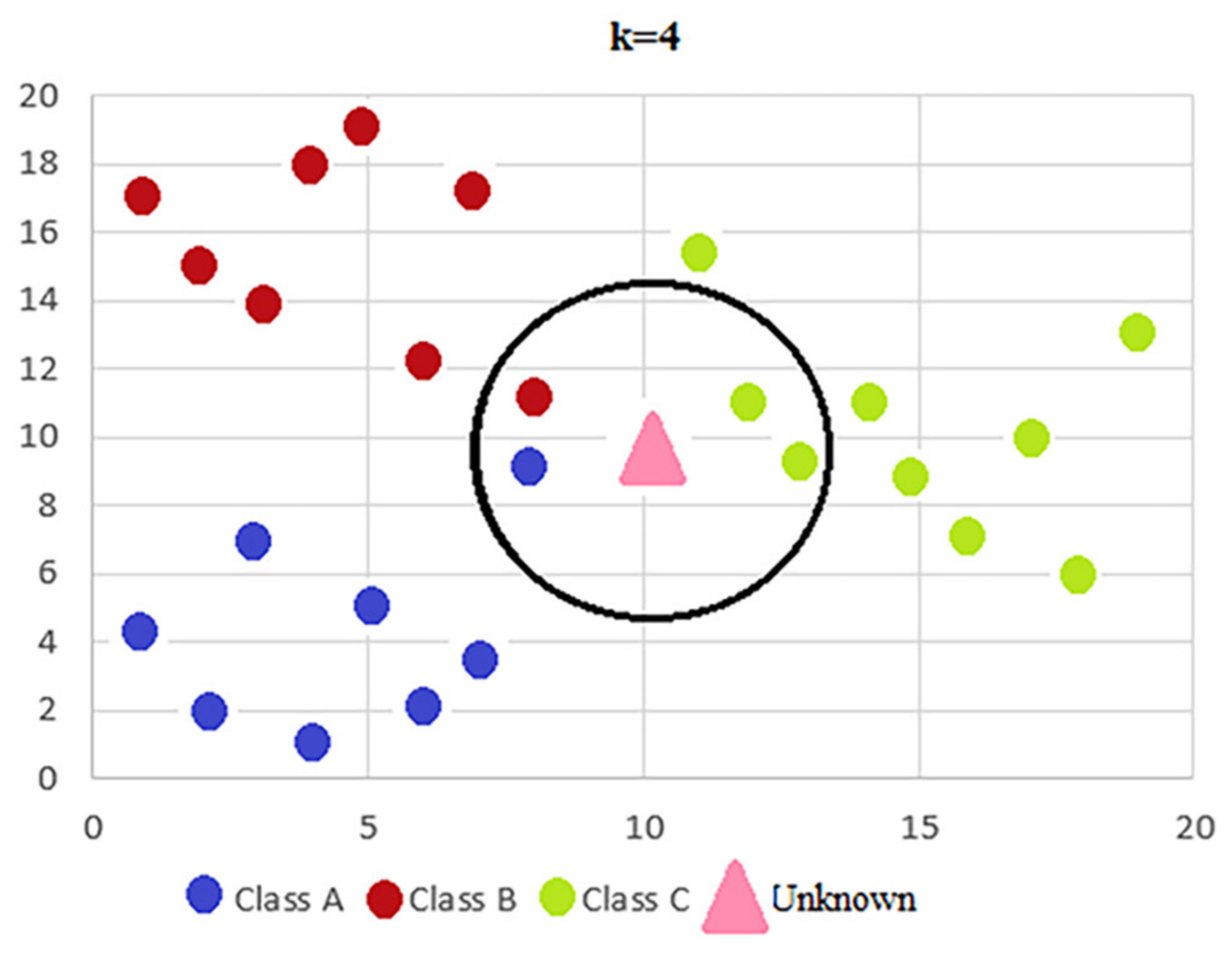
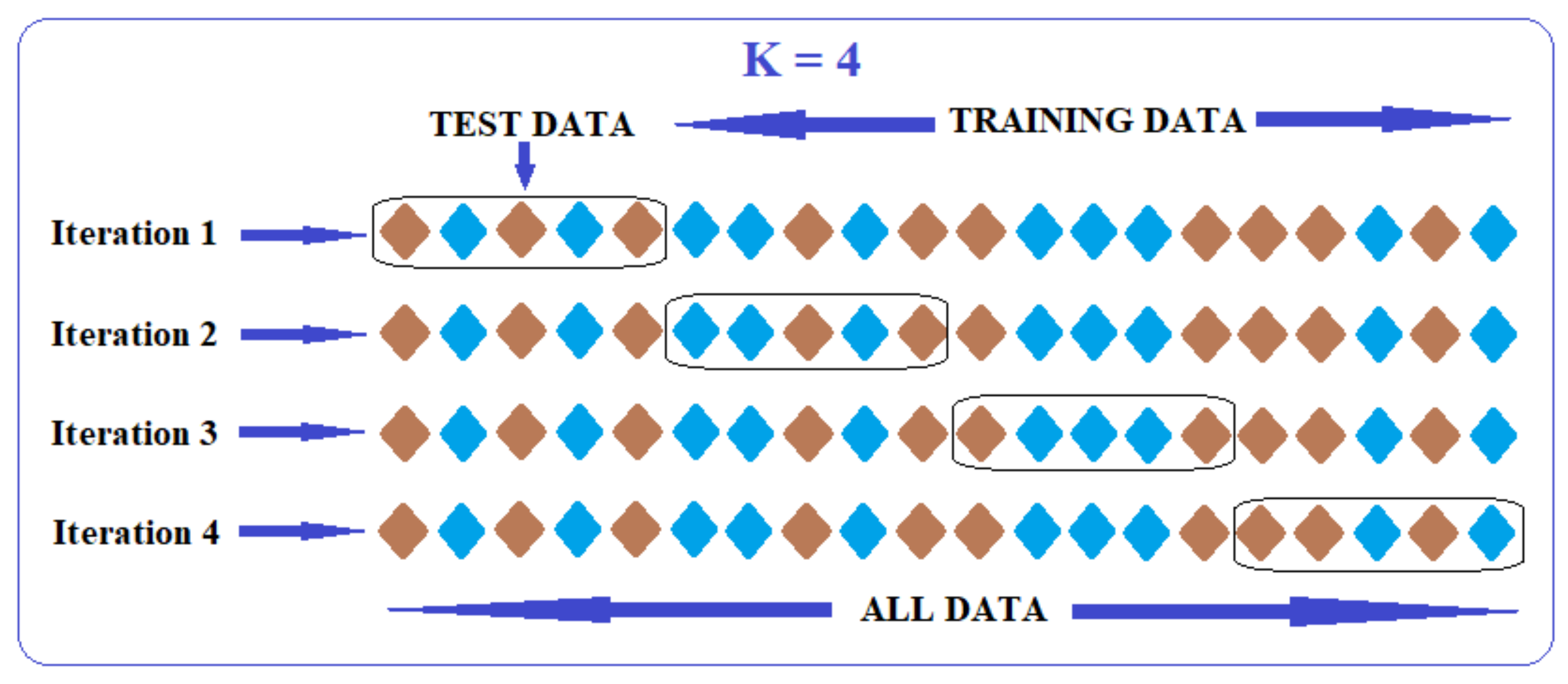
4.2.1. K-Nearest Neighbours
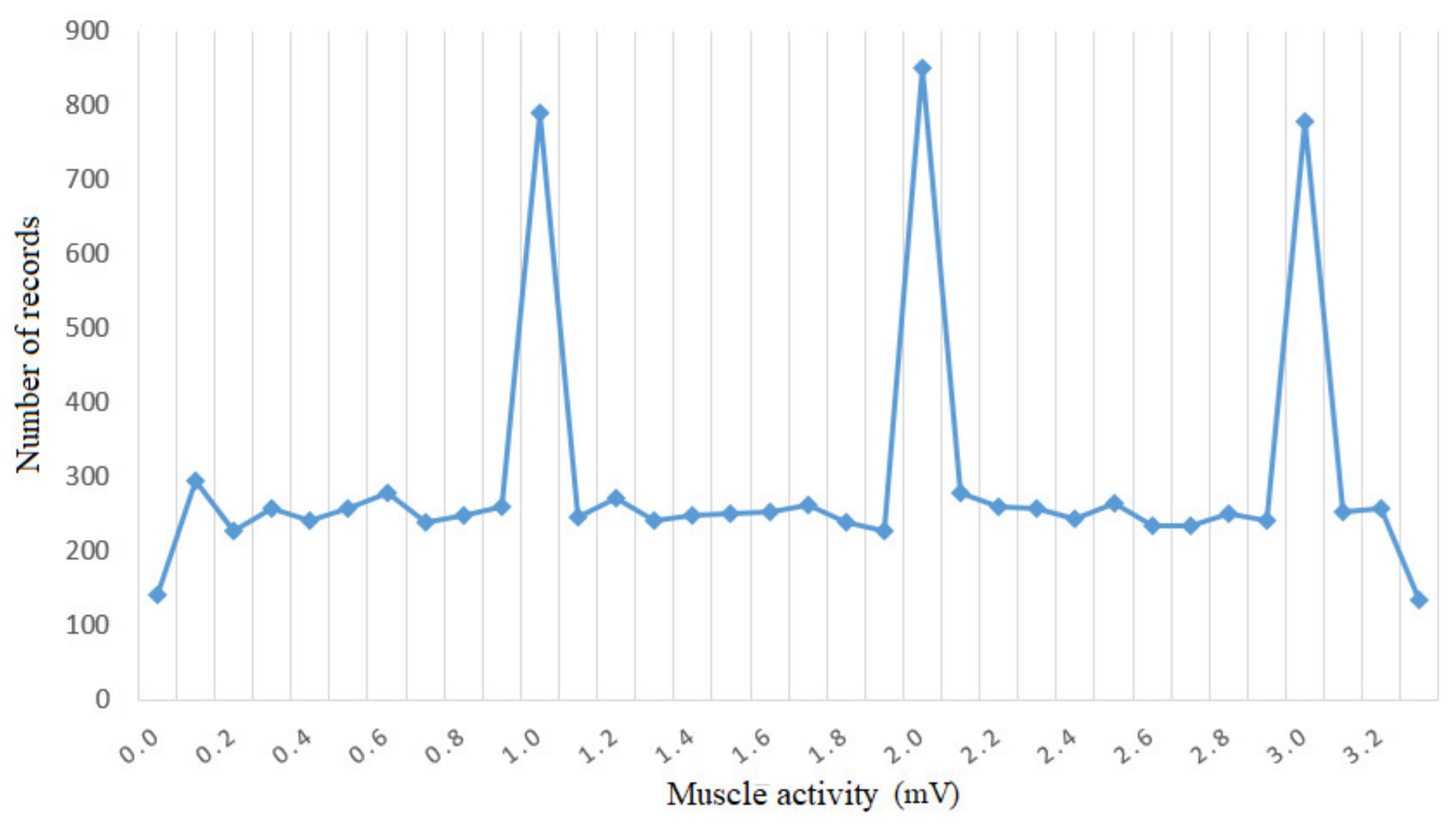
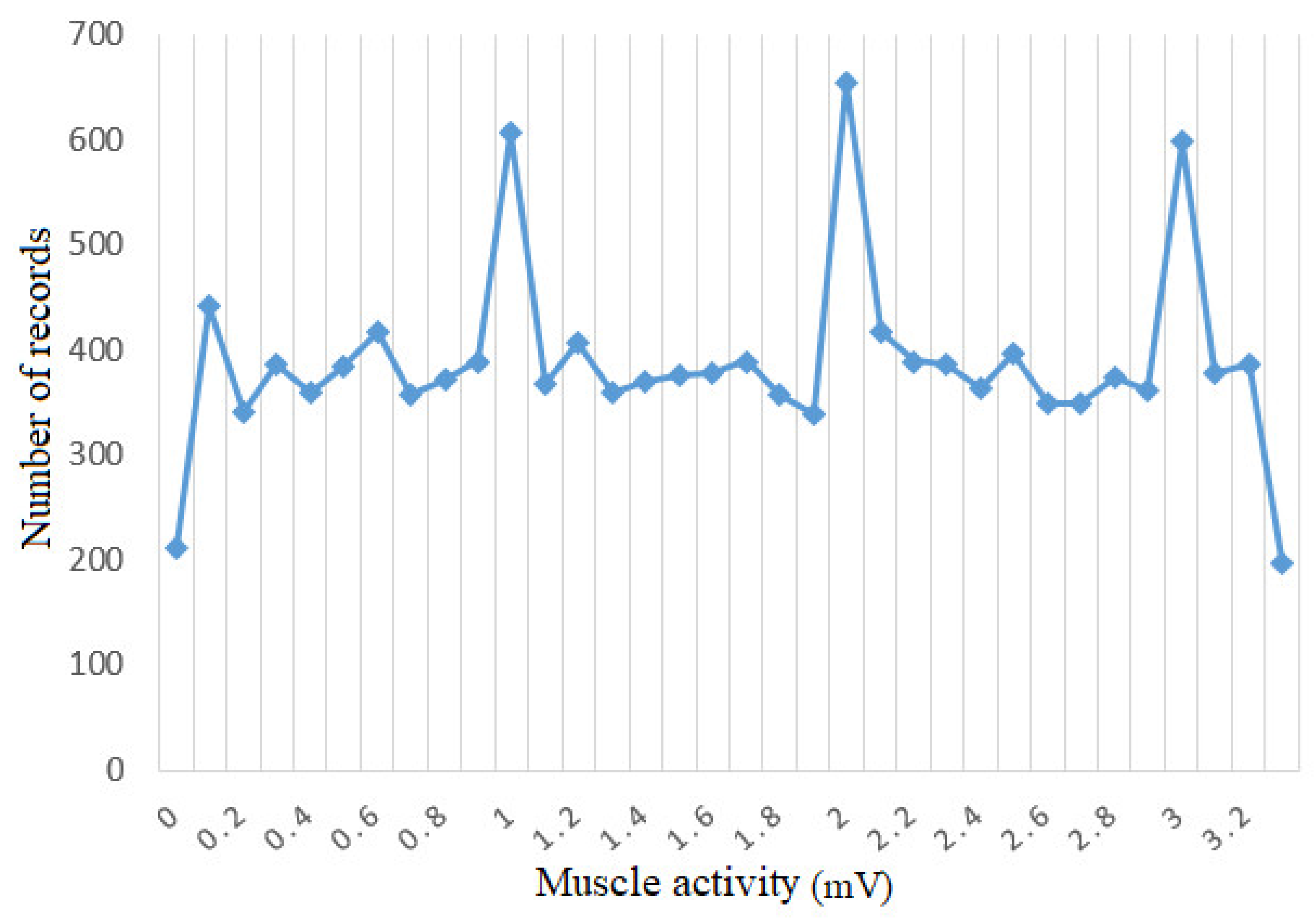
4.2.2. Preliminary Analysis and Preprocessing of the Data Set
- M—the value returned by the sensor that measures muscle intensity;
- Ax—projection on the Ox axis of the measured acceleration;
- Ay—projection on the Oy axis of the measured acceleration;
- Az—projection on the Oz axis of the measured acceleration;
- Px—projection on the Ox axis of foot position;
- Py—projection on the Oy axis of foot position;
- Pz—projection on the Oz axis of foot position;
- S—value that specifies the score obtained by the patient in the previous game.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| M | Ax | Ay | Az | Px | Py | Pz | S |
|---|---|---|---|---|---|---|---|
| 0.0774 | −0.0498 | 0.0007 | 0.9277 | 248.554 | 1297.854 | 1765.564 | 0 |
| 0.0105 | −0.1013 | 0.0378 | 0.9338 | 246.6993 | 1284.16 | 1777.141 | 0.4 |
| 0.2208 | −0.1143 | 0.2205 | 0.8694 | 256.5768 | 1259.951 | 1792.288 | 0.8 |
| 0.7986 | −0.1304 | 0.1609 | 0.885 | 243.2331 | 1246.401 | 1810.49 | 0.6 |
| 0.9203 | −0.1643 | 0.1575 | 0.8877 | 250.1196 | 1231.634 | 1817.76 | 1 |
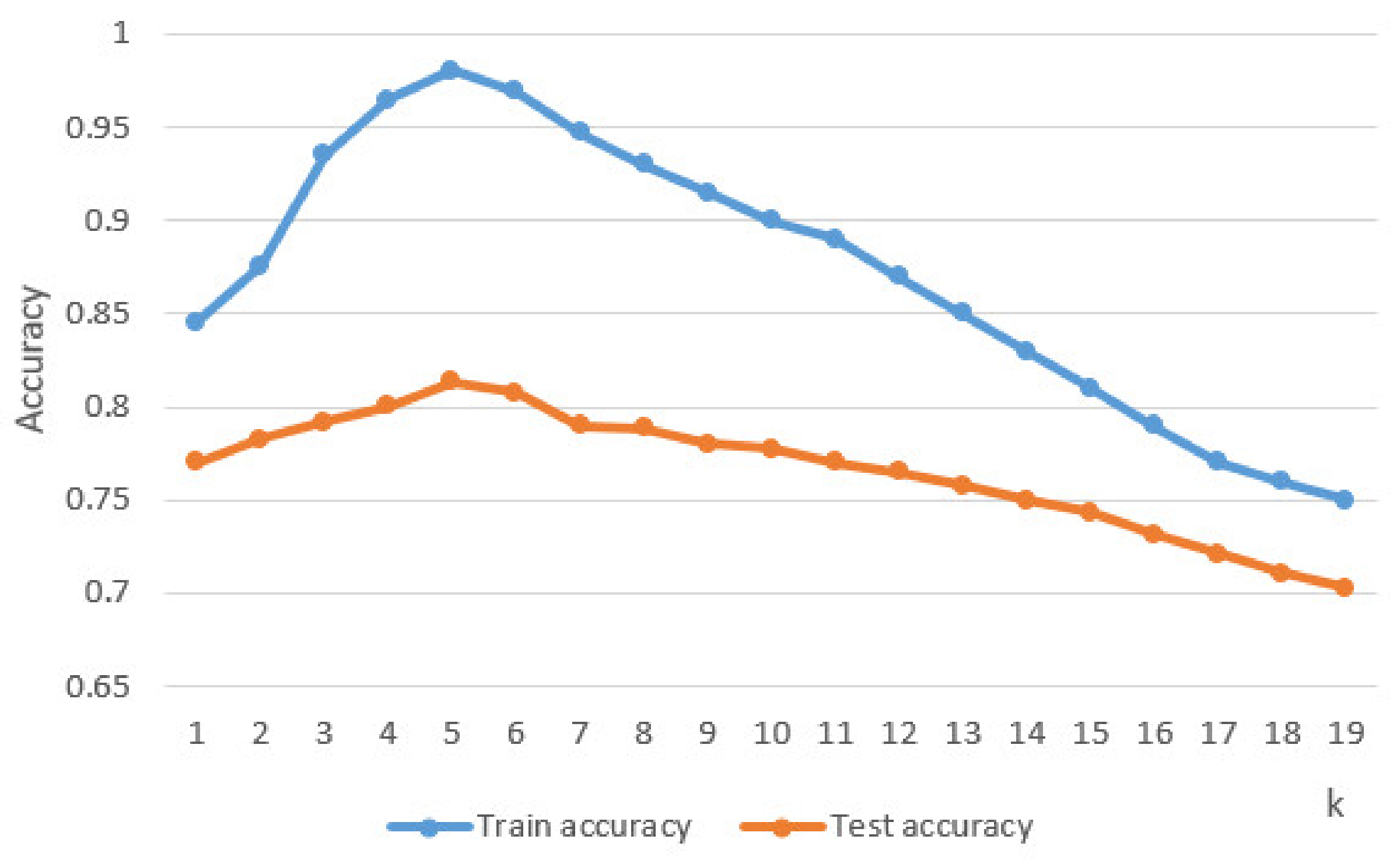
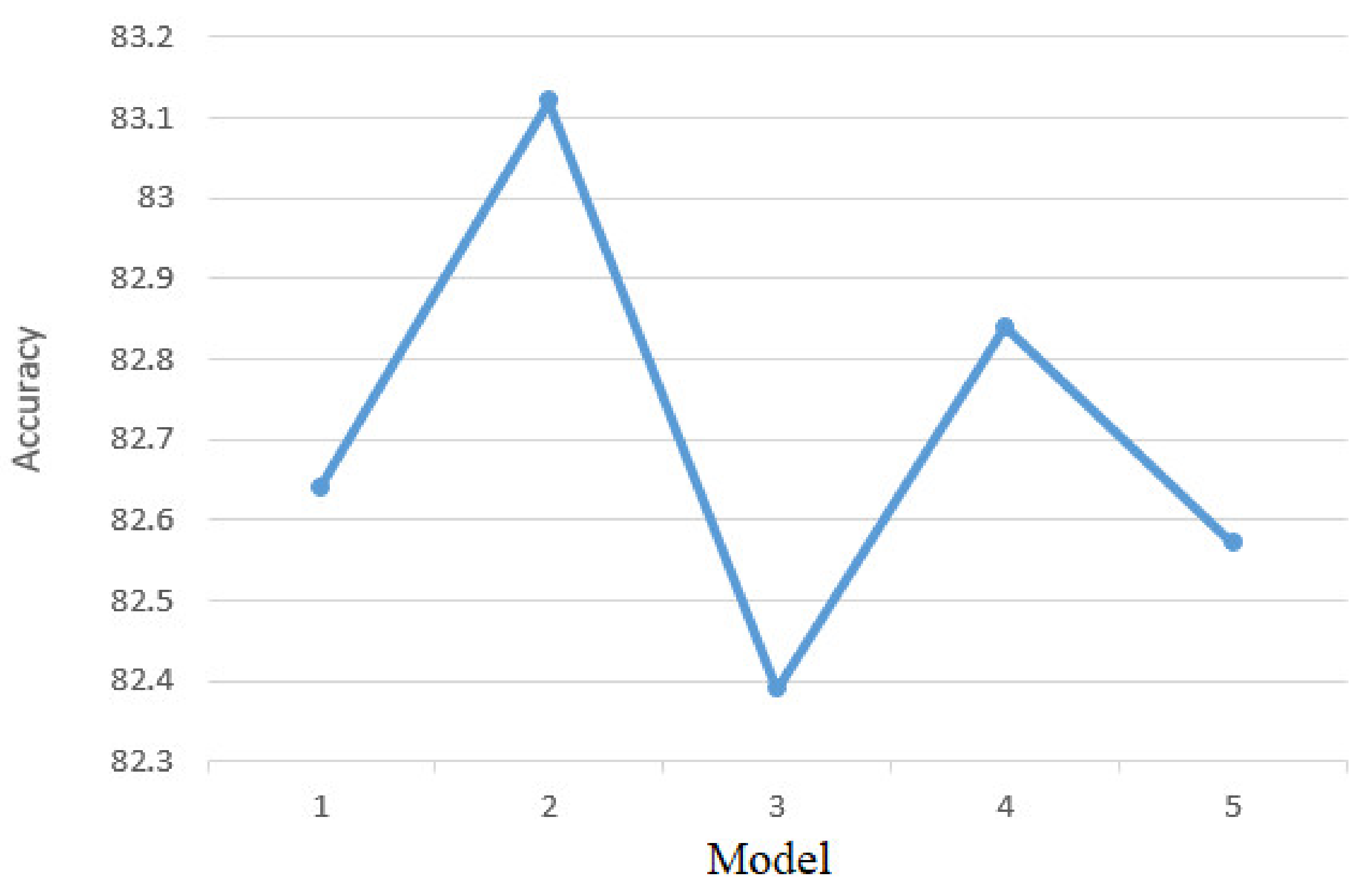
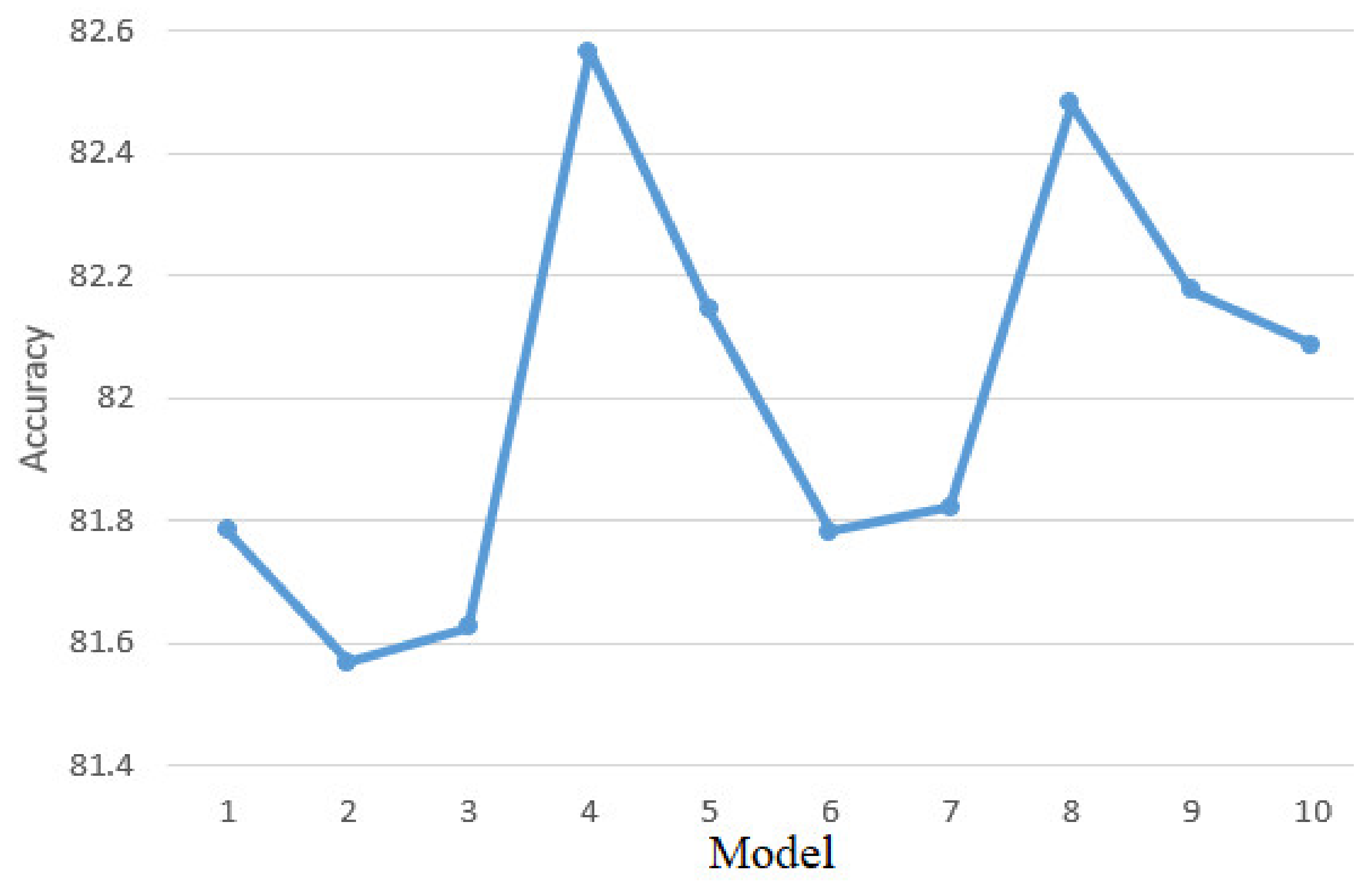
4.2.3. Model Training
4.2.4. Evaluation of the Trained Model
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Varani, S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M. Heart Disease and Stroke Statistics—2020 Update: A Report From the American Heart Association. Circulation 2020, 141, 139–596. [Google Scholar] [CrossRef]
- MAYO CLINIC. Available online: mayoclinic.org/diseases-conditions/stroke/diagnosis-treatment/drc-20350119 (accessed on 19 August 2020).
- Masmoudi, M.; Djekoune, O.; Zenati, N.; Benrachou, D. Design and development of 3D environment and virtual reality interaction: Application to functional rehabilitation. In Proceedings of the International Conference on Embedded Systems in Telecommunications and Instrumentation, Annaba, Algeria, 28–30 October 2019. [Google Scholar]
- Major, Z.Z.; Vaida, C.; Major, K.A.; Tucan, P.; Simori, G.; Banica, A.; Brusturean, E.; Burz, A.; Craciunas, R.; Ulinici, I.; et al. The Impact of Robotic Rehabilitation on the Motor System in Neurological Diseases. A Multimodal Neurophysiological Approach. Int. J. Environ. Res. Public Health 2020, 17, 6557. [Google Scholar] [CrossRef]
- Iglesia, D.H.; Mendes, A.; González, G.; Diego, M.; Juan, F. Connected Elbow Exoskeleton System for Rehabilitation Training Based on Virtual Reality and Context-Aware. Sensors 2020, 20, 858. [Google Scholar]
- Scalona, E.; Taborri, J.; Hayes, D.R.; Del Prete, Z.; Rossi, S.; Palermo, E. Is the Neuromuscular Organization of Throwing Unchanged in Virtual Reality? Implications for Upper Limb Rehabilitation. Electronics 2019, 8, 1495. [Google Scholar] [CrossRef] [Green Version]
- Sierotowicz, M.; Connan, M.; Castellini, C. Human-In-The-Loop Assessment of an Ultralight, Low-Cost Body Posture Tracking Device. Sensors 2020, 20, 890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Luzio, F.S.; Lauretti, C.; Cordella, F.; Draicchio, F.; Zollo, L. Visual vs vibrotactile feedback for posture assessment during upper-limb robot-aided rehabilitation. Appl. Ergon. 2020, 82, 102950. [Google Scholar] [CrossRef]
- Joo, S.Y.; Cho, Y.S.; Lee, S.Y.; Seok, H.; Seo, C.H. Effects of Virtual Reality-Based Rehabilitation on Burned Hands: A Prospective, Randomized, Single-Blind Study. J. Clin. Med. 2020, 9, 731. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, B.; Menezes, P. An Adaptive Virtual Reality-Based Serious Game for Therapeutic Rehabilitation. Int. J. Online Biomed. Eng. 2020, 16, 63–71. [Google Scholar] [CrossRef] [Green Version]
- Zakharov, A.V.; Bulanov, V.A.; Khivintseva, E.V.; Kolsanov, A.V.; Bushkova, Y.V.; Ivanova, G.E. Stroke Affected Lower Limbs Rehabilitation Combining Virtual Reality With Tactile Feedback. Front. Robot. 2020, 7, 1–7. [Google Scholar] [CrossRef]
- Wang, H.; Lin, M.; Lin, Z.; Wang, X.; Niu, J.; Yu, H.; Zhang, L.; Vladareanu, L. Virtual reality training system based on lower limb rehabilitation robot. Int. J. Eng. Technol. 2018, 7, 119–122. [Google Scholar] [CrossRef]
- Lee, H.S.; Park, Y.J.; Park, S.W. The Effects of Virtual Reality Training on Function in Chronic Stroke Patients: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2019, 2019, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Mirelman, A.; Bonato, P.; Deutsch, J.E. Effects of Training with a Robot-Virtual Reality System Compared With a Robot Alone on the Gait of Individuals after Stroke. Stroke 2009, 40, 169–174. [Google Scholar] [CrossRef]
- Burdea, G.C.; Cioi, D.; Kale, A.; Janes, W.E.; Ross, S.A.; Engsberg, J.R. Robotics and Gaming to Improve Ankle Strength, Motor Control, and Function in Children With Cerebral Palsy—A Case Study Series. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 165–173. [Google Scholar] [CrossRef] [Green Version]
- Zimmerli, L.; Jacky, M.; Lünenburger, L.; Riener, R.; Bolliger, M. Increasing Patient Engagement during Virtual Reality-Based Motor Rehabilitation. Arch. Phys. Med. Rehabil. 2013, 94, 1737–1746. [Google Scholar] [CrossRef]
- Esfahlani, S.S.; Cirstea, S.; Sanaei, A.; Wilson, G. An adaptive self-organizing fuzzy logic controller in a serious game for motor impairment rehabilitation. In Proceedings of the 2017 IEEE 26th International Symposium on Industrial Electronics (ISIE), Edinburgh, UK, 19–21 June 2017; pp. 1311–1318. [Google Scholar]
- Angamuthu, K.; Anandu, K.B.; Abhishek, S.; Williams, L.; Pius, R. Effect of materials and designs of brake rotor discs on factor of safety and displacement assessed using auto desk fusion360. Int. J. Recent Technol. Eng. 2019, 8, 3186–3192. [Google Scholar]
- Kharmoum, N.; Retal, S.; Ziti, S.; Omary, F. A Novel Automatic Transformation Method from the Business Value Model to the UML Use Case Diagram. Adv. Intell. Syst. Comput. 2020, 1104, 38–50. [Google Scholar]
- Ribeiro, L.; Duarte, L.M.; Machado, R.; Costa, A.; Cota, É.F.; Bezerra, J.S. Use case evolution analysis based on graph transformation with negative application conditions. Sci. Comput. Program. 2020, 198, 102495. [Google Scholar] [CrossRef]
- Gittleman, A. Computing with C# and the Net Framework; Jones and Bartlett Publishers: Burlington, NJ, USA, 2011; pp. 98–123. [Google Scholar]
- Thuan, T.; Hoang, L. Net Framework Essentials; O’Reilly & Associates, Inc.: Sebastopol, CA, USA, 2015; pp. 78–98. [Google Scholar]
- Wolf, M.; Trentsios, P.; Kubatzki, N.; Urbanietz, C.; Enzner, G. Implementing Continuous-Azimuth Binaural Sound in Unity 3D. In Proceedings of the 2020 IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops (VRW), Atlanta, GA, USA, 22–26 March 2020; pp. 384–389. [Google Scholar]
- Chifu, E.S.; Chifu, V.R. An Unsupervised Neural Model for Aspect Based Opinion Mining. In Proceedings of the 2019 IEEE 15th International Conference on Intelligent Computer Communication and Processing (ICCP), Cluj-Napoca, Romania, 5–7 September 2019; pp. 151–157. [Google Scholar]
- Borsos, Z.; Lemnaru, C.; Potolea, R. Dealing with overlap and imbalance: A new metric and approach. Pattern Anal. Appl. 2016, 21, 381–395. [Google Scholar] [CrossRef]
- Ghiormez, L.; Panoiu, M.; Pânoiu, C.; Pop, C. Power control of an electric arc furnace using intelligent techniques. In Proceedings of the 2018 IEEE International Conference on Industrial Technology (ICIT), Lyon, France, 20–22 February 2018; pp. 292–297. [Google Scholar]
- Muscalagiu, I.; Popa, H.E.; Negru, V. Improving the performances of asynchronous search algorithms in scale-free networks using the nogood processor technique. Comput. Inform. 2015, 34, 254–274. [Google Scholar]
- Groza, A.; Ozturk, P.; Razvan-Slavescu, R.; Marginean, A. Climate change opinions in online debate sites. Comput. Sci. Inf. Syst. 2020, 17, 93–115. [Google Scholar] [CrossRef] [Green Version]
- Rob, R.; Tirian, G.O.; Panoiu, C. Intelligent Acquisition System used in Mechanical Laboratory. In Proceedings of the International Conference on Circuits, Systems, Communications and Computers, Corfu, Greece, 14–17 July 2016. [Google Scholar]
- Kück, M.; Freitag, M. Forecasting of customer demands for production planning by local k-nearest neighbor models. Int. J. Prod. Econ. 2021, 231, 107837. [Google Scholar] [CrossRef]
- Cuntan, C.D.; Baciu, I.; Osaci, M. Operational Study of a Frequency Converter with a Control sequence utilizing Xilinx Software. Acta Polytech. Hung. 2015, 12, 201–212. [Google Scholar]
- Guo, H.; Hong, H. Research on Filtering Algorithm of MEMS Gyroscope Based on Information Fusion. Sensors 2019, 19, 3552. [Google Scholar] [CrossRef] [Green Version]
- Molla, M.M.I.; Jui, J.J.; Bari, B.S.; Rashid, M.; Hasan, J. Cardiotocogram Data Classification Using Random Forest Based Machine Learning Algorithm. Lect. Notes Electr. Eng. 2020, 666, 357–369. [Google Scholar] [CrossRef]
- Bilski, J.; Kowalczyk, B.; Marchlewska, A.; Zurada, J.M. Local Levenberg-Marquardt Algorithm for Learning Feedforwad Neural Networks. J. Artif. Intell. Soft Comput. Res. 2020, 10, 299–316. [Google Scholar] [CrossRef]
- Leevy, J.L.; Khoshgoftaar, T.M.; Bauder, R.A.; Seliya, N. Investigating the relationship between time and predictive model maintenance. J. Big Data 2020, 7, 1–19. [Google Scholar] [CrossRef]
- Zareapoor, M.; Shamsolmoali, P.; Yang, J. Oversampling adversarial network for class-imbalanced fault diagnosis. Mech. Syst. Signal Process. 2021, 149, 107175. [Google Scholar] [CrossRef]
- Sequeira, A.M.; Lousa, D.; Rocha, M. ProPythia: A Python Automated Platform for the Classification of Proteins Using Machine Learning. Adv. Intell. Syst. Comput. 2021, 1240, 32–41. [Google Scholar]
- Carillo, E.R.; Dispo, S.; Fallarco, R.V.H.; Mateo, K.F.; Garcia, R.; Sejera, M.; Valiente, F.L. Gum Disease Detection in the Front Part of the Mouth Using Convolutional Neural Network Through the Use of Keras with TensorFlow as Backend. In Proceedings of the International Conference on Biomedical Engineering and Technology, Tokyo, Japan, 15–18 September 2020; pp. 144–150. [Google Scholar]
- Rubi, B.; Morcegol, B.; Perez, R. Adaptive Nonlinear Guidance Law Using Neural Networks Applied to a Quadrotor. In Proceedings of the 2019 IEEE 15th International Conference on Control and Automation (ICCA), Edinburgh, UK, 16–19 July 2019; pp. 1626–1631. [Google Scholar]
- Rad, K.R.; Maleki, A. A scalable estimate of the out-of-sample prediction error via approximate leave-one-out cross-validation. J. R. Stat. Soc. Ser. B Stat. Methodol. 2020, 82, 965–996. [Google Scholar] [CrossRef]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Covaciu, F.; Pisla, A.; Iordan, A.-E. Development of a Virtual Reality Simulator for an Intelligent Robotic System Used in Ankle Rehabilitation. Sensors 2021, 21, 1537. https://doi.org/10.3390/s21041537
Covaciu F, Pisla A, Iordan A-E. Development of a Virtual Reality Simulator for an Intelligent Robotic System Used in Ankle Rehabilitation. Sensors. 2021; 21(4):1537. https://doi.org/10.3390/s21041537
Chicago/Turabian StyleCovaciu, Florin, Adrian Pisla, and Anca-Elena Iordan. 2021. "Development of a Virtual Reality Simulator for an Intelligent Robotic System Used in Ankle Rehabilitation" Sensors 21, no. 4: 1537. https://doi.org/10.3390/s21041537