
Standardized Computer-Assisted Analysis of PRAME Immunoreactivity in Dysplastic Nevi and Superficial Spreading Melanomas
 ,
,  ,
,
Abstract
:1. Introduction
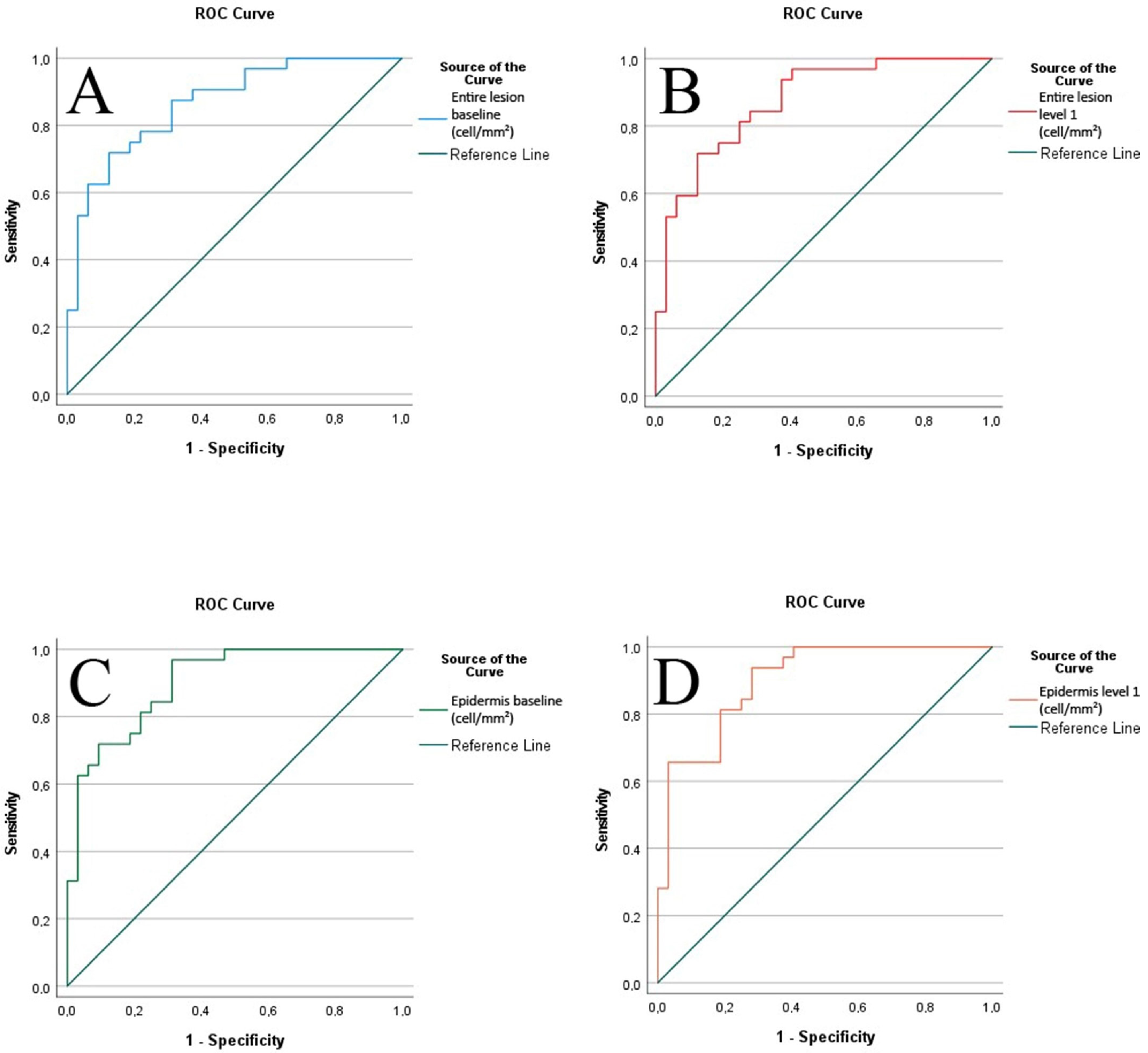
2. Results
3. Discussion
4. Materials and Methods
4.1. Immunohistochemistry
4.2. Image Data Acquisition
4.3. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Botti, G.; Marra, L.; Anniciello, A.; Scognamiglio, G.; Gigantino, V.; Cantile, M. Immune-phenotypical markers for the differential diagnosis of melanocytic lesions. Int. J. Clin. Exp. Pathol. 2015, 8, 9742–9751. [Google Scholar]
- Dinehart, M.S.; Dinehart, S.M.; Sukpraprut-Braaten, S.; High, W.A. Immunohistochemistry utilization in the diagnosis of melanoma. J. Cutan. Pathol. 2020, 47, 446–450. [Google Scholar] [CrossRef] [PubMed]
- Dass, S.E.; Huizenga, T.; Farshchian, M.; Mehregan, D.R. Comparison of SOX-10, HMB-45, and Melan-A in Benign Melanocytic Lesions. Clin. Cosmet Investig. Dermatol. 2021, 14, 1419–1425. [Google Scholar] [CrossRef] [PubMed]
- Rodic, N.; Zampella, J.; Sharma, R.; Burns, K.H.; Taube, J.M. Diagnostic utility of 5-hydroxymethylcytosine immunohistochemistry in melanocytic proliferations. J. Cutan. Pathol. 2015, 42, 807–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.J.; Vilain, R.E.; Granter, S.R.; Hu, N.R.; Bresler, S.C.; Xu, S.; Frank, A.H.; Mihm, M.C., Jr.; Saw, R.P.; Fletcher, C.D.; et al. 5-Hydroxymethylcytosine is a nuclear biomarker to assess biological potential in histologically ambiguous heavily pigmented melanocytic neoplasms. J. Cutan. Pathol. 2017, 44, 249–255. [Google Scholar] [CrossRef]
- Hilliard, N.J.; Krahl, D.; Sellheyer, K. p16 expression differentiates between desmoplastic Spitz nevus and desmoplastic melanoma. J. Cutan. Pathol. 2009, 36, 753–759. [Google Scholar] [CrossRef]
- Rawson, R.V.; Shteinman, E.R.; Ansar, S.; Vergara, I.A.; Thompson, J.F.; Long, G.V.; Scolyer, R.A.; Wilmott, J.S. Diagnostic utility of PRAME, p53 and 5-hmC immunostaining for distinguishing melanomas from naevi, neurofibromas, scars and other histological mimics. Pathology 2022, 54, 863–873. [Google Scholar] [CrossRef]
- Roszik, J.; Wang, W.L.; Livingston, J.A.; Roland, C.L.; Ravi, V.; Yee, C.; Hwu, P.; Futreal, A.; Lazar, A.J.; Patel, S.R.; et al. Overexpressed PRAME is a potential immunotherapy target in sarcoma subtypes. Clin. Sarcoma Res. 2017, 7, 11. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Barger, C.J.; Eng, K.H.; Klinkebiel, D.; Link, P.A.; Omilian, A.; Bshara, W.; Odunsi, K.; Karpf, A.R. PRAME expression and promoter hypomethylation in epithelial ovarian cancer. Oncotarget 2016, 7, 45352–45369. [Google Scholar] [CrossRef] [Green Version]
- Pujol, J.L.; De Pas, T.; Rittmeyer, A.; Vallieres, E.; Kubisa, B.; Levchenko, E.; Wiesemann, S.; Masters, G.A.; Shen, R.; Tjulandin, S.A.; et al. Safety and Immunogenicity of the PRAME Cancer Immunotherapeutic in Patients with Resected Non-Small Cell Lung Cancer: A Phase I Dose Escalation Study. J. Thorac. Oncol. 2016, 11, 2208–2217. [Google Scholar] [CrossRef] [Green Version]
- Cazzato, G.; Mangialardi, K.; Falcicchio, G.; Colagrande, A.; Ingravallo, G.; Arezzo, F.; Giliberti, G.; Trilli, I.; Loizzi, V.; Lettini, T.; et al. Preferentially Expressed Antigen in Melanoma (PRAME) and Human Malignant Melanoma: A Retrospective Study. Genes 2022, 13, 545. [Google Scholar] [CrossRef]
- Ricci, C.; Franceschini, T.; Giunchi, F.; Grillini, M.; Ambrosi, F.; Massari, F.; Mollica, V.; Colecchia, M.; Fiorentino, M. Immunohistochemical Expression of Preferentially Expressed Antigen in Melanoma (PRAME) in the Uninvolved Background Testis, Germ Cell Neoplasia In Situ, and Germ Cell Tumors of the Testis. Am. J. Clin. Pathol. 2022, 157, 644–648. [Google Scholar] [CrossRef]
- Xu, Y.; Zou, R.; Wang, J.; Wang, Z.W.; Zhu, X. The role of the cancer testis antigen PRAME in tumorigenesis and immunotherapy in human cancer. Cell Prolif. 2020, 53, e12770. [Google Scholar] [CrossRef]
- Gezgin, G.; Luk, S.J.; Cao, J.; Dogrusoz, M.; van der Steen, D.M.; Hagedoorn, R.S.; Krijgsman, D.; van der Velden, P.A.; Field, M.G.; Luyten, G.P.M.; et al. PRAME as a Potential Target for Immunotherapy in Metastatic Uveal Melanoma. JAMA Ophthalmol. 2017, 135, 541–549. [Google Scholar] [CrossRef]
- Alomari, A.K.; Tharp, A.W.; Umphress, B.; Kowal, R.P. The utility of PRAME immunohistochemistry in the evaluation of challenging melanocytic tumors. J. Cutan. Pathol. 2021, 48, 1115–1123. [Google Scholar] [CrossRef] [PubMed]
- Koh, S.S.; Lau, S.K.; Scapa, J.V.; Cassarino, D.S. PRAME immunohistochemistry of spitzoid neoplasms. J. Cutan. Pathol. 2022, 49, 709–716. [Google Scholar] [CrossRef] [PubMed]
- Raghavan, S.S.; Wang, J.Y.; Kwok, S.; Rieger, K.E.; Novoa, R.A.; Brown, R.A. PRAME expression in melanocytic proliferations with intermediate histopathologic or spitzoid features. J. Cutan. Pathol. 2020, 47, 1123–1131. [Google Scholar] [CrossRef] [PubMed]
- Gassenmaier, M.; Hahn, M.; Metzler, G.; Bauer, J.; Yazdi, A.S.; Keim, U.; Garbe, C.; Wagner, N.B.; Forchhammer, S. Diffuse PRAME Expression Is Highly Specific for Thin Melanomas in the Distinction from Severely Dysplastic Nevi but Does Not Distinguish Metastasizing from Non-Metastasizing Thin Melanomas. Cancers 2021, 13, 3864. [Google Scholar] [CrossRef] [PubMed]
- Parra, O.; Linos, K.; Li, Z.; Yan, S. PRAME expression in melanocytic lesions of the nail. J. Cutan. Pathol. 2022, 49, 610–617. [Google Scholar] [CrossRef]
- Plotzke, J.M.; Zoumberos, N.A.; Hrycaj, S.M.; Harms, P.W.; Bresler, S.C.; Chan, M.P. PRAME expression is similar in scar and desmoplastic melanoma. J. Cutan. Pathol. 2022, 49, 829–832. [Google Scholar] [CrossRef] [PubMed]
- Ruby, K.N.; Li, Z.; Yan, S. Aberrant expression of HMB45 and negative PRAME expression in halo nevi. J. Cutan. Pathol. 2021, 48, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Lohman, M.E.; Steen, A.J.; Grekin, R.C.; North, J.P. The utility of PRAME staining in identifying malignant transformation of melanocytic nevi. J. Cutan. Pathol. 2021, 48, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Gradecki, S.E.; Slingluff, C.L., Jr.; Gru, A.A. PRAME expression in 155 cases of metastatic melanoma. J. Cutan. Pathol. 2021, 48, 479–485. [Google Scholar] [CrossRef]
- Ahmadian, S.S.; Dryden, I.J.; Naranjo, A.; Toland, A.; Cayrol, R.A.; Born, D.E.; Egbert, P.S.; Brown, R.A.; Mruthyunjaya, P.; Lin, J.H. Preferentially Expressed Antigen in Melanoma Immunohistochemistry Labeling in Uveal Melanomas. Ocul. Oncol. Pathol. 2022, 8, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Googe, P.B.; Flanigan, K.L.; Miedema, J.R. Preferentially Expressed Antigen in Melanoma Immunostaining in a Series of Melanocytic Neoplasms. Am. J. Dermatopathol. 2021, 43, 794–800. [Google Scholar] [CrossRef] [PubMed]
- Gradecki, S.E.; Valdes-Rodriguez, R.; Wick, M.R.; Gru, A.A. PRAME immunohistochemistry as an adjunct for diagnosis and histological margin assessment in lentigo maligna. Histopathology 2021, 78, 1000–1008. [Google Scholar] [CrossRef] [PubMed]
- Tio, D.; Willemsen, M.; Krebbers, G.; Kasiem, F.R.; Hoekzema, R.; van Doorn, R.; Bekkenk, M.W.; Luiten, R.M. Differential Expression of Cancer Testis Antigens on Lentigo Maligna and Lentigo Maligna Melanoma. Am. J. Dermatopathol. 2020, 42, 625–627. [Google Scholar] [CrossRef]
- Grillini, M.; Ricci, C.; Pino, V.; Pedrini, S.; Fiorentino, M.; Corti, B. HMB45/PRAME, a Novel Double Staining for the Diagnosis of Melanocytic Neoplasms: Technical Aspects, Results, and Comparison With Other Commercially Available Staining (PRAME and Melan A/PRAME). Appl. Immunohistochem. Mol. Morphol. 2022, 30, 14–18. [Google Scholar] [CrossRef]
- Olds, H.; Utz, S.; Abrams, J.; Terrano, D.; Mehregan, D. Use of PRAME immunostaining to distinguish early melanoma in situ from benign pigmented conditions. J. Cutan. Pathol. 2022, 49, 510–514. [Google Scholar] [CrossRef]
- Lezcano, C.; Jungbluth, A.A.; Nehal, K.S.; Hollmann, T.J.; Busam, K.J. PRAME Expression in Melanocytic Tumors. Am. J. Surg. Pathol. 2018, 42, 1456–1465. [Google Scholar] [CrossRef]
- Bankhead, P.; Loughrey, M.B.; Fernandez, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open source software for digital pathology image analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, J.V.; Pan, J.; Rai, S.N.; Galandiuk, S. ROC-ing along: Evaluation and interpretation of receiver operating characteristic curves. Surgery 2016, 159, 1638–1645. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Evaluation cohort | Superficial spreading melanoma | Dysplastic nevus | ||
| N | 32 | 32 | ||
| Tumor thickness | Mean: 0.42 mm | |||
| Standard deviation: 0.2 mm | ||||
| Nevus type | Junctional nevus: 90.6% (29/32) | |||
| Compound nevus: 9.4% (3/32) | ||||
| Location (n) | Head/Neck: 3 | Head/Neck: 3 | ||
| Trunk: 14 | Trunk: 18 | |||
| Upper extremities: 10 | Upper extremities: 6 | |||
| Lower extremities: 5 | Lower extremities: 5 | |||
| Gender (n) | Female: 18 | Female: 18 | ||
| Male: 14 | Male: 14 | |||
| Age | Mean: 57.56 years | Mean: 54.16 years | ||
| Standard deviation: 14.2 | Standard deviation: 20.1 | |||
| Validation cohort | Superficial spreading melanoma | Dysplastic nevus | ||
| N | 8 | 9 | ||
| Tumor thickness | Mean: 0.66 mm | |||
| Standard deviation: 0.39 mm | ||||
| Nevus type | Junctional nevus: 44.4% (4/9) | |||
| Compound nevus: 55.6% (5/9) | ||||
| Location | Head/Neck: 1 | Head/Neck: 0 | ||
| Trunk: 3 | Trunk: 6 | |||
| Upper extremities: 0 | Upper extremities: 2 | |||
| Lower extremities: 4 | Lower extremities: 1 | |||
| Gender (n) | Female: 4 | Female: 2 | ||
| Male: 4 | Male: 7 | |||
| Age | Mean: 57.75 years | Mean: 52.9 years | ||
| Standard deviation: 22.1 | Standard deviation: 22.4 | |||
| Evaluation Cohort | Diagnosis | N | Mean | Standard Deviation | Standard Error of the Mean | t-Test (Two-Sided) |
|---|---|---|---|---|---|---|
| Entire lesion (positive cells/mm2) | DN | 32 | 60.5 | 130.1 | 23 | p < 0.001 |
| SMM | 32 | 455.3 | 428.2 | 75.6 | ||
| Epidermis (positive cells/mm2) | DN | 32 | 70.3 | 156.8 | 27.7 | p < 0.001 |
| SMM | 32 | 656.3 | 612.9 | 108.3 |
| Validation Cohort | Positive Cells/mm2—Entire Lesion | Expected Coordinate in ROC: Sensitivity | Expected Coordinate in ROC: 1-Specificity | Prediction According to Cut-Off Value (K-S-Test) of 97.7 Positive Cells/mm2 | Correct Prediction | Accuracy |
|---|---|---|---|---|---|---|
| Sample 1 | 413.73 | 0.438 | 0.031 | Melanoma | Yes | 94.1% |
| Sample 2 | 0 | 1.000 | 1.000 | Nevus | Yes | |
| Sample 3 | 1406.9 | 0.000 | 0.000 | Melanoma | Yes | |
| Sample 4 | 131.17 | 0.625 | 0.063 | Melanoma | Yes | |
| Sample 5 | 0 | 1.000 | 1.000 | Nevus | Yes | |
| Sample 6 | 1747 | 0.000 | 0.000 | Melanoma | Yes | |
| Sample 7 | 0 | 1.000 | 1.000 | Nevus | Yes | |
| Sample 8 | 1959.5 | 0.000 | 0.000 | Melanoma | Yes | |
| Sample 9 | 2219.6 | 0.000 | 0.000 | Melanoma | Yes | |
| Sample 10 | 0 | 1.000 | 1.000 | Nevus | Yes | |
| Sample 11 | 57.13 | 0.781 | 0.313 | Nevus | Yes | |
| Sample 12 | 0 | 1.000 | 1.000 | Nevus | Yes | |
| Sample 13 | 89.49 | 0.750 | 0.219 | Nevus | No | |
| Sample 14 | 887 | 0.188 | 0.000 | Melanoma | Yes | |
| Sample 15 | 31.42 | 0.906 | 0.406 | Nevus | Yes | |
| Sample 16 | 0 | 1.000 | 1.000 | Nevus | Yes | |
| Sample 17 | 37.1 | 0.875 | 0.375 | Nevus | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koch, E.A.T.; Erdmann, M.; Berking, C.; Kiesewetter, F.; Kramer, R.; Schliep, S.; Heppt, M.V. Standardized Computer-Assisted Analysis of PRAME Immunoreactivity in Dysplastic Nevi and Superficial Spreading Melanomas. Int. J. Mol. Sci. 2023, 24, 6388. https://doi.org/10.3390/ijms24076388
Koch EAT, Erdmann M, Berking C, Kiesewetter F, Kramer R, Schliep S, Heppt MV. Standardized Computer-Assisted Analysis of PRAME Immunoreactivity in Dysplastic Nevi and Superficial Spreading Melanomas. International Journal of Molecular Sciences. 2023; 24(7):6388. https://doi.org/10.3390/ijms24076388
Chicago/Turabian StyleKoch, Elias A. T., Michael Erdmann, Carola Berking, Franklin Kiesewetter, Rafaela Kramer, Stefan Schliep, and Markus V. Heppt. 2023. "Standardized Computer-Assisted Analysis of PRAME Immunoreactivity in Dysplastic Nevi and Superficial Spreading Melanomas" International Journal of Molecular Sciences 24, no. 7: 6388. https://doi.org/10.3390/ijms24076388