
Pharmacokinetic Markers of Clinical Outcomes in Severe Mental Illness: A Systematic Review

 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
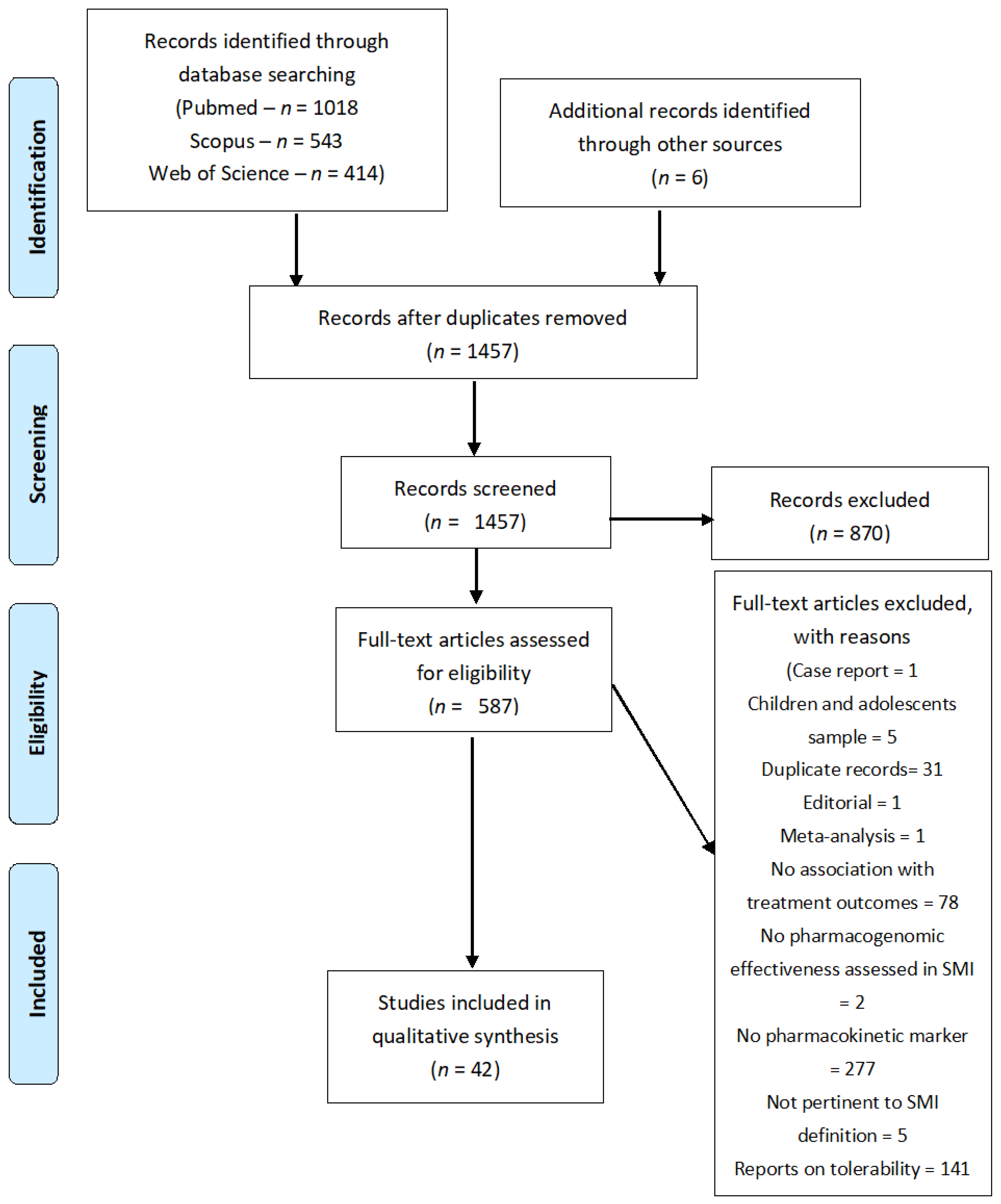
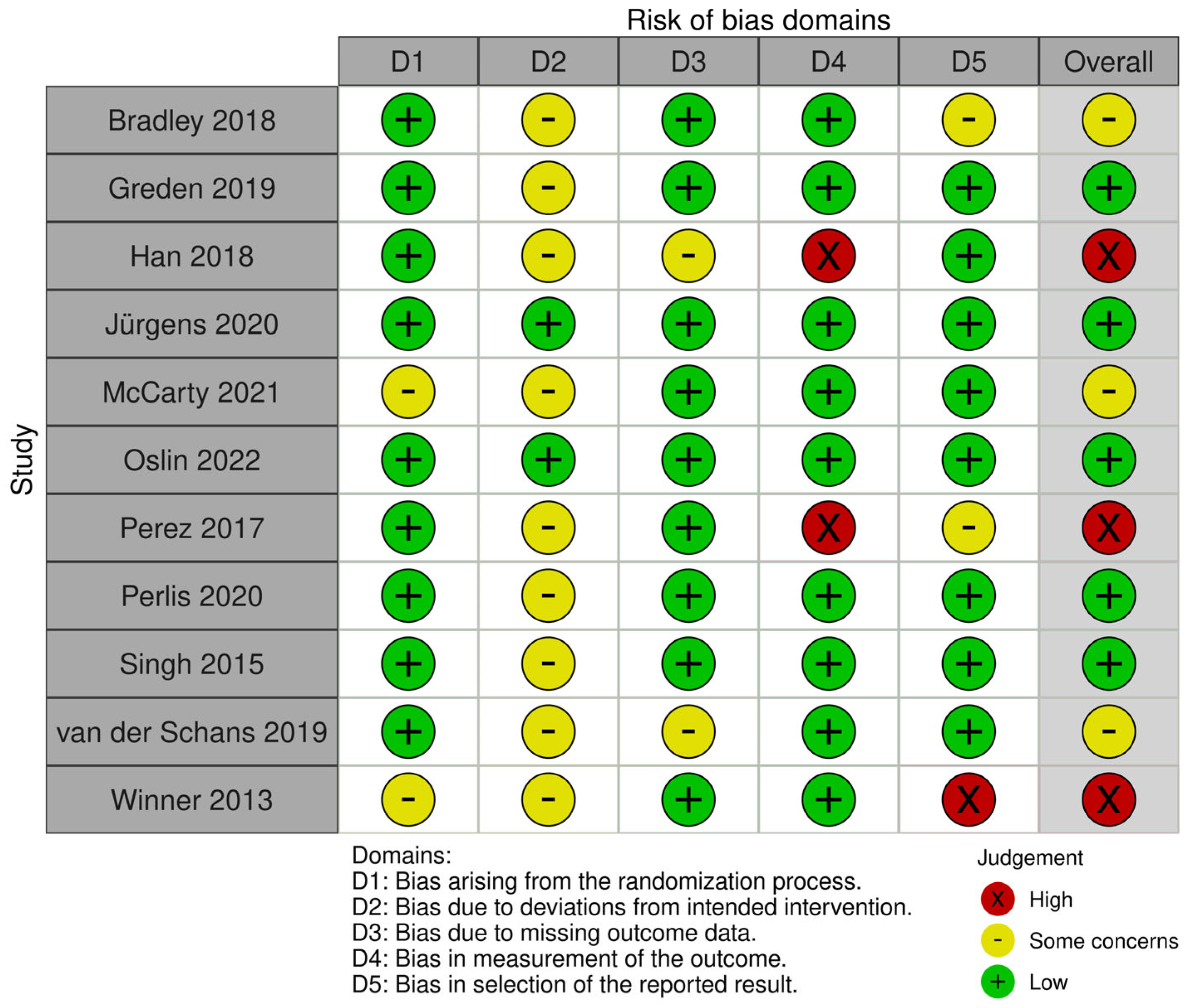
3.1. Search Results and Bias Assessment
3.2. PGx Outcomes
3.2.1. Schizophrenia

| Author, Year | Study Design | Sample Size | Sample Characteristics | Diagnostic Category | Main Outcomes Reported | Inclusion Criteria | Exclusion Criteria | Country | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Almoguera et al., 2013 [45] | Open-label study | 75 | M 41, F 34; -<40 y.o. (n = 25) -40–59 y.o. (n = 39) - ≥ 60 y.o. (n = 11) | SCZ (DSM-IV) | Association of PGx test and RIS treatment outcomes | -Admitted to an acute inpatient unit | N/A | SPN | CYP2D6 poor metabolism appeared to be associated with greater T-PANSS improvement |
| Gregoor et al., 2013 [46] | Case–control study | 528 | -Cases n =222 (M 151, F 71) -Controls n = 306 (M 161, F 145) | SCZ (DSM-IV) | Association of CYP2D6 phenotypes and probability of switching to CLZ | -Psychotic disorder -Received two AP trials of at least one month each | N/A | NET | No statistically significant association between CYP2D6 phenotypes and outcomes |
| Grossman et al., 2008 [55] | CATIE Cohort | 708 | See Suppl. Material | SCZ (DSM-IV) | Association of 25 functional variants in metabolizing enzymes with treatment outcomes | -18–65 y.o. | -Intolerance or no response to treatments -Pregnancy, breastfeeding | USA | No association with treatment efficacy |
| Jürgens et al., 2020 [30] | RCT | 669 | -GGT n = 95 (mean age: 42 y.o.) -SCM n = 94 (mean age: 40 y.o.) -CG n = 101 (mean age: 42 y.o.) | SCZ | Association of CYP2D6 or CYP2C19 phenotypes and 1-year AP treatment outcome | -No previous PGx testing -≥ 18 y.o. | -Not adherent to the treatment protocol | DEN | No association between the tested phenotypes and treatment outcomes |
| Jovanović et al., 2010 [47] | Open-label study | 83 | M 17, F 66 (mean age 30.3 ± 8.1 y.o.) | SCZ (DSM-IV) | Association of CYP2D6 (*3,*4,*6), ABCB1 (G2677T/A and C3435T) genotypes with 8-week RIS treatment outcomes | -FEP -No prior AP exposure -Oral RIS -Diazepam and biperiden only two medications allowed | N/A | CRO | No statistically significant association between the tested polymorphisms and symptom change |
| Kaur et al., 2017 [48] | Open-label study | 443 | M 262, F 157 (mean age: 31.3 ± 9.5 y.o.) | SCZ (DSM-IV) | Association of CYP2D6 phenotype with 12- week RIS treatment outcomes (response T-PANSS ≥ 50% from baseline) | -18–55 y.o. -Caregiver that could monitor treatment adherence | -SUD other than tobacco -MR -LAI -Metabolic syndrome -Severe medical or surgical co-morbidity | IND | CYP2D6*4 polymorphism frequency differed significantly in terms of T-PANSS change when drop-outs were excluded from the analysis |
| Lesche et al., 2019 [56] | Retrospective cohort study | 66 | M 48, F 18 (mean age: 40 ± 10 y.o.) | SCZ (DSM-IV) | Association of CYP1A2, CYP2D6, CYP2C19 phenotypes with CLZ treatment outcomes (T-PANSS score) | -On CLZ treatment -18–65 y.o. | N/A | AUT | CYP1A2, CYP2D6, CYP2C19 activity score impact appears limited compared to nongenetic factors |
| Lin et al., 2006 [58] | Open-label study | 41 | M 33, 8 F (mean age 35.6 ± 8.8 y.o.) | SCZ (DSM-IV) | Association of three PGP polymorphisms and 6-week OLA treatment outcomes (% change BPRS) | -18–65 y.o. -BPRS ≥ 42 | -SUD -Unstable medical illness | USA | For ABCB1 3435T carriers, OLA plasma levels correlated with % BPRS change |
| Lu et al., 2021 [49] | Open-label study | 76 | M 38, F 38–mean age: 45 y.o. | SCZ | Association of CYP2D6 phenotypes and 8-week RIS treatment | -No AP exposure for 1 year and recent hospital admission | -ECT in the 3 months prior to enrollment -Medical illnesses | CHN | Significant changes in PANSS score between CYP2D6 phenotypes |
| Müller et al., 2012 [50] | Retrospective cohort study | 35 SCZ, 39 OCD | N/A | SCZ, OCD (DSM-IV) | Association of pharmacokinetic markers and treatment response | N/A | N/A | CAN | No statistically significant association between CYP2D6 phenotypes and treatment outcomes |
| Nikisch et al., 2011 [57] | Open-label study | 22 | M 14, 8 F (age range: 22–49 y.o.) | SCZ (DSM-IV) | Association of clinical response with ABCB1 with 4-week quetiapine treatment outcomes (PANSS change) | -PANSS ≥ 60 -CGI ≥ 2 -Started on QUE | -Other DSM-IV Axis I diagnosis -CLZ -LAI -Severe somatic conditions | GER | Noncarriers of the 3435TT genotype showed greater changes in the PANSS score |
| Nozawa et al., 2008 [51] | Open-label study | 51 | M 34, F 17 (mean age: 32.6 ± 9.6 y.o.) | SCZ (DSM-IV) | Association functional polymorphisms of UGT1A4, CYP1A2, and CYP2D6 with OLA treatment outcomes | N/A | N/A | JPN | No association between the tested genotypes and BPRS change |
| Rajkumar et al., 2012 [59] | Retrospective cohort study | 101 | CLZ duration 4–174 months (73 M, 28 F; mean age: 35.4 ± 9.4 y.o.) | SCZ (DSM-IV) | CYP1A2 SNP and treatment response | -TRS -Stable dose of clozapine for at least 12 weeks -South Indian ethnicity | -Neurological illnesses -Intellectual disability -Sensory impairment precluding the assessment | IND | No association with clozapine treatment response |
| Vijayan et al., 2012 [53] | Case–control study | 192 | Dravidian (responders: n = 130 (68%), nonresponders n = 62 (32%)) | SCZ (DSM-IV) | Association of ABCB1 gene polymorphisms with treatment response after 1 year AP | N/A | -SAD -Neurological or general medical condition that may precipitate psychotic symptoms | IND | Homozygous genotypes of rs1045642 and rs2032582 were associated with a better response |
| Xing et al., 2006 [54] | Open-label study | 130 | Han Chinese (45 M, 85 F; mean age 36.27 ± 11.18 y.o.) | SCZ (DSM-IV) | Association of nine polymorphisms of ABCB1 gene with % BPRS improvement on RIS therapy | N/A | -No physical complications or other psychiatric co-morbidity, TRS -No previous exposure to 2nd GEN-AP | CHN | Individuals with C1236T TT genotype (rs1128503) presented higher % improvements |
| Xu et al., 2016 [52] | Open-label study | 995 | Han Chinese | SCZ (DSM-IV) | Association of 77 single-nucleotide polymorphisms of 25 candidate genes and treatment response | N/A | -Physical co-morbidity -SUD -TRS -No previous AP exposure | CHN | Several associations emerged with various genes |
| Yasui-Furukori et al., 2006 [60] | Open-label study | 33 | Inpatients (mean age 37.3 ± 12.8 y.o.) | SCZ (DSM-IV) | Association of MDR1 gene polymorphisms and clinical response to BPD (BPRS score change) | -BPRS ≥ 18 -No psychotropics four weeks before enrolment | -Psychiatric co-morbidity -Epilepsy -AUD, SUD -Significant physical or neurological disorders | JPN | -No association of symptom improvement with the C3435T genotypes |
3.2.2. Major Depressive Disorder
| Author, Year | Study Design | Sample Size | Sample Characteristics | Diagnostic Category | Main Outcomes Reported | Inclusion Criteria | Exclusion Criteria | Country | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Altar et al., 2015 [41] | Secondary analysis—open-label trial | 334 | -81 La Crosse -18 Hamm Clinic -20 Pine Rest -119 TAU -96 chart review | MDD | Combinatorial PGx test of four CYP450 enzymes, SLC6A4, and HTR2A (mean change HDRS score) | -18–75 y.o. -HDRS ≥ 14 -Failed one medication trial | -SCZ, BD I, SCA | USA | The combinatorial PGx test discriminated between poor and good treatment outcomes |
| Bradley et al., 2018 [31] | RCT | 685 | -GGT n = 352 (M 95, F 257, mean age: 47.8 ± 14.5 -TAU n = 333 (M 92, F 241, mean age: 47.3 ± 15.2) | MDD and anxiety (DSM-5, unclear anxiety diagnosis) | Association of the NeuroIDgenetix test with 12-week treatment outcomes (remission HDRS ≤ 7, response HDRS change ≥ 50%) | -19–87 y.o. -Undergoing a new trial of AD (either as first or subsequent treatment trials) | -BD, SCZ, PD -Traumatic brain injury -Chronic kidney disease stages 4–5 -Malabsorption -Pregnancy -Abnormal hepatic functioning -High risk of suicide | USA | GGT group presented a higher remission and response rate for depression |
| Breitenstein et al., 2014 [61] | Open-label study | 116 | -GGT n = 58 M 26, F 32 (mean age: 48.5 ± 15.1) -Control n = 58-M 26, F 32 (mean age: 46.5 ± 14.6) | MDD | Association of ABCB1 polymorphism testing and AD treatment outcomes (hospital stay, mean HDRS change) | -Admission to the involved hospital and ABCB1 testing | N/A | GER | ABCB1 test was associated with lower HDRS scores; rs2032583, rs2235015, and dose increase were associated with shorter hospital stays |
| Calabrò et al., 2022 [62] | Retrospective cohort study | 540 | Mean age: 52.2 ± 14.2 | MDD (DSM-IV) | Association of CYP2C19 phenotypes and treatment outcomes (response MDRS ≥ 50% change and MDRS < 22–TRD ≥ ineffective two trials of 4-week duration) | -MDRS 22 after adequate, 4-week AD trial | -SUD active previous six months | ITA | PM presented higher response and remission |
| Dong et al., 2009 [63] | Open-label study | 272 | Mean age: 38 ± 10 y.o. | MDD (DSM-IV) | Association of five SNPs of ABCB1 gene with 8-week DES or FLX therapy (remission HDRS < 8) | -HDRS ≥ 18 | -Active medical illness -High suicide risk -Pregnancy or breastfeeding -BDZ or AD treatment in the two weeks prior to enrollment -Illicit drug use in the three months before enrollment -Current involvement in psychotherapy -No Mexican American heritage | USA | No association between treatment outcomes and the tested ABCB1 SNPs |
| Forester et al., 2020 [42] | Post hoc analysis—GUIDED cohort | 206 | M 56, F 150 (mean age: 49.4 ± 4.4 y.o.) | MDD (DSM-IV) | Association of combinatorial PGx testing and treatment outcomes with 24 weeks’ AD treatment among ≥ 65 y.o. (response HDRS ≥ 50% change from baseline, remission HDRS ≤ 7) | -≥18 y.o. -Inadequate response to AD treatment of ≥6 weeks’ duration or intolerability -QIDS-C16 and QIDS-SR ≥11 -Follow the protocol | -High suicide risk -BD I or II -Delirium, dementia, SCZ, or psychotic disorders -Psychotic features -Inpatient -Prior PGx test -Pregnancy or breastfeeding -ECT, DBS, or TMS -Gastric bypass -Unstable medical illness | USA | Higher remission and response rates at eight weeks of treatment |
| Greden et al., 2019 [36] | RCT | 1167 | -GGT 717—M 219, F 498 -TAU 618—M 192, F 489 | MDD | Association of PGx testing (Genesight) with 24-week treatment outcomes (remission HDRS ≤ 7, QIDS-C16 ≤ 5, PHQ-9 ≤ 5) | -≥18 y.o. -QIDS-C16 and QIDS-SR16 ≥ 11 -At least one medication trial with inadequate response | -High suicide risk -Psychiatric or cognitive co-morbidity -HDRS ≤ 14 | USA | GGT did not improve symptom severity change but improved remission and response rates |
| Gressier et al., 2014 [64] | Open-label study | 87 | -UM n= 11 -EM n = 141 -PM n = 21 | MDD (DSM-IV) | Association of 4 weeks of flexible AD treatment and CYP2D6 genotypes (% HDRS change and CGI-I). | -≥18 y.o. -HDRS ≥ 18 | -Psychotic disorder -Brain disorders or unstable physical illness -SUD | FRA | No association between the studied phenotypes and treatment outcomes. Ultrarapid carriers taking CYP2D6 inhibitors had lower AD responses compared with the other genotypes |
| Han et al., 2013 [33] | Open-label study | 94 | -PP n = 28 (mean age: 48.2 ± 17.7) -PS n = 38 (mean age: 44.9 ± 15.2) -SS n = 28 (mean age: 44.8 ± 15.5) | MDD (DSM-IV) | Association of CYP2D6 P34S with 12-week ESC treatment outcomes (response HDRS ≥ 50% change from baseline) | -HDRS ≥ 18 | -SCZ, SCZ, psychotic features in the past six months, BD, dementia -Personal or family history of AUD or SUD | SKR | P allele associated with better ESC treatment outcome as compared with the others |
| Jeon et al., 2009 [65] | Open-label trial | 153 | M 38, F 115 | MDD (DSM-IV) | Association of CYP2D6 P34S polymorphisms and 12-week mirtazapine treatment outcomes (remission—unspecified criteria, HDRS and CGI-S % change) | -HDRS ≥ 18 -≥ 18 y.o. | -SCA, SCZ, AUD, SUD, dementia -Personal or family history of SUD -Use of BDZ or MS | SKR | S allele was associated with smaller changes in HDRS and CGI-S scores |
| Kato et al., 2008 [66] | Open-label study | 68 | N/A | MDD (DSM-IV) | Association of three ABCB1 polymorphisms with 6-week PAR treatment outcomes (HDRS % change from baseline) | N/A | -SUD other than tobacco -Unstable medical illness -Pregnancy -ECT in the six months prior to enrollment | JPN | The ABCB1 G2677T/A genotype appeared to be associated with symptom changes |
| Lin et al., 2010 [67] | Open-label study | 241 | Han Chinese (mean age: 41 y.o.) | MDD (DSM-IV) | Association of CYP1A2 genetic polymorphisms with 8-week PAR treatment outcomes (HDRS ≤ 7, HAM-A ≤ 17, CGI-S ≤ 2) | -HDRS ≥ 14 -No previous PAR exposure | -SCZ, SCA, SUD, dementia | TWN | Three SNPs appeared to be associated with MDD remission |
| McCarthy et al., 2021 [32] | RCT | 182 | -GGT n = 75, (mean age: 52.5 ± 1.5 y.o.) -TAU n = 74 (mean age: 50.3 ± 1.6 y.o.) | MDD, BD, PTSD | Association of PGx markers and pharmacological treatment outcomes (CGI change with AD, AP, MS treatment) | -Failure of one or more first-line medications (AD or MS) | N/A | USA | No statistically significant difference in GGT vs. TAU response |
| Oslin et al., 2022 [37] | RCT | 1944 | -GGT (n = 966, M 737, F 229, mean age: 48 y.o.), -TAU (n = 978, M 716, F 262, mean age: 47 y.o.) | MDD | Efficacy of GGT in improving outcomes for MDD treatment (remission PHQ-9 ≤ 5) | -Receiving care at VAMC -18 to 80 y.o. -MDD with at least one previous episode -New trial of AD monotherapy | -SUD -BD -Psychosis -BOR, ASO -AP, buprenorphine or naltrexone augmentation -No bank account for payments | USA | Small nonpersistent improvement in remission rate for GGT as compared with TAU |
| Singh et al., 2015 [39] | RCT | 148 | -GGT n = 74 (M 31, F 43; mean age: 44.2) -TAU n = 74 (M 28, F 46; mean age: 44.3) | MDD (DSM-5) | Association of PGx with 12-week treatment outcomes between GGT and TAU (HDRS ≤7) | -HDRS < 18 | -Psychotic disorders -BD -SUD -PD | AUS | Higher remission rates in the GGT group as compared with TAU |
| Pérez et al., 2017 [34] | RCT | 316 | M 115, F 201 -GGT (n = 155, mean age: 51.7 ± 12.0 y.o.) -TAU (n = 161, mean age: 50.7 ± 13.1 y.o.) | MDD (DSM-IV) | Association of PGx panel (Neuropharmagen®), with treatment outcomes (PGI-I ≤ 2 after 12-week AD treatment) | -CGI-S ≥ 4 -MDD -Starting a new treatment trial or medication switch | -No MDD diagnosis -Pregnancy -Breastfeeding -Treatment with strong 2D6 inhibitors (i. e. quinidine, cinacalcet, and/or terbinafine) | SPN | Higher treatment response in GGT as compared to TAU at 12 weeks |
| Perlis et al., 2010 [38] | Secondary analysis | 250 | M 92, F 158 (mean age: 44.2 ± 12.6 y.o.) | MDD (DSM-IV) | Association of polymorphisms of the PDE1A, PDE1C, PDE6A, PDE11A, ABCB1, GRIK4, SLC6A4, OPRM1 genes with 7-week DUL treatment (HDRS score change) | -HDRS ≥ 15 allowed co-morbid GAD | -OCD | USA | Polymorphisms in PDE1A, PDE1C, PDE6A, PDE11A, ABCB1, GRIK4, SLC6A4, and OPRM1 genes showed no statistically significant associations with duloxetine treatment response |
| Perlis et al., 2020 [68] | RCT | 304 | -GGT n = 151 (M 44, F 107; mean age: 47.8 ± 12.3) -TAU n = 153 (M 42, F 111; mean age: 47.6 ± 12.0) | MDD (DSM-IV) | Association of PGx test (Genecept Assay version 2.0) with 8-week AD treatment outcomes (change in SIGH-D-17 from baseline) | -SIGH-D-17 ≥ 18 -18–75 y.o. -Failure of at least one AD trial of adequate duration/dose | -Neurocognitive disorders, SCZ spectrum, personality disorders, BD, trauma disorders, PD | USA | No statistically significant difference in the SIGH-D-17 change between GGT and TAU |
| Ruano et al., 2013 [69] | Open-label study | 149 | Inpatients, M 58, F 91 | MDD (DSM-IV) | Association of CYP2D6 metabolism rate and hospitalization length (CIT 34.9%, QUE 31.5%, RIS 29.5, TRA 25.5%, VNL 18.8%, BUP 17.4%, SER 12.8%, FLX 12.8%, MRT 8.7%, ARI 4.7%, OLA 3.4%, TCAs 3.4%, ZIP 3.4%, PAR 3.4%) | -MDD requiring hospitalization | N/A | USA | Longer hospital stays among individuals with deficient CYP2D6 metabolism |
| Tiwari et al., 2022 [43] | RCT | 371 | M 98, F 178; (mean age: 41.1 ± 14.1 y.o.) | MDD (DSM-IV) | Evaluated GGT vs. TAU after eight weeks of AD treatment (mean % HDRS change) | -≥18 y.o. -Inadequate response to at least one psychotropic included in the GGT test panel -QIDS-C16 score ≥11 at screening -QIDS-SR16 at screening and baseline | -Significant suicidal risk -Psychiatric or cognitive disorders, severe co-occurring psychiatric or cognitive disorders, and/or unstable or significant medical conditions | CAN | No difference in remission or response rate between GGT and TAU |
| Tsai et al., 2010 [70] | Open-label study | 100 | Han Chinese | MDD (DSM-IV-TR) | Association of CYP450 polymorphisms (*4, *5, and *10 on CYP2D6, *2, *3, and *17 on CYP2C19, and *18 on CYP3A4) and ESC response (remission HDRS ≤ 10 at 8 weeks) | -HDRS ≥14 -7-day washout AD | -Past failed trial on ESC | TWN | Intermediate CYP2D6 metabolism is associated with ↑ rates of remission |
| van der Schans et al., 2019 [40] | RCT | 106 | M 40, F 66 | MDD (DSM-IV) | Association of CYP2D6 genetic variations and treatment outcomes with NOR or VNL (QIDS-SR score change) | -≥ 60 y.o. | -AD other than VNL or NOR -Medications that may interact with VNL or NOR -AST or ALT elevations -<30 mL/min GFR | NET | No significant differences between genotypes for depression severity |
| Winner et al., 2013 [35] | RCT | 51 | -GGT= M 8, F 18 (mean age: 50.6 ± 14.6) -TAU= M 2 F 23 (mean age: 47.8 ± 13.9) | MDD (DSM-IV) | Association of PGx testing (Genesight) with 12-week treatment outcomes (response HDRS ≥ 50 % change, remission HDRS ≤ 7) | -HDRS ≥ 14 | -Requirement for inpatient treatment -ECT -SCZ, SCA, BD | USA | No statistically significant improvement for GGT as compared with TAU in remission |
3.2.3. Bipolar Disorder
| Author, Year | Study Design | Sample Size | Sample Characteristics | Diagnostic Category | Main Outcomes Reported | Inclusion Criteria | Exclusion Criteria | Country | Main Results |
|---|---|---|---|---|---|---|---|---|---|
| Callegari et al., 2019 [44] | Prospective cohort study | 30 | Mean age: 48 ± 15 y.o. | BD (DSM-IV) | Association of PGx testing with emergency service access (cost associated with emergency service use) | -CGI-S ≥ 3 -Discordant therapy compared to what was suggested by PGx therapy in the 12 months prior to study start -Concordant therapy with PGx in the 12 months after the beginning of the study | N/A | ITA | Significant cost savings associated with switching to PGx-concordant testing |
| Huilei et al., 2020 [71] | Open-label study | 200 | -GGT—M 68, F 31 -TAU—M 70, F 30 | BD (DSM-IV) | Association of CYP2D6 with 12-week pharmacological treatment outcomes (CGI-E) | -HDRS ≥ 20 | -Serious medical illness -≥2 failed treatment trials -Use of medications that might interact with practised treatment | CHN | GGT appeared to be associated with greater efficacy compared with TAU |
| McCarthy et al., 2021 [32] | RCT | 182 | -GGT n = 75, (mean age: 52.5 ± 1.5 y.o.) -TAU n = 74 (mean age: 50.3 ± 1.6 y.o.) | MDD, BD, PTSD | Association of PGx markers and pharmacological treatment outcomes (CGI change with AD, AP, MS treatment) | -Failure of one or more first-line medications (AD or MS) | N/A | USA | No statistically significant difference in GGT vs. TAU response |
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wainberg, M.L.; Lu, F.G.; Riba, M.B. Global Mental Health. Acad. Psychiatry 2016, 40, 647–649. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.K.; Hayes, R.D.; Perera, G.; Broadbent, M.T.; Fernandes, A.C.; Lee, W.E.; Hotopf, M.; Stewart, R. Life expectancy at birth for people with serious mental illness and other major disorders from a secondary mental health care case register in London. PLoS ONE 2011, 6, e19590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzales, L.; Kois, L.E.; Chen, C.; Lopez-Aybar, L.; McCullough, B.; McLaughlin, K.J. Reliability of the Term “Serious Mental Illness”: A Systematic Review. Psychiatr. Serv. 2022, 73, 1255–1262. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, D.; Hancock, K.J.; Kisely, S. The gap in life expectancy from preventable physical illness in psychiatric patients in Western Australia: Retrospective analysis of population based registers. BMJ 2013, 346, f2539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melo, A.P.S.; Dippenaar, I.N.; Johnson, S.C.; Weaver, N.D.; de Assis Acurcio, F.; Malta, D.C.; Ribeiro, A.L.P.; Junior, A.A.G.; Wool, E.E.; Naghavi, M.; et al. All-cause and cause-specific mortality among people with severe mental illness in Brazil’s public health system, 2000–15: A retrospective study. Lancet Psychiatry 2022, 9, 771–781. [Google Scholar] [CrossRef] [PubMed]
- Barcella, C.A.; Polcwiartek, C.; Mohr, G.H.; Hodges, G.; Sondergaard, K.; Niels Bang, C.; Andersen, M.P.; Fosbol, E.; Kober, L.; Schou, M.; et al. Severe mental illness is associated with increased mortality and severe course of COVID-19. Acta Psychiatr. Scand. 2021, 144, 82–91. [Google Scholar] [CrossRef]
- Fekadu, W.; Mihiretu, A.; Craig, T.K.J.; Fekadu, A. Multidimensional impact of severe mental illness on family members: Systematic review. BMJ Open 2019, 9, e032391. [Google Scholar] [CrossRef] [Green Version]
- Tirfessa, K.; Lund, C.; Medhin, G.; Hailemichael, Y.; Fekadu, A.; Hanlon, C. Food insecurity among people with severe mental disorder in a rural Ethiopian setting: A comparative, population-based study. Epidemiol. Psychiatr. Sci. 2019, 28, 397–407. [Google Scholar] [CrossRef] [Green Version]
- Zergaw, A.; Hailemariam, D.; Alem, A.; Kebede, D. A longitudinal comparative analysis of economic and family caregiver burden due to bipolar disorder. Afr. J. Psychiatry 2008, 11, 191–198. [Google Scholar] [CrossRef] [Green Version]
- Thornicroft, G.; Chatterji, S.; Evans-Lacko, S.; Gruber, M.; Sampson, N.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Alonso, J.; Andrade, L.; Borges, G.; et al. Undertreatment of people with major depressive disorder in 21 countries. Br. J. Psychiatry 2017, 210, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Virelli, C.R.; Mohiuddin, A.G.; Kennedy, J.L. Barriers to clinical adoption of pharmacogenomic testing in psychiatry: A critical analysis. Transl. Psychiatry 2021, 11, 509. [Google Scholar] [CrossRef] [PubMed]
- Akil, H.; Gordon, J.; Hen, R.; Javitch, J.; Mayberg, H.; McEwen, B.; Meaney, M.J.; Nestler, E.J. Treatment resistant depression: A multi-scale, systems biology approach. Neurosci. Biobehav. Rev. 2018, 84, 272–288. [Google Scholar] [CrossRef] [PubMed]
- Buch, A.M.; Liston, C. Dissecting diagnostic heterogeneity in depression by integrating neuroimaging and genetics. Neuropsychopharmacology 2021, 46, 156–175. [Google Scholar] [CrossRef] [PubMed]
- Cai, N.; Choi, K.W.; Fried, E.I. Reviewing the genetics of heterogeneity in depression: Operationalizations, manifestations and etiologies. Hum. Mol. Genet. 2020, 29, R10–R18. [Google Scholar] [CrossRef] [PubMed]
- Klein, D.F.; Stewart, J. Genes and environment: Nosology and psychiatry. Neurotox. Res. 2004, 6, 11–15. [Google Scholar] [CrossRef]
- Bryant, R.A.; Galatzer-Levy, I.; Hadzi-Pavlovic, D. The Heterogeneity of Posttraumatic Stress Disorder in DSM-5. JAMA Psychiatry 2022, 80, 189–191. [Google Scholar] [CrossRef]
- Osser, D. Psychopharmacology Algorithms; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2021. [Google Scholar]
- Szatmari, P.; Susser, E. Being Precise About Precision Mental Health. JAMA Psychiatry 2022, 79, 1149–1150. [Google Scholar] [CrossRef]
- Fernandes, B.S.; Williams, L.M.; Steiner, J.; Leboyer, M.; Carvalho, A.F.; Berk, M. The new field of ‘precision psychiatry’. BMC Med. 2017, 15, 80. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Stahl, S.M. Precision and personalized assessment, diagnosis and treatment in psychiatry. CNS Spectr. 2021, 26, 326–332. [Google Scholar] [CrossRef]
- Hagerty, S.L. Toward Precision Characterization and Treatment of Psychopathology: A Path Forward and Integrative Framework of the Hierarchical Taxonomy of Psychopathology and the Research Domain Criteria. Perspect. Psychol. Sci. 2022, 18, 17456916221079597. [Google Scholar] [CrossRef]
- Lin, E.; Lin, C.H.; Lane, H.Y. Precision Psychiatry Applications with Pharmacogenomics: Artificial Intelligence and Machine Learning Approaches. Int. J. Mol. Sci. 2020, 21, 969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bousman, C.A.; Bengesser, S.A.; Aitchison, K.J.; Amare, A.T.; Aschauer, H.; Baune, B.T.; Asl, B.B.; Bishop, J.R.; Burmeister, M.; Chaumette, B.; et al. Review and Consensus on Pharmacogenomic Testing in Psychiatry. Pharmacopsychiatry 2021, 54, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Fanni, D.; Pinna, F.; Gerosa, C.; Paribello, P.; Carpiniello, B.; Faa, G.; Manchia, M. Anatomical distribution and expression of CYP in humans: Neuropharmacological implications. Drug Dev. Res. 2021, 82, 628–667. [Google Scholar] [CrossRef] [PubMed]
- Stingl, J.; Viviani, R. Polymorphism in CYP2D6 and CYP2C19, members of the cytochrome P450 mixed-function oxidase system, in the metabolism of psychotropic drugs. J. Intern. Med. 2015, 277, 167–177. [Google Scholar] [CrossRef] [Green Version]
- PharmGKB. Available online: https://www.pharmgkb.org/guidelineAnnotations (accessed on 26 November 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Jürgens, G.; Andersen, S.E.; Rasmussen, H.B.; Werge, T.; Jensen, H.D.; Kaas-Hansen, B.S.; Nordentoft, M. Effect of Routine Cytochrome P450 2D6 and 2C19 Genotyping on Antipsychotic Drug Persistence in Patients with Schizophrenia: A Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e2027909. [Google Scholar] [CrossRef]
- Bradley, P.; Shiekh, M.; Mehra, V.; Vrbicky, K.; Layle, S.; Olson, M.C.; Maciel, A.; Cullors, A.; Garces, J.A.; Lukowiak, A.A. Improved efficacy with targeted pharmacogenetic-guided treatment of patients with depression and anxiety: A randomized clinical trial demonstrating clinical utility. J. Psychiatr. Res. 2018, 96, 100–107. [Google Scholar] [CrossRef]
- McCarthy, M.J.; Chen, Y.; Demodena, A.; Leckband, S.G.; Fischer, E.; Golshan, S.; Suppes, T.; Kelsoe, J.R. A prospective study to determine the clinical utility of pharmacogenetic testing of veterans with treatment-resistant depression. J. Psychopharmacol. 2021, 35, 992–1002. [Google Scholar] [CrossRef]
- Han, K.M.; Chang, H.S.; Choi, I.K.; Ham, B.J.; Lee, M.S. CYP2D6 P34S Polymorphism and Outcomes of Escitalopram Treatment in Koreans with Major Depression. Psychiatry Investig. 2013, 10, 286–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez, V.; Salavert, A.; Espadaler, J.; Tuson, M.; Saiz-Ruiz, J.; Sáez-Navarro, C.; Bobes, J.; Baca-García, E.; Vieta, E.; Olivares, J.M.; et al. Efficacy of prospective pharmacogenetic testing in the treatment of major depressive disorder: Results of a randomized, double-blind clinical trial. BMC Psychiatry 2017, 17, 250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winner, J.G.; Carhart, J.M.; Altar, C.A.; Allen, J.D.; Dechairo, B.M. A prospective, randomized, double-blind study assessing the clinical impact of integrated pharmacogenomic testing for major depressive disorder. Discov. Med. 2013, 16, 219–227. [Google Scholar] [PubMed]
- Greden, J.F.; Parikh, S.V.; Rothschild, A.J.; Thase, M.E.; Dunlop, B.W.; DeBattista, C.; Conway, C.R.; Forester, B.P.; Mondimore, F.M.; Shelton, R.C.; et al. Impact of pharmacogenomics on clinical outcomes in major depressive disorder in the GUIDED trial: A large, patient- and rater-blinded, randomized, controlled study. J. Psychiatr. Res. 2019, 111, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Oslin, D.W.; Lynch, K.G.; Shih, M.C.; Ingram, E.P.; Wray, L.O.; Chapman, S.R.; Kranzler, H.R.; Gelernter, J.; Pyne, J.M.; Stone, A.; et al. Effect of Pharmacogenomic Testing for Drug-Gene Interactions on Medication Selection and Remission of Symptoms in Major Depressive Disorder: The PRIME Care Randomized Clinical Trial. JAMA 2022, 328, 151–161. [Google Scholar] [CrossRef]
- Perlis, R.H.; Fijal, B.; Dharia, S.; Heinloth, A.N.; Houston, J.P. Failure to Replicate Genetic Associations with Antidepressant Treatment Response in Duloxetine-Treated Patients. Biol. Psychiatry 2010, 67, 1110–1113. [Google Scholar] [CrossRef]
- Singh, A.B. Improved Antidepressant Remission in Major Depression via a Pharmacokinetic Pathway Polygene Pharmacogenetic Report. Clin. Psychopharmacol. Neurosci. 2015, 13, 150–156. [Google Scholar] [CrossRef] [Green Version]
- Van der Schans, J.; Hak, E.; Postma, M.; Breuning, L.; Brouwers, J.R.B.J.; Ditters, K.; Jansen, P.A.F.; Kok, R.M.; Maring, J.G.; van Marum, R.; et al. Effects of Pharmacogenetic Screening for CYP2D6 Among Elderly Starting Therapy with Nortriptyline or Venlafaxine: A Pragmatic Randomized Controlled Trial (CYSCE Trial). J. Clin. Psychopharmacol. 2019, 39, 583–590. [Google Scholar] [CrossRef] [Green Version]
- Altar, C.A.; Carhart, J.M.; Allen, J.D.; Hall-Flavin, D.K.; Dechairo, B.M.; Winner, J.G. Clinical validity: Combinatorial pharmacogenomics predicts antidepressant responses and healthcare utilizations better than single gene phenotypes. Pharm. J. 2015, 15, 443–451. [Google Scholar] [CrossRef]
- Forester, B.P.; Parikh, S.V.; Weisenbach, S.; Ajilore, O.; Vahia, I.; Rothschild, A.J.; Thase, M.E.; Dunlop, B.W.; DeBattista, C.; Conway, C.R.; et al. Combinatorial Pharmacogenomic Testing Improves Outcomes for Older Adults with Depression. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2020, 28, 933–945. [Google Scholar] [CrossRef]
- Tiwari, A.K.; Zai, C.C.; Altar, C.A.; Tanner, J.A.; Davies, P.E.; Traxler, P.; Li, J.; Cogan, E.S.; Kucera, M.T.; Gugila, A.; et al. Clinical utility of combinatorial pharmacogenomic testing in depression: A Canadian patient- and rater-blinded, randomized, controlled trial. Transl. Psychiatry 2022, 12, 101. [Google Scholar] [CrossRef] [PubMed]
- Callegari, C.; Isella, C.; Caselli, I.; Poloni, N.; Ielmini, M. Pharmacogenetic Tests in Reducing Accesses to Emergency Services and Days of Hospitalization in Bipolar Disorder: A 2-Year Mirror Analysis. J. Pers. Med. 2019, 9, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almoguera, B.; Riveiro-Alvarez, R.; Lopez-Castroman, J.; Dorado, P.; Vaquero-Lorenzo, C.; Fernandez-Piqueras, J.; Llerena, A.; Abad-Santos, F.; Baca-García, E.; Dal-Ré, R.; et al. CYP2D6 poor metabolizer status might be associated with better response to risperidone treatment. Pharm. Genom. 2013, 23, 627–630. [Google Scholar] [CrossRef] [PubMed]
- Gregoor, J.G.; van der Weide, K.; van der Weide, J.; van Megen, H.J.G.M.; Egberts, A.C.G.; Heerdink, E.R. The association between CYP2D6 genotype and switching antipsychotic medication to clozapine. Eur. J. Clin. Pharmacol. 2013, 69, 1927–1932. [Google Scholar] [CrossRef]
- Jovanovic, N.; Bozina, N.; Lovric, M.; Medved, V.; Jakovljevic, M.; Peles, A.M. The role of CYP2D6 and ABCB1 pharmacogenetics in drug-naive patients with first-episode schizophrenia treated with risperidone. Eur. J. Clin. Pharmacol. 2010, 66, 1109–1117. [Google Scholar] [CrossRef] [Green Version]
- Kaur, G.; Gupta, D.; Chavan, B.S.; Sinhmar, V.; Prasad, R.; Tripathi, A.; Garg, P.D.; Gupta, R.; Khurana, H.; Gautam, S.; et al. Identification of genetic correlates of response to Risperidone: Findings of a multicentric schizophrenia study from India. Asian J. Psychiatr. 2017, 29, 174–182. [Google Scholar] [CrossRef]
- Lu, J.; Yang, Y.; Lu, J.; Wang, Z.; He, Y.; Yan, Y.; Fu, K.; Jiang, W.; Xu, Y.; Wu, R.; et al. Effect of CYP2D6 polymorphisms on plasma concentration and therapeutic effect of risperidone. BMC Psychiatry 2021, 21, 70. [Google Scholar] [CrossRef]
- Muller, D.J.; Brandl, E.J.; Hwang, R.; Tiwari, A.K.; Sturgess, J.E.; Zai, C.C.; Lieberman, J.A.; Kennedy, J.L.; Richter, M.A. The AmpliChip(R) CYP450 test and response to treatment in schizophrenia and obsessive compulsive disorder: A pilot study and focus on cases with abnormal CYP2D6 drug metabolism. Genet. Test. Mol. Biomark. 2012, 16, 897–903. [Google Scholar] [CrossRef]
- Nozawa, M.; Ohnuma, T.; Matsubara, Y.; Sakai, Y.; Hatano, T.; Hanzawa, R.; Shibata, N.; Arai, H. The relationship between the response of clinical symptoms and plasma olanzapine concentration, based on pharmacogenetics: Juntendo University Schizophrenia Projects (JUSP). Ther. Drug Monit. 2008, 30, 35–40. [Google Scholar] [CrossRef]
- Xu, Q.; Wu, X.; Li, M.; Huang, H.; Minica, C.; Yi, Z.; Wang, G.; Shen, L.; Xing, Q.; Shi, Y.; et al. Association studies of genomic variants with treatment response to risperidone, clozapine, quetiapine and chlorpromazine in the Chinese Han population. Pharm. J. 2016, 16, 357–365. [Google Scholar] [CrossRef]
- Vijayan, N.N.; Mathew, A.; Balan, S.; Natarajan, C.; Nair, C.M.; Allencherry, P.M.; Banerjee, M. Antipsychotic drug dosage and therapeutic response in schizophrenia is influenced by ABCB1 genotypes: A study from a south Indian perspective. Pharmacogenomics 2012, 13, 1119–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, Q.; Gao, R.; Li, H.; Feng, G.; Xu, M.; Duan, S.; Meng, J.; Zhang, A.; Qin, S.; He, L. Polymorphisms of the ABCB1 gene are associated with the therapeutic response to risperidone in Chinese schizophrenia patients. Pharmacogenomics 2006, 7, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Grossman, I.; Sullivan, P.F.; Walley, N.; Liu, Y.; Dawson, J.R.; Gumbs, C.; Gaedigk, A.; Leeder, J.S.; McEvoy, J.P.; Weale, M.E.; et al. Genetic determinants of variable metabolism have little impact on the clinical use of leading antipsychotics in the CATIE study. Genet. Med. Off. J. Am. Coll. Med. Genet. 2008, 10, 720–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lesche, D.; Mostafa, S.; Everall, I.; Pantelis, C.; Bousman, C.A. Impact of CYP1A2, CYP2C19, and CYP2D6 genotype- and phenoconversion-predicted enzyme activity on clozapine exposure and symptom severity. Pharmacogenomics J. 2020, 20, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Nikisch, G.; Baumann, P.; Oneda, B.; Kiessling, B.; Weisser, H.; Mathé, A.A.; Yoshitake, T.; Kehr, J.; Wiedemann, G.; Eap, C.B. Cytochrome P450 and ABCB1 Genetics: Association with Quetiapine and Norquetiapine Plasma and Cerebrospinal Fluid Concentrations and with Clinical Response in Patients Suffering from Schizophrenia. A Pilot Study. J. Psychopharmacol. 2011, 25, 896–907. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Ellingrod, V.L.; Bishop, J.R.; Miller, D.D. The relationship between P-glycoprotein (PGP) polymorphisms and response to olanzapine treatment in schizophrenia. Ther. Drug Monit. 2006, 28, 668–672. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, A.P.; Poonkuzhali, B.; Kuruvilla, A.; Srivastava, A.; Jacob, M.; Jacob, K.S. Association between CYP1A2 gene single nucleotide polymorphisms and clinical responses to clozapine in patients with treatment-resistant schizophrenia. Acta Neuropsychiatr. 2013, 25, 2–11. [Google Scholar] [CrossRef]
- Yasui-Furukori, N.; Saito, M.; Nakagami, T.; Kaneda, A.; Tateishi, T.; Kaneko, S. Association between Multidrug Resistance 1 (MDR1) Gene Polymorphisms and Therapeutic Response to Bromperidol in Schizophrenic Patients: A Preliminary Study. Prog. Neuropsychopharmacol. Biol. Psychiatry 2006, 30, 286–291. [Google Scholar] [CrossRef]
- Breitenstein, B.; Scheuer, S.; Pfister, H.; Uhr, M.; Lucae, S.; Holsboer, F.; Ising, M.; Brückl, T.M. The clinical application of ABCB1 genotyping in antidepressant treatment: A pilot study. CNS Spectrums 2014, 19, 165–175. [Google Scholar] [CrossRef]
- Calabrò, M.; Fabbri, C.; Kasper, S.; Zohar, J.; Souery, D.; Montgomery, S.; Albani, D.; Forloni, G.; Ferentinos, P.; Rujescu, D.; et al. Metabolizing status of CYP2C19 in response and side effects to medications for depression: Results from a naturalistic study. Eur. Neuropsychopharmacol. 2022, 56, 100–111. [Google Scholar] [CrossRef]
- Dong, C.; Wong, M.L.; Licinio, J. Sequence variations of ABCB1, SLC6A2, SLC6A3, SLC6A4, CREB1, CRHR1 and NTRK2: Association with major depression and antidepressant response in Mexican-Americans. Mol. Psychiatry 2009, 14, 1105–1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gressier, F.; Verstuyft, C.; Hardy, P.; Becquemont, L.; Corruble, E. Response to CYP2D6 substrate antidepressants is predicted by a CYP2D6 composite phenotype based on genotype and comedications with CYP2D6 inhibitors. J. Neural Transm. 2015, 122, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.O.; Chang, H.S.; Lee, H.Y.; Ham, B.J.; Kang, R.H.; Jeong, Y.J.; Lee, M.S. CYP2D6 P34S Polymorphism and Mirtazapine Responses in Koreans with Major Depression. Mol. Cell. Toxicol. 2009, 5, 346–353. [Google Scholar]
- Kato, M.; Fukuda, T.; Serretti, A.; Wakeno, M.; Okugawa, G.; Ikenaga, Y.; Hosoi, Y.; Takekita, Y.; Mandelli, L.; Azuma, J.; et al. ABCB1 (MDR1) Gene Polymorphisms are Associated with the Clinical Response to Paroxetine in Patients with Major Depressive Disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 398–404. [Google Scholar] [CrossRef]
- Lin, K.M.; Tsou, H.H.; Tsai, I.J.; Hsiao, M.C.; Hsiao, C.F.; Liu, C.Y.; Shen, W.W.; Tang, H.S.; Fang, C.K.; Wu, C.S.; et al. CYP1A2 Genetic Polymorphisms are Associated with Treatment Response to the Antidepressant Paroxetine. Pharmacogenomics 2010, 11, 1535–1543. [Google Scholar] [CrossRef]
- Perlis, R.H.; Dowd, D.; Fava, M.; Lencz, T.; Krause, D.S. Randomized, controlled, participant- and rater-blind trial of pharmacogenomic test-guided treatment versus treatment as usual for major depressive disorder. Depress. Anxiety 2020, 37, 834–841. [Google Scholar] [CrossRef]
- Ruano, G.; Szarek, B.L.; Villagra, D.; Gorowski, K.; Kocherla, M.; Seip, R.L.; Goethe, J.W.; Schwartz, H.I. Length of psychiatric hospitalization is correlated with CYP2D6 functional status in inpatients with major depressive disorder. Biomark. Med. 2013, 7, 429–439. [Google Scholar] [CrossRef] [Green Version]
- Tsai, M.H.; Lin, K.M.; Hsiao, M.C.; Shen, W.W.; Lu, M.L.; Tang, H.S.; Fang, C.K.; Wu, C.S.; Lu, S.C.; Liu, S.C.; et al. Genetic Polymorphisms of Cytochrome P450 Enzymes Influence Metabolism of the Antidepressant Escitalopram and Treatment Response. Pharmacogenomics 2010, 11, 537–546. [Google Scholar] [CrossRef]
- Huilei, X.; Siyu, C.; Jianghua, X.; Jidong, R.; Yi, R. Clinical utility of pharmacogenetic testing in the treatment of bipolar disorder of Chinese patients. Pharmacogenomics 2020, 21, 761–770. [Google Scholar] [CrossRef]
- Thakran, S.; Guin, D.; Singh, P.; Singh, P.; Kukal, S.; Rawat, C.; Yadav, S.; Kushwaha, S.S.; Srivastava, A.K.; Hasija, Y.; et al. Genetic Landscape of Common Epilepsies: Advancing towards Precision in Treatment. Int. J. Mol. Sci. 2020, 21, 7784. [Google Scholar] [CrossRef]
- DeLuca, J.; Oliver, T.; Hulsopple, C.; Selig, D.; Por, E.; Turner, C.; Hellwig, L.; Livezey, J. Applying Pharmacogenomic Guidelines to Combat Medical Care. Mil. Med. 2021, 187, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Hayward, J.; McDermott, J.; Qureshi, N.; Newman, W. Pharmacogenomic testing to support prescribing in primary care: A structured review of implementation models. Pharmacogenomics 2021, 22, 761–776. [Google Scholar] [CrossRef] [PubMed]
- Duarte, J.D.; Cavallari, L.H. Pharmacogenetics to guide cardiovascular drug therapy. Nat. Rev. Cardiol. 2021, 18, 649–665. [Google Scholar] [CrossRef] [PubMed]
- Diasio, R.B.; Innocenti, F.; Offer, S.M. Pharmacogenomic-Guided Therapy in Colorectal Cancer. Clin. Pharmacol. Ther. 2021, 110, 616–625. [Google Scholar] [CrossRef]
- Barker, C.I.S.; Groeneweg, G.; Maitland-van der Zee, A.H.; Rieder, M.J.; Hawcutt, D.B.; Hubbard, T.J.; Swen, J.J.; Carleton, B.C. Pharmacogenomic testing in paediatrics: Clinical implementation strategies. Br. J. Clin. Pharmacol. 2022, 88, 4297–4310. [Google Scholar] [CrossRef]
- Lipschultz, E.; Danahey, K.; Truong, T.M.; Schierer, E.; Volchenboum, S.L.; Ratain, M.J.; O’Donnell, P.H. Creation of a pharmacogenomics patient portal complementary to an existing institutional provider-facing clinical decision support system. JAMIA Open 2021, 4, ooab067. [Google Scholar] [CrossRef]
- Brown, L.C.; Stanton, J.D.; Bharthi, K.; Maruf, A.A.; Muller, D.J.; Bousman, C.A. Pharmacogenomic Testing and Depressive Symptom Remission: A Systematic Review and Meta-Analysis of Prospective, Controlled Clinical Trials. Clin. Pharmacol. Ther. 2022, 112, 1303–1317. [Google Scholar] [CrossRef]
- Bousman, C.A.; Arandjelovic, K.; Mancuso, S.G.; Eyre, H.A.; Dunlop, B.W. Pharmacogenetic tests and depressive symptom remission: A meta-analysis of randomized controlled trials. Pharmacogenomics 2019, 20, 37–47. [Google Scholar] [CrossRef] [Green Version]
- Iosifescu, D.V. Pharmacogenomic Testing for Next-Step Antidepressant Selection: Still a Work in Progress. JAMA 2022, 328, 146–148. [Google Scholar] [CrossRef]
- Meyer, J.M.; Stahl, M.S. The Clinical Use of Antipsychotic Plasma Levels; Cambridge University Press: Cambridge, UK, 2021; pp. 114–146. [Google Scholar]
- Rosenblat, J.D.; Lee, Y.; McIntyre, R.S. The effect of pharmacogenomic testing on response and remission rates in the acute treatment of major depressive disorder: A meta-analysis. J. Affect. Disord. 2018, 241, 484–491. [Google Scholar] [CrossRef]
- Carta, A.; Del Zompo, M.; Meloni, A.; Mola, F.; Paribello, P.; Pinna, F.; Pinna, M.; Pisanu, C.; Manchia, M.; Squassina, A.; et al. Cost-Utility Analysis of Pharmacogenetic Testing Based on CYP2C19 or CYP2D6 in Major Depressive Disorder: Assessing the Drivers of Different Cost-Effectiveness Levels from an Italian Societal Perspective. Clin. Drug. Investig. 2022, 42, 733–746. [Google Scholar] [CrossRef] [PubMed]
- Tanner, J.A.; Davies, P.E.; Overall, C.C.; Grima, D.; Nam, J.; Dechairo, B.M. Cost-effectiveness of combinatorial pharmacogenomic testing for depression from the Canadian public payer perspective. Pharmacogenomics 2020, 21, 521–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodman, C.W.; Brett, A.S. Race and Pharmacogenomics-Personalized Medicine or Misguided Practice? JAMA 2021, 325, 625–626. [Google Scholar] [CrossRef] [PubMed]
- Blazy, C.; Ellingrod, V.; Ward, K. Variability Between Clinical Pharmacogenetics Implementation Consortium (CPIC((R))) Guidelines and a Commercial Pharmacogenetics Laboratory in Genotype to Phenotype Interpretations for Patients Utilizing Psychotropics. Front. Pharmacol. 2022, 13, 939313. [Google Scholar] [CrossRef]
- Tafazoli, A.; Guchelaar, H.J.; Miltyk, W.; Kretowski, A.J.; Swen, J.J. Applying Next-Generation Sequencing Platforms for Pharmacogenomic Testing in Clinical Practice. Front. Pharmacol. 2021, 12, 693453. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paribello, P.; Manchia, M.; Pinna, F.; Isayeva, U.; Squassina, A.; Pisanu, C.; Balderi, L.; Contu, M.; Pinna, M.; Carpiniello, B. Pharmacokinetic Markers of Clinical Outcomes in Severe Mental Illness: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 4776. https://doi.org/10.3390/ijms24054776
Paribello P, Manchia M, Pinna F, Isayeva U, Squassina A, Pisanu C, Balderi L, Contu M, Pinna M, Carpiniello B. Pharmacokinetic Markers of Clinical Outcomes in Severe Mental Illness: A Systematic Review. International Journal of Molecular Sciences. 2023; 24(5):4776. https://doi.org/10.3390/ijms24054776
Chicago/Turabian StyleParibello, Pasquale, Mirko Manchia, Federica Pinna, Ulker Isayeva, Alessio Squassina, Claudia Pisanu, Lorenzo Balderi, Martina Contu, Marco Pinna, and Bernardo Carpiniello. 2023. "Pharmacokinetic Markers of Clinical Outcomes in Severe Mental Illness: A Systematic Review" International Journal of Molecular Sciences 24, no. 5: 4776. https://doi.org/10.3390/ijms24054776