
Protective Effect of Oxygen and Isoflurane in Rodent Model of Intestinal Ischemia-Reperfusion Injury
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Oxygen Supplementation
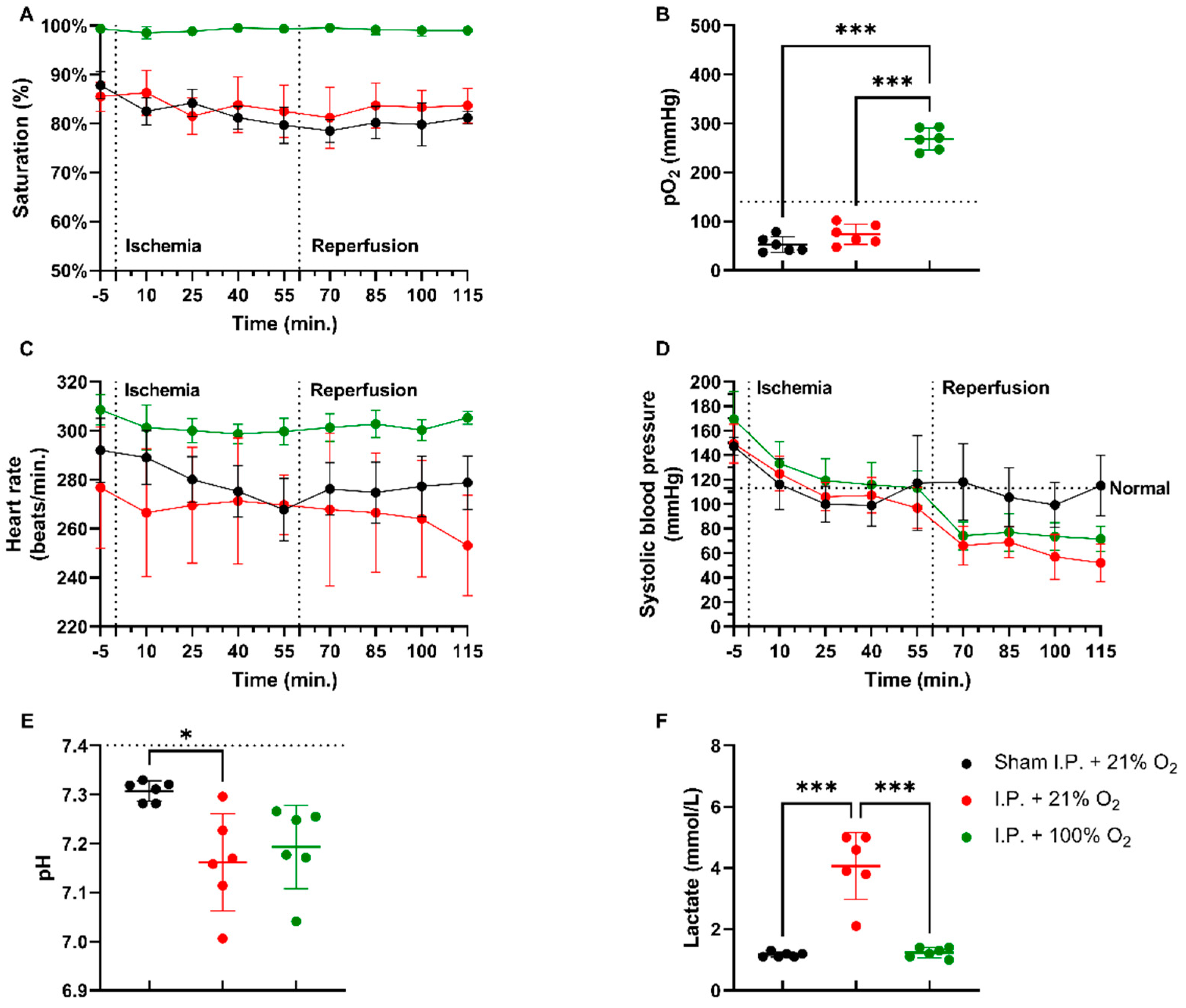
2.1.1. Oxygen Supplementation Improved Cardiovascular Stability and Prevented Acidosis in Intestinal IRI
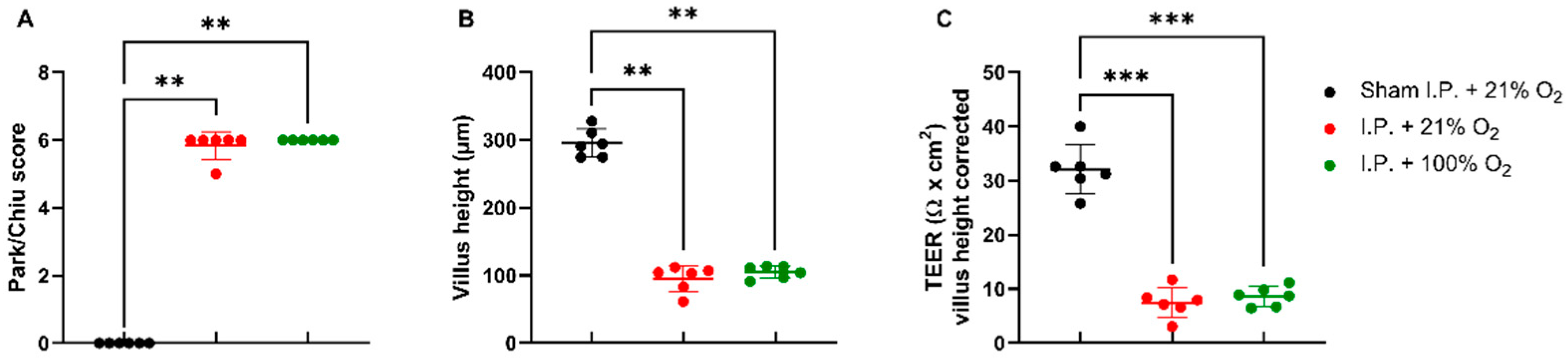
2.1.2. Oxygen Supplementation Did Not Protect against Intestinal Damage
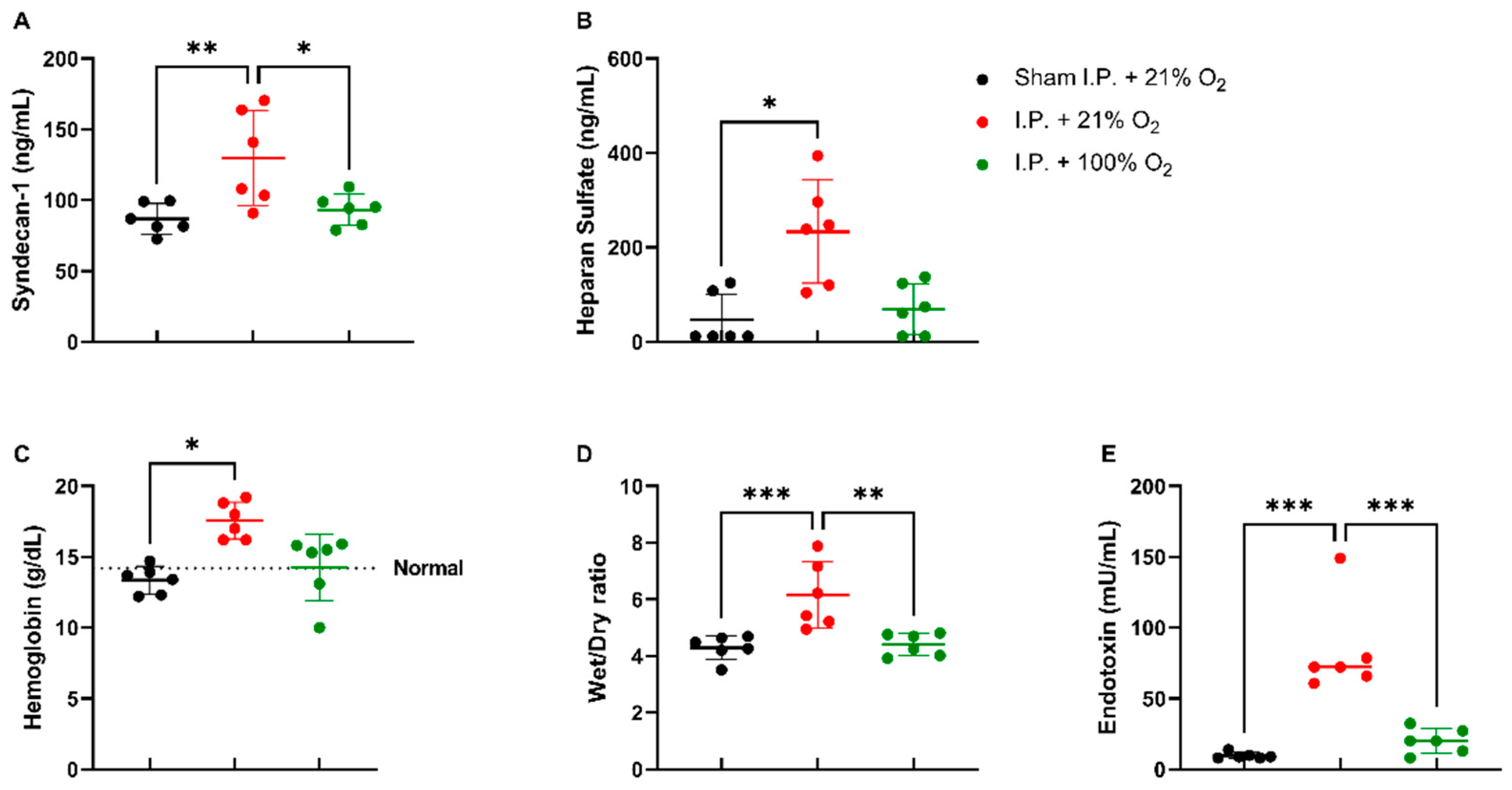
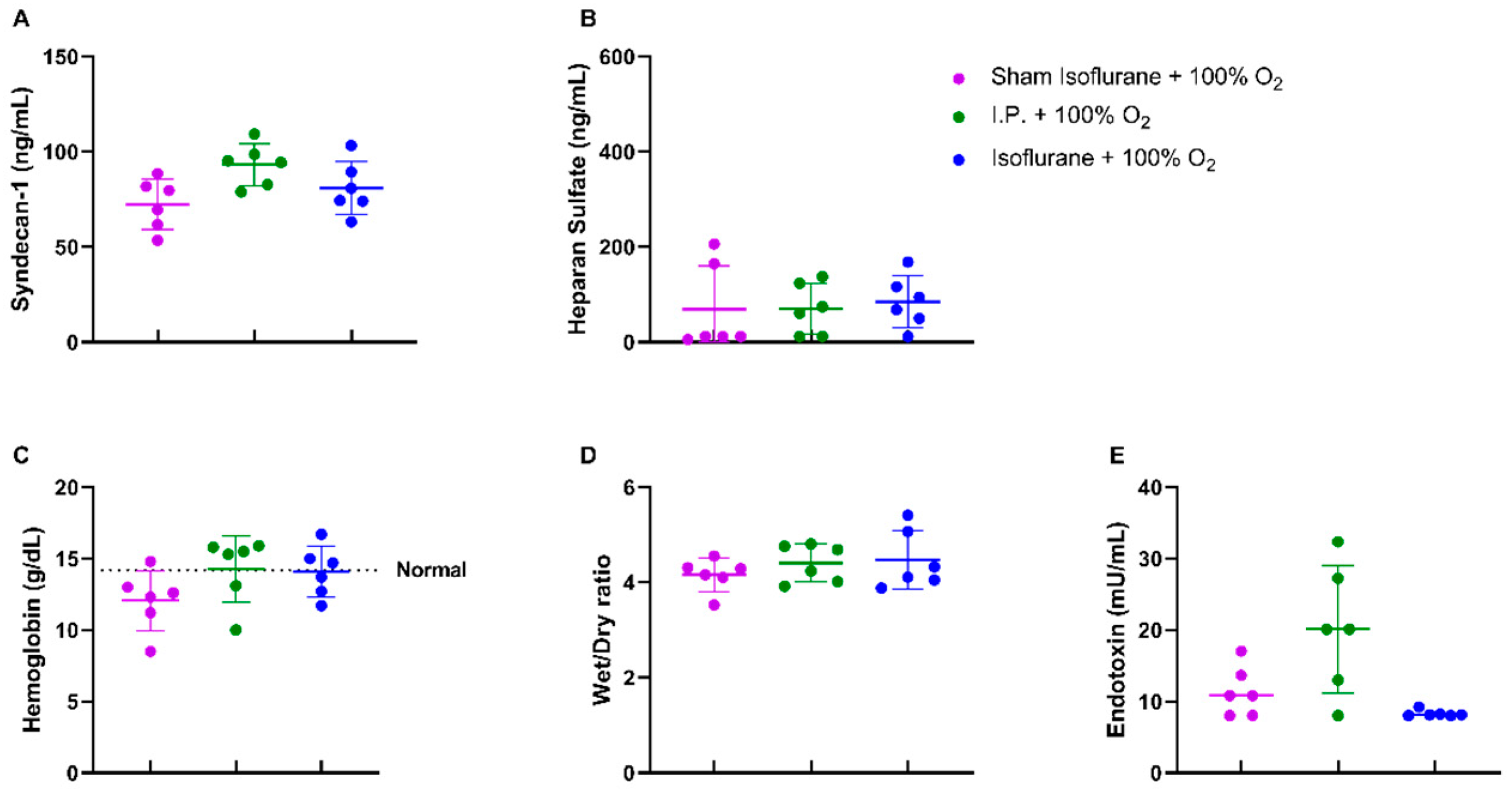
2.1.3. Oxygen Supplementation Preserved Vascular Permeability and Prevented Endotoxin Translocation Following IRI
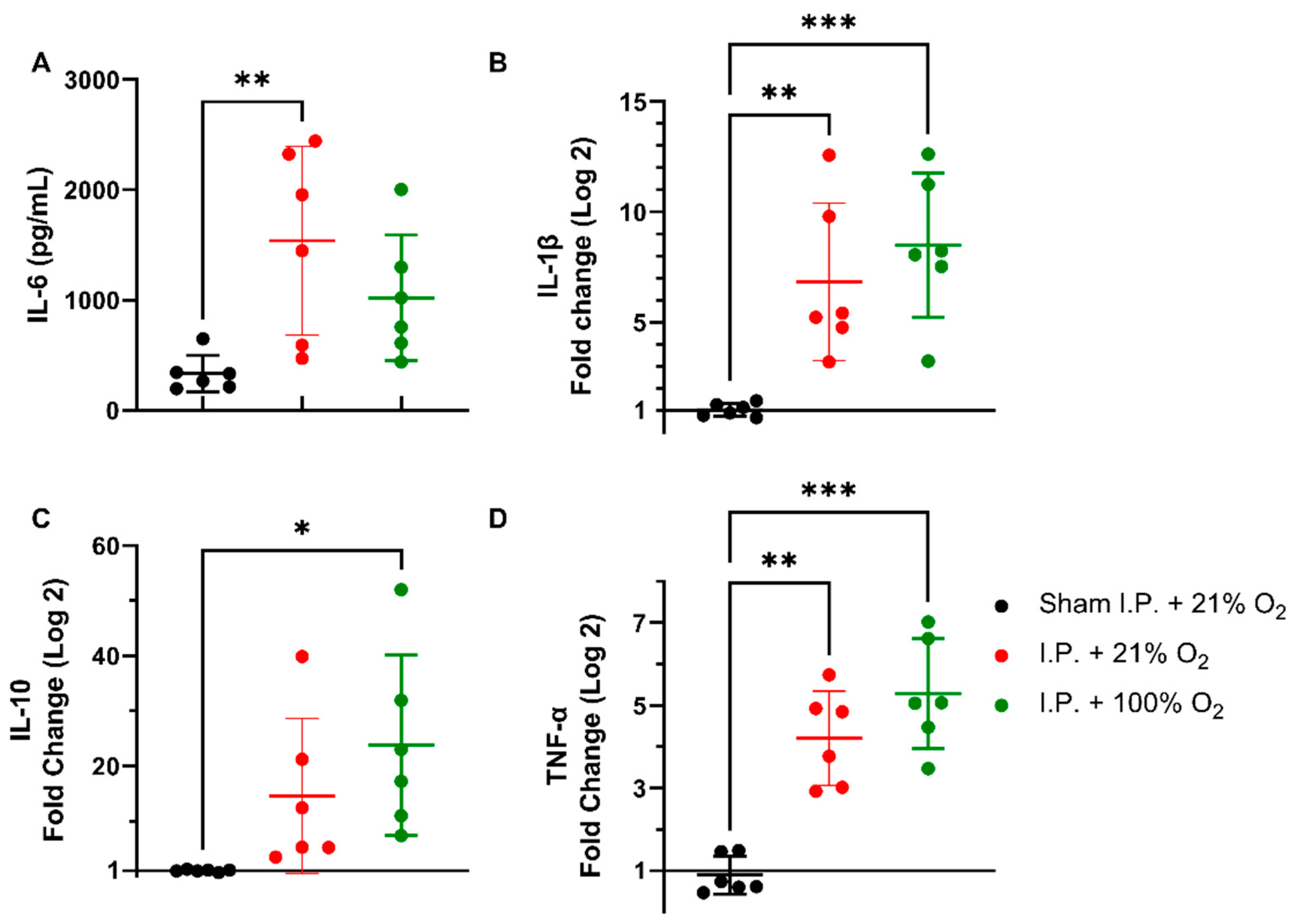
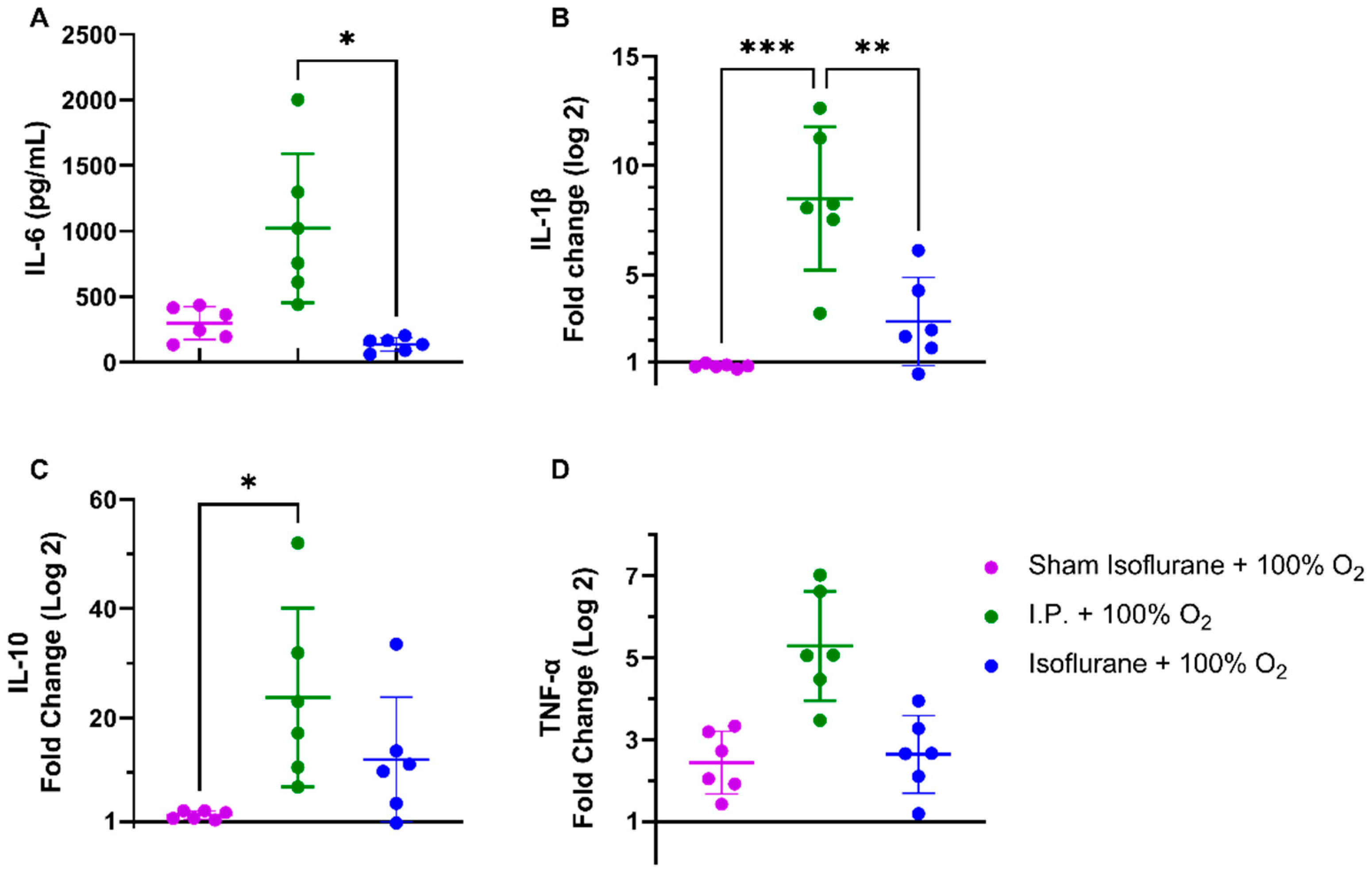
2.1.4. Oxygen Supplementation Did Not Prevent the Inflammatory Response Provoked by IRI
2.2. Isoflurane Anesthesia
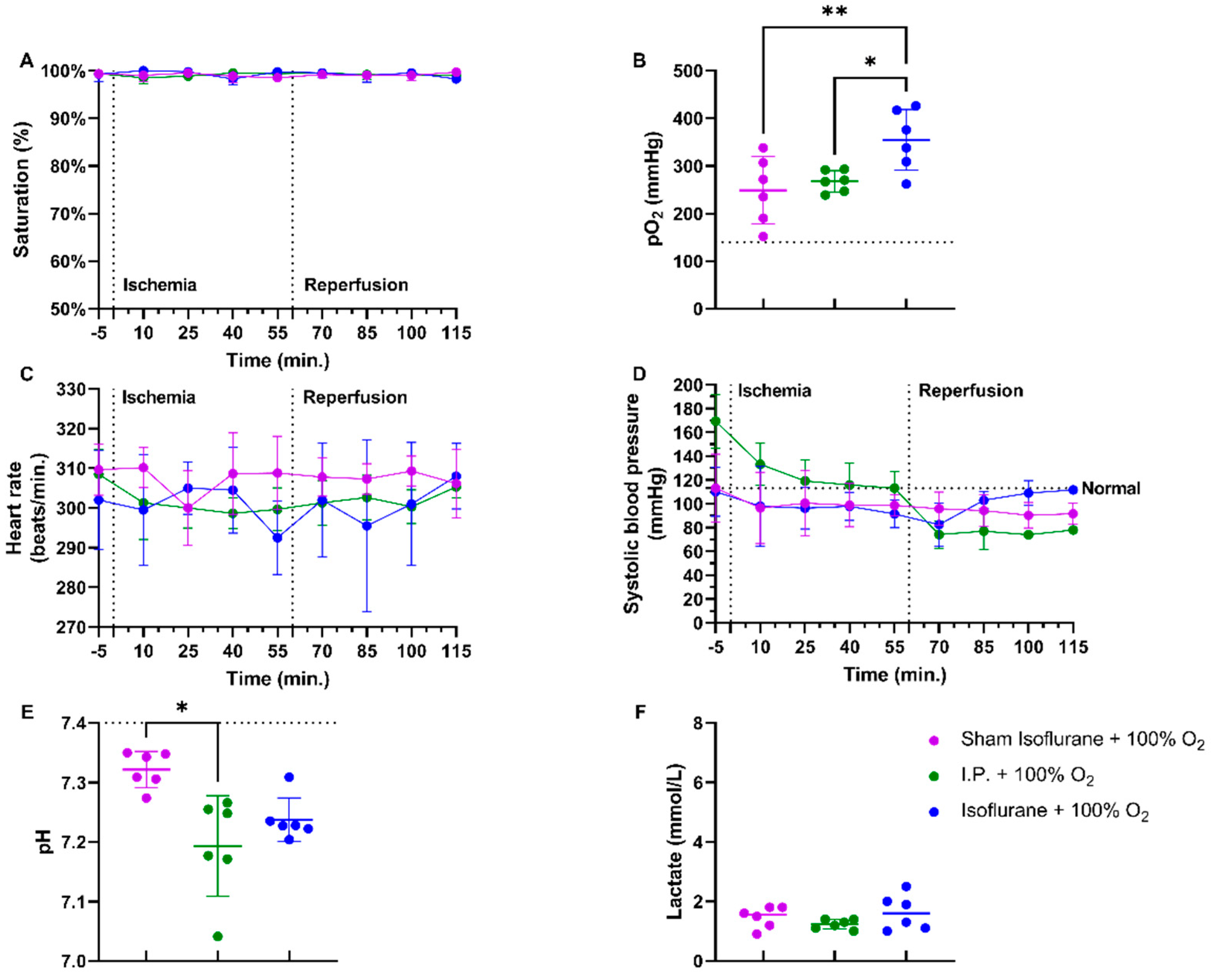
2.2.1. Isoflurane Anesthesia Prevented Reperfusion Hypotension in Intestinal IRI and Acidosis
2.2.2. Isoflurane Protected against Histopathological Damage and Preserved Intestinal Permeability, Provoked by IRI
2.2.3. Isoflurane Did Not Additionally Protect Vascular Permeability or Reduce Endotoxin Translocation in the Case of Oxygen Supplementation
2.2.4. Isoflurane Impeded the Inflammatory Response Following IRI
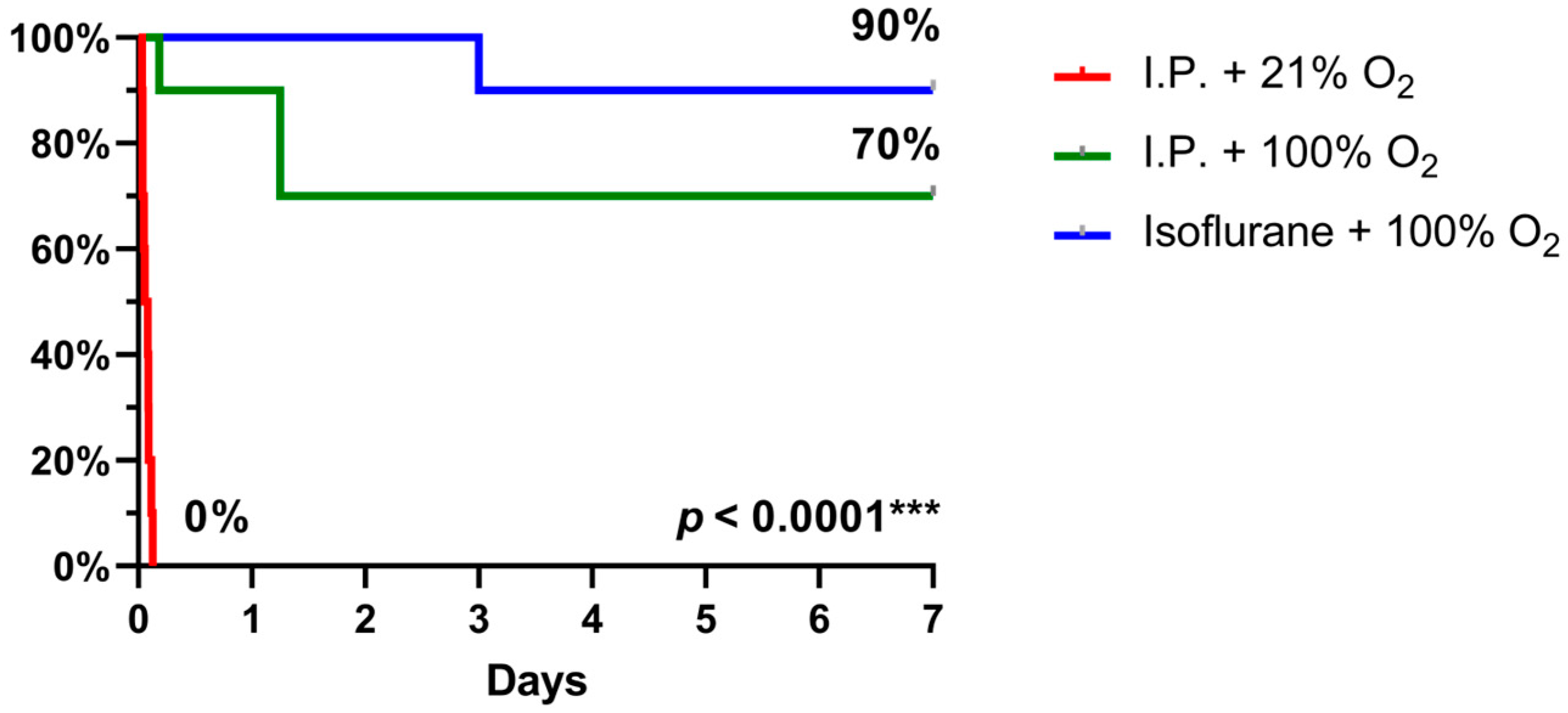
2.3. Oxygen Supplementation and Isoflurane Improved Survival Following IRI
3. Discussion
4. Materials and Methods
4.1. Animal Model
4.2. Anesthesia
4.3. Surgery
4.4. Vital Signs
4.5. Blood and Tissue Sampling
4.6. Arterial Blood Gas Analysis
4.7. Histological Evaluation
4.8. Ussing Chamber Experiments
Electrophysiological Parameters
4.9. Endotoxin Levels
4.10. Edema
4.11. ELISA
4.12. Quantitative Reverse-Transcription Polymerase Chain Reaction (qRT-PCR)
4.13. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carden, D.L.; Granger, D.N. Pathophysiology of ischaemia-reperfusion injury. J. Pathol. 2000, 190, 255–266. [Google Scholar] [CrossRef]
- Bala, M.; Catena, F.; Kashuk, J.; De Simone, B.; Gomes, C.A.; Weber, D.; Sartelli, M.; Coccolini, F.; Kluger, Y.; Abu-Zidan, F.M.; et al. Acute mesenteric ischemia: Updated guidelines of the world society of emergency surgery. World J. Emerg. Surg. 2022, 17, 54. [Google Scholar] [CrossRef] [PubMed]
- Vollmar, B.; Menger, M.D. Intestinal ischemia/reperfusion: Microcirculatory pathology and functional consequences. Langenbeck’s Arch. Surg. 2011, 396, 13–29. [Google Scholar] [CrossRef]
- Eltzschig, H.K.; Eckle, T. Ischemia and reperfusion—From mechanism to translation. Nat. Med. 2011, 17, 1391–1401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallick, I.H.; Yang, W.; Winslet, M.C.; Seifalian, A.M. Ischemia—Reperfusion injury of the intestine and protective strategies against injury. Dig. Dis. Sci. 2004, 49, 1359–1377. [Google Scholar] [CrossRef]
- Cai, J.; Chen, X.; Liu, X.; Li, Z.; Shi, A.; Tang, X.; Xia, P.; Zhang, J.; Yu, P. AMPK: The key to ischemia-reperfusion injury. J. Cell Physiol. 2022, 237, 4079–4096. [Google Scholar] [CrossRef]
- Liao, S.; Luo, J.; Kadier, T.; Ding, K.; Chen, R.; Meng, Q. Mitochondrial DNA release contributes to intestinal ischemia/reperfusion injury. Front. Pharmacol. 2022, 13, 854994. [Google Scholar] [CrossRef] [PubMed]
- Fan, S.; Xu, Y.; Li, K.; Li, B.; Diao, Y. Ellagic acid alleviates mice intestinal ischemia-reperfusion injury: A study based on transcriptomics combined with functional experiments. Chem. Biodivers. 2022, 19, e202200345. [Google Scholar] [CrossRef]
- Bosi, A.; Banfi, D.; Bistoletti, M.; Catizzone, L.M.; Chiaravalli, A.M.; Moretto, P.; Moro, E.; Karousou, E.; Viola, M.; Giron, M.C.; et al. Hyaluronan regulates neuronal and immune function in the rat small intestine and colonic microbiota after ischemic/reperfusion injury. Cells 2022, 11, 3370. [Google Scholar] [CrossRef] [PubMed]
- Lenaerts, K.; Ceulemans, L.J.; Hundscheid, I.H.R.; Grootjans, J.; Dejong, C.H.C.; Olde Damink, S.W.M. New insights in intestinal ischemia–reperfusion injury. Curr. Opin. Organ Transpl. 2013, 18, 298–303. [Google Scholar] [CrossRef]
- Shi, Y.; Zhang, X.; Wan, Z.; Liu, X.; Chen, F.; Zhang, J.; Leng, Y. Mesenchymal stem cells against intestinal ischemia–reperfusion injury: A systematic review and meta-analysis of preclinical studies. Stem Cell Res. Ther. 2022, 13, 216. [Google Scholar] [CrossRef]
- Chen, Z.; Wang, Z.; Liu, D.; Zhao, X.; Ning, S.; Liu, X.; Wang, G.; Zhang, F.; Luo, F.; Yao, J.; et al. Critical role of caveolin-1 in intestinal ischemia reperfusion by inhibiting protein kinase C βII. Free Radic. Biol. Med. 2023, 194, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Ceulemans, L.; Verbeke, L.; Decuypere, J.P.; Farré, R.; De Hertogh, G.; Lenaerts, K.; Jochmans, I.; Monbaliu, D.; Nevens, F.; Tack, J.; et al. Farnesoid X receptor activation attenuates intestinal ischemia reperfusion injury in rats. PLoS ONE 2017, 12, e0169331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, S.L.; Duke-Novakovski, T.; Singh, B. The immune response to anesthesia: Part 1. Vet. Anaesth. Analg. 2014, 41, 113–126. [Google Scholar] [CrossRef] [PubMed]
- Anderson, S.L.; Duke-Novakovski, T.; Singh, B. The immune response to anesthesia: Part 2 sedatives, opioids, and injectable anesthetic agents. Vet. Anaesth. Analg. 2014, 41, 553–566. [Google Scholar] [CrossRef] [PubMed]
- Wilding, L.A.; Hampel, J.A.; Khoury, B.M.; Kang, S.; Machado-Aranda, D.; Raghavendran, K.; Nemzek, J.A. Benefits of 21% oxygen compared with 100% oxygen for delivery of isoflurane to mice (Mus musculus) and rats (Rattus norvegicus). J. Am. Assoc. Lab. Anim. Sci. 2017, 56, 148–154. [Google Scholar]
- Cámara, C.R.; Guzmán, F.J.; Barrera, E.A.; Cabello, A.J.; Garcia, A.; Fernández, N.E.; Caballero, E.; Ancer, J. Ketamine anesthesia reduces intestinal ischemia/reperfusion injury in rats. World J. Gastroenterol. 2008, 14, 5192. [Google Scholar] [CrossRef]
- Guzmán-De La Garza, F.J.; Cámara-Lemarroy, C.R.; Ballesteros-Elizondo, R.G.; Alarcón-Galván, G.; Cordero-Pérez, P.; Fernández-Garza, N.E. Ketamine reduces intestinal injury and inflammatory cell infiltration after ischemia/reperfusion in rats. Surg. Today 2010, 40, 1055–1062. [Google Scholar] [CrossRef]
- Eroglu, A. The effect of intravenous anesthetics on ischemia-reperfusion injury. BioMed Res. Int. 2014, 2014, 821513. [Google Scholar] [CrossRef]
- Sukhotnik, I.; Coran, A.G.; Greenblatt, R.; Brod, V.; Mogilner, J.; Shiloni, E.; Shaoul, R.; Bitterman, H. Effect of 100% oxygen on E-selectin expression, recruitment of neutrophils and enterocyte apoptosis following intestinal ischemia-reperfusion in a rat. Pediatr. Surg. Int. 2008, 24, 29–35. [Google Scholar] [CrossRef]
- Sukhotnik, I.; Brod, V.; Lurie, M.; Rahat, M.A.; Shnizer, S.; Lahat, N.; Mogilner, J.G.; Bitterman, H. The effect of 100% oxygen on intestinal preservation and recovery following ischemia-reperfusion injury in rats. Crit. Care Med. 2009, 37, 1054–1061. [Google Scholar] [CrossRef] [PubMed]
- Beck-Schimmer, B.; Bonvini, J.M.; Schadde, E.; Dutkowski, P.; Oberkofler, C.E.; Lesurtel, M.; DeOliveira, M.L.; Figueira, E.R.; Rocha Filho, J.A.; Auler, J.O.C., Jr.; et al. Conditioning with sevoflurane in liver transplantation. Transplantation 2015, 99, 1606–1612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieuwenhuijs-Moeke, G.J.; Nieuwenhuijs, V.B.; Seelen, M.A.J.; Berger, S.P.; van den Heuvel, M.C.; Burgerhof, J.G.M.; Ottens, P.J.; Ploeg, R.J.; Leuvenink, H.G.; Struys, M.M. Propofol-based anaesthesia versus sevoflurane-based anaesthesia for living donor kidney transplantation: Results of the VAPOR-1 randomized controlled trial. Br. J. Anaesth. 2017, 118, 720–732. [Google Scholar] [CrossRef] [Green Version]
- Abassi, Z.; Armaly, Z.; Heyman, S.N. Glycocalyx degradation in ischemia-reperfusion injury. Am. J. Pathol. 2020, 190, 752–767. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Wang, S.; Fan, Z. Oxidative stress in intestinal ischemia-reperfusion. Front. Med. 2022, 8, 750731. [Google Scholar] [CrossRef]
- Kim, M.; Park, S.W.; Kim, M.; D’Agati, V.D.; Lee, H.T. Isoflurane post-conditioning protects against intestinal ischemia-reperfusion injury and multiorgan dysfunction via transforming growth factor-β1 generation. Ann. Surg. 2012, 255, 492–503. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.T.; Kim, M.; Kim, M.; Kim, N.; Billings, F.T.; D’Agati, V.D.; Emala, C.W. Isoflurane protects against renal ischemia and reperfusion injury and modulates leukocyte infiltration in mice. Am. J. Physiol. 2007, 293, F713–F722. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Ding, R.; Huang, W.; Miao, L.; Li, J.; Li, Y. Sevoflurane protects against intestinal ischemia-reperfusion injury by activating peroxisome proliferator-activated receptor gamma/nuclear factor-κB pathway in rats. Pharmacology 2019, 105, 231–242. [Google Scholar] [CrossRef]
- Cho, S.S.C.; Rudloff, I.; Berger, P.J.; Irwin, M.G.; Nold, M.F.; Cheng, W.; Nold-Petry, C.A. Remifentanil ameliorates intestinal ischemia-reperfusion injury. BMC Gastroenterol. 2013, 13, 69. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Wang, G.; Zhai, X.; Hu, Y.; Gao, D.; Ma, L.; Yao, J.; Tian, X. Selective inhibition of protein kinase C β2 attenuates the adaptor P66Shc-mediated intestinal ischemia–reperfusion injury. Cell Death Dis. 2014, 5, e1164. [Google Scholar] [CrossRef] [Green Version]
- Bilbao, J.; Garcia-Alonso, I.; Portugal, V.; Barcelo, P.; Apecechea, A.; Mendez, J. Efficacy of antioxidant therapy (folic acid and alphatocopherol) in intestinal lesions produced by reperfusion. Cir. Esp. 1992, 51, 262–265. [Google Scholar]
- Simon, A.R.; Rai, U.; Fanburg, B.L.; Cochran, B.H. Activation of the JAK-STAT pathway by reactive oxygen species. Am. J. Physiol. Cell Physiol. 1998, 275, 1640–1652. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Jiang, X.; Tai, W.; Shi, E. Emulsified isoflurane induces postconditioning against myocardial infarction via JAK-STAT pathway. J. Surg. Res. 2012, 178, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Kawai, S.; Takagi, Y.; Kaneko, S.; Kurosawa, T. Effect of three types of mixed anesthetic agents alternate to ketamine in mice. Exp. Anim. 2011, 60, 481–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, S.M.; Sneyd, J.R. Nitrous oxide in modern anaesthetic practice. BJA Educ. 2016, 16, 87–91. [Google Scholar] [CrossRef] [Green Version]
- Zafirova, Z.; Sheehan, C.; Hosseinian, L. Update on nitrous oxide and its use in anesthesia practice. Best Pract. Res. Clin. Anaesthesiol. 2018, 32, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Szabó, A.; Vollmar, B.; Boros, M.; Menger, M.D. Gender differences in ischemia-reperfusion-induced microcirculatory and epithelial dysfunctions in the small intestine. Life Sci. 2006, 78, 3058–3065. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, W.; Wu, G. Intestinal ischemic reperfusion injury: Recommended rats model and comprehensive review for protective strategies. Biomed. Pharmacother. 2021, 138, 111482. [Google Scholar] [CrossRef]
- Percie du Sert, N.; Hurst, V.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; et al. The ARRIVE guidelines 2.0: Updated guidelines for reporting animal research. PLoS Biol. 2020, 18, e3000410. [Google Scholar] [CrossRef]
- Chiu, C.J.; McArdle, A.H.; Brown, R.; Scott, H.J.; Gurd, F.N. Intestinal mucosal lesion in low-flow states: I. A morphological, hemodynamic, and metabolic reappraisal. Arch. Surg. 1970, 101, 478–483. [Google Scholar] [CrossRef]
- Park, P.; Haglund, U.; Bulkley, G.; Fält, K. The sequence of development of intestinal tissue injury after strangulation ischemia and reperfusion. Surgery 1990, 107, 574–580. [Google Scholar] [PubMed]
- Grootjans, J.; Thuijls, G.; Derikx, J.P.M.; Van Dam, R.M.; Dejong, C.H.C.; Buurman, W.A. Rapid lamina propria retraction and zipper-like constriction of the epithelium preserves the epithelial lining in human small intestine exposed to ischaemia-reperfusion. J. Pathol. 2011, 224, 411–419. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
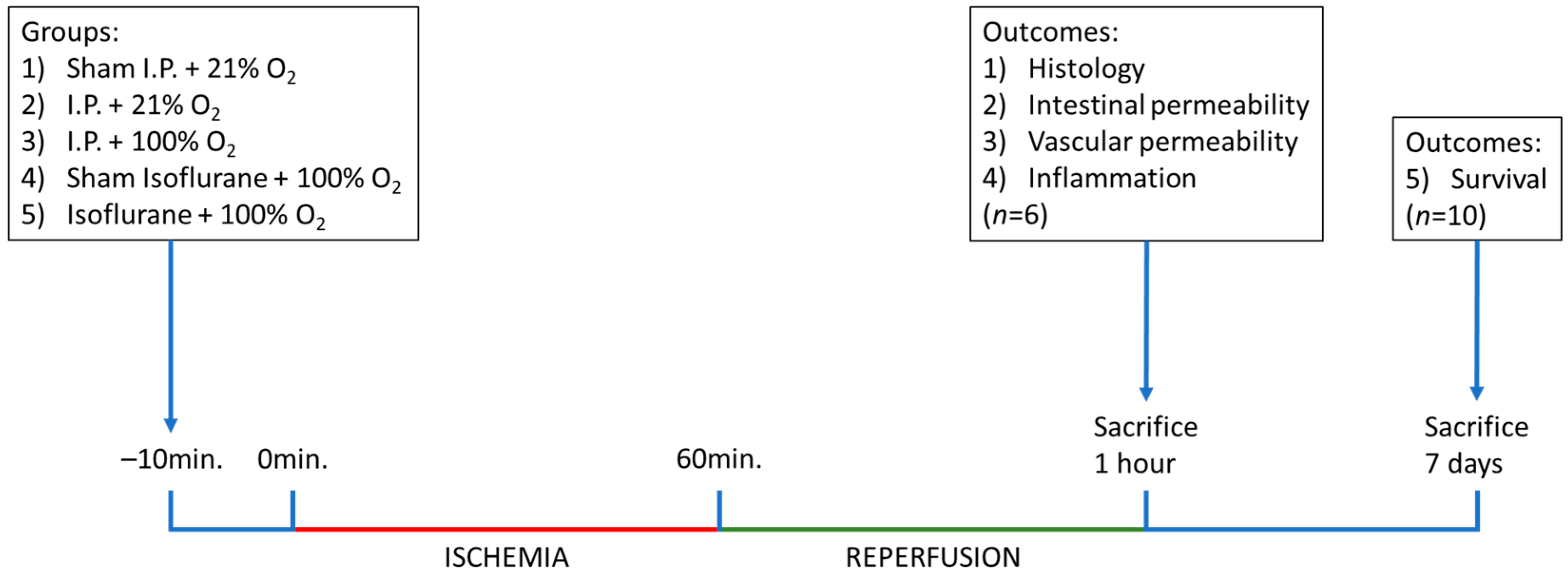
| Group | Ischemia | Oxygen | Anesthesia |
|---|---|---|---|
| Sham I.P. + 21% O2 | Sham | 21% | Ketamine–Xylazine |
| I.P. + 21% O2 | 60 min | 21% | Ketamine–Xylazine |
| I.P. + 100% O2 | 60 min | 100% | Ketamine–Xylazine |
| Sham isoflurane + 100% O2 | Sham | 100% | Isoflurane |
| Isoflurane + 100% O2 | 60 min | 100% | Isoflurane |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clarysse, M.; Accarie, A.; Farré, R.; Canovai, E.; Monbaliu, D.; Gunst, J.; De Hertogh, G.; Vanuytsel, T.; Pirenne, J.; Ceulemans, L.J. Protective Effect of Oxygen and Isoflurane in Rodent Model of Intestinal Ischemia-Reperfusion Injury. Int. J. Mol. Sci. 2023, 24, 2587. https://doi.org/10.3390/ijms24032587
Clarysse M, Accarie A, Farré R, Canovai E, Monbaliu D, Gunst J, De Hertogh G, Vanuytsel T, Pirenne J, Ceulemans LJ. Protective Effect of Oxygen and Isoflurane in Rodent Model of Intestinal Ischemia-Reperfusion Injury. International Journal of Molecular Sciences. 2023; 24(3):2587. https://doi.org/10.3390/ijms24032587
Chicago/Turabian StyleClarysse, Mathias, Alison Accarie, Ricard Farré, Emilio Canovai, Diethard Monbaliu, Jan Gunst, Gert De Hertogh, Tim Vanuytsel, Jacques Pirenne, and Laurens J. Ceulemans. 2023. "Protective Effect of Oxygen and Isoflurane in Rodent Model of Intestinal Ischemia-Reperfusion Injury" International Journal of Molecular Sciences 24, no. 3: 2587. https://doi.org/10.3390/ijms24032587