
Lupus Nephritis Risk Factors and Biomarkers: An Update

Abstract
:
1. Introduction
2. Epidemiology of LN
- A young age at SLE diagnosis, which favors LN with a cut-off fixed at 33 years old [2]. This explains that LN frequency (80% vs. 30–50%) is two-fold higher in patients with juvenile-onset as compared to adult-onset together with a more severe disease and fatal evolution with 10% ESKD in juvenile-onset as compared to 4% in adult-onset [3,4].
- The prevalence of LN varies by race and ethnicity with African/Caribbean and Asian/Pacific islanders at high risk (35–80%), Hispanic (30–50%) at moderate risk, and Caucasian at low risk (15–25%). In addition, it has been further demonstrated that black SLE patients with African ancestors are characterized by a more aggressive renal disease when considering histological lesions, disease activity scores, lower therapeutic response, and worse outcome as compared to white patients [5].
- A higher frequency is reported in males as compared to females (1.1×–1.7×), which is not influenced by race/ethnicity. This contrasts with the strong sex bias reported in SLE especially during childbearing for females (female-to-male ratio: 6–13:1). SLE males have an older age at disease onset but early damage; however, conflicting results between males and females, most probably in conjunction with their racial/ethnic background, are reported when considering histological classification, disease activity, therapeutic response, flares, ESKD, and mortality [6,7].
- Heritability is high in SLE, which results in a relative risk to develop SLE estimated at 30% in monozygotic twins to 5–7% in dizygotic twins and first-degree relatives, with males being rarely affected [8]. Among LN patients with a familial SLE history, fever appeared to be more frequent as well as a poor renal outcome [9,10]; this is contrasted by a lower risk to develop LN, photosensitivity, and thrombocytopenia as compared to non-familial SLE [11].

{kind=link}
{kind=link}
{kind=link}
| Epidemiological Factor | Predict LN | Disease Activity | Therapeutic Response | Flares | ESKD |
|---|---|---|---|---|---|
| Juvenile SLE | 2× in juvenile | Juvenile > adult | Adult > juvenile | Juvenile > adult | Juvenile > adult |
| Race/ethnicity (black/white) | 2× in black | Black > white | White > black | Black > white | 9× in black |
| Male vs. female | 1.1×–1.7× | Conflict results | Conflict results | Conflict results | Conflict results |
| Familial cases | Protective | Variable | Unknown | Unknown | High |
| Monogenic SLE | Yes (<5 years old) | High | Unknown | Unknown | Unknown |
3. Renal Histology
| Predict Disease Activity | Therapeutic Response | Predict Flares | Predict ESKD | |
|---|---|---|---|---|
| Proliferative LN (class III/IV ± V) | Yes (1st/2nd biopsy) | Non-responder (2nd > 1st biopsy) | No | Yes (2nd > 1st biopsy) |
| IFTA (Chronicity) | No | Responder (>25%) | No | Yes (baseline > 25%) |
| TMA | Yes (independent) | Yes (independent) | Unknown | Yes (independent) |
| Tissular C1q+/C3+/− | Yes | Responder | Yes | No |
| Tissular C1q−/C3+ | No | Non-responder | No | Yes |
4. Genetic/Epigenetic/Transcriptomic Pathways and Related Biomarkers in LN
| Pathways | Factors | Related Biomarkers |
|---|---|---|
| DNA/RNA clearance | DNASE1L3 *, DNAse1 *, RNASEH2A/B/C * | DNAse activity |
| Complement | C1q *, C1s *, C1r *, C2 *, C4 (CNV), C3 * | C3, C4, CH50 |
| DNA/RNA sensing & Type I IFN | TLR7 *, IFIH1/MDA5 *, IRF7 *, IRF5, TASL, IRAK1, STAT4, IFI16 | Type I IFN signature, IFN-α, anti-interferon Abs |
| Type II IFN | IFN-γ | Type II IFN signature, IFN-γ |
4.1. RNA/DNA Clearance by Nucleases
4.2. Classical Complement Pathway
4.3. Type I and Type II Interferons
- Proliferative class III/IV LN are characterized by prominent type I and type II IFN signatures in renal epithelial cells.
- Membranous class V LN can be distinguished by elevated type I IFN and tumor necrosis (TNF)-α signatures together with an altered cell metabolism signature in renal epithelial cells, thus suggesting distinct pathophysiology processes between proliferative and membranous LN.
- Type I IFN level in renal tubular cells correlates with an elevated IFTA chronicity index, which supports a role for type I IFN, reinforced or not with type II IFN, to promote ESKD.
- When detected in renal leukocytes, the type I IFN response drives an extrafollicular B cell response with aged/autoreactive B cells (ABC) and T follicular regulatory CD4+ T cells.
- An IFN signature in renal tubular cells recapitulates the IFN signature in skin biopsies, and the IFN signature in infiltrating renal leukocytes can be appreciated by exploring peripheral blood mononuclear cells (PBMCs).
5. Nephropathic Antibodies in LN
- Abs targeting RNA/DNA nucleic acids.
- Abs targeting glomerular antigens, particularity the part of them which cross-react with anti-dsDNA Abs.
- Functional Abs targeting pathophysiological pathways (e.g., anti-DNAse1L3 Abs, anti-C1q Abs, anti-IFN Abs, please refer to Section 4).
- Abs targeting anti-phospholipids and cofactors.
| Autoantibody (Ab) | Predict LN (Histology) | Predict Disease Activity | Therapeutic Response | Predict Flares | Predict ESKD |
|---|---|---|---|---|---|
| Anti-dsDNA Abs | High levels (III & IV > V) | High levels | Responder | High levels | Low |
| Anti-Sm Abs | No | Suspected | Unknown | Suspected | Suspected |
| Anti-SSB Abs | No | No | No | No | No |
| Anti-α actinin Abs | Yes | Yes | Unknown | Unknown | Unknown |
| Anti-CL/β2 GPI Abs | No | No | Low | No | Yes (thrombotic microangiopathy) |
5.1. Abs Targeting Nucleic Acids
5.2. Anti-dsDNA/Glomerular Antibodies
5.3. Anti-Phospholipid Antibodies
6. Urinary Biomarkers Associated with LN
| Biomarker | Active LN/Glomerulonephritis | Therapeutic Response | Predict Flares | Predict ESKD |
|---|---|---|---|---|
| Renal markers | 24 h proteinuria, SUA, uGAL3BP | 24 h proteinuria | 24 h proteinuria | 24 h proteinuria, SUA, GFR |
| Cytokine/chemokines | TWEAK, MCP-1/CCL2 | TWEAK, MCP-1/CCL2, BAFF | MCP-1/CCL2 | TWEAK, MCP-1/CCL2 |
| Cell adhesion molecules | ALCAM, VCAM, NGAL, KIM1, sCD163 | VCAM1, sCD163, | VCAM1, sCD163, KIM1 | NGAL, ALCAM, VCAM1, KIM1, sCD163 |
| miRs | miR-146a, miR-204, miR-30c, miR-3201, miR-1273e | miR-135 | miR-146a | miR-146a |
6.1. Proteinuria and Protein to Creatinuria Ratio
6.2. Cytokines/Chemokines
6.3. Cell Adhesion Molecules
6.4. mi-RNAs
7. Lessons from Therapeutic Trials
- A better control of the type I IFN pathway, complement fractions, and anti-dsDNA/C1q Abs levels is reported with anifrolumab and belimumab [133,134]. Post-hoc analysis has further reported that responders presented an elevated type I IFN signature at baseline, which supports using this biomarker for therapeutic decisions although it has not been validated in a controlled trial [135,136]. According to Weeding et al., a reduction in urinary sCD163 best predicts a complete response when belimumab is used as an add-on therapy [137].
- A better control of complement fractions and anti-dsDNA/C1q Abs levels is reported with all anti-CD20 mAbs, but among them, only obinutizumab (class II anti-CD20 mAbs) was effective in improving renal response compared with the SOC [66,138,139,140]. Future directions regarding anti-B cell therapies in LN are related to the use of combinations between anti-CD20 and anti-BAFF, the use of anti-CD38 mAb (daratumab) to target long-lived plasma-cells not covered by anti-CD20 mAbs, and the use of CAR T cells that have reported a complete response in six refractory SLE patients, all with LN [65,141,142,143].
| Drugs | Renal Response vs. Controls (%) | Complement Consumption | Anti-dsDNA Abs | Anti-C1q Abs | Anti-SSA/B and Anti-Sm/RNP | Other Biomarkers |
|---|---|---|---|---|---|---|
| SOC (e.g., mycophenolic acid) [144,145,146] | 20–40% | Improvement | Decrease | Decrease | No effect | Control Type I IFN |
| Jak inhibitors vs. SOC [131,147] | Similar to SOC | No effect | Decrease | Unknown | Decrease at high level | Control Type I/II IFN |
| Voclosporin vs. SOC [132] | 44% vs. 23% | No effect | Decrease | Decrease | No effect | Unknown |
| Anifrolumab vs. SOC [133,135] | 45% vs. 31% | Improvement | Decrease | Decrease | No effect | IFN-I high |
| Belimumab vs. SOC [134,136,137,148,149] | 43% vs. 32% | Improvement | Decrease | Unknown | Decrease at high level | IFN-I high, sCD163 |
| Obinituzimab (type II anti-CD20) [138] | 35% vs. 23% | Improvement | Decrease | Decrease | No effect | Unknown |
| Refractory SLE (mostly LN) | ||||||
| Belimumab + rituximab [141,150,151] | 52% vs. 41% | Improvement | CR: delayed negativity | CR: decrease | CR: mild decrease | Unknown |
| CAR T cells [65] | 100% | Normalization | Negativation | Negativation | Negativation | Unknown |
| Daratumab (CD38) [67,142] | Normalization | Decrease | Decrease | Unknown | Control Type I IFN | |
8. Future Challenges
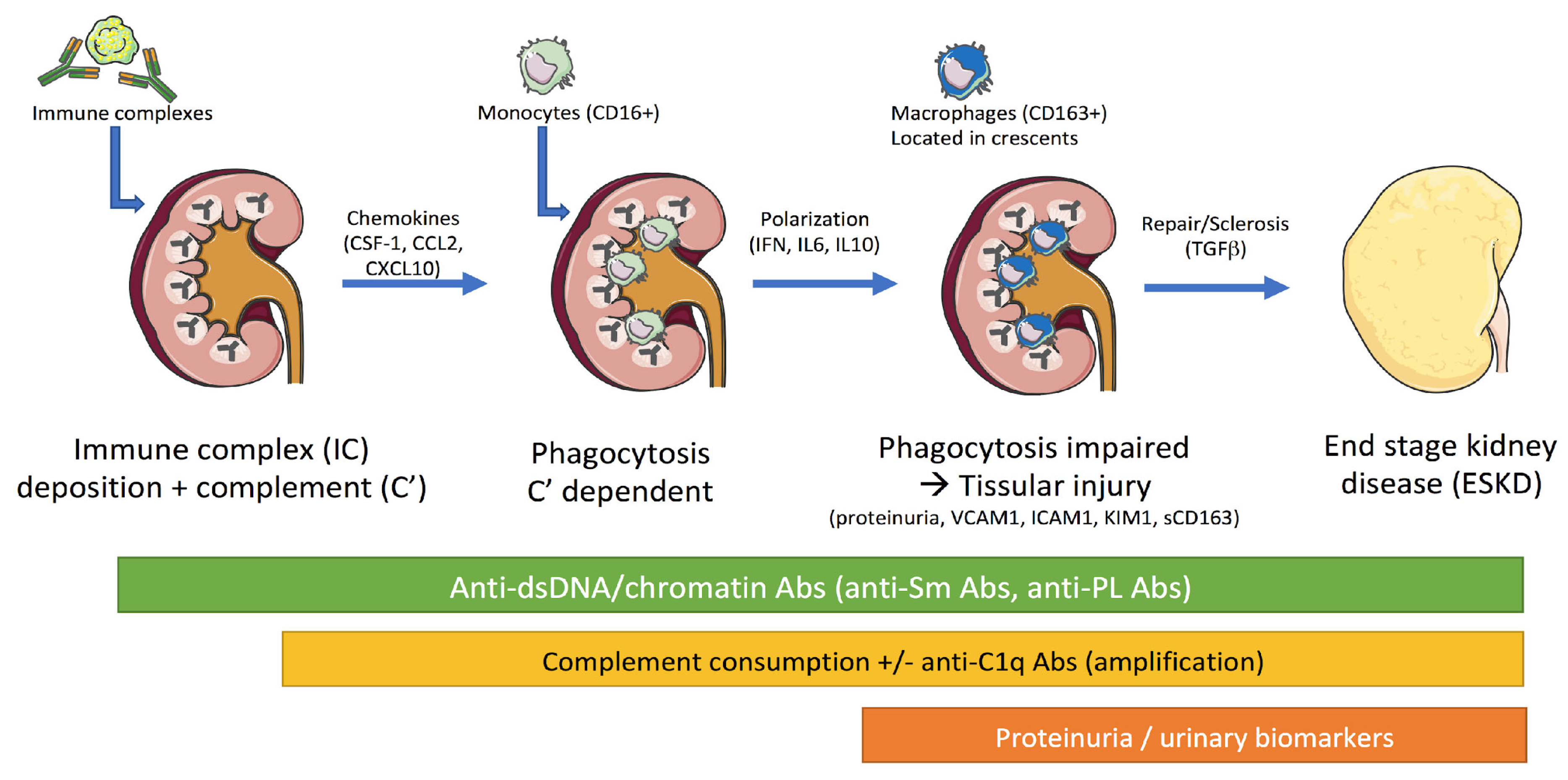
- Challenge 1: Better understand the molecular pathways implicated in LN and for that, single-cell multi-omic analysis may be informative (e.g., Sc-RNASeq, Sc-proteomic…) and contribute to the identification of new biomarkers in LN. Recently, kidney samples from patients with lupus nephritis and from healthy control subjects were analyzed thanks to single-cell RNA sequencing [27]. The analysis revealed 21 subsets of leukocytes active in the disease, including multiple populations of myeloid cells. Classification and annotation of myeloid cell clusters (C) revealed resident and infiltrating populations. Focused analysis of the 466 cells in myeloid clusters C4 and C6 revealed 5 finer clusters. Two of them were found to express CD163 transcripts, suggesting that such an approach can allow for the identification of the glomerular urinary sCD163-producing cells. Because these cells have been implicated in renal prognosis, it could represent a new prognostic factor to correlate to renal outcome. In-depth characterization of renal immune cells is a pre-requisite to then screen for therapeutic candidates including drug repurposing approaches using virtual and experimental screening techniques.
- Challenge 2: Properly evaluate biomarkers and for that, validation of such requires multi-ethnic and larger cohorts as well as well-annotated clinical cohorts with the main objectives being to provide more reliable biomarkers with a high performance in terms of sensitivity and specificity (≥90%) that can (i) replace initial/follow-up renal biopsies; (ii) determine the therapy that is the best fit for the patient; (iii) prevent ESKD/fatal evolutions; and (iv) reduce side effects.
- Challenge 3: Evaluate the complementarity and determine the minimal number of biomarkers combined with clinical signs to help in better guiding clinicians and researchers in their choices. For that, one example would be to develop “LN scores” integrating clinical signs with circulating and urinary biomarkers by using advances in bioinformatics using artificial intelligence, available databases from real-life cohorts, and studies on longitudinal evolution [152].
- Challenge 4: Propose new criteria for the evaluation of LN activity, LN fibrosis, therapeutic response/choice, and for that, more accurate biomarkers have to be selected in order to capture moderate and mild changes, and to avoid hospitalizations and invasive exams. One example is that accurate biomarkers could help both for the early detection of refractory forms of LN before the usual clinical visit, and to distinguish residual proteinuria from active proteinuria, which is currently impossible without biopsy. Another example is that nephrologists have to weigh the benefit/risk ratio for empiric steroid therapy when anti-phospholipid syndrome is associated with SLE and when patients should not interrupt anti-coagulant therapies. This is of particular complexity when LN is active and the patient has already experienced severe thrombotic complications. In such a situation, a non-invasive signature of renal activity could allow for tailoring appropriate immunosuppressive intensity to the clinical situation.
- Challenge 5: Characterize and recruit for future clinical trials cohorts of homogeneous LN patients with similar biological profiles (aka, endotypes), organ involvement, comorbidities, and severity.
- Challenge 6: Use adapted biomarkers to identify LN patients at particular risk of associated severe organ involvement and damage, for severe drug side effects, and for infection/tumor susceptibility.
- Challenge 7: Develop biomarkers to improve pregnancy outcomes as this is a major concern in women with SLE regarding LN flares, pre-eclampsia, and congenital heart block in the fetus involving anti-SSA Abs.
- Challenge 8: Propose biomarkers toward LN as health-related quality of life including, for example, fatigue, pain, and psychological behaviors which are aspects of LN of high concern for patients and result, in part, from immunological processes.
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anders, H.-J.; Saxena, R.; Zhao, M.-H.; Parodis, I.; Salmon, J.E.; Mohan, C. Lupus Nephritis. Nat. Rev. Dis. Primers 2020, 6, 7. [Google Scholar] [CrossRef] [PubMed]
- Seligman, V.A.; Lum, R.F.; Olson, J.L.; Li, H.; Criswell, L.A. Demographic Differences in the Development of Lupus Nephritis: A Retrospective Analysis. Am. J. Med. 2002, 112, 726–729. [Google Scholar] [CrossRef]
- Renaudineau, Y.; Muller, S.; Hedrich, C.M.; Chauveau, D.; Bellière, J.; De Almeida, S.; Damoiseaux, J.; Scherlinger, M.; Guery, J.C.; Sailler, L.; et al. Immunological and Translational Key Challenges in Systemic Lupus Erythematosus: A Symposium Update. J. Transl. Autoimmun. 2023, 6, 100199. [Google Scholar] [CrossRef] [PubMed]
- Robinson, G.A.; Peng, J.; Dönnes, P.; Coelewij, L.; Naja, M.; Radziszewska, A.; Wincup, C.; Peckham, H.; Isenberg, D.A.; Ioannou, Y.; et al. Disease-Associated and Patient-Specific Immune Cell Signatures in Juvenile-Onset Systemic Lupus Erythematosus: Patient Stratification Using a Machine-Learning Approach. Lancet Rheumatol. 2020, 2, e485–e496. [Google Scholar] [CrossRef] [PubMed]
- Korbet, S.M.; Schwartz, M.M.; Evans, J.; Lewis, E.J.; Collaborative Study Group. Severe Lupus Nephritis: Racial Differences in Presentation and Outcome. J. Am. Soc. Nephrol. JASN 2007, 18, 244–254. [Google Scholar] [CrossRef] [PubMed]
- Trentin, F.; Signorini, V.; Maria Manca, L.; Cascarano, G.; Gualtieri, L.; Schilirò, D.; Valevich, A.; Cardelli, C.; Carli, L.; Elefante, E.; et al. Gender Differences in SLE: Report from a Cohort of 417 Caucasian Patients. Lupus Sci. Med. 2023, 10, e000880. [Google Scholar] [CrossRef]
- Ramírez Sepúlveda, J.I.; Bolin, K.; Mofors, J.; Leonard, D.; Svenungsson, E.; Jönsen, A.; Bengtsson, C.; DISSECT Consortium; Nordmark, G.; Rantapää Dahlqvist, S.; et al. Sex Differences in Clinical Presentation of Systemic Lupus Erythematosus. Biol. Sex Differ. 2019, 10, 60. [Google Scholar] [CrossRef]
- Brooks, W.H.; Le Dantec, C.; Pers, J.-O.; Youinou, P.; Renaudineau, Y. Epigenetics and Autoimmunity. J. Autoimmun. 2010, 34, J207–J219. [Google Scholar] [CrossRef]
- Wang, Z.; Tang, Z.; Zhang, H.T.; Hu, W.X.; Liu, Z.H.; Li, L.S. Clinicopathological Characteristics of Familial SLE Patients with Lupus Nephritis. Lupus 2009, 18, 243–248. [Google Scholar] [CrossRef]
- Huang, X.; Tang, Z.; Wu, X.; Zhang, L.; Fan, W.; Zhang, H.; Hu, W.; Liu, Z. Long-Term Renal Outcomes and Related Risk Factors of Familial Systemic Lupus Erythematosus Patients with Lupus Nephritis. Clin. Nephrol. 2018, 90, 262–269. [Google Scholar] [CrossRef]
- Chen, L.Y.; Shi, Z.R.; Tan, G.Z.; Han, Y.F.; Tang, Z.Q.; Wang, L. Systemic Lupus Erythematosus with and without a Family History: A Meta-Analysis. Lupus 2018, 27, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Izquierdo, M.; Rodriguez-Almaraz, E.; Pego-Reigosa, J.M.; López-Longo, F.J.; Calvo-Alén, J.; Olivé, A.; Fernández-Nebro, A.; Martinez-Taboada, V.; Vela-Casasempere, P.; Freire, M.; et al. Characterization of Patients with Lupus Nephritis Included in a Large Cohort from the Spanish Society of Rheumatology Registry of Patients with Systemic Lupus Erythematosus (RELESSER). Medicine 2016, 95, e2891. [Google Scholar] [CrossRef] [PubMed]
- Du, K.; Zhang, X.; Feng, J.; Zhong, S.; Qi, J.; Lin, Z. Renal Response and Its Predictive Factors of Lupus Nephritis: A 2-Year Real-World Study of 56 Hospital-Based Patients. Clin. Rheumatol. 2022, 41, 3363–3371. [Google Scholar] [CrossRef] [PubMed]
- Bajema, I.M.; Wilhelmus, S.; Alpers, C.E.; Bruijn, J.A.; Colvin, R.B.; Terence Cook, H.; D’Agati, V.D.; Ferrario, F.; Haas, M.; Jennette, J.C.; et al. Revision of the International Society of Nephrology/Renal Pathology Society Classification for Lupus Nephritis: Clarification of Definitions, and Modified National Institutes of Health Activity and Chronicity Indices. Kidney Int. 2018, 93, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Almaraz, E.; Gutiérrez-Solís, E.; Rabadán, E.; Rodríguez, P.; Alonso, M.; Carmona, L.; de Yébenes, M.J.G.; Morales, E.; Galindo-Izquierdo, M. Searching for a Prognostic Index in Lupus Nephritis. Eur. J. Med. Res. 2023, 28, 19. [Google Scholar] [CrossRef] [PubMed]
- Tamirou, F.; Lauwerys, B.R.; Dall’Era, M.; Mackay, M.; Rovin, B.; Cervera, R.; Houssiau, F.A.; MAINTAIN Nephritis Trial Investigators. A Proteinuria Cut-off Level of 0.7 g/Day after 12 Months of Treatment Best Predicts Long-Term Renal Outcome in Lupus Nephritis: Data from the MAINTAIN Nephritis Trial. Lupus Sci. Med. 2015, 2, e000123. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Kostopoulou, M.; Cheema, K.; Anders, H.-J.; Aringer, M.; Bajema, I.; Boletis, J.; Frangou, E.; Houssiau, F.A.; Hollis, J.; et al. 2019 Update of the Joint European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) Recommendations for the Management of Lupus Nephritis. Ann. Rheum. Dis. 2020, 79, 713–723. [Google Scholar] [CrossRef]
- Gatto, M.; Radice, F.; Saccon, F.; Calatroni, M.; Frontini, G.; Trezzi, B.; Zen, M.; Ghirardello, A.; Tamborini, F.; Binda, V.; et al. Clinical and Histological Findings at Second but Not at First Kidney Biopsy Predict End-Stage Kidney Disease in a Large Multicentric Cohort of Patients with Active Lupus Nephritis. Lupus Sci. Med. 2022, 9, e000689. [Google Scholar] [CrossRef]
- Koopman, J.J.E.; Rennke, H.G.; McMahon, G.M.; Waikar, S.S.; Costenbader, K.H. Associations between Renal Deposits of Complement Factors, Disease Activity and Loss of Renal Function in Lupus Nephritis. J. Clin. Pathol. 2022, 75, 789–790. [Google Scholar] [CrossRef]
- Kim, H.; Kim, T.; Kim, M.; Lee, H.W.; Kim, Y.; Kang, M.S.; Kim, J. Activation of the Alternative Complement Pathway Predicts Renal Outcome in Patients with Lupus Nephritis. Lupus 2020, 29, 862–871. [Google Scholar] [CrossRef]
- Chen, X.; Cheng, W.; Wang, G.; Qi, Y.; Xiao, J.; Wang, X.; Zhao, Z. Clinical Characteristics and Prognosis of Renal Thrombotic Microangiopathy in Lupus Nephritis. Iran. J. Kidney Dis. 2021, 15, 169–176. [Google Scholar] [PubMed]
- Gupta, K.L.; Bharati, J.; Anakutti, H.; Pattanashetti, N.; Rathi, M.; Ramachandran, R.; Nada, R. Contribution of Clinically Indicated Repeat Renal Biopsy in Indian Patients with Lupus Nephritis. Indian J. Nephrol. 2020, 30, 377–381. [Google Scholar] [CrossRef]
- Lledó-Ibáñez, M.G.; Xipell, M.; Ferreira, M.; Solé, M.; Garcia-Herrera, A.; Cervera, R.; Quintana, L.F.; Espinosa, G. Kidney Biopsy in Lupus Nephritis after Achieving Clinical Renal Remission: Paving the Way for Renal Outcome Assessment. Clin. Kidney J. 2022, 15, 2081–2088. [Google Scholar] [CrossRef] [PubMed]
- Charras, A.; Haldenby, S.; Smith, E.M.D.; Egbivwie, N.; Olohan, L.; Kenny, J.G.; Schwarz, K.; Roberts, C.; Al-Abadi, E.; Armon, K.; et al. Panel Sequencing Links Rare, Likely Damaging Gene Variants with Distinct Clinical Phenotypes and Outcomes in Juvenile-Onset SLE. Rheumatology 2023, 62, SI210–SI225. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.J.; Cañete, P.F.; Wang, H.; Medhavy, A.; Bones, J.; Roco, J.A.; He, Y.; Qin, Y.; Cappello, J.; Ellyard, J.I.; et al. TLR7 Gain-of-Function Genetic Variation Causes Human Lupus. Nature 2022, 605, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Vinuesa, C.G.; Shen, N.; Ware, T. Genetics of SLE: Mechanistic Insights from Monogenic Disease and Disease-Associated Variants. Nat. Rev. Nephrol. 2023, 19, 558–572. [Google Scholar] [CrossRef] [PubMed]
- Arazi, A.; Rao, D.A.; Berthier, C.C.; Davidson, A.; Liu, Y.; Hoover, P.J.; Chicoine, A.; Eisenhaure, T.M.; Jonsson, A.H.; Li, S.; et al. The Immune Cell Landscape in Kidneys of Patients with Lupus Nephritis. Nat. Immunol. 2019, 20, 902–914. [Google Scholar] [CrossRef]
- Barturen, G.; Babaei, S.; Català-Moll, F.; Martínez-Bueno, M.; Makowska, Z.; Martorell-Marugán, J.; Carmona-Sáez, P.; Toro-Domínguez, D.; Carnero-Montoro, E.; Teruel, M.; et al. Integrative Analysis Reveals a Molecular Stratification of Systemic Autoimmune Diseases. Arthritis Rheumatol. 2021, 73, 1073–1085. [Google Scholar] [CrossRef]
- Niu, Z.; Zhang, P.; Tong, Y. Value of HLA-DR Genotype in Systemic Lupus Erythematosus and Lupus Nephritis: A Meta-Analysis. Int. J. Rheum. Dis. 2015, 18, 17–28. [Google Scholar] [CrossRef]
- Chowdhary, V.R.; Dai, C.; Tilahun, A.Y.; Hanson, J.A.; Smart, M.K.; Grande, J.P.; Rajagopalan, G.; Fu, S.-M.; David, C.S. A Central Role for HLA-DR3 in Anti-Smith Antibody Responses and Glomerulonephritis in a Transgenic Mouse Model of Spontaneous Lupus. J. Immunol. 2015, 195, 4660–4667. [Google Scholar] [CrossRef]
- Al-Mayouf, S.M.; Sunker, A.; Abdwani, R.; Al Abrawi, S.; Almurshedi, F.; Alhashmi, N.; Al Sonbul, A.; Sewairi, W.; Qari, A.; Abdallah, E.; et al. Loss-of-Function Variant in DNASE1L3 Causes a Familial Form of Systemic Lupus Erythematosus. Nat. Genet. 2011, 43, 1186–1188. [Google Scholar] [CrossRef] [PubMed]
- Bruschi, M.; Bonanni, A.; Petretto, A.; Vaglio, A.; Pratesi, F.; Santucci, L.; Migliorini, P.; Bertelli, R.; Galetti, M.; Belletti, S.; et al. Neutrophil Extracellular Traps Profiles in Patients with Incident Systemic Lupus Erythematosus and Lupus Nephritis. J. Rheumatol. 2020, 47, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Hartl, J.; Serpas, L.; Wang, Y.; Rashidfarrokhi, A.; Perez, O.A.; Sally, B.; Sisirak, V.; Soni, C.; Khodadadi-Jamayran, A.; Tsirigos, A.; et al. Autoantibody-Mediated Impairment of DNASE1L3 Activity in Sporadic Systemic Lupus Erythematosus. J. Exp. Med. 2021, 218, e20201138. [Google Scholar] [CrossRef] [PubMed]
- De Holanda, M.I.; Klumb, E.; Imada, A.; Lima, L.A.; Alcântara, I.; Gregório, F.; Christiani, L.F.; Martins, C.O.; Timoner, B.E.; Motta, J.; et al. The Prevalence of HLA Alleles in a Lupus Nephritis Population. Transpl. Immunol. 2018, 47, 37–43. [Google Scholar] [CrossRef]
- Dasdemir, S.; Yildiz, M.; Celebi, D.; Sahin, S.; Aliyeva, N.; Haslak, F.; Gunalp, A.; Adrovic, A.; Barut, K.; Artim Esen, B.; et al. Genetic Screening of Early-Onset Patients with Systemic Lupus Erythematosus by a Targeted next-Generation Sequencing Gene Panel. Lupus 2022, 31, 330–337. [Google Scholar] [CrossRef]
- Kallenberg, C.G.M. Anti-C1q Autoantibodies. Autoimmun. Rev. 2008, 7, 612–615. [Google Scholar] [CrossRef]
- Liu, L.; Wang, R.; Ding, H.; Tian, L.; Gao, T.; Bao, C. The Utility of Urinary Biomarker Panel in Predicting Renal Pathology and Treatment Response in Chinese Lupus Nephritis Patients. PLoS ONE 2020, 15, e0240942. [Google Scholar] [CrossRef]
- Trouw, L.A.; Groeneveld, T.W.L.; Seelen, M.A.; Duijs, J.M.G.J.; Bajema, I.M.; Prins, F.A.; Kishore, U.; Salant, D.J.; Verbeek, J.S.; Van Kooten, C.; et al. Anti-C1q Autoantibodies Deposit in Glomeruli but Are Only Pathogenic in Combination with Glomerular C1q-Containing Immune Complexes. J. Clin. Investig. 2004, 114, 679–688. [Google Scholar] [CrossRef]
- Lodi, L.; Mastrolia, M.V.; Bello, F.; Rossi, G.M.; Angelotti, M.L.; Crow, Y.J.; Romagnani, P.; Vaglio, A. Type I Interferon-Related Kidney Disorders. Kidney Int. 2022, 101, 1142–1159. [Google Scholar] [CrossRef]
- Nehar-Belaid, D.; Hong, S.; Marches, R.; Chen, G.; Bolisetty, M.; Baisch, J.; Walters, L.; Punaro, M.; Rossi, R.J.; Chung, C.H.; et al. Mapping Systemic Lupus Erythematosus Heterogeneity at the Single-Cell Level. Nat. Immunol. 2020, 21, 1094–1106. [Google Scholar] [CrossRef]
- Coit, P.; Ortiz-Fernandez, L.; Lewis, E.E.; McCune, J.W.; Maksimowicz-McKinnon, K.; Sawalha, A.H. A Longitudinal and Transancestral Analysis of DNA Methylation Patterns and Disease Activity in Lupus Patients. JCI Insight 2020, 5, 143654. [Google Scholar] [CrossRef] [PubMed]
- Garaud, S.; Le Dantec, C.; Jousse-Joulin, S.; Hanrotel-Saliou, C.; Saraux, A.; Mageed, R.A.; Youinou, P.; Renaudineau, Y. IL-6 Modulates CD5 Expression in B Cells from Patients with Lupus by Regulating DNA Methylation. J. Immunol. 2009, 182, 5623–5632. [Google Scholar] [CrossRef] [PubMed]
- Obermoser, G.; Presnell, S.; Domico, K.; Xu, H.; Wang, Y.; Anguiano, E.; Thompson-Snipes, L.; Ranganathan, R.; Zeitner, B.; Bjork, A.; et al. Systems Scale Interactive Exploration Reveals Quantitative and Qualitative Differences in Response to Influenza and Pneumococcal Vaccines. Immunity 2013, 38, 831–844. [Google Scholar] [CrossRef] [PubMed]
- Chiche, L.; Jourde-Chiche, N.; Whalen, E.; Presnell, S.; Gersuk, V.; Dang, K.; Anguiano, E.; Quinn, C.; Burtey, S.; Berland, Y.; et al. Modular Transcriptional Repertoire Analyses of Adults with Systemic Lupus Erythematosus Reveal Distinct Type I and Type II Interferon Signatures. Arthritis Rheumatol. 2014, 66, 1583–1595. [Google Scholar] [CrossRef]
- Munroe, M.E.; Lu, R.; Zhao, Y.D.; Fife, D.A.; Robertson, J.M.; Guthridge, J.M.; Niewold, T.B.; Tsokos, G.C.; Keith, M.P.; Harley, J.B.; et al. Altered Type II Interferon Precedes Autoantibody Accrual and Elevated Type I Interferon Activity Prior to Systemic Lupus Erythematosus Classification. Ann. Rheum. Dis. 2016, 75, 2014–2021. [Google Scholar] [CrossRef]
- Yiu, G.; Rasmussen, T.K.; Tsai, B.L.; Diep, V.K.; Haddon, D.J.; Tsoi, J.; Miller, G.D.; Comin-Anduix, B.; Deleuran, B.; Crooks, G.M.; et al. High Interferon Signature Leads to Increased STAT1/3/5 Phosphorylation in PBMCs From SLE Patients by Single Cell Mass Cytometry. Front. Immunol. 2022, 13, 833636. [Google Scholar] [CrossRef]
- Kennedy, W.P.; Maciuca, R.; Wolslegel, K.; Tew, W.; Abbas, A.R.; Chaivorapol, C.; Morimoto, A.; McBride, J.M.; Brunetta, P.; Richardson, B.C.; et al. Association of the Interferon Signature Metric with Serological Disease Manifestations but Not Global Activity Scores in Multiple Cohorts of Patients with SLE. Lupus Sci. Med. 2015, 2, e000080. [Google Scholar] [CrossRef]
- Der, E.; Suryawanshi, H.; Morozov, P.; Kustagi, M.; Goilav, B.; Ranabothu, S.; Izmirly, P.; Clancy, R.; Belmont, H.M.; Koenigsberg, M.; et al. Tubular Cell and Keratinocyte Single-Cell Transcriptomics Applied to Lupus Nephritis Reveal Type I IFN and Fibrosis Relevant Pathways. Nat. Immunol. 2019, 20, 915–927. [Google Scholar] [CrossRef]
- Fava, A.; Buyon, J.; Mohan, C.; Zhang, T.; Belmont, M.H.; Izmirly, P.; Clancy, R.; Trujillo, J.M.; Fine, D.; Zhang, Y.; et al. Integrated Urine Proteomics and Renal Single-Cell Genomics Identify an IFN-γ Response Gradient in Lupus Nephritis. JCI Insight 2020, 5, e138345. [Google Scholar] [CrossRef]
- Korsten, P.; Tampe, B. A Transcriptome Array-Based Approach Links Proteinuria and Distinct Molecular Signatures to Intrarenal Expression of Type I Interferon IFNA5 in Lupus Nephritis. Int. J. Mol. Sci. 2023, 24, 10636. [Google Scholar] [CrossRef]
- Wang, X.; Fu, S.; Yu, J.; Ma, F.; Zhang, L.; Wang, J.; Wang, L.; Tan, Y.; Yi, H.; Wu, H.; et al. Renal Interferon-Inducible Protein 16 Expression Is Associated with Disease Activity and Prognosis in Lupus Nephritis. Arthritis Res. Ther. 2023, 25, 112. [Google Scholar] [CrossRef]
- Morimoto, A.M.; Flesher, D.T.; Yang, J.; Wolslegel, K.; Wang, X.; Brady, A.; Abbas, A.R.; Quarmby, V.; Wakshull, E.; Richardson, B.; et al. Association of Endogenous Anti-Interferon-α Autoantibodies with Decreased Interferon-Pathway and Disease Activity in Patients with Systemic Lupus Erythematosus. Arthritis Rheumatol. 2011, 63, 2407–2415. [Google Scholar] [CrossRef] [PubMed]
- Nolte, K.U.; Günther, G.; von Wussow, P. Epitopes Recognized by Neutralizing Therapy-Induced Human Anti-Interferon-Alpha Antibodies Are Localized within the N-Terminal Functional Domain of Recombinant Interferon-Alpha 2. Eur. J. Immunol. 1996, 26, 2155–2159. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Tatouli, I.P.; Rosen, L.B.; Hasni, S.; Alevizos, I.; Manna, Z.G.; Rivera, J.; Jiang, C.; Siegel, R.M.; Holland, S.M.; et al. Distinct Functions of Autoantibodies Against Interferon in Systemic Lupus Erythematosus: A Comprehensive Analysis of Anticytokine Autoantibodies in Common Rheumatic Diseases. Arthritis Rheumatol. 2016, 68, 1677–1687. [Google Scholar] [CrossRef] [PubMed]
- Harris, B.D.; Kuruganti, S.; Deshpande, A.; Goepfert, P.A.; Chatham, W.W.; Walter, M.R. Characterization of Type-I IFN Subtype Autoantibodies and Activity in SLE Serum and Urine. Lupus 2020, 29, 1095–1105. [Google Scholar] [CrossRef]
- Siddiqi, K.Z.; Wilhelm, T.R.; Ulff-Møller, C.J.; Jacobsen, S. Cluster of Highly Expressed Interferon-Stimulated Genes Associate More with African Ancestry than Disease Activity in Patients with Systemic Lupus Erythematosus. A Systematic Review of Cross-Sectional Studies. Transl. Res. J. Lab. Clin. Med. 2021, 238, 63–75. [Google Scholar] [CrossRef]
- Simon, Q.; Grasseau, A.; Boudigou, M.; Le Pottier, L.; Bettachioli, E.; Cornec, D.; Rouvière, B.; Jamin, C.; Le Lann, L.; PRECISESADS Clinical Consortium; et al. A Proinflammatory Cytokine Network Profile in Th1/Type 1 Effector B Cells Delineates a Common Group of Patients in Four Systemic Autoimmune Diseases. Arthritis Rheumatol. 2021, 73, 1550–1561. [Google Scholar] [CrossRef]
- Gómez-Bañuelos, E.; Fava, A.; Andrade, F. An Update on Autoantibodies in Systemic Lupus Erythematosus. Curr. Opin. Rheumatol. 2023, 35, 61–67. [Google Scholar] [CrossRef]
- Mannik, M.; Merrill, C.E.; Stamps, L.D.; Wener, M.H. Multiple Autoantibodies Form the Glomerular Immune Deposits in Patients with Systemic Lupus Erythematosus. J. Rheumatol. 2003, 30, 1495–1504. [Google Scholar]
- Ichinose, K.; Kitamura, M.; Sato, S.; Eguchi, M.; Okamoto, M.; Endo, Y.; Tsuji, S.; Takatani, A.; Shimizu, T.; Umeda, M.; et al. Complete Renal Response at 12 Months after Induction Therapy Is Associated with Renal Relapse-Free Rate in Lupus Nephritis: A Single-Center, Retrospective Cohort Study. Lupus 2019, 28, 501–509. [Google Scholar] [CrossRef]
- Rodriguez-Jimenez, N.A.; Perez-Guerrero, E.E.; Gamez-Nava, J.I.; Sanchez-Mosco, D.I.; Saldaña-Cruz, A.M.; Alcaraz-Lopez, M.F.; Fajardo-Robledo, N.S.; Muñoz-Valle, J.F.; Bonilla-Lara, D.; Diaz-Rizo, V.; et al. Anti-Nucleosome Antibodies Increase the Risk of Renal Relapse in a Prospective Cohort of Patients with Clinically Inactive Systemic Lupus Erythematosus. Sci. Rep. 2020, 10, 12698. [Google Scholar] [CrossRef] [PubMed]
- Pisetsky, D.S.; Lipsky, P.E. New Insights into the Role of Antinuclear Antibodies in Systemic Lupus Erythematosus. Nat. Rev. Rheumatol. 2020, 16, 565–579. [Google Scholar] [CrossRef] [PubMed]
- Bost, C.; Arleevskaya, M.I.; Brooks, W.H.; Plaza, S.; Guery, J.-C.; Renaudineau, Y. Non-Coding RNA Xist Contribution in Systemic Lupus Erythematosus and Rheumatoid Arthritis. Clin. Immunol. 2022, 236, 108937. [Google Scholar] [CrossRef] [PubMed]
- Arbuckle, M.R.; McClain, M.T.; Rubertone, M.V.; Scofield, R.H.; Dennis, G.J.; James, J.A.; Harley, J.B. Development of Autoantibodies before the Clinical Onset of Systemic Lupus Erythematosus. N. Engl. J. Med. 2003, 349, 1526–1533. [Google Scholar] [CrossRef] [PubMed]
- Mackensen, A.; Müller, F.; Mougiakakos, D.; Böltz, S.; Wilhelm, A.; Aigner, M.; Völkl, S.; Simon, D.; Kleyer, A.; Munoz, L.; et al. Anti-CD19 CAR T Cell Therapy for Refractory Systemic Lupus Erythematosus. Nat. Med. 2022, 28, 2124–2132. [Google Scholar] [CrossRef]
- Seret, G.; Hanrotel, C.; Bendaoud, B.; Le Meur, Y.; Renaudineau, Y. Homozygous FCGR3A-158F Mutation Is Associated with Delayed B-Cell Depletion Following Rituximab but with Preserved Efficacy in a Patient with Refractory Lupus Nephritis. Clin. Kidney J. 2013, 6, 74–76. [Google Scholar] [CrossRef]
- Alexander, T.; Ostendorf, L.; Biesen, R.; Schneider, U.; Burmester, G.R.; Hiepe, F. Sustained Responses after Anti-CD38 Treatment with Daratumumab in Two Patients with Refractory Systemic Lupus Erythematosus. Ann. Rheum. Dis. 2023. Online ahead of print. [Google Scholar] [CrossRef]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. Ann. Rheum. Dis. 2019, 78, 1151–1159. [Google Scholar] [CrossRef]
- Wang, X.; Xia, Y. Anti-Double Stranded DNA Antibodies: Origin, Pathogenicity, and Targeted Therapies. Front. Immunol. 2019, 10, 1667. [Google Scholar] [CrossRef]
- Bardin, N.; Desplat-Jego, S.; Daniel, L.; Chiche, N.J.; Sanmarco, M. BioPlex 2200 Multiplexed System: Simultaneous Detection of Anti-DsDNA and Anti-Chromatin Antibodies in Patients with Systemic Lupus Erythematosus. Autoimmunity 2009, 42, 63–68. [Google Scholar] [CrossRef]
- Croquefer, S.; Guéguen, P.; Renaudineau, Y.; Jousse, S.; Renaudineau, É.; Bendaoud, B.; Hanrotel, C.; Devauchelle, V.; Youinou, P. Les anticorps anti-ADN ne sont plus ce qu’ils étaient!… L’apport des nouvelles techniques de dépistag e au diagnostic du lupus érythémateux disséminé. Rev. Francoph. Lab. 2006, 2006, 25–32. [Google Scholar] [CrossRef]
- Gladman, D.D.; Ibañez, D.; Urowitz, M.B. Systemic Lupus Erythematosus Disease Activity Index 2000. J. Rheumatol. 2002, 29, 288–291. [Google Scholar] [PubMed]
- Vanarsa, K.; Soomro, S.; Zhang, T.; Strachan, B.; Pedroza, C.; Nidhi, M.; Cicalese, P.; Gidley, C.; Dasari, S.; Mohan, S.; et al. Quantitative Planar Array Screen of 1000 Proteins Uncovers Novel Urinary Protein Biomarkers of Lupus Nephritis. Ann. Rheum. Dis. 2020, 79, 1349–1361. [Google Scholar] [CrossRef] [PubMed]
- Damoiseaux, J.; van Beers, J. Autoantibodies to DsDNA in the Diagnosis, Classification and Follow-up of Patients with Systemic Lupus Erythematosus. J. Transl. Autoimmun. 2023, 6, 100191. [Google Scholar] [CrossRef]
- Lemerle, J.; Brooks, W.H.; Renaudineau, Y. Anti-DNA and Anti-Nucleosome Antibodies: An Update. Lupus Open Access 2017, 2, e105. [Google Scholar] [CrossRef]
- Migliorini, P.; Baldini, C.; Rocchi, V.; Bombardieri, S. Anti-Sm and Anti-RNP Antibodies. Autoimmunity 2005, 38, 47–54. [Google Scholar] [CrossRef]
- Liu, N.; Li, D.; Zhou, Y.; Zhang, X.; Liu, S.; Ma, R. Development and Validation of a Prognostic Nomogram for the Renal Relapse of Lupus Nephritis. Med. Clin. 2023. Online ahead of print. [Google Scholar] [CrossRef]
- Lemerle, J.; Renaudineau, Y. Anti-Sm and Anti-U1-RNP Antibodies: An Update. Lupus Open Access 2016, 1, e104. [Google Scholar] [CrossRef]
- Mostoslavsky, G.; Fischel, R.; Yachimovich, N.; Yarkoni, Y.; Rosenmann, E.; Monestier, M.; Baniyash, M.; Eilat, D. Lupus Anti-DNA Autoantibodies Cross-React with a Glomerular Structural Protein: A Case for Tissue Injury by Molecular Mimicry. Eur. J. Immunol. 2001, 31, 1221–1227. [Google Scholar] [CrossRef]
- Deocharan, B.; Qing, X.; Lichauco, J.; Putterman, C. Alpha-Actinin Is a Cross-Reactive Renal Target for Pathogenic Anti-DNA Antibodies. J. Immunol. 2002, 168, 3072–3078. [Google Scholar] [CrossRef]
- Renaudineau, Y.; Croquefer, S.; Jousse, S.; Renaudineau, E.; Devauchelle, V.; Guéguen, P.; Hanrotel, C.; Gilburd, B.; Saraux, A.; Shoenfeld, Y.; et al. Association of Alpha-Actinin-Binding Anti-Double-Stranded DNA Antibodies with Lupus Nephritis. Arthritis Rheumatol. 2006, 54, 2523–2532. [Google Scholar] [CrossRef] [PubMed]
- Hanrotel-Saliou, C.; Segalen, I.; Le Meur, Y.; Youinou, P.; Renaudineau, Y. Glomerular Antibodies in Lupus Nephritis. Clin. Rev. Allergy Immunol. 2011, 40, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Seret, G.; Cañas, F.; Di Costanzo, L.P.; Hanrotel-Saliou, C.; Jousse-Joulin, S.; Le Meur, Y.; Saraux, A.; Valeri, A.; Putterman, C.; Youinou, P.; et al. Anti-Alpha-Actinin Antibodies Are Part of the Anti-Cell Membrane Antibody Spectrum That Characterize Patients with Lupus Nephritis. J. Autoimmun. 2015, 61, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Croquefer, S.; Renaudineau, Y.; Jousse, S.; Gueguen, P.; Ansart, S.; Saraux, A.; Youinou, P. The anti-Alpha-Actinin Test Completes anti-DNA Determination in Systemic Lupus Erythematosus. Ann. N. Y. Acad. Sci. 2005, 1050, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Lambrianides, A.; Giles, I.; Ioannou, Y.; Mason, L.; Latchman, D.S.; Manson, J.J.; Isenberg, D.A.; Rahman, A. Arginine Mutation Alters Binding of a Human Monoclonal Antibody to Antigens Linked to Systemic Lupus Erythematosus and the Antiphospholipid Syndrome. Arthritis Rheumatol. 2007, 56, 2392–2401. [Google Scholar] [CrossRef]
- Li, Q.-Z.; Xie, C.; Wu, T.; Mackay, M.; Aranow, C.; Putterman, C.; Mohan, C. Identification of Autoantibody Clusters That Best Predict Lupus Disease Activity Using Glomerular Proteome Arrays. J. Clin. Investig. 2005, 115, 3428–3439. [Google Scholar] [CrossRef]
- Becker-Merok, A.; Kalaaji, M.; Haugbro, K.; Nikolaisen, C.; Nilsen, K.; Rekvig, O.P.; Nossent, J.C. Alpha-Actinin-Binding Antibodies in Relation to Systemic Lupus Erythematosus and Lupus Nephritis. Arthritis Res. Ther. 2006, 8, R162. [Google Scholar] [CrossRef]
- Manson, J.J.; Ma, A.; Rogers, P.; Mason, L.J.; Berden, J.H.; van der Vlag, J.; D’Cruz, D.P.; Isenberg, D.A.; Rahman, A. Relationship between Anti-DsDNA, Anti-Nucleosome and Anti-Alpha-Actinin Antibodies and Markers of Renal Disease in Patients with Lupus Nephritis: A Prospective Longitudinal Study. Arthritis Res. Ther. 2009, 11, R154. [Google Scholar] [CrossRef]
- Marziale, A.; Bettacchioli, E.; Picart, G.; Nafai, S.; Galinat, H.; Meroni, P.L.; Frostegard, J.; PRECISESADS Clinical Consortium; Alarcon-Riquelme, M.E.; Renaudineau, Y. Antiphospholipid Autoantibody Detection Is Important in All Patients with Systemic Autoimmune Diseases. J. Autoimmun. 2020, 115, 102524. [Google Scholar] [CrossRef]
- Gerhardsson, J.; Sundelin, B.; Zickert, A.; Padyukov, L.; Svenungsson, E.; Gunnarsson, I. Histological Antiphospholipid-Associated Nephropathy versus Lupus Nephritis in Patients with Systemic Lupus Erythematosus: An Observational Cross-Sectional Study with Longitudinal Follow-Up. Arthritis Res. Ther. 2015, 17, 109. [Google Scholar] [CrossRef]
- Hernandez-Molina, G.; García-Trejo, L.P.; Uribe, N.; Cabral, A.R. Thrombotic Microangiopathy and Poor Renal Outcome in Lupus Patients with or without Antiphospholipid Syndrome. Clin. Exp. Rheumatol. 2015, 33, 503–508. [Google Scholar] [PubMed]
- Rousselin, C.; Amoura, Z.; Faguer, S.; Bataille, P.; Boffa, J.-J.; Canaud, G.; Guerrot, D.; Noémie Jourde-Chiche for the GCLR; Karras, A.; Auxenfants, E.; et al. Renal and Vascular Outcomes in Patients with Isolated Antiphospholipid Syndrome Nephropathy. J. Autoimmun. 2022, 132, 102889. [Google Scholar] [CrossRef] [PubMed]
- Domingues, V.; Chock, E.Y.; Dufrost, V.; Risse, J.; Seshan, S.V.; Barbhaiya, M.; Sartelet, H.; Erkan, D.; Wahl, D.; Zuily, S. Increased Risk of Acute and Chronic Microvascular Renal Lesions Associated with Antiphospholipid Antibodies in Patients with Systemic Lupus Erythematosus: A Systematic Review and Meta-Analysis. Autoimmun. Rev. 2022, 21, 103158. [Google Scholar] [CrossRef]
- Tsai, C.-Y.; Li, K.-J.; Shen, C.-Y.; Lu, C.-H.; Lee, H.-T.; Wu, T.-H.; Ng, Y.-Y.; Tsao, Y.-P.; Hsieh, S.-C.; Yu, C.-L. Decipher the Immunopathological Mechanisms and Set Up Potential Therapeutic Strategies for Patients with Lupus Nephritis. Int. J. Mol. Sci. 2023, 24, 10066. [Google Scholar] [CrossRef] [PubMed]
- Seret, G.; Le Meur, Y.; Renaudineau, Y.; Youinou, P. Mesangial Cell-Specific Antibodies Are Central to the Pathogenesis of Lupus Nephritis. Clin. Dev. Immunol. 2012, 2012, 579670. [Google Scholar] [CrossRef]
- Sakhi, H.; Moktefi, A.; Bouachi, K.; Audard, V.; Hénique, C.; Remy, P.; Ollero, M.; El Karoui, K. Podocyte Injury in Lupus Nephritis. J. Clin. Med. 2019, 8, 1340. [Google Scholar] [CrossRef]
- Jamaly, S.; Rakaee, M.; Abdi, R.; Tsokos, G.C.; Fenton, K.A. Interplay of Immune and Kidney Resident Cells in the Formation of Tertiary Lymphoid Structures in Lupus Nephritis. Autoimmun. Rev. 2021, 20, 102980. [Google Scholar] [CrossRef]
- Tao, J.; Zhao, J.; Qi, X.-M.; Wu, Y.-G. Complement-Mediated M2/M1 Macrophage Polarization May Be Involved in Crescent Formation in Lupus Nephritis. Int. Immunopharmacol. 2021, 101 Pt A, 108278. [Google Scholar] [CrossRef]
- Li, J.; Liu, C.-H.; Xu, D.-L.; Gao, B. Significance of CD163-Positive Macrophages in Proliferative Glomerulonephritis. Am. J. Med. Sci. 2015, 350, 387–392. [Google Scholar] [CrossRef]
- Endo, N.; Tsuboi, N.; Furuhashi, K.; Shi, Y.; Du, Q.; Abe, T.; Hori, M.; Imaizumi, T.; Kim, H.; Katsuno, T.; et al. Urinary Soluble CD163 Level Reflects Glomerular Inflammation in Human Lupus Nephritis. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2016, 31, 2023–2033. [Google Scholar] [CrossRef]
- Zhang, T.; Li, H.; Vanarsa, K.; Gidley, G.; Mok, C.C.; Petri, M.; Saxena, R.; Mohan, C. Association of Urine SCD163 With Proliferative Lupus Nephritis, Fibrinoid Necrosis, Cellular Crescents and Intrarenal M2 Macrophages. Front. Immunol. 2020, 11, 671. [Google Scholar] [CrossRef] [PubMed]
- Palazzo, L.; Lindblom, J.; Mohan, C.; Parodis, I. Current Insights on Biomarkers in Lupus Nephritis: A Systematic Review of the Literature. J. Clin. Med. 2022, 11, 5759. [Google Scholar] [CrossRef] [PubMed]
- Leung, Y.Y.; Szeto, C.C.; Tam, L.S.; Lam, C.W.K.; Li, E.K.; Wong, K.C.; Yu, S.W.; Kun, E.W. Urine Protein-to-Creatinine Ratio in an Untimed Urine Collection Is a Reliable Measure of Proteinuria in Lupus Nephritis. Rheumatology 2007, 46, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Morell, M.; Pérez-Cózar, F.; Marañón, C. Immune-Related Urine Biomarkers for the Diagnosis of Lupus Nephritis. Int. J. Mol. Sci. 2021, 22, 7143. [Google Scholar] [CrossRef]
- Gutiérrez-Peredo, G.B.; Montaño-Castellón, I.; Gutiérrez-Peredo, A.J.; Juan, P.; Ticona, A.; Montaño-Castellón, F.; Oliveira Filho, J.C.B.; Pinto Almeida, A.R. Comparison of Urinary Protein/Creatinine Ratio as an Alternative to 24-Hour Proteinuria in Lupus Nephritis: TUNARI Study. Nephron 2023, 6, 1–7. [Google Scholar] [CrossRef]
- Medina-Rosas, J.; Yap, K.S.; Anderson, M.; Su, J.; Touma, Z. Utility of Urinary Protein-Creatinine Ratio and Protein Content in a 24-Hour Urine Collection in Systemic Lupus Erythematosus: A Systematic Review and Meta-Analysis. Arthritis Care Res. 2016, 68, 1310–1319. [Google Scholar] [CrossRef]
- Rovin, B.H.; Adler, S.G.; Barratt, J.; Bridoux, F.; Burdge, K.A.; Chan, T.M.; Cook, H.T.; Fervenza, F.C.; Gibson, K.L.; Glassock, R.J.; et al. Executive Summary of the KDIGO 2021 Guideline for the Management of Glomerular Diseases. Kidney Int. 2021, 100, 753–779. [Google Scholar] [CrossRef]
- Banos, A.; Bertsias, G. Flares in Lupus Nephritis: Risk Factors and Strategies for Their Prevention. Curr. Rheumatol. Rep. 2023, 25, 183–191. [Google Scholar] [CrossRef]
- Kapsia, E.; Marinaki, S.; Michelakis, I.; Liapis, G.; Sfikakis, P.P.; Boletis, J.; Tektonidou, M.G. Predictors of Early Response, Flares, and Long-Term Adverse Renal Outcomes in Proliferative Lupus Nephritis: A 100-Month Median Follow-Up of an Inception Cohort. J. Clin. Med. 2022, 11, 5017. [Google Scholar] [CrossRef]
- Ahmed, H.E.; Hassan, S.A.E.-M.; Teama, M.A.M.; Badr, F.M. Serum Uric Acid as a Predictor for Nephritis in Egyptian Patients with Systemic Lupus Erythematosus. Lupus 2021, 30, 378–384. [Google Scholar] [CrossRef]
- Han, Y.; Lu, X.; Xiao, S.; Qin, J.; Zheng, L.; Feng, Y.; Cai, Y.; Qiu, R.; Huang, Q.; Yang, M. Association between Serum Uric Acid Level and Systemic Lupus Erythematosus Kidney Outcome: An Observational Study in Southern Chinese Population and a Meta-Analysis. Lupus 2023, 32, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Faustini, F.; Idborg, H.; Fuzzi, E.; Larsson, A.; Lie, W.-R.; Pötzsch, S.; Okitsu, S.L.; Svenungsson, E.; Gunnarsson, I. Urine Galectin-3 Binding Protein Reflects Nephritis Activity in Systemic Lupus Erythematosus. Lupus 2023, 32, 252–262. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.; Shen, Y.; Lin, C.; Qin, L.; He, S.; Dai, M.; Okitsu, S.L.; DeMartino, J.A.; Guo, Q.; Shen, N. Urinary Galectin-3 Binding Protein (G3BP) as a Biomarker for Disease Activity and Renal Pathology Characteristics in Lupus Nephritis. Arthritis Res. Ther. 2022, 24, 77. [Google Scholar] [CrossRef]
- Zhang, T.; Duran, V.; Vanarsa, K.; Mohan, C. Targeted Urine Proteomics in Lupus Nephritis—A Meta-Analysis. Expert Rev. Proteom. 2020, 17, 767–776. [Google Scholar] [CrossRef] [PubMed]
- Mohan, C.; Zhang, T.; Putterman, C. Pathogenic Cellular and Molecular Mediators in Lupus Nephritis. Nat. Rev. Nephrol. 2023, 19, 491–508. [Google Scholar] [CrossRef]
- Guimarães, J.D.A.R.; da Conceição Furtado, S.; Lucas, A.C.D.S.; Mori, B.; Barcellos, J.F.M. Diagnostic Test Accuracy of Novel Biomarkers for Lupus Nephritis-An Overview of Systematic Reviews. PLoS ONE 2022, 17, e0275016. [Google Scholar] [CrossRef]
- Phatak, S.; Chaurasia, S.; Mishra, S.K.; Gupta, R.; Agrawal, V.; Aggarwal, A.; Misra, R. Urinary B Cell Activating Factor (BAFF) and a Proliferation-Inducing Ligand (APRIL): Potential Biomarkers of Active Lupus Nephritis. Clin. Exp. Immunol. 2017, 187, 376–382. [Google Scholar] [CrossRef]
- Whittall-Garcia, L.; Goliad, K.; Kim, M.; Bonilla, D.; Gladman, D.; Urowitz, M.; Fortin, P.R.; Atenafu, E.G.; Touma, Z.; Wither, J. Identification and Validation of a Urinary Biomarker Panel to Accurately Diagnose and Predict Response to Therapy in Lupus Nephritis. Front. Immunol. 2022, 13, 889931. [Google Scholar] [CrossRef]
- Pérez-Arias, A.A.; Méndez-Pérez, R.A.; Cruz, C.; Zavala-Miranda, M.F.; Romero-Diaz, J.; Márquez-Macedo, S.E.; Comunidad-Bonilla, R.A.; García-Rueda, C.C.; Mejía-Vilet, J.M. The First-Year Course of Urine MCP-1 and Its Association with Response to Treatment and Long-Term Kidney Prognosis in Lupus Nephritis. Clin. Rheumatol. 2023, 42, 83–92. [Google Scholar] [CrossRef]
- Moran, S.M.; Scott, J.; Clarkson, M.R.; Conlon, N.; Dunne, J.; Griffin, M.D.; Griffin, T.P.; Groarke, E.; Holian, J.; Judge, C.; et al. The Clinical Application of Urine Soluble CD163 in ANCA-Associated Vasculitis. J. Am. Soc. Nephrol. JASN 2021, 32, 2920–2932. [Google Scholar] [CrossRef]
- Soliman, S.A.; Stanley, S.; Vanarsa, K.; Ismail, F.; Chiu Mok, C.; Mohan, C. Exploring Urine: Serum Fractional Excretion Ratios as Potential Biomarkers for Lupus Nephritis. Front. Immunol. 2022, 13, 910993. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Yadav, A.; Aggarwal, A. Urinary Soluble CD163 Is a Good Biomarker for Renal Disease Activity in Lupus Nephritis. Clin. Rheumatol. 2021, 40, 941–948. [Google Scholar] [CrossRef]
- Lei, R.; Vu, B.; Kourentzi, K.; Soomro, S.; Danthanarayana, A.N.; Brgoch, J.; Nadimpalli, S.; Petri, M.; Mohan, C.; Willson, R.C. A Novel Technology for Home Monitoring of Lupus Nephritis That Tracks the Pathogenic Urine Biomarker ALCAM. Front. Immunol. 2022, 13, 1044743. [Google Scholar] [CrossRef] [PubMed]
- Gasparin, A.A.; Bueno de Andrade, N.P.; Hax, V.; Palominos, P.E.; Siebert, M.; Marx, R.; Guilherme Schaefer, P.; Veronese, F.V.; Monticielo, O.A. Urinary Soluble VCAM-1 Is a Useful Biomarker of Disease Activity and Treatment Response in Lupus Nephritis. BMC Rheumatol. 2020, 4, 67. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.Y.C.; Yung, S.; Km Chau, M.; So Tang, C.; Yh Yap, D.; Hn Tang, A.; Ky Ying, S.; Kwong Lee, C.; Chan, T.M. Clinico-Pathological Associations of Serum VCAM-1 and ICAM-1 Levels in Patients with Lupus Nephritis. Lupus 2021, 30, 1039–1050. [Google Scholar] [CrossRef]
- Yang, G.; Guo, N.; Yin, J.; Wu, J. Elevated Soluble CD163 Predicts Renal Function Deterioration in Lupus Nephritis: A Cohort Study in Eastern China. J. Int. Med. Res. 2021, 49, 3000605211049963. [Google Scholar] [CrossRef]
- Roointan, A.; Gholaminejad, A.; Shojaie, B.; Hudkins, K.L.; Gheisari, Y. Candidate MicroRNA Biomarkers in Lupus Nephritis: A Meta-Analysis of Profiling Studies in Kidney, Blood and Urine Samples. Mol. Diagn. Ther. 2023, 27, 141–158. [Google Scholar] [CrossRef]
- Perez-Hernandez, J.; Martinez-Arroyo, O.; Ortega, A.; Galera, M.; Solis-Salguero, M.A.; Chaves, F.J.; Redon, J.; Forner, M.J.; Cortes, R. Urinary Exosomal MiR-146a as a Marker of Albuminuria, Activity Changes and Disease Flares in Lupus Nephritis. J. Nephrol. 2021, 34, 1157–1167. [Google Scholar] [CrossRef]
- Garcia-Vives, E.; Solé, C.; Moliné, T.; Vidal, M.; Agraz, I.; Ordi-Ros, J.; Cortés-Hernández, J. The Urinary Exosomal MiRNA Expression Profile Is Predictive of Clinical Response in Lupus Nephritis. Int. J. Mol. Sci. 2020, 21, 1372. [Google Scholar] [CrossRef]
- Roccatello, D.; Fenoglio, R.; Caniggia, I.; Kamgaing, J.; Naretto, C.; Cecchi, I.; Rubini, E.; Rossi, D.; De Simone, E.; Del Vecchio, G.; et al. Daratumumab Monotherapy for Refractory Lupus Nephritis. Nat. Med. 2023, 29, 2041–2047. [Google Scholar] [CrossRef]
- Hasni, S.A.; Gupta, S.; Davis, M.; Poncio, E.; Temesgen-Oyelakin, Y.; Carlucci, P.M.; Wang, X.; Naqi, M.; Playford, M.P.; Goel, R.R.; et al. Phase 1 Double-Blind Randomized Safety Trial of the Janus Kinase Inhibitor Tofacitinib in Systemic Lupus Erythematosus. Nat. Commun. 2021, 12, 3391. [Google Scholar] [CrossRef] [PubMed]
- Arriens, C.; Onno Teng, Y.K.; Ginzler, E.M.; Parikh, S.V.; Askanase, A.D.; Saxena, A.; Gibson, K.; Caster, D.J.; Atsumi, T.; Lisk, L.; et al. Update on the Efficacy and Safety Profile of Voclosporin: An Integrated Analysis of Clinical Trials in Lupus Nephritis. Arthritis Care Res. 2023, 75, 1399–1408. [Google Scholar] [CrossRef] [PubMed]
- Jayne, D.; Rovin, B.; Mysler, E.F.; Furie, R.A.; Houssiau, F.A.; Trasieva, T.; Knagenhjelm, J.; Schwetje, E.; Chia, Y.L.; Tummala, R.; et al. Phase II Randomised Trial of Type I Interferon Inhibitor Anifrolumab in Patients with Active Lupus Nephritis. Ann. Rheum. Dis. 2022, 81, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Dooley, M.A.; Houssiau, F.; Aranow, C.; D’Cruz, D.P.; Askanase, A.; Roth, D.A.; Zhong, Z.J.; Cooper, S.; Freimuth, W.W.; Ginzler, E.M.; et al. Effect of Belimumab Treatment on Renal Outcomes: Results from the Phase 3 Belimumab Clinical Trials in Patients with SLE. Lupus 2013, 22, 63–72. [Google Scholar] [CrossRef]
- Dörner, T.; Tanaka, Y.; Petri, M.A.; Smolen, J.S.; Wallace, D.J.; Dow, E.R.; Higgs, R.E.; Rocha, G.; Crowe, B.; Benschop, R.J.; et al. Baricitinib-Associated Changes in Global Gene Expression during a 24-Week Phase II Clinical Systemic Lupus Erythematosus Trial Implicates a Mechanism of Action through Multiple Immune-Related Pathways. Lupus Sci. Med. 2020, 7, e000424. [Google Scholar] [CrossRef]
- Wilkinson, C.; Henderson, R.B.; Jones-Leone, A.R.; Flint, S.M.; Lennon, M.; Levy, R.A.; Ji, B.; Bass, D.L.; Roth, D. The Role of Baseline BLyS Levels and Type 1 Interferon-Inducible Gene Signature Status in Determining Belimumab Response in Systemic Lupus Erythematosus: A Post Hoc Meta-Analysis. Arthritis Res. Ther. 2020, 22, 102. [Google Scholar] [CrossRef]
- Weeding, E.; Fava, A.; Mohan, C.; Magder, L.; Goldman, D.; Petri, M. Urine Proteomic Insights from the Belimumab in Lupus Nephritis Trial. Lupus Sci. Med. 2022, 9, e000763. [Google Scholar] [CrossRef]
- Furie, R.A.; Aroca, G.; Cascino, M.D.; Garg, J.P.; Rovin, B.H.; Alvarez, A.; Fragoso-Loyo, H.; Zuta-Santillan, E.; Schindler, T.; Brunetta, P.; et al. B-Cell Depletion with Obinutuzumab for the Treatment of Proliferative Lupus Nephritis: A Randomised, Double-Blind, Placebo-Controlled Trial. Ann. Rheum. Dis. 2022, 81, 100–107. [Google Scholar] [CrossRef]
- Rovin, B.H.; Furie, R.; Latinis, K.; Looney, R.J.; Fervenza, F.C.; Sanchez-Guerrero, J.; Maciuca, R.; Zhang, D.; Garg, J.P.; Brunetta, P.; et al. Efficacy and Safety of Rituximab in Patients with Active Proliferative Lupus Nephritis: The Lupus Nephritis Assessment with Rituximab Study. Arthritis Rheumatol. 2012, 64, 1215–1226. [Google Scholar] [CrossRef]
- Masoud, S.; McAdoo, S.P.; Bedi, R.; Cairns, T.D.; Lightstone, L. Ofatumumab for B Cell Depletion in Patients with Systemic Lupus Erythematosus Who Are Allergic to Rituximab. Rheumatology 2018, 57, 1156–1161. [Google Scholar] [CrossRef]
- Atisha-Fregoso, Y.; Malkiel, S.; Harris, K.M.; Byron, M.; Ding, L.; Kanaparthi, S.; Barry, W.T.; Gao, W.; Ryker, K.; Tosta, P.; et al. Phase II Randomized Trial of Rituximab Plus Cyclophosphamide Followed by Belimumab for the Treatment of Lupus Nephritis. Arthritis Rheumatol. 2021, 73, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Ostendorf, L.; Burns, M.; Durek, P.; Anne Heinz, G.; Heinrich, F.; Garantziotis, P.; Enghard, P.; Richter, U.; Biesen, R.; Schneider, U.; et al. Targeting CD38 with Daratumumab in Refractory Systemic Lupus Erythematosus. N. Engl. J. Med. 2020, 383, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- Mougiakakos, D.; Krönke, G.; Völkl, S.; Kretschmann, S.; Aigner, M.; Kharboutli, S.; Böltz, S.; Manger, B.; Mackensen, A.; Schett, G. CD19-Targeted CAR T Cells in Refractory Systemic Lupus Erythematosus. N. Engl. J. Med. 2021, 385, 567–569. [Google Scholar] [CrossRef] [PubMed]
- Dooley, M.A.; Cosio, F.G.; Nachman, P.H.; Falkenhain, M.E.; Hogan, S.L.; Falk, R.J.; Hebert, L.A. Mycophenolate Mofetil Therapy in Lupus Nephritis: Clinical Observations. J. Am. Soc. Nephrol. JASN 1999, 10, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Grootscholten, C.; Dieker, J.W.C.; McGrath, F.D.; Roos, A.; Derksen, R.H.W.M.; van der Vlag, J.; Daha, M.R.; Berden, J.H.M. A Prospective Study of Anti-Chromatin and Anti-C1q Autoantibodies in Patients with Proliferative Lupus Nephritis Treated with Cyclophosphamide Pulses or Azathioprine/Methylprednisolone. Ann. Rheum. Dis. 2007, 66, 693–696. [Google Scholar] [CrossRef]
- Shigesaka, M.; Ito, T.; Inaba, M.; Imai, K.; Yamanaka, H.; Azuma, Y.; Tanaka, A.; Amuro, H.; Nishizawa, T.; Son, Y.; et al. Mycophenolic Acid, the Active Form of Mycophenolate Mofetil, Interferes with IRF7 Nuclear Translocation and Type I IFN Production by Plasmacytoid Dendritic Cells. Arthritis Res. Ther. 2020, 22, 264. [Google Scholar] [CrossRef]
- Dörner, T.; van Vollenhoven, R.F.; Doria, A.; Jia, B.; Terres, J.A.R.; Silk, M.E.; de Bono, S.; Fischer, P.; Wallace, D.J. Baricitinib Decreases Anti-DsDNA in Patients with Systemic Lupus Erythematosus: Results from a Phase II Double-Blind, Randomized, Placebo-Controlled Trial. Arthritis Res. Ther. 2022, 24, 112. [Google Scholar] [CrossRef]
- Furie, R.; Rovin, B.H.; Houssiau, F.; Malvar, A.; Onno Teng, Y.K.; Contreras, G.; Amoura, Z.; Yu, X.; Mok, C.C.; Santiago, M.B.; et al. Two-Year, Randomized, Controlled Trial of Belimumab in Lupus Nephritis. N. Engl. J. Med. 2020, 383, 1117–1128. [Google Scholar] [CrossRef]
- Stohl, W.; Hiepe, F.; Latinis, K.M.; Thomas, M.; Scheinberg, M.A.; Clarke, A.; Aranow, C.; Wellborne, F.R.; Abud-Mendoza, C.; Hough, D.R.; et al. Belimumab Reduces Autoantibodies, Normalizes Low Complement Levels, and Reduces Select B Cell Populations in Patients with Systemic Lupus Erythematosus. Arthritis Rheumatol. 2012, 64, 2328–2337. [Google Scholar] [CrossRef]
- Kraaij, T.; Arends, E.J.; van Dam, L.S.; Kamerling, S.W.A.; van Daele, P.L.A.; Bredewold, O.W.; Ray, A.; Bakker, J.A.; Scherer, H.U.; Huizinga, T.J.W.; et al. Long-Term Effects of Combined B-Cell Immunomodulation with Rituximab and Belimumab in Severe, Refractory Systemic Lupus Erythematosus: 2-Year Results. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc.-Eur. Ren. Assoc. 2021, 36, 1474–1483. [Google Scholar] [CrossRef]
- Van Dam, L.S.; Osmani, Z.; Kamerling, S.W.A.; Kraaij, T.; Bakker, J.A.; Scherer, H.U.; Rabelink, T.J.; Voll, R.E.; Alexander, T.; Isenberg, D.A.; et al. A Reverse Translational Study on the Effect of Rituximab, Rituximab plus Belimumab, or Bortezomib on the Humoral Autoimmune Response in SLE. Rheumatology 2020, 59, 2734–2745. [Google Scholar] [CrossRef] [PubMed]
- Alves, P.; Bandaria, J.; Leavy, M.B.; Gliklich, B.; Boussios, C.; Su, Z.; Curhan, G. Validation of a machine learning approach to estimate Systemic Lupus Erythematosus Disease Activity Index score categories and application in a real-world dataset. RMD Open 2021, 7, e001586. [Google Scholar] [CrossRef] [PubMed]


| Biomarker | Predict LN | Disease Activity | Therapeutic Response | Predict Flares | Predict ESKD |
|---|---|---|---|---|---|
| Anti-DNASE1L3 Abs, DNase activity | Yes | Yes | Responder | Unknown | Unknown |
| Anti-C1q Abs | Proliferative LN | Low | No | Mild | Unknown |
| Serum C3/C4/CH50 | No | Consumption | Responder | Consumption | No |
| IFN signature (I ± II); IFN-alpha | Elevated levels | Elevated levels | Responder | Elevated levels | Elevated levels |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Renaudineau, Y.; Brooks, W.; Belliere, J. Lupus Nephritis Risk Factors and Biomarkers: An Update. Int. J. Mol. Sci. 2023, 24, 14526. https://doi.org/10.3390/ijms241914526
Renaudineau Y, Brooks W, Belliere J. Lupus Nephritis Risk Factors and Biomarkers: An Update. International Journal of Molecular Sciences. 2023; 24(19):14526. https://doi.org/10.3390/ijms241914526
Chicago/Turabian StyleRenaudineau, Yves, Wesley Brooks, and Julie Belliere. 2023. "Lupus Nephritis Risk Factors and Biomarkers: An Update" International Journal of Molecular Sciences 24, no. 19: 14526. https://doi.org/10.3390/ijms241914526