

Prognostic Significance of Activated Monocytes in Patients with ST-Elevation Myocardial Infarction

Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
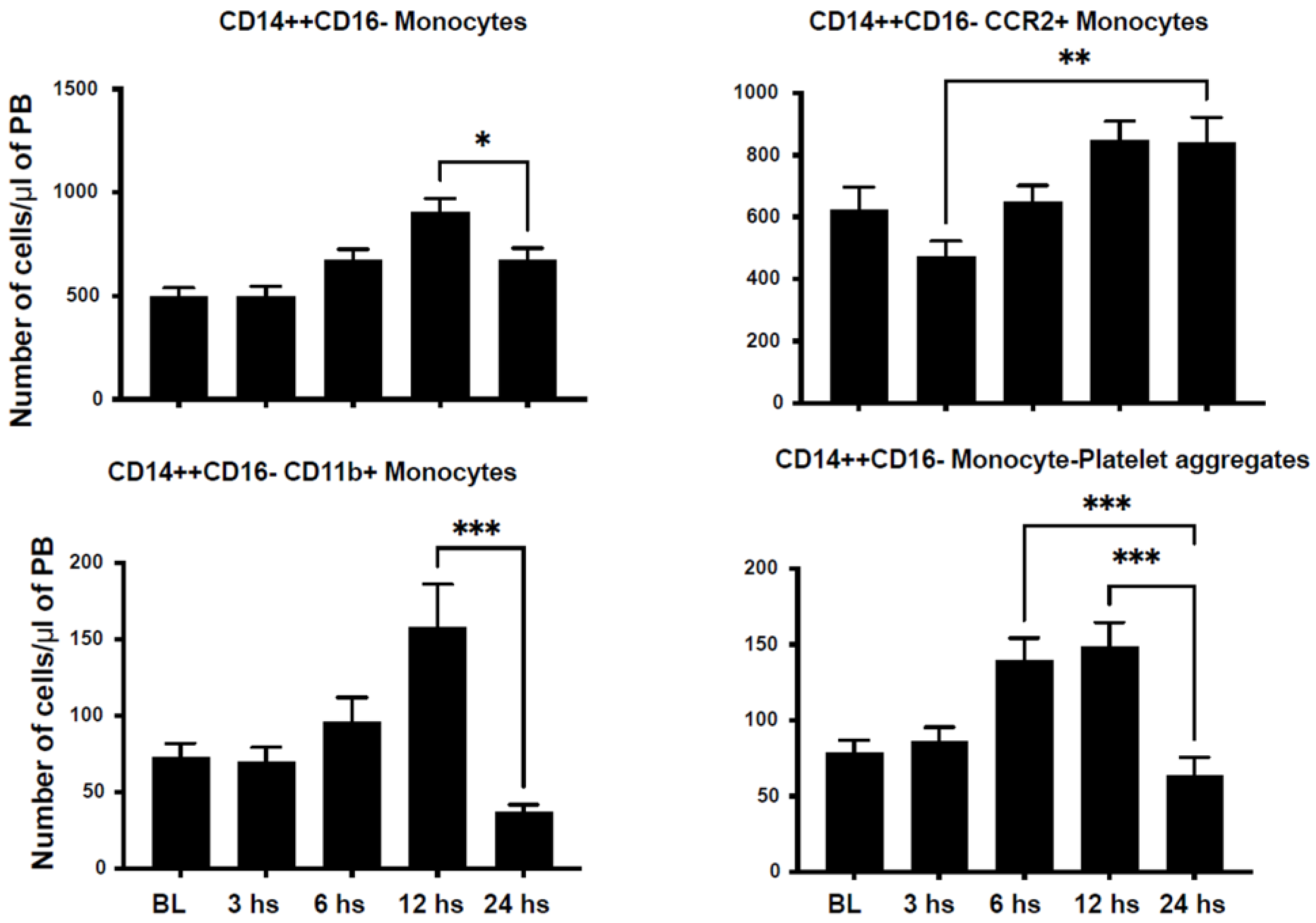
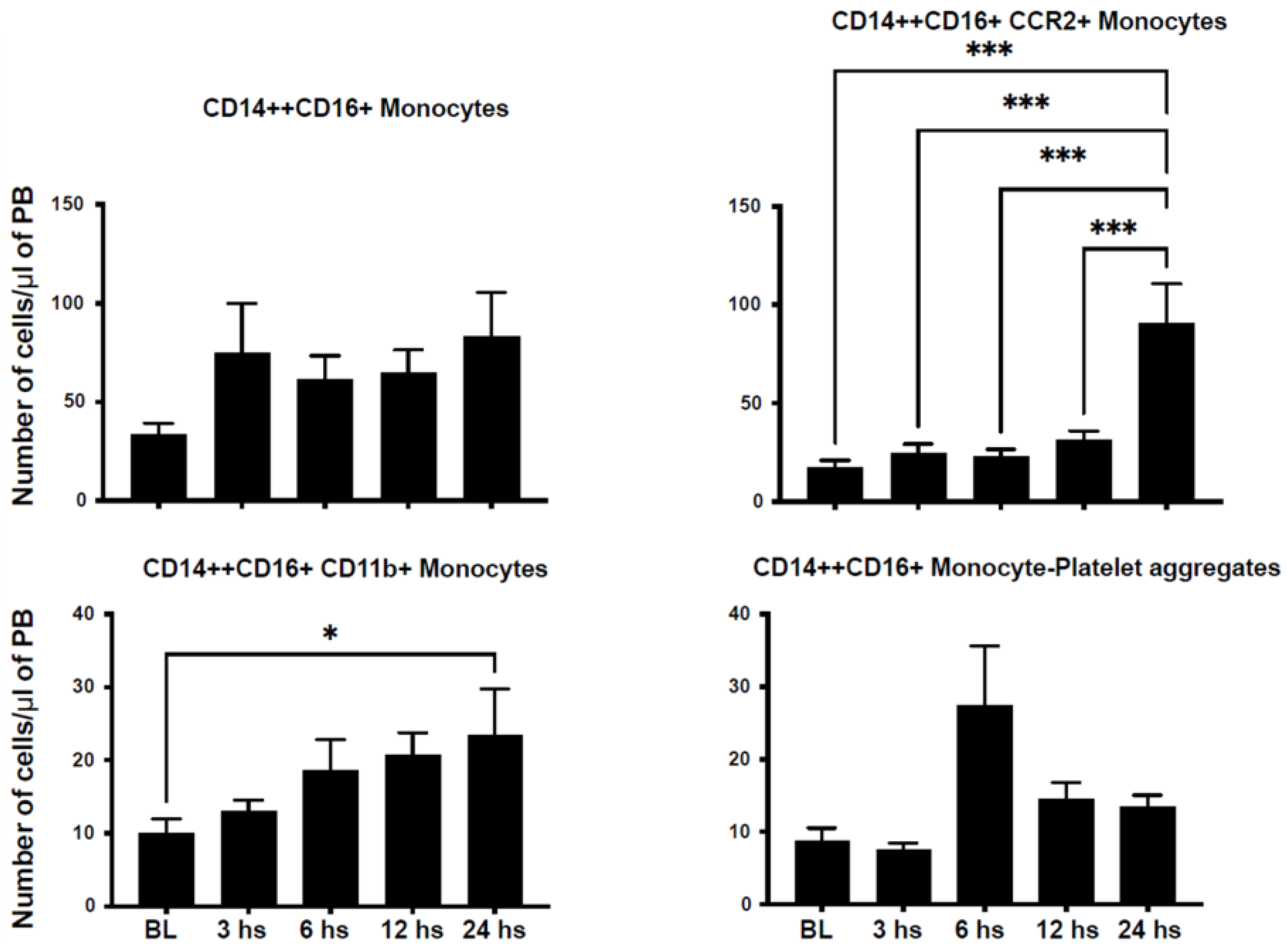
2.2. Mobilization of Inflammatory Cells
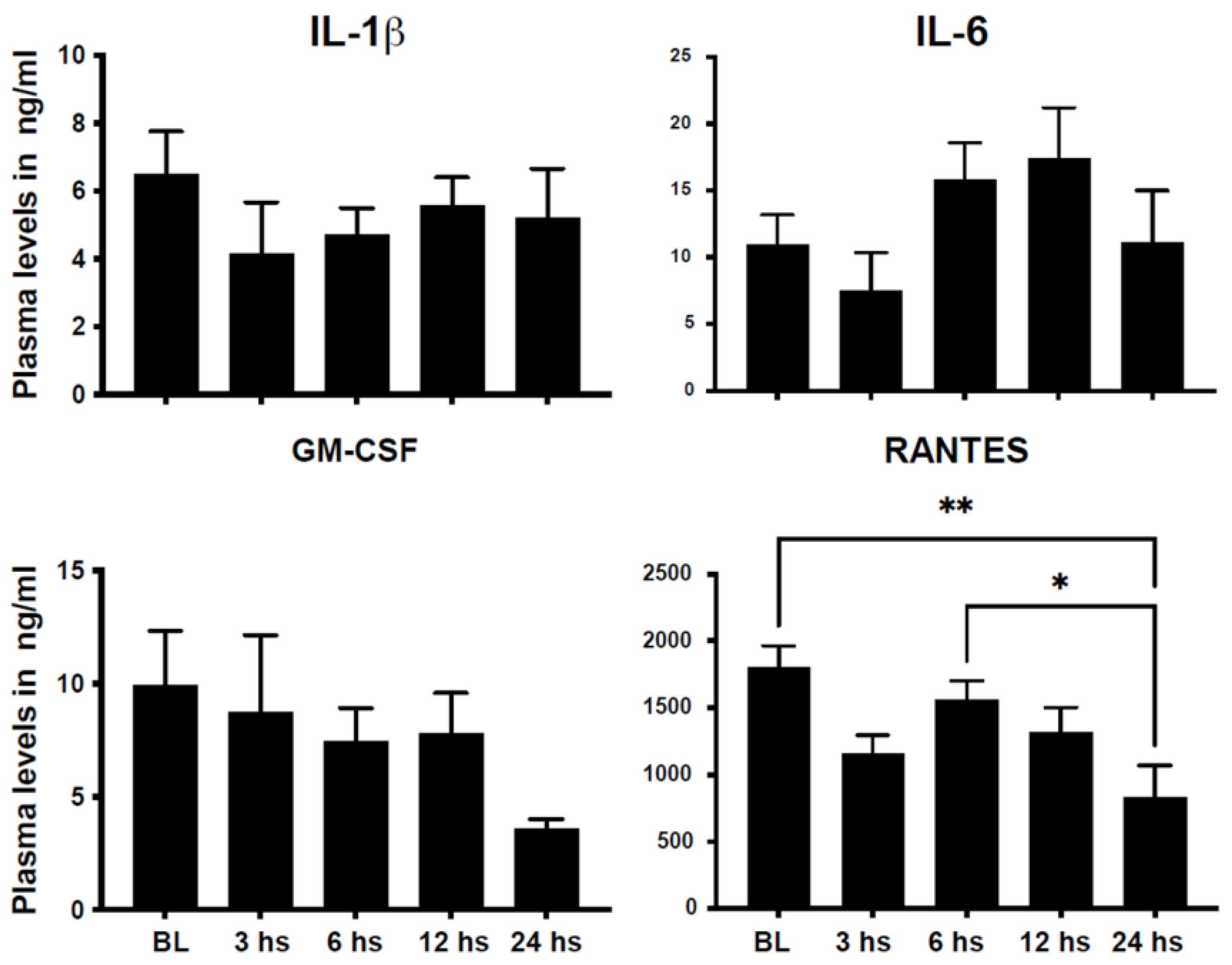
2.3. Changes in Plasma Cytokines after STEMI in Humans
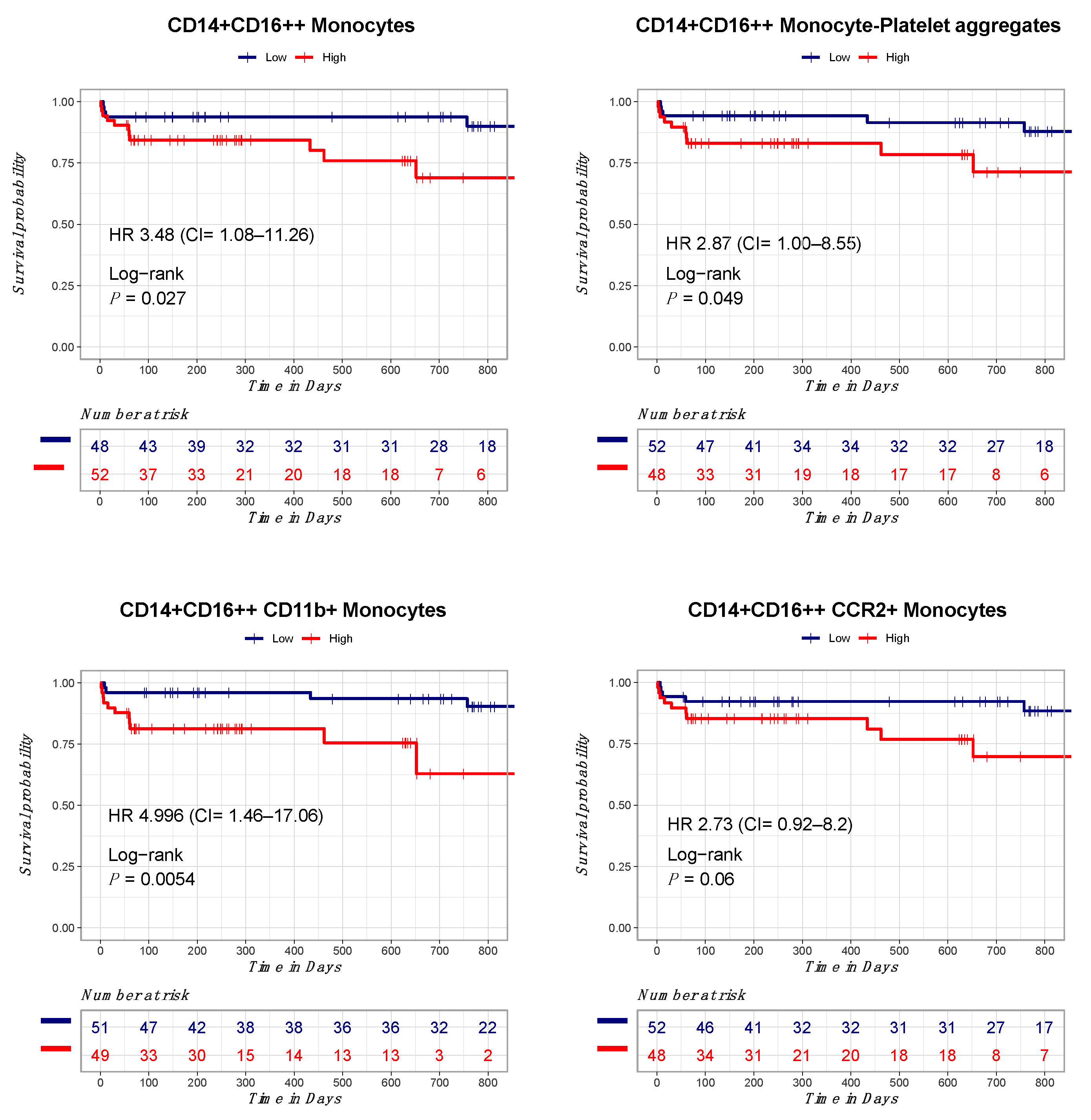
2.4. Correlation between Circulating Monocytes and Clinical Outcomes
3. Discussion
4. Materials and Methods
4.1. Patient Enrollment
4.2. Flow Cytometry
4.3. Luminex Assay
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thom, T.; Haase, N.; Rosamond, W.; Howard, V.J.; Rumsfeld, J.; Manolio, T.; Zheng, Z.J.; Flegal, K.; O’Donnell, C.; Kittner, S.; et al. Heart disease and stroke statistics–2006 update: A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2006, 113, e85–e151. [Google Scholar] [PubMed] [Green Version]
- Peterson, E.D.; Roe, M.T.; Chen, A.Y.; Fonarow, G.C.; Lytle, B.L.; Cannon, C.P.; Rumsfeld, J.S. The NCDR ACTION Registry-GWTG: Transforming contemporary acute myocardial infarction clinical care. Heart 2010, 96, 1798–1802. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Choi, K.H.; Lee, J.M.; Kim, H.K.; Hwang, D.; Rhee, T.M.; Kim, J.; Park, T.K.; Yang, J.H.; Song, Y.B.; et al. Prognostic Implications of Door-to-Balloon Time and Onset-to-Door Time on Mortality in Patients with ST -Segment-Elevation Myocardial Infarction Treated with Primary Percutaneous Coronary Intervention. J. Am. Heart Assoc. 2019, 8, e012188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchis-Gomar, F.; Perez-Quilis, C.; Leischik, R.; Lucia, A. Epidemiology of coronary heart disease and acute coronary syndrome. Ann. Transl. Med. 2016, 4, 256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabay, C.; Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef]
- Buffon, A.; Biasucci, L.M.; Liuzzo, G.; D’Onofrio, G.; Crea, F.; Maseri, A. Widespread coronary inflammation in unstable angina. N. Engl. J. Med. 2002, 347, 5–12. [Google Scholar] [CrossRef]
- Tahir, S.; Steffens, S. Nonclassical monocytes in cardiovascular physiology and disease. Am. J. Physiol. Cell Physiol. 2021, 320, C761–C770. [Google Scholar] [CrossRef]
- Berg, K.E.; Ljungcrantz, I.; Andersson, L.; Bryngelsson, C.; Hedblad, B.; Fredrikson, G.N.; Nilsson, J.; Björkbacka, H. Elevated CD14++CD16− monocytes predict cardiovascular events. Circ. Cardiovasc. Genet. 2012, 5, 122–131. [Google Scholar] [CrossRef] [Green Version]
- Urra, X.; Villamor, N.; Amaro, S.; Gomez-Choco, M.; Obach, V.; Oleaga, L.; Planas, A.M.; Chamorro, A. Monocyte subtypes predict clinical course and prognosis in human stroke. J. Cereb. Blood Flow. Metab. 2009, 29, 994–1002. [Google Scholar] [CrossRef] [Green Version]
- Auffray, C.; Fogg, D.; Garfa, M.; Elain, G.; Join-Lambert, O.; Kayal, S.; Sarnacki, S.; Cumano, A.; Lauvau, G.; Geissmann, F. Monitoring of blood vessels and tissues by a population of monocytes with patrolling behavior. Science 2007, 317, 666–670. [Google Scholar] [CrossRef] [Green Version]
- Hamers, A.A.J.; Dinh, H.Q.; Thomas, G.D.; Marcovecchio, P.; Blatchley, A.; Nakao, C.S.; Kim, C.; McSkimming, C.; Taylor, A.M.; Nguyen, A.T.; et al. Human Monocyte Heterogeneity as Revealed by High-Dimensional Mass Cytometry. Arter. Thromb. Vasc. Biol. 2019, 39, 25–36. [Google Scholar] [CrossRef]
- Rossol, M.; Kraus, S.; Pierer, M.; Baerwald, C.; Wagner, U. The CD14(bright) CD16+ monocyte subset is expanded in rheumatoid arthritis and promotes expansion of the Th17 cell population. Arthritis Rheum. 2012, 64, 671–677. [Google Scholar] [CrossRef]
- Rogacev, K.S.; Cremers, B.; Zawada, A.M.; Seiler, S.; Binder, N.; Ege, P.; Grosse-Dunker, G.; Heisel, I.; Hornof, F.; Jeken, J.; et al. CD14++CD16+ monocytes independently predict cardiovascular events: A cohort study of 951 patients referred for elective coronary angiography. J. Am. Coll. Cardiol. 2012, 60, 1512–1520. [Google Scholar] [CrossRef] [Green Version]
- Azeredo, E.L.; Neves-Souza, P.C.; Alvarenga, A.R.; Reis, S.R.; Torrentes-Carvalho, A.; Zagne, S.M.; Nogueira, R.M.; Oliveira-Pinto, L.M.; Kubelka, C.F. Differential regulation of toll-like receptor-2, toll-like receptor-4, CD16 and human leucocyte antigen-DR on peripheral blood monocytes during mild and severe dengue fever. Immunology 2010, 130, 202–216. [Google Scholar] [CrossRef]
- Nagareddy, P.R.; Sreejit, G.; Abo-Aly, M.; Jaggers, R.M.; Chelvarajan, L.; Johnson, J.; Pernes, G.; Athmanathan, B.; Abdel-Latif, A.; Murphy, A.J. NETosis Is Required for S100A8/A9-Induced Granulopoiesis after Myocardial Infarction. Arter. Thromb. Vasc. Biol. 2020, 40, 2805–2807. [Google Scholar] [CrossRef]
- Sreejit, G.; Abdel-Latif, A.; Athmanathan, B.; Annabathula, R.; Dhyani, A.; Noothi, S.K.; Quaife-Ryan, G.A.; Al-Sharea, A.; Pernes, G.; Dragoljevic, D.; et al. Neutrophil-Derived S100A8/A9 Amplify Granulopoiesis after Myocardial Infarction. Circulation 2020, 141, 1080–1094. [Google Scholar] [CrossRef]
- Coelho-Lima, J.; Georgiopoulos, G.; Ahmed, J.; Adil, S.E.R.; Gaskin, D.; Bakogiannis, C.; Sopova, K.; Ahmed, F.; Ahmed, H.; Spray, L.; et al. Prognostic value of admission high-sensitivity troponin in patients with ST-elevation myocardial infarction. Heart 2021, 107, 1881–1888. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Rev. Esp. Cardiol. 2017, 70, 1082. [Google Scholar] [CrossRef]
- McLeod, P.; Adamson, P.D.; Coffey, S. Do we need early risk stratification after ST-elevation myocardial infarction? Heart 2021, 107, 1852–1853. [Google Scholar] [CrossRef]
- Tripathi, H.; Al-Darraji, A.; Abo-Aly, M.; Peng, H.; Shokri, E.; Chelvarajan, L.; Donahue, R.R.; Levitan, B.M.; Gao, E.; Hernandez, G.; et al. Autotaxin inhibition reduces cardiac inflammation and mitigates adverse cardiac remodeling after myocardial infarction. J. Mol. Cell Cardiol. 2020, 149, 95–114. [Google Scholar] [CrossRef]
- Maekawa, Y.; Anzai, T.; Yoshikawa, T.; Asakura, Y.; Takahashi, T.; Ishikawa, S.; Mitamura, H.; Ogawa, S. Prognostic significance of peripheral monocytosis after reperfused acute myocardial infarction: A possible role for left ventricular remodeling. J. Am. Coll. Cardiol. 2002, 39, 241–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panizzi, P.; Swirski, F.K.; Figueiredo, J.L.; Waterman, P.; Sosnovik, D.E.; Aikawa, E.; Libby, P.; Pittet, M.; Weissleder, R.; Nahrendorf, M. Impaired infarct healing in atherosclerotic mice with Ly-6C(hi) monocytosis. J. Am. Coll. Cardiol. 2010, 55, 1629–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zouggari, Y.; Ait-Oufella, H.; Bonnin, P.; Simon, T.; Sage, A.P.; Guerin, C.; Vilar, J.; Caligiuri, G.; Tsiantoulas, D.; Laurans, L.; et al. B lymphocytes trigger monocyte mobilization and impair heart function after acute myocardial infarction. Nat. Med. 2013, 19, 1273–1280. [Google Scholar] [CrossRef] [PubMed]
- Dutta, P.; Courties, G.; Wei, Y.; Leuschner, F.; Gorbatov, R.; Robbins, C.S.; Iwamoto, Y.; Thompson, B.; Carlson, A.L.; Heidt, T.; et al. Myocardial infarction accelerates atherosclerosis. Nature 2012, 487, 325–329. [Google Scholar] [CrossRef] [Green Version]
- Askari, N.; Lipps, C.; Voss, S.; Staubach, N.; Grun, D.; Klingenberg, R.; von Jeinsen, B.; Wolter, J.S.; Kriechbaum, S.; Dorr, O.; et al. Circulating Monocyte Subsets Are Associated with Extent of Myocardial Injury but not with Type of Myocardial Infarction. Front. Cardiovasc. Med. 2021, 8, 741890. [Google Scholar] [CrossRef]
- Dutta, P.; Nahrendorf, M. Monocytes in myocardial infarction. Arter. Thromb. Vasc. Biol. 2015, 35, 1066–1070. [Google Scholar] [CrossRef] [Green Version]
- Mangold, A.; Hofbauer, T.M.; Ondracek, A.S.; Artner, T.; Scherz, T.; Speidl, W.S.; Krychtiuk, K.A.; Sadushi-Kolici, R.; Jakowitsch, J.; Lang, I.M. Neutrophil extracellular traps and monocyte subsets at the culprit lesion site of myocardial infarction patients. Sci. Rep. 2019, 9, 16304. [Google Scholar] [CrossRef] [Green Version]
- Tapp, L.D.; Shantsila, E.; Wrigley, B.J.; Pamukcu, B.; Lip, G.Y. The CD14++CD16+ monocyte subset and monocyte-platelet interactions in patients with ST-elevation myocardial infarction. J. Thromb. Haemost. 2012, 10, 1231–1241. [Google Scholar] [CrossRef]
- Zhou, X.; Liu, X.L.; Ji, W.J.; Liu, J.X.; Guo, Z.Z.; Ren, D.; Ma, Y.Q.; Zeng, S.; Xu, Z.W.; Li, H.X.; et al. The Kinetics of Circulating Monocyte Subsets and Monocyte-Platelet Aggregates in the Acute Phase of ST-Elevation Myocardial Infarction: Associations with 2-Year Cardiovascular Events. Medicine 2016, 95, e3466. [Google Scholar] [CrossRef]
- Krychtiuk, K.A.; Lenz, M.; Richter, B.; Hohensinner, P.J.; Kastl, S.P.; Mangold, A.; Huber, K.; Hengstenberg, C.; Wojta, J.; Heinz, G.; et al. Monocyte subsets predict mortality after cardiac arrest. J. Leukoc. Biol. 2021, 109, 1139–1146. [Google Scholar] [CrossRef]
- Sarma, J.; Laan, C.A.; Alam, S.; Jha, A.; Fox, K.A.; Dransfield, I. Increased platelet binding to circulating monocytes in acute coronary syndromes. Circulation 2002, 105, 2166–2171. [Google Scholar] [CrossRef] [Green Version]
- Shantsila, E.; Lip, G.Y. The role of monocytes in thrombotic disorders. Insights from tissue factor, monocyte-platelet aggregates and novel mechanisms. Thromb. Haemost. 2009, 102, 916–924. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. Jama 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic and Clinical Variables | N (%), Mean (SD), or Median (IQR) |
|---|---|
| Age | 58.9 (1.03) |
| Sex, female | 25 (25%) |
| BMI | 28.8 (0.62) |
| Diabetes mellitus | 31 (31%) |
| Hypertension | 67 (67%) |
| Hyperlipidaemia | 35 (35%) |
| Current smoker | 55 (55%) |
| Congestive heart failure | 1 (1%) |
| Baseline LVEF | 46.07 (13.8) |
| Previous myocardial infarction | 14 (14%) |
| Previous coronary revascularization | 24 (24%) |
| Previous coronary bypass surgery | 1 (1%) |
| Previous stroke | 4 (4%) |
| Peripheral vascular disease | 2 (2%) |
| Chronic kidney disease | 1 (1%) |
| Door to balloon time in minutes * | 33.5 (28.4) |
| Race | |
| White | 92 (92%) |
| African American | 5 (5%) |
| Culprit artery | |
| Left anterior descending | 31 (31%) |
| Left circumflex | 15 (15%) |
| Right coronary artery | 50 (50%) |
| Medications at discharge | |
| Statins | 97 (97%) |
| Angiotensin converting enzyme | 63 (63%) |
| Angiotensin receptor blocker | 10 (10%) |
| Beta blocker | 93 (93%) |
| Aspirin | 96 (96%) |
| P2Y12 inhibitors | 100 (100%) |
| Ticagrelor | 85 (85%) |
| Clopidogrel | 11 (11%) |
| Prasugrel | 4 (4%) |
| Models | Hazardous Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|
| Model 1 | |||
| CD14+CD16++ monocytes | 4.30 | 1.25–14.81 | 0.02 |
| Age | 1.06 | 1.01–1.11 | 0.007 |
| Stroke | 14.03 | 2.61–75.31 | 0.002 |
| Congestive heart failure | 18.41 | 1.92–176.40 | 0.01 |
| Model 2 | |||
| CD14+CD16++/CCR2+ | 3.82 | 1.06–13.76 | 0.04 |
| Age | 1.05 | 1.01–1.11 | 0.01 |
| Stroke | 17.89 | 2.77–115.24 | 0.002 |
| Congestive heart failure | 16.52 | 1.69–161.28 | 0.01 |
| Model 3 | |||
| CD14+CD16++/CD42b+ | 3.37 | 1.07–10.64 | 0.03 |
| Age | 1.06 | 1.01–1.11 | 0.007 |
| Stroke | 12.02 | 2.29–63.12 | 0.003 |
| Congestive heart failure | 18.04 | 1.87–174.13 | 0.01 |
| Model 4 | |||
| CD14+CD16++/CD11b+ | 5.17 | 1.48–18.06 | 0.009 |
| Age | 1.05 | 1.01–1.10 | 0.01 |
| Stroke | 14.58 | 2.76–76.94 | 0.001 |
| Congestive heart failure | 15.64 | 1.62–150.95 | 0.01 |
| Model 5 | |||
| CD14+ HLA-DR+ | 7.57 | 2.00–28.57 | 0.002 |
| Age | 1.09 | 1.03–1.16 | 0.001 |
| Stroke | 14.86 | 2.68–82.30 | 0.001 |
| Congestive heart failure | 23.59 | 2.38–233.17 | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abo-Aly, M.; Shokri, E.; Chelvarajan, L.; Tarhuni, W.M.; Tripathi, H.; Abdel-Latif, A. Prognostic Significance of Activated Monocytes in Patients with ST-Elevation Myocardial Infarction. Int. J. Mol. Sci. 2023, 24, 11342. https://doi.org/10.3390/ijms241411342
Abo-Aly M, Shokri E, Chelvarajan L, Tarhuni WM, Tripathi H, Abdel-Latif A. Prognostic Significance of Activated Monocytes in Patients with ST-Elevation Myocardial Infarction. International Journal of Molecular Sciences. 2023; 24(14):11342. https://doi.org/10.3390/ijms241411342
Chicago/Turabian StyleAbo-Aly, Mohamed, Elica Shokri, Lakshman Chelvarajan, Wadea M. Tarhuni, Himi Tripathi, and Ahmed Abdel-Latif. 2023. "Prognostic Significance of Activated Monocytes in Patients with ST-Elevation Myocardial Infarction" International Journal of Molecular Sciences 24, no. 14: 11342. https://doi.org/10.3390/ijms241411342