
Clinical and Molecular Insights of Radiation-Induced Breast Sarcomas: Is There Hope on the Horizon for Effective Treatment of This Aggressive Disease?



Abstract
:1. Introduction on Breast Sarcomas
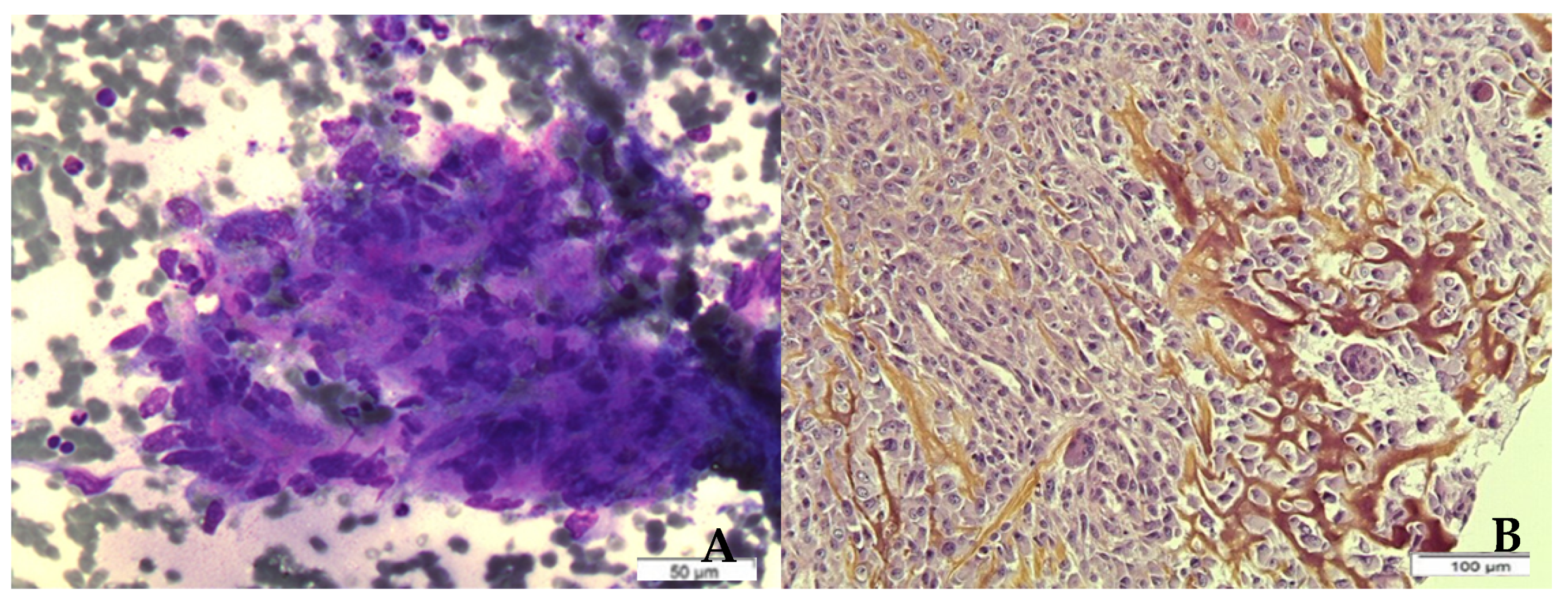
2. Histological Findings in Radiation-Induced Breast Sarcomas—Focus on Angiosarcoma
3. Genetic Alterations in Radiation-Induced Breast Sarcomas
4. Pathophysiology
5. Clinical Presentation of Radiation-Induced Breast Sarcomas
6. Management of Early Disease
6.1. Surgery
6.2. Radiation Therapy
6.3. Systemic Therapy (Adjuvant/Neoadjuvant Chemotherapy)
7. Management of Inoperable/Metastatic Disease
7.1. Chemotherapy
7.2. Bevacizumab
7.3. Tyrosine Kinase Inhibitors
7.4. Immunotherapy
8. Prognosis
9. Conclusions and Perspectives
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Adem, C.; Reynolds, C.; Ingle, J.N.; Nascimento, A.G. Primary Breast Sarcoma: Clinicopathologic Series from the Mayo Clinic and Review of the Literature. Br. J. Cancer 2004, 91, 237–241. [Google Scholar] [CrossRef]
- Pencavel, T.; Allan, C.P.; Thomas, J.M.; Hayes, A.J. Treatment for Breast Sarcoma: A Large, Single-Centre Series. Eur. J. Surg. Oncol. 2011, 37, 703–708. [Google Scholar] [CrossRef] [Green Version]
- Confavreux, C.; Lurkin, A.; Mitton, N.; Blondet, R.; Saba, C.; Ranchère, D.; Sunyach, M.-P.; Thiesse, P.; Biron, P.; Blay, J.-Y.; et al. Sarcomas and Malignant Phyllodes Tumours of the Breast—A Retrospective Study. Eur. J. Cancer 2006, 42, 2715–2721. [Google Scholar] [CrossRef]
- Barrow, B.J.; Janjan, N.A.; Gutman, H.; Benjamin, R.S.; Allen, P.; Romsdahl, M.M.; Ross, M.I.; Pollock, R.E. Role of Radiotherapy in Sarcoma of the Breast—A Retrospective Review of the M.D. Anderson Experience. Radiother. Oncol. 1999, 52, 173–178. [Google Scholar] [CrossRef]
- Zelek, L.; Llombart-Cussac, A.; Terrier, P.; Pivot, X.; Guinebretiere, J.M.; Le Pechoux, C.; Tursz, T.; Rochard, F.; Spielmann, M.; Le Cesne, A. Prognostic Factors in Primary Breast Sarcomas: A Series of Patients with Long-Term Follow-Up. J. Clin. Oncol. 2003, 21, 2583–2588. [Google Scholar] [CrossRef] [PubMed]
- Lahat, G.; Lev, D.; Gerstenhaber, F.; Madewell, J.; Le-Petross, H.; Pollock, R.E. Sarcomas of the Breast. Expert Rev. Anticancer Ther. 2012, 12, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Duncan, M.A.; Lautner, M.A. Sarcomas of the Breast. Surg. Clin. N. Am. 2018, 98, 869–876. [Google Scholar] [CrossRef]
- Bousquet, G.; Confavreux, C.; Magné, N.; de Lara, C.T.; Poortmans, P.; Senkus, E.; de Lafontan, B.; Bolla, M.; Largillier, R.; Lagneau, E.; et al. Outcome and Prognostic Factors in Breast Sarcoma: A Multicenter Study from the Rare Cancer Network. Radiother. Oncol. 2007, 85, 355–361. [Google Scholar] [CrossRef]
- Brady, M.S.; Garfein, C.F.; Petrek, J.A.; Brennan, M.F. Post-Treatment Sarcoma in Breast Cancer Patients. Ann. Surg. Oncol. 1994, 1, 66–72. [Google Scholar] [CrossRef]
- Lagrange, J.L.; Ramaioli, A.; Chateau, M.C.; Marchal, C.; Resbeut, M.; Richaud, P.; Lagarde, P.; Rambert, P.; Tortechaux, J.; Seng, S.H.; et al. Sarcoma after Radiation Therapy: Retrospective Multiinstitutional Study of 80 Histologically Confirmed Cases. Radiology 2000, 216, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Mackillop, W.J. Increased Risk of Soft Tissue Sarcoma after Radiotherapy in Women with Breast Carcinoma. Cancer 2001, 92, 172–180. [Google Scholar] [CrossRef]
- Voutsadakis, I.A.; Zaman, K.; Leyvraz, S. Breast Sarcomas: Current and Future Perspectives. Breast 2011, 20, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, F.; Granath, F.; Smedby, K.E.; Zedenius, J.; Bränström, R.; Nilsson, I.-L. Sarcoma of the Breast: Breast Cancer History as Etiologic and Prognostic Factor-A Population-Based Case-Control Study. Breast Cancer Res. Treat. 2020, 183, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Yap, J.; Chuba, P.J.; Thomas, R.; Aref, A.; Lucas, D.; Severson, R.K.; Hamre, M. Sarcoma as a Second Malignancy after Treatment for Breast Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2002, 52, 1231–1237. [Google Scholar] [CrossRef]
- Karlsson, P.; Holmberg, E.; Samuelsson, A.; Johansson, K.A.; Wallgren, A. Soft Tissue Sarcoma after Treatment for Breast Cancer—A Swedish Population-Based Study. Eur. J. Cancer 1998, 34, 2068–2075. [Google Scholar] [CrossRef]
- Cahan, W.G.; Woodard, H.Q.; Higinbotham, N.L.; Stewart, F.W.; Coley, B.L. Sarcoma Arising in Irradiated Bone: Report of Eleven Cases. Cancer 1998, 82, 8–34. [Google Scholar] [CrossRef]
- Arlen, M.; Higinbotham, N.L.; Huvos, A.G.; Marcove, R.C.; Miller, T.; Shah, I.C. Radiation-Induced Sarcoma of Bone. Cancer 1971, 28, 1087–1099. [Google Scholar] [CrossRef]
- Cha, C.; Antonescu, C.R.; Quan, M.L.; Maru, S.; Brennan, M.F. Long-Term Results with Resection of Radiation-Induced Soft Tissue Sarcomas. Ann. Surg. 2004, 239, 903–910. [Google Scholar] [CrossRef]
- Mark, R.J.; Poen, J.; Tran, L.M.; Fu, Y.S.; Selch, M.T.; Parker, R.G. Postirradiation Sarcomas. A Single-Institution Study and Review of the Literature. Cancer 1994, 73, 2653–2662. [Google Scholar] [CrossRef]
- Al-Benna, S.; Poggemann, K.; Steinau, H.-U.; Steinstraesser, L. Diagnosis and Management of Primary Breast Sarcoma. Breast Cancer Res. Treat. 2010, 122, 619–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirova, Y.M.; Vilcoq, J.R.; Asselain, B.; Sastre-Garau, X.; Fourquet, A. Radiation-Induced Sarcomas after Radiotherapy for Breast Carcinoma: A Large-Scale Single-Institution Review. Cancer 2005, 104, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, S.J.; Pinnock, N.; Giblin, V.; Fisher, C.; Thway, K.; Thomas, J.M.; Hayes, A.J. Treatment and Outcome of Radiation-Induced Soft-Tissue Sarcomas at a Specialist Institution. Eur. J. Surg. Oncol. 2009, 35, 654–659. [Google Scholar] [CrossRef]
- Penel, N.; Bui, B.N.; Bay, J.-O.; Cupissol, D.; Ray-Coquard, I.; Piperno-Neumann, S.; Kerbrat, P.; Fournier, C.; Taieb, S.; Jimenez, M.; et al. Phase II Trial of Weekly Paclitaxel for Unresectable Angiosarcoma: The ANGIOTAX Study. J. Clin. Oncol. 2008, 26, 5269–5274. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, D.K.; Reynolds, C.; Grant, C.S.; Farley, D.R.; Donohue, J.H. Radiation-Induced Breast Sarcoma. Am. J. Surg. 2002, 184, 356–358. [Google Scholar] [CrossRef]
- Billings, S.D.; McKenney, J.K.; Folpe, A.L.; Hardacre, M.C.; Weiss, S.W. Cutaneous Angiosarcoma Following Breast-Conserving Surgery and Radiation: An Analysis of 27 Cases. Am. J. Surg. Pathol. 2004, 28, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Stewart, F.W.; Treves, N. Lymphangiosarcoma in Postmastectomy Lymphedema; a Report of Six Cases in Elephantiasis Chirurgica. Cancer 1948, 1, 64–81. [Google Scholar] [CrossRef]
- Hung, J.; Hiniker, S.M.; Lucas, D.R.; Griffith, K.A.; McHugh, J.B.; Meirovitz, A.; Thomas, D.G.; Chugh, R.; Herman, J.M. Sporadic versus Radiation-Associated Angiosarcoma: A Comparative Clinicopathologic and Molecular Analysis of 48 Cases. Sarcoma 2013, 2013, 798403. [Google Scholar] [CrossRef] [Green Version]
- De Smet, S.; Vandermeeren, L.; Christiaens, M.-R.; Samson, I.; Stas, M.; Van Limbergen, E.; De Wever, I. Radiation-Induced Sarcoma: Analysis of 46 Cases. Acta Chir. Belg. 2008, 108, 574–579. [Google Scholar] [CrossRef]
- McGowan, T.S.; Cummings, B.J.; O’Sullivan, B.; Catton, C.N.; Miller, N.; Panzarella, T. An Analysis of 78 Breast Sarcoma Patients without Distant Metastases at Presentation. Int. J. Radiat. Oncol. Biol. Phys. 2000, 46, 383–390. [Google Scholar] [CrossRef]
- Torres, K.E.; Ravi, V.; Kin, K.; Yi, M.; Guadagnolo, B.A.; May, C.D.; Arun, B.K.; Hunt, K.K.; Lam, R.; Lahat, G.; et al. Long-Term Outcomes in Patients with Radiation-Associated Angiosarcomas of the Breast Following Surgery and Radiotherapy for Breast Cancer. Ann. Surg. Oncol. 2013, 20, 1267–1274. [Google Scholar] [CrossRef] [Green Version]
- Hodgson, N.C.; Bowen-Wells, C.; Moffat, F.; Franceschi, D.; Avisar, E. Angiosarcomas of the Breast: A Review of 70 Cases. Am. J. Clin. Oncol. 2007, 30, 570–573. [Google Scholar] [CrossRef] [PubMed]
- Palta, M.; Morris, C.G.; Grobmyer, S.R.; Copeland, E.M.; Mendenhall, N.P. Angiosarcoma after Breast-Conserving Therapy: Long-Term Outcomes with Hyperfractionated Radiotherapy. Cancer 2010, 116, 1872–1878. [Google Scholar] [CrossRef] [PubMed]
- Fineberg, S.; Rosen, P.P. Cutaneous Angiosarcoma and Atypical Vascular Lesions of the Skin and Breast after Radiation Therapy for Breast Carcinoma. Am. J. Clin. Pathol. 1994, 102, 757–763. [Google Scholar] [CrossRef] [PubMed]
- Brodie, C.; Provenzano, E. Vascular Proliferations of the Breast. Histopathology 2008, 52, 30–44. [Google Scholar] [CrossRef]
- Fraga-Guedes, C.; Gobbi, H.; Mastropasqua, M.G.; Rocha, R.M.; Botteri, E.; Toesca, A.; Viale, G. Clinicopathological and Immunohistochemical Study of 30 Cases of Post-Radiation Atypical Vascular Lesion of the Breast. Breast Cancer Res. Treat. 2014, 146, 347–354. [Google Scholar] [CrossRef]
- Brenn, T.; Fletcher, C.D.M. Postradiation Vascular Proliferations: An Increasing Problem. Histopathology 2006, 48, 106–114. [Google Scholar] [CrossRef]
- Patton, K.T.; Deyrup, A.T.; Weiss, S.W. Atypical Vascular Lesions after Surgery and Radiation of the Breast: A Clinicopathologic Study of 32 Cases Analyzing Histologic Heterogeneity and Association with Angiosarcoma. Am. J. Surg. Pathol. 2008, 32, 943–950. [Google Scholar] [CrossRef]
- Mattoch, I.W.; Robbins, J.B.; Kempson, R.L.; Kohler, S. Post-Radiotherapy Vascular Proliferations in Mammary Skin: A Clinicopathologic Study of 11 Cases. J. Am. Acad. Dermatol. 2007, 57, 126–133. [Google Scholar] [CrossRef]
- Heymann, S.; Delaloge, S.; Rahal, A.; Caron, O.; Frebourg, T.; Barreau, L.; Pachet, C.; Mathieu, M.-C.; Marsiglia, H.; Bourgier, C. Radio-Induced Malignancies after Breast Cancer Postoperative Radiotherapy in Patients with Li-Fraumeni Syndrome. Radiat. Oncol. 2010, 5, 104. [Google Scholar] [CrossRef] [Green Version]
- Le, A.N.; Harton, J.; Desai, H.; Powers, J.; Zelley, K.; Bradbury, A.R.; Nathanson, K.L.; Shah, P.D.; Doucette, A.; Freedman, G.M.; et al. Frequency of Radiation-Induced Malignancies Post-Adjuvant Radiotherapy for Breast Cancer in Patients with Li-Fraumeni Syndrome. Breast Cancer Res. Treat. 2020, 181, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Santi, R.; Cetica, V.; Franchi, A.; Pepi, M.; Cesinaro, A.M.; Miracco, C.; Paglierani, M.; De Giorgi, V.; Delfino, C.; Difonzo, E.M.; et al. Tumour Suppressor Gene TP53 Mutations in Atypical Vascular Lesions of Breast Skin Following Radiotherapy. Histopathology 2011, 58, 455–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gondim, G.R.M.; Formiga, M.N.C.; Castro, D.G.; Silva, M.L.G.; Chen, M.; Fogaroli, R.; Ramos, H.; Coelho, T.M.; Pellizzon, A.C.A.; Da Costa, A.A.B.A. Adjuvant radiation therapy in patients with breast cancer and Li-Fraumeni syndrome: Oncologic results and incidence of second neoplasms. J. Clin. Oncol. 2018, 36, e12589. [Google Scholar] [CrossRef]
- Williams, S.B.; Reed, M. Cutaneous Angiosarcoma after Breast Conserving Treatment for Bilateral Breast Cancers in a BRCA-1 Gene Mutation Carrier—A Case Report and Review of the Literature. Surgeon 2009, 7, 250. [Google Scholar] [CrossRef]
- Sadeghi, F.; Asgari, M.; Matloubi, M.; Ranjbar, M.; Karkhaneh Yousefi, N.; Azari, T.; Zaki-Dizaji, M. Molecular Contribution of BRCA1 and BRCA2 to Genome Instability in Breast Cancer Patients: Review of Radiosensitivity Assays. Biol. Proced. Online 2020, 22, 23. [Google Scholar] [CrossRef]
- Schlosser, S.; Rabinovitch, R.; Shatz, Z.; Galper, S.; Shahadi-Dromi, I.; Finkel, S.; Jacobson, G.; Rasco, A.; Friedman, E.; Laitman, Y.; et al. Radiation-Associated Secondary Malignancies in BRCA Mutation Carriers Treated for Breast Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 353–359. [Google Scholar] [CrossRef]
- Wong, F.L.; Boice, J.D.; Abramson, D.H.; Tarone, R.E.; Kleinerman, R.A.; Stovall, M.; Goldman, M.B.; Seddon, J.M.; Tarbell, N.; Fraumeni, J.F.; et al. Cancer Incidence after Retinoblastoma. Radiation Dose and Sarcoma Risk. JAMA 1997, 278, 1262–1267. [Google Scholar] [CrossRef]
- Franken, N.a.P.; van Bree, C.; ten Cate, R.; van Oven, C.H.; Haveman, J. Importance of TP53 and RB in the Repair of Potentially Lethal Damage and Induction of Color Junctions after Exposure to Ionizing Radiation. Radiat. Res. 2002, 158, 707–714. [Google Scholar] [CrossRef]
- Manner, J.; Radlwimmer, B.; Hohenberger, P.; Mössinger, K.; Küffer, S.; Sauer, C.; Belharazem, D.; Zettl, A.; Coindre, J.-M.; Hallermann, C.; et al. MYC High Level Gene Amplification Is a Distinctive Feature of Angiosarcomas after Irradiation or Chronic Lymphedema. Am. J. Pathol. 2010, 176, 34–39. [Google Scholar] [CrossRef]
- Fraga-Guedes, C.; André, S.; Mastropasqua, M.G.; Botteri, E.; Toesca, A.; Rocha, R.M.; Peradze, N.; Rotmensz, N.; Viale, G.; Veronesi, P.; et al. Angiosarcoma and Atypical Vascular Lesions of the Breast: Diagnostic and Prognostic Role of MYC Gene Amplification and Protein Expression. Breast Cancer Res. Treat. 2015, 151, 131–140. [Google Scholar] [CrossRef]
- Mentzel, T.; Schildhaus, H.U.; Palmedo, G.; Büttner, R.; Kutzner, H. Postradiation Cutaneous Angiosarcoma after Treatment of Breast Carcinoma Is Characterized by MYC Amplification in Contrast to Atypical Vascular Lesions after Radiotherapy and Control Cases: Clinicopathological, Immunohistochemical and Molecular Analysis of 66 Cases. Mod. Pathol. 2012, 25, 75–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, S.-C.; Zhang, L.; Sung, Y.-S.; Chen, C.-L.; Kao, Y.-C.; Agaram, N.P.; Singer, S.; Tap, W.D.; D’Angelo, S.; Antonescu, C.R. Recurrent CIC Gene Abnormalities in Angiosarcomas: A Molecular Study of 120 Cases with Concurrent Investigation of PLCG1, KDR, MYC, and FLT4 Gene Alterations. Am. J. Surg. Pathol. 2016, 40, 645–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez, A.P.; Sun, Y.; Tubbs, R.R.; Goldblum, J.R.; Billings, S.D. FISH for MYC Amplification and Anti-MYC Immunohistochemistry: Useful Diagnostic Tools in the Assessment of Secondary Angiosarcoma and Atypical Vascular Proliferations. J. Cutan. Pathol. 2012, 39, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Zhang, L.; Chang, N.-E.; Singer, S.; Maki, R.G.; Antonescu, C.R. Consistent MYC and FLT4 Gene Amplification in Radiation-Induced Angiosarcoma but Not in Other Radiation-Associated Atypical Vascular Lesions. Genes Chromosomes Cancer 2011, 50, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Ginter, P.S.; Mosquera, J.M.; MacDonald, T.Y.; D’Alfonso, T.M.; Rubin, M.A.; Shin, S.J. Diagnostic Utility of MYC Amplification and Anti-MYC Immunohistochemistry in Atypical Vascular Lesions, Primary or Radiation-Induced Mammary Angiosarcomas, and Primary Angiosarcomas of Other Sites. Hum. Pathol. 2014, 45, 709–716. [Google Scholar] [CrossRef]
- Berrington de Gonzalez, A.; Kutsenko, A.; Rajaraman, P. Sarcoma Risk after Radiation Exposure. Clin. Sarcoma Res. 2012, 2, 18. [Google Scholar] [CrossRef] [Green Version]
- Rubino, C.; Shamsaldin, A.; Lê, M.G.; Labbé, M.; Guinebretière, J.-M.; Chavaudra, J.; de Vathaire, F. Radiation Dose and Risk of Soft Tissue and Bone Sarcoma after Breast Cancer Treatment. Breast Cancer Res. Treat. 2005, 89, 277–288. [Google Scholar] [CrossRef]
- Virtanen, A.; Pukkala, E.; Auvinen, A. Incidence of Bone and Soft Tissue Sarcoma after Radiotherapy: A Cohort Study of 295,712 Finnish Cancer Patients. Int. J. Cancer 2006, 118, 1017–1021. [Google Scholar] [CrossRef]
- Tucker, M.A.; D’Angio, G.J.; Boice, J.D.; Strong, L.C.; Li, F.P.; Stovall, M.; Stone, B.J.; Green, D.M.; Lombardi, F.; Newton, W. Bone Sarcomas Linked to Radiotherapy and Chemotherapy in Children. N. Engl. J. Med. 1987, 317, 588–593. [Google Scholar] [CrossRef]
- Marchal, C.; Weber, B.; de Lafontan, B.; Resbeut, M.; Mignotte, H.; du Chatelard, P.P.; Cutuli, B.; Reme-Saumon, M.; Broussier-Leroux, A.; Chaplain, G.; et al. Nine Breast Angiosarcomas after Conservative Treatment for Breast Carcinoma: A Survey from French Comprehensive Cancer Centers. Int. J. Radiat. Oncol. Biol. Phys. 1999, 44, 113–119. [Google Scholar] [CrossRef]
- Rombouts, A.J.M.; Huising, J.; Hugen, N.; Siesling, S.; Poortmans, P.M.; Nagtegaal, I.D.; de Wilt, J.H.W. Assessment of Radiotherapy-Associated Angiosarcoma After Breast Cancer Treatment in a Dutch Population-Based Study. JAMA Oncol. 2019, 5, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Burtt, J.J.; Thompson, P.A.; Lafrenie, R.M. Non-Targeted Effects and Radiation-Induced Carcinogenesis: A Review. J. Radiol. Prot. 2016, 36, R23–R35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sordillo, P.P.; Chapman, R.; Hajdu, S.I.; Magill, G.B.; Golbey, R.B. Lymphangiosarcoma. Cancer 1981, 48, 1674–1679. [Google Scholar] [CrossRef]
- Virtanen, A.; Pukkala, E.; Auvinen, A. Angiosarcoma after Radiotherapy: A Cohort Study of 332,163 Finnish Cancer Patients. Br. J. Cancer 2007, 97, 115–117. [Google Scholar] [CrossRef] [PubMed]
- Mito, J.K.; Mitra, D.; Barysauskas, C.M.; Mariño-Enriquez, A.; Morgan, E.A.; Fletcher, C.D.M.; Raut, C.P.; Baldini, E.H.; Doyle, L.A. A Comparison of Outcomes and Prognostic Features for Radiation-Associated Angiosarcoma of the Breast and Other Radiation-Associated Sarcomas. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 425–435. [Google Scholar] [CrossRef]
- Mery, C.M.; George, S.; Bertagnolli, M.M.; Raut, C.P. Secondary Sarcomas after Radiotherapy for Breast Cancer: Sustained Risk and Poor Survival. Cancer 2009, 115, 4055–4063. [Google Scholar] [CrossRef]
- Vorburger, S.A.; Xing, Y.; Hunt, K.K.; Lakin, G.E.; Benjamin, R.S.; Feig, B.W.; Pisters, P.W.T.; Ballo, M.T.; Chen, L.; Trent, J.; et al. Angiosarcoma of the Breast. Cancer 2005, 104, 2682–2688. [Google Scholar] [CrossRef]
- Tomasini, C.; Grassi, M.; Pippione, M. Cutaneous Angiosarcoma Arising in an Irradiated Breast. Case Report and Review of the Literature. Dermatology 2004, 209, 208–214. [Google Scholar] [CrossRef]
- Holm, M.; Aggerholm-Pedersen, N.; Mele, M.; Jørgensen, P.; Baerentzen, S.; Safwat, A. Primary Breast Sarcoma: A Retrospective Study over 35 Years from a Single Institution. Acta Oncol. 2016, 55, 584–590. [Google Scholar] [CrossRef] [Green Version]
- Brenn, T.; Fletcher, C.D.M. Radiation-Associated Cutaneous Atypical Vascular Lesions and Angiosarcoma: Clinicopathologic Analysis of 42 Cases. Am. J. Surg. Pathol. 2005, 29, 983–996. [Google Scholar] [CrossRef]
- Chikarmane, S.A.; Gombos, E.C.; Jagadeesan, J.; Raut, C.; Jagannathan, J.P. MRI Findings of Radiation-Associated Angiosarcoma of the Breast (RAS). J. Magn. Reson. Imaging 2015, 42, 763–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheth, G.R.; Cranmer, L.D.; Smith, B.D.; Grasso-Lebeau, L.; Lang, J.E. Radiation-Induced Sarcoma of the Breast: A Systematic Review. Oncologist 2012, 17, 405–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberman, L.; Dershaw, D.D.; Kaufman, R.J.; Rosen, P.P. Angiosarcoma of the Breast. Radiology 1992, 183, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Alves, I.; Marques, J.C. Radiation-Induced Angiosarcoma of the Breast: A Retrospective Analysis of 15 Years’ Experience at an Oncology Center. Radiol. Bras. 2018, 51, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Jallali, N.; James, S.; Searle, A.; Ghattaura, A.; Hayes, A.; Harris, P. Surgical Management of Radiation-Induced Angiosarcoma after Breast Conservation Therapy. Am. J. Surg. 2012, 203, 156–161. [Google Scholar] [CrossRef]
- Cohen-Hallaleh, R.B.; Smith, H.G.; Smith, R.C.; Stamp, G.F.; Al-Muderis, O.; Thway, K.; Miah, A.; Khabra, K.; Judson, I.; Jones, R.; et al. Radiation Induced Angiosarcoma of the Breast: Outcomes from a Retrospective Case Series. Clin. Sarcoma Res. 2017, 7, 15. [Google Scholar] [CrossRef] [Green Version]
- Erel, E.; Vlachou, E.; Athanasiadou, M.; Hassan, S.; Chandrasekar, C.R.; Peart, F. Management of Radiation-Induced Sarcomas in a Tertiary Referral Centre: A Review of 25 Cases. Breast 2010, 19, 424–427. [Google Scholar] [CrossRef]
- Seinen, J.M.; Styring, E.; Verstappen, V.; Vult von Steyern, F.; Rydholm, A.; Suurmeijer, A.J.H.; Hoekstra, H.J. Radiation-Associated Angiosarcoma after Breast Cancer: High Recurrence Rate and Poor Survival despite Surgical Treatment with R0 Resection. Ann. Surg. Oncol. 2012, 19, 2700–2706. [Google Scholar] [CrossRef] [Green Version]
- Sher, T.; Hennessy, B.T.; Valero, V.; Broglio, K.; Woodward, W.A.; Trent, J.; Hunt, K.K.; Hortobagyi, G.N.; Gonzalez-Angulo, A.M. Primary Angiosarcomas of the Breast. Cancer 2007, 110, 173–178. [Google Scholar] [CrossRef] [Green Version]
- Linthorst, M.; van Geel, A.N.; Baartman, E.A.; Oei, S.B.; Ghidey, W.; van Rhoon, G.C.; van der Zee, J. Effect of a Combined Surgery, Re-Irradiation and Hyperthermia Therapy on Local Control Rate in Radio-Induced Angiosarcoma of the Chest Wall. Strahlenther. Onkol. 2013, 189, 387–393. [Google Scholar] [CrossRef]
- Banks, J.; George, J.; Potter, S.; Gardiner, M.D.; Ives, C.; Shaaban, A.M.; Singh, J.; Sherriff, J.; Hallissey, M.T.; Horgan, K.; et al. Breast Angiosarcoma Surveillance Study: UK National Audit of Management and Outcomes of Angiosarcoma of the Breast and Chest Wall. Br. J. Surg. 2021, 108, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Gullett, N.P.; Delman, K.; Folpe, A.L.; Johnstone, P.A.S. National Surgical Patterns of Care: Regional Lymphadenectomy of Breast Sarcomas. Am. J. Clin. Oncol. 2007, 30, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Fraga-Guedes, C.; Gobbi, H.; Mastropasqua, M.G.; Botteri, E.; Luini, A.; Viale, G. Primary and Secondary Angiosarcomas of the Breast: A Single Institution Experience. Breast Cancer Res. Treat. 2012, 132, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Depla, A.L.; Scharloo-Karels, C.H.; de Jong, M.A.A.; Oldenborg, S.; Kolff, M.W.; Oei, S.B.; van Coevorden, F.; van Rhoon, G.C.; Baartman, E.A.; Scholten, R.J.; et al. Treatment and Prognostic Factors of Radiation-Associated Angiosarcoma (RAAS) after Primary Breast Cancer: A Systematic Review. Eur. J. Cancer 2014, 50, 1779–1788. [Google Scholar] [CrossRef] [PubMed]
- Modesto, A.; Filleron, T.; Chevreau, C.; Le Pechoux, C.; Rochaix, P.; Le Guellec, S.; Ducassou, A.; Gangloff, D.; Ferron, G.; Delannes, M. Role of Radiation Therapy in the Conservative Management of Sarcoma within an Irradiated Field. Eur. J. Surg. Oncol. 2014, 40, 187–192. [Google Scholar] [CrossRef]
- Ghareeb, E.R.; Bhargava, R.; Vargo, J.A.; Florea, A.V.; Beriwal, S. Primary and Radiation-Induced Breast Angiosarcoma: Clinicopathologic Predictors of Outcomes and the Impact of Adjuvant Radiation Therapy. Am. J. Clin. Oncol. 2016, 39, 463–467. [Google Scholar] [CrossRef]
- Yin, M.; Wang, W.; Drabick, J.J.; Harold, H.A. Prognosis and Treatment of Non-Metastatic Primary and Secondary Breast Angiosarcoma: A Comparative Study. BMC Cancer 2017, 17, 295. [Google Scholar] [CrossRef] [Green Version]
- Smith, T.L.; Morris, C.G.; Mendenhall, N.P. Angiosarcoma after Breast-Conserving Therapy: Long-Term Disease Control and Late Effects with Hyperfractionated Accelerated Re-Irradiation (HART). Acta Oncol. 2014, 53, 235–241. [Google Scholar] [CrossRef] [Green Version]
- De Jong, M.A.A.; Oldenborg, S.; Bing Oei, S.; Griesdoorn, V.; Kolff, M.W.; Koning, C.C.E.; van Tienhoven, G. Reirradiation and Hyperthermia for Radiation-Associated Sarcoma. Cancer 2012, 118, 180–187. [Google Scholar] [CrossRef]
- Souba, W.W.; McKenna, R.J.; Meis, J.; Benjamin, R.; Raymond, A.K.; Mountain, C.F. Radiation-Induced Sarcomas of the Chest Wall. Cancer 1986, 57, 610–615. [Google Scholar] [CrossRef]
- Gutkin, P.M.; Ganjoo, K.N.; Lohman, M.; von Eyben, R.; Charville, G.W.; Nazerali, R.S.; Dirbas, F.M.; Horst, K.C. Angiosarcoma of the Breast: Management and Outcomes. Am. J. Clin. Oncol. 2020, 43, 820–825. [Google Scholar] [CrossRef] [PubMed]
- Abdou, Y.; Elkhanany, A.; Attwood, K.; Ji, W.; Takabe, K.; Opyrchal, M. Primary and Secondary Breast Angiosarcoma: Single Center Report and a Meta-Analysis. Breast Cancer Res. Treat. 2019, 178, 523–533. [Google Scholar] [CrossRef] [PubMed]
- McClelland, S.; Hatfield, J.; Degnin, C.; Chen, Y.; Mitin, T. Extent of Resection and Role of Adjuvant Treatment in Resected Localized Breast Angiosarcoma. Breast Cancer Res. Treat. 2019, 175, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Arnaout, A.; Wedman, D.M.; El-Sayed, S.; Acharya, V.; Lad, S. Neoadjuvant Gemcitabine-Taxane Chemotherapy for Radiation-Induced Angiosarcoma of the Breast: A Case Report. Breast J. 2012, 18, 276–278. [Google Scholar] [CrossRef]
- Lewcun, J.A.; Pameijer, C.; Kass, R.; Cream, L.; Hershock, D.; Brooks, A.J.; Dodge, D.G. Doxorubicin, Paclitaxel, and Cisplatin Based Chemotherapy for the Treatment of Angiosarcoma: Two Case Reports. Int. J. Surg. Case Rep. 2020, 68, 83–87. [Google Scholar] [CrossRef]
- Quadros, C.A.; Vasconcelos, A.; Andrade, R.; Ramos, R.S.; Studart, E.; Nascimento, G.; Trajano, A. Good Outcome after Neoadjuvant Chemotherapy and Extended Surgical Resection for a Large Radiation-Induced High-Grade Breast Sarcoma. Int. Semin. Surg. Oncol. 2006, 3, 18. [Google Scholar] [CrossRef] [Green Version]
- Italiano, A.; Chen, C.-L.; Thomas, R.; Breen, M.; Bonnet, F.; Sevenet, N.; Longy, M.; Maki, R.G.; Coindre, J.-M.; Antonescu, C.R. Alterations of the P53 and PIK3CA/AKT/MTOR Pathways in Angiosarcomas: A Pattern Distinct from Other Sarcomas with Complex Genomics. Cancer 2012, 118, 5878–5887. [Google Scholar] [CrossRef] [Green Version]
- D’Angelo, S.P.; Antonescu, C.R.; Kuk, D.; Qin, L.; Moraco, N.; Carvajal, R.C.; Chi, P.; Dickson, M.A.; Gounder, M.; Keohan, M.L.; et al. High-Risk Features in Radiation-Associated Breast Angiosarcomas. Br. J. Cancer 2013, 109, 2340–2346. [Google Scholar] [CrossRef] [Green Version]
- Stacchiotti, S.; Palassini, E.; Sanfilippo, R.; Vincenzi, B.; Arena, M.G.; Bochicchio, A.M.; De Rosa, P.; Nuzzo, A.; Turano, S.; Morosi, C.; et al. Gemcitabine in Advanced Angiosarcoma: A Retrospective Case Series Analysis from the Italian Rare Cancer Network. Ann. Oncol. 2012, 23, 501–508. [Google Scholar] [CrossRef]
- Gennaro, M.; Valeri, B.; Casalini, P.; Carcangiu, M.L.; Gronchi, A.; Conti, A.R.; Agresti, R.; Greco, M. Angiosarcoma of the Breast and Vascular Endothelial Growth Factor Receptor. Tumori 2010, 96, 930–935. [Google Scholar] [CrossRef]
- Itakura, E.; Yamamoto, H.; Oda, Y.; Tsuneyoshi, M. Detection and Characterization of Vascular Endothelial Growth Factors and Their Receptors in a Series of Angiosarcomas. J. Surg. Oncol. 2008, 97, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Agulnik, M.; Yarber, J.L.; Okuno, S.H.; von Mehren, M.; Jovanovic, B.D.; Brockstein, B.E.; Evens, A.M.; Benjamin, R.S. An Open-Label, Multicenter, Phase II Study of Bevacizumab for the Treatment of Angiosarcoma and Epithelioid Hemangioendotheliomas. Ann. Oncol. 2013, 24, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Ray-Coquard, I.L.; Domont, J.; Tresch-Bruneel, E.; Bompas, E.; Cassier, P.A.; Mir, O.; Piperno-Neumann, S.; Italiano, A.; Chevreau, C.; Cupissol, D.; et al. Paclitaxel Given Once per Week with or Without Bevacizumab in Patients with Advanced Angiosarcoma: A Randomized Phase II Trial. J. Clin. Oncol. 2015, 33, 2797–2802. [Google Scholar] [CrossRef] [PubMed]
- Weiner, T.M.; Liu, E.T.; Craven, R.J.; Cance, W.G. Expression of Growth Factor Receptors, the Focal Adhesion Kinase, and Other Tyrosine Kinases in Human Soft Tissue Tumors. Ann. Surg. Oncol. 1994, 1, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Van der Graaf, W.T.A.; Blay, J.-Y.; Chawla, S.P.; Kim, D.-W.; Bui-Nguyen, B.; Casali, P.G.; Schöffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. Pazopanib for Metastatic Soft-Tissue Sarcoma (PALETTE): A Randomised, Double-Blind, Placebo-Controlled Phase 3 Trial. Lancet 2012, 379, 1879–1886. [Google Scholar] [CrossRef]
- Kollár, A.; Jones, R.L.; Stacchiotti, S.; Gelderblom, H.; Guida, M.; Grignani, G.; Steeghs, N.; Safwat, A.; Katz, D.; Duffaud, F.; et al. Pazopanib in Advanced Vascular Sarcomas: An EORTC Soft Tissue and Bone Sarcoma Group (STBSG) Retrospective Analysis. Acta Oncol. 2017, 56, 88–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maki, R.G.; D’Adamo, D.R.; Keohan, M.L.; Saulle, M.; Schuetze, S.M.; Undevia, S.D.; Livingston, M.B.; Cooney, M.M.; Hensley, M.L.; Mita, M.M.; et al. Phase II Study of Sorafenib in Patients with Metastatic or Recurrent Sarcomas. J. Clin. Oncol. 2009, 27, 3133–3140. [Google Scholar] [CrossRef] [Green Version]
- Von Mehren, M.; Rankin, C.; Goldblum, J.R.; Demetri, G.D.; Bramwell, V.; Ryan, C.W.; Borden, E. Phase 2 Southwest Oncology Group-Directed Intergroup Trial (S0505) of Sorafenib in Advanced Soft Tissue Sarcomas. Cancer 2012, 118, 770–776. [Google Scholar] [CrossRef] [Green Version]
- D’Angelo, S.P.; Antonescu, C.R.; Keohan, M.L.; Carvajal, R.D.; Dickson, M.A.; Gounder, M.M.; Moraco, N.H.; Singer, S.; Schwartz, G.K.; Tap, W.D. Activity of Sorafenib in Radiation-Associated Breast Angiosarcomas Harboring MYC and FLT4 Amplifications. J. Clin. Oncol. 2012, 30, 10019. [Google Scholar] [CrossRef]
- Komdeur, R.; Hoekstra, H.J.; Molenaar, W.M.; Van Den Berg, E.; Zwart, N.; Pras, E.; Plaza-Menacho, I.; Hofstra, R.M.W.; Van Der Graaf, W.T.A. Clinicopathologic Assessment of Postradiation Sarcomas: KIT as a Potential Treatment Target. Clin. Cancer Res. 2003, 9, 2926–2932. [Google Scholar]
- Malone, E.R.; Anderson, N.; Lewin, J.H.; O’Sullivan, B.; Dickson, B.; Shlien, A.; Abdul Razak, A.R. Immune Signature and Molecular Profiling of Radiation-Induced Sarcoma (RIS). J. Clin. Oncol. 2019, 37, 11040. [Google Scholar] [CrossRef]
- Chan, J.Y.; Lim, J.Q.; Yeong, J.; Ravi, V.; Guan, P.; Boot, A.; Tay, T.K.Y.; Selvarajan, S.; Md Nasir, N.D.; Loh, J.H.; et al. Multiomic Analysis and Immunoprofiling Reveal Distinct Subtypes of Human Angiosarcoma. J. Clin. Investig. 2020, 130, 5833–5846. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, S.P.; Mahoney, M.R.; Van Tine, B.A.; Atkins, J.; Milhem, M.M.; Jahagirdar, B.N.; Antonescu, C.R.; Horvath, E.; Tap, W.D.; Schwartz, G.K.; et al. Nivolumab with or without Ipilimumab Treatment for Metastatic Sarcoma (Alliance A091401): Two Open-Label, Non-Comparative, Randomised, Phase 2 Trials. Lancet Oncol. 2018, 19, 416–426. [Google Scholar] [CrossRef]
- Martin-Broto, J.; Hindi, N.; Grignani, G.; Martinez-Trufero, J.; Redondo, A.; Valverde, C.; Stacchiotti, S.; Lopez-Pousa, A.; D’Ambrosio, L.; Gutierrez, A.; et al. Nivolumab and Sunitinib Combination in Advanced Soft Tissue Sarcomas: A Multicenter, Single-Arm, Phase Ib/II Trial. J. Immunother. Cancer 2020, 8, e001561. [Google Scholar] [CrossRef] [PubMed]
- Florou, V.; Rosenberg, A.E.; Wieder, E.; Komanduri, K.V.; Kolonias, D.; Uduman, M.; Castle, J.C.; Buell, J.S.; Trent, J.C.; Wilky, B.A. Angiosarcoma Patients Treated with Immune Checkpoint Inhibitors: A Case Series of Seven Patients from a Single Institution. J. Immunother. Cancer 2019, 7, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahat, G.; Dhuka, A.R.; Hallevi, H.; Xiao, L.; Zou, C.; Smith, K.D.; Phung, T.L.; Pollock, R.E.; Benjamin, R.; Hunt, K.K.; et al. Angiosarcoma: Clinical and Molecular Insights. Ann. Surg. 2010, 251, 1098–1106. [Google Scholar] [CrossRef]
- Gladdy, R.A.; Qin, L.-X.; Moraco, N.; Edgar, M.A.; Antonescu, C.R.; Alektiar, K.M.; Brennan, M.F.; Singer, S. Do Radiation-Associated Soft Tissue Sarcomas Have the Same Prognosis as Sporadic Soft Tissue Sarcomas? J. Clin. Oncol. 2010, 28, 2064–2069. [Google Scholar] [CrossRef] [Green Version]
- Antonescu, C.R.; Yoshida, A.; Guo, T.; Chang, N.-E.; Zhang, L.; Agaram, N.P.; Qin, L.-X.; Brennan, M.F.; Singer, S.; Maki, R.G. KDR Activating Mutations in Human Angiosarcomas Are Sensitive to Specific Kinase Inhibitors. Cancer Res. 2009, 69, 7175–7179. [Google Scholar] [CrossRef] [Green Version]
- Schuetze, S.M.; Zhao, L.; Chugh, R.; Thomas, D.G.; Lucas, D.R.; Metko, G.; Zalupski, M.M.; Baker, L.H. Results of a Phase II Study of Sirolimus and Cyclophosphamide in Patients with Advanced Sarcoma. Eur. J. Cancer 2012, 48, 1347–1353. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Primary Breast Sarcoma | Radiation-Induced Breast Sarcoma | |
|---|---|---|
| Frequency | Rare | Rare |
| Age | 5th–6th decade | Depends on first cancer age and latency period |
| Risk factors | Unknown, genetic predisposition | Young age of RT, long latency period, high radiation dosage, alkylating agents, genetic predisposition |
| Clinical presentation | Unilateral breast lump | Unilateral breast lump, discoloration, purplish-red nodules, thickening or elevation of the skin, and a diffuse pattern of extension |
| Histology | UPS, FS, AS | AS |
| Prognosis | Poor | Poor |
| Author | Year of Publication | Treatment Period | Total N | AS (%) | Median Age (Years) | Latency Period (Years) | Median T (cm) |
|---|---|---|---|---|---|---|---|
| Karlsson | 1998 | 1958–1992 | 67 | 47.8 | NA | NA | NA |
| Lagrange | 2000 | 1975–1995 | 14 | 42.9 | 65.5 | NA | NA |
| Blanchard | 2002 | 1975–2001 | 34 | 35.3 | 62.3 (mean) | 12.7 (mean) | NA |
| Billings | 2004 | <2004 | 27 | 100 | 70 | 4.9 | 4 |
| Kirova | 2005 | 1984–2005 | 18 | 72.2 | 66.5 | 7.3 | NA |
| Sher | 2007 | 1965–2002 | 13 | 100 | 72 | 7 | NA |
| Hodgson | 2007 | 1981–2000 | 31 | 100 | 72.9 (mean) | 5.2 (mean) | NA |
| Palta | 2010 | 1997–2006 | 14 | 100 | 66.5 | 7.7 | ΝA |
| Pencavel | 2011 | 1996–2006 | 19 | 78.9 | 61 (mean) | ΝA | NA |
| Seinen | 2012 | 1990–2009 | 35 | 100 | 67 | 7 | 4 |
| Fraga-Guedes | 2012 | 1999–2009 | 20 | 100 | 66 | 7.5 | 2.8 |
| Torres | 2013 | 1993–2011 | 95 | 100 | 71 | 7 | 5 |
| Linthorst | 2013 | 2000–2011 | 23 | 100 | 70 | 8.8 | NA |
| D’Angelo | 2013 | 1982–2011 | 79 | 100 | 68 | 7 | 4.2 |
| Cohen-Hallaleh | 2017 | 2000–2014 | 49 | 100 | 72 | 7.5 | 5 |
| Gervais | 2017 | 1994–2014 | 20 | 100 | 71 | 8 | 5–10 |
| Yin | 2017 | 1973–2012 | 173 | 100 | 70–74 | NA | NA |
| Abdou | 2019 | 1990–2015 | 13 | 100 | 71 | 7.8 | 6.9 |
| Rombouts | 2019 | 1989–2017 | 209 | 100 | 73 | 8 | NM |
| Gutkin | 2020 | 1998–2019 | 34 | 100 | 72 | 6.9 | 5.6 (mean) |
| Author | Year of Publication | Nodal Involvem. | Type of Surgery (Ν) | Margin Status (Ν) | Adjuvant RT (%) | (neo)Adjuvant Chemo (%) | OS/DFS (Years) | Prognostic Association |
|---|---|---|---|---|---|---|---|---|
| Karlsson | 1998 | NA | NA | NA | NA | NA | NA | no |
| Lagrange | 2000 | NA | 2 MA, 8 WLE | 2 R2 | 28.6 | 35.7 | NA | surgery |
| Blanchard | 2002 | NA | 30/34 surgery | NA | 30 | 43 | NA | size |
| Billings | 2004 | NA | 10 MA, 10 WLE | NA | 10 | 20 | ΝA | no |
| Kirova | 2005 | NA | 11 MA, 5 WLE | NA | 5.6 | 5.6 | mOS = 22 m | no |
| Sher | 2007 | ΝΕ | 12 MA, 1 WLE | ΝA | 0 | NA | NA | size |
| Hodgson | 2007 | NA | 25 MA, 1 WLE | NA | 0 | NA | NA | no |
| Palta | 2010 | 2/14 | 14 ΜA | NA | 100 (HART) | 0 | 5y-OS = 86%, 5y-PFS = 64% | benefit of HART in addition to surgery |
| Pencavel | 2011 | 0/3 | 12 MA, 6 WLE | ΝA | ΝA | ΝA | mDFS = 30 m. 5y-DFS = 26% | surgery at experienced center |
| Seinen | 2012 | NA | 24 MA, 7 WLE | 23 R0, 1R1, 7 R2 | 3.2 | 3.2 | mDFS = 16 m | amenable to surgery for local recurrence |
| Fraga-Guedes | 2012 | 0 | 15 MA | ΝA | 10 | 50 | 5y-OS = 28.2% | grade, prior RT |
| Torres | 2013 | 0 | 60 MA, 27 WLE | 81 RO, 4 R1, 4 R2 | 0 | 52 | 5y-OS = 91% | size |
| Linthorst | 2013 | NA | 10 MA, 1 WLE | 4/11 R0, 6/11 R1, 1/11 R2 | 34.8 | 0 | mOS = 18 m | reRT + hyperthermia (local control) |
| D’Angelo | 2013 | NA | 65 MA, 13 WLE | 45 R0, 12 R1, 8 R2 | ΝA | 11.4 | mDSS = 3 y. | age > 68 y, depth |
| Cohen-Hallaleh | 2017 | NE | 38 MA | 32/37 R0 | 0 | 19.1 | mOS = 37 m (resectable) | size, resectability |
| Gervais | 2017 | NA | 19 MA, 1 WLE | 18 R0 | 35 | 50 | mOS = 51 m | no |
| Yin | 2017 | NA | NA | NA | 12.7 | NA | mOS = 32 m | age, tumor spread |
| Abdou | 2019 | NA | 9 MA | NA | 7.7 | 61.5 | mOS = 64.2 m | no |
| Rombouts | 2019 | NA | ΝA | ΝA | 9.1 | 1.4 | 5y-OS = 40.5% | no |
| Gutkin | 2020 | 0 | 27 MA, 4 WLE | 12 R0, 6 R1 | 8.8 | 44.1 | mOS = 16.9 y | chemotherapy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kokkali, S.; Moreno, J.D.; Klijanienko, J.; Theocharis, S. Clinical and Molecular Insights of Radiation-Induced Breast Sarcomas: Is There Hope on the Horizon for Effective Treatment of This Aggressive Disease? Int. J. Mol. Sci. 2022, 23, 4125. https://doi.org/10.3390/ijms23084125
Kokkali S, Moreno JD, Klijanienko J, Theocharis S. Clinical and Molecular Insights of Radiation-Induced Breast Sarcomas: Is There Hope on the Horizon for Effective Treatment of This Aggressive Disease? International Journal of Molecular Sciences. 2022; 23(8):4125. https://doi.org/10.3390/ijms23084125
Chicago/Turabian StyleKokkali, Stefania, Jose Duran Moreno, Jerzy Klijanienko, and Stamatios Theocharis. 2022. "Clinical and Molecular Insights of Radiation-Induced Breast Sarcomas: Is There Hope on the Horizon for Effective Treatment of This Aggressive Disease?" International Journal of Molecular Sciences 23, no. 8: 4125. https://doi.org/10.3390/ijms23084125