
Fourier-Transform Infra-Red Microspectroscopy Can Accurately Diagnose Colitis and Assess Severity of Inflammation

 and
and
Abstract
:1. Introduction
1.1. Role of Histology in IBD
1.2. Application of Biospectroscopy Technologies in IBD
1.3. Aim and Hypothesis
2. Results
2.1. General Results
2.2. Hyperspectral Image Analysis Results of Intestinal Mucosa
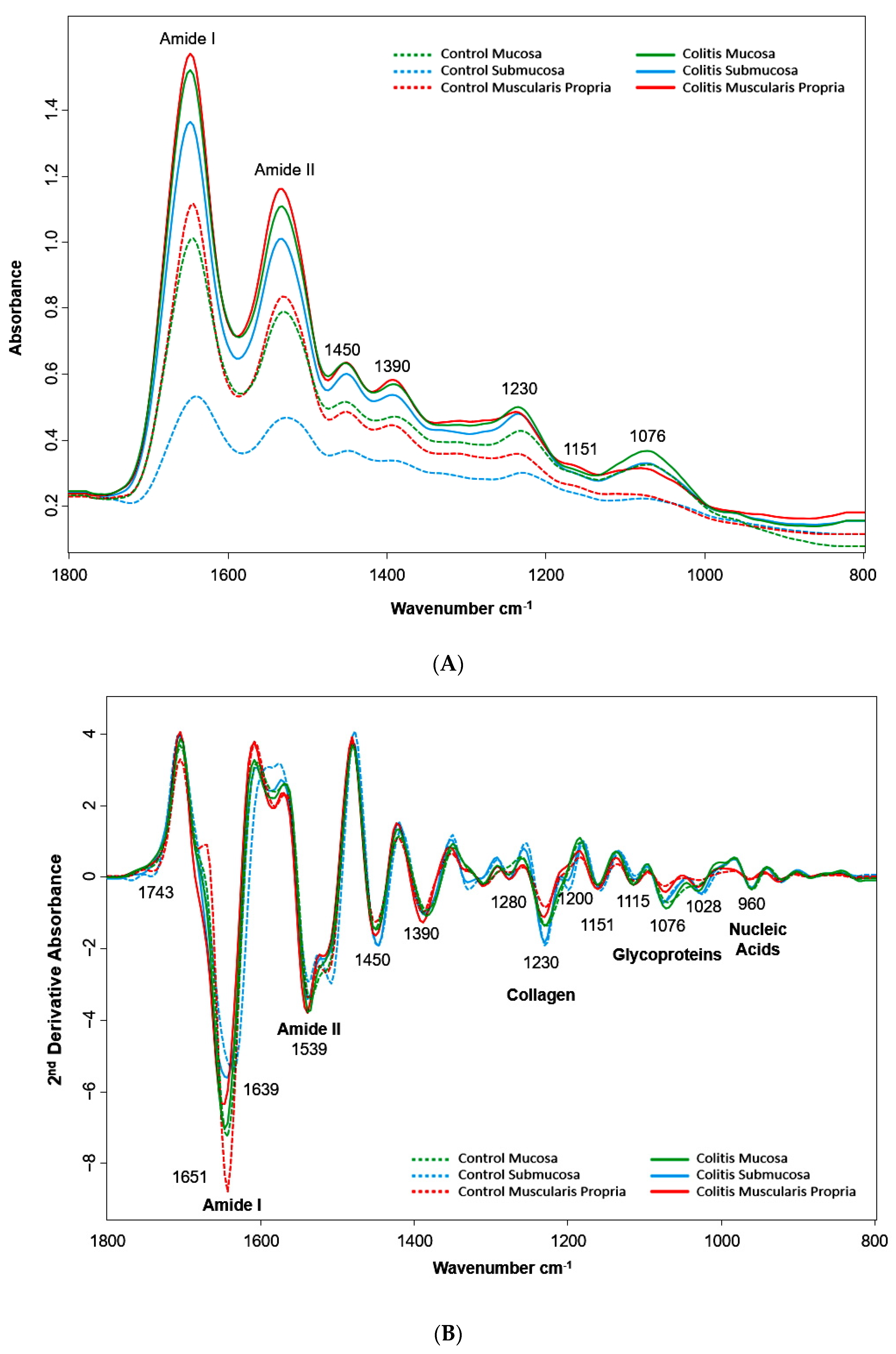
2.2.1. Biochemical Composition
2.2.2. Artificial Neural Network Hyperspectral Image Classifier
2.3. Tissue Colitis Classification
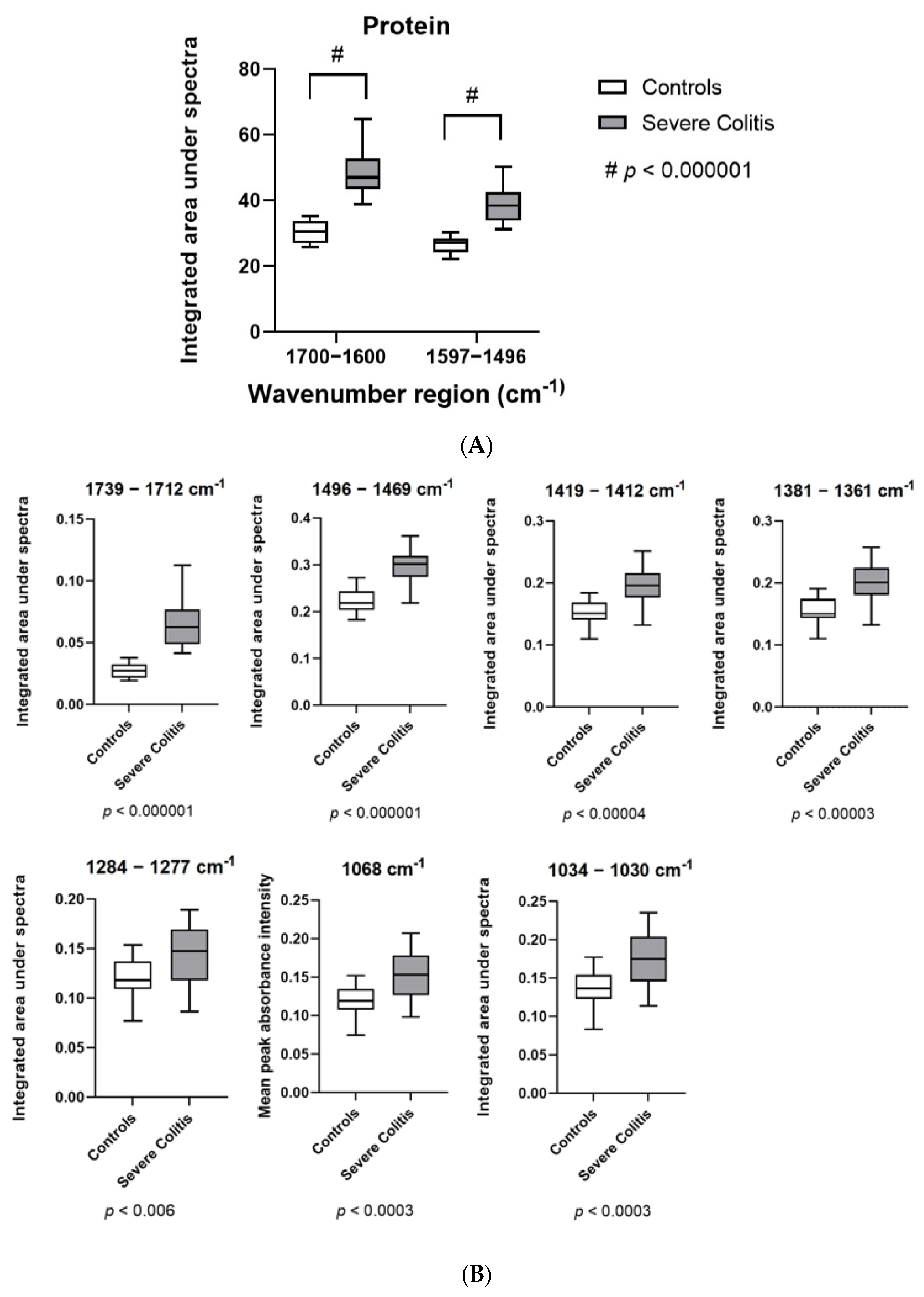
2.3.1. Spectral Biomarkers for Colitis
2.3.2. Colitis Severity Classification
3. Discussion
4. Materials and Methods
4.1. Colitis Induction and Treatment Intervention
4.2. Sample Preparation and Assessment
4.3. FTIR Hyperspectral Imaging Acquisition
4.4. Spectral Data Preprocessing
4.5. Spectral Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANN | Artificial neural network |
| AUROC | Area under receiver operating characteristics |
| CA | Classification accuracy |
| DSS | Dextran sodium sulfate |
| FTIR | Fourier-transform infra-red |
| H&E | Haematoxylin and eosin stain |
| IBD | Inflammatory bowel disease |
| kNN | k-nearest neighbour |
| LV | Latent variables |
| MC | Mucosa |
| SubMC | Submucosa |
| MP | Muscularis propria |
| PC | Principal components |
| PCA | Principal component analysis |
| PLS-DA | Partial least squares discriminant analysis |
References
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2018, 390, 2769–2778. [Google Scholar] [CrossRef]
- G.B.D. Inflammatory Bowel Disease Collaborators. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 17–30. [Google Scholar] [CrossRef] [Green Version]
- Magro, F.; Langner, C.; Driessen, A.; Ensari, A.; Geboes, K.; Mantzaris, G.J.; Villanacci, V.; Becheanu, G.; Nunes, P.B.; Cathomas, G.; et al. European consensus on the histopathology of inflammatory bowel disease. J. Crohn’s Colitis 2013, 7, 827–851. [Google Scholar] [CrossRef] [Green Version]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68, s1–s106. [Google Scholar] [CrossRef] [Green Version]
- Dal Buono, A.; Roda, G.; Argollo, M.; Peyrin-Biroulet, L.; Danese, S. Histological healing: Should it be considered as a new outcome for ulcerative colitis? Expert Opin. Biol. Ther. 2020, 20, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Odze, R.D. IBD: Role of the pathologist in the diagnosis and management of IBD. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 625–626. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.J.; Trevisan, J.; Bassan, P.; Bhargava, R.; Butler, H.J.; Dorling, K.M.; Fielden, P.R.; Fogarty, S.W.; Fullwood, N.J.; Heys, K.A.; et al. Using Fourier transform IR spectroscopy to analyze biological materials. Nat. Protoc. 2014, 9, 1771–1791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Argov, S.; Sahu, R.K.; Bernshtain, E.; Salman, A.; Shohat, G.; Zelig, U.; Mordechai, S. Inflammatory bowel diseases as an intermediate stage between normal and cancer: A FTIR-microspectroscopy approach. Biopolymers 2004, 75, 384–392. [Google Scholar] [CrossRef]
- Li, X.; Li, Q.B.; Zhang, G.J.; Xu, Y.Z.; Sun, X.J.; Shi, J.S.; Zhang, Y.F.; Wu, J.G. Identification of colitis and cancer in colon biopsies by Fourier Transform Infrared spectroscopy and chemometrics. Scient. World J. 2012, 2012, 936149. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Hao, C.; Kang, X.; Zhang, J.; Sun, X.; Wang, W.; Zeng, H. Colorectal Cancer and Colitis Diagnosis Using Fourier Transform Infrared Spectroscopy and an Improved K-Nearest-Neighbour Classifier. Sensors 2017, 17, 2739. [Google Scholar] [CrossRef] [Green Version]
- Katukuri, V.K.; Hargrove, J.; Miller, S.J.; Rahal, K.; Kao, J.Y.; Wolters, R.; Zimmermann, E.M.; Wang, T.D. Detection of colonic inflammation with Fourier transform infrared spectroscopy using a flexible silver halide fiber. Biomed. Opt. Express 2010, 1, 1014–1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Titus, J.; Viennois, E.; Merlin, D.; Perera, A.G.U. Minimally invasive screening for colitis using attenuated total internal reflectance fourier transform infrared spectroscopy. J. Biophotonics 2017, 10, 465–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghimire, H.; Jayaweera, P.V.V.; Perera, A.G.U. Longitudinal analysis of molecular alteration in serum samples of dextran sodium sulfate-induced colitis mice by using infrared spectroscopy. Infrared Phys. Technol. 2019, 97, 33–37. [Google Scholar] [CrossRef]
- Ghimire, H.; Hu, X.; Qin, G.; Perera, A.G.U. Optimizing infrared spectral discrimination to enhance disease diagnostics: Monitoring the signatures of inflammatory bowel diseases with anti-TNFalpha therapy. Biomed. Opt. Express 2020, 11, 4679–4694. [Google Scholar] [CrossRef]
- Titus, J.; Ghimire, H.; Viennois, E.; Merlin, D.; Unil Perera, A.G. Protein secondary structure analysis of dried blood serum using infrared spectroscopy to identify markers for colitis screening. J. Biophotonics 2018, 11, e201700057. [Google Scholar] [CrossRef]
- Heraud, P.; Ng, E.S.; Caine, S.; Yu, Q.C.; Hirst, C.; Mayberry, R.; Bruce, A.; Wood, B.R.; McNaughton, D.; Stanley, E.G.; et al. Fourier transform infrared microspectroscopy identifies early lineage commitment in differentiating human embryonic stem cells. Stem Cell Res. 2010, 4, 140–147. [Google Scholar] [CrossRef] [Green Version]
- Wood, B.R. The importance of hydration and DNA conformation in interpreting infrared spectra of cells and tissues. Chem. Soc. Rev. 2016, 45, 1980–1998. [Google Scholar] [CrossRef]
- Walsh, M.J.; Fellous, T.G.; Hammiche, A.; Lin, W.R.; Fullwood, N.J.; Grude, O.; Bahrami, F.; Nicholson, J.M.; Cotte, M.; Susini, J.; et al. Fourier transform infrared microspectroscopy identifies symmetric PO(2)(-) modifications as a marker of the putative stem cell region of human intestinal crypts. Stem Cells 2008, 26, 108–118. [Google Scholar]
- Sahu, R.K.; Salman, A.; Mordechai, S. Tracing overlapping biological signals in mid-infrared using colonic tissues as a model system. World J. Gastroenterol. 2017, 23, 286–296. [Google Scholar] [CrossRef]
- Jackson, M.; Choo, L.P.; Watson, P.H.; Halliday, W.C.; Mantsch, H.H. Beware of connective tissue proteins: Assignment and implications of collagen absorptions in infrared spectra of human tissues. Biochim. Biophys. Acta 1995, 1270, 1–6. [Google Scholar] [CrossRef]
- Mello, M.L.S.; Vidal, B. Changes in the infrared microspectroscopic characteristics of DNA caused by cationic elements, different base richness and single-stranded form. PLoS ONE 2012, 7, e43169. [Google Scholar] [CrossRef] [PubMed]
- Erben, U.; Loddenkemper, C.; Doerfel, K.; Spieckermann, S.; Haller, D.; Heimesaat, M.M.; Zeitz, M.; Siegmund, B.; Kuhl, A.A. A guide to histomorphological evaluation of intestinal inflammation in mouse models. Int. J. Clin. Exp. Pathol. 2014, 7, 4557–4576. [Google Scholar] [PubMed]
- Zucchiatti, P.; Mitri, E.; Kenig, S.; Bille, F.; Kourousias, G.; Bedolla, D.E.; Vaccari, L. Contribution of Ribonucleic Acid (RNA) to the Fourier Transform Infrared (FTIR) Spectrum of Eukaryotic Cells. Anal. Chem. 2016, 88, 12090–12098. [Google Scholar] [CrossRef] [PubMed]
- Lasch, P.; Haensch, W.; Lewis, E.N.; Kidder, L.H.; Naumann, D. Characterization of Colorectal Adenocarcinoma Sections by Spatially Resolved FT-IR Microspectroscopy. Appl. Spectrosc. 2002, 56, 1–9. [Google Scholar] [CrossRef]
- Bielecki, C.; Bocklitz, T.W.; Schmitt, M.; Krafft, C.; Marquardt, C.; Gharbi, A.; Knosel, T.; Stallmach, A.; Popp, J. Classification of inflammatory bowel diseases by means of Raman spectroscopic imaging of epithelium cells. J. Biomed. Opt. 2012, 17, 076030. [Google Scholar] [CrossRef] [Green Version]
- Morasso, C.; Truffi, M.; Vanna, R.; Albasini, S.; Mazzucchelli, S.; Colombo, F.; Sorrentino, L.; Sampietro, G.; Ardizzone, S.; Corsi, F. Raman Analysis Reveals Biochemical Differences in Plasma of Crohn’s Disease Patients. J. Crohn’s Colitis 2020, 14, 1572–1580. [Google Scholar] [CrossRef]
- Bi, X.; Walsh, A.; Mahadevan-Jansen, A.; Herline, A. Development of spectral markers for the discrimination of ulcerative colitis and Crohn’s disease using Raman spectroscopy. Dis. Colon Rectum 2011, 54, 48–53. [Google Scholar] [CrossRef]
- Veenstra, M.A.; Palyvoda, O.; Alahwal, H.; Jovanovski, M.; Reisner, L.A.; King, B.; Poulik, J.; Klein, M.D. Raman spectroscopy in the diagnosis of ulcerative colitis. Eur. J. Pediatr. Surg. 2015, 25, 56–59. [Google Scholar]
- Addis, J.; Mohammed, N.; Rotimi, O.; Magee, D.; Jha, A.; Subramanian, V. Raman spectroscopy of endoscopic colonic biopsies from patients with ulcerative colitis to identify mucosal inflammation and healing. Biomed. Opt. Express 2016, 7, 2022–2035. [Google Scholar] [CrossRef]
- Ding, H.; Dupont, A.W.; Singhal, S.; Scott, L.D.; Guha, S.; Younes, M.; Bi, X. In vivo analysis of mucosal lipids reveals histological disease activity in ulcerative colitis using endoscope-coupled Raman spectroscopy. Biomed. Opt. Express 2017, 8, 3426–3439. [Google Scholar] [CrossRef] [Green Version]
- Kirchberger-Tolstik, T.; Pradhan, P.; Vieth, M.; Grunert, P.; Popp, J.; Bocklitz, T.W.; Stallmach, A. Towards an Interpretable Classifier for Characterization of Endoscopic Mayo Scores in Ulcerative Colitis Using Raman Spectroscopy. Anal. Chem. 2020, 92, 13776–13784. [Google Scholar] [CrossRef] [PubMed]
- Tefas, C.; Tantau, M. Clinical Applications of Raman Spectroscopy in Inflammatory Bowel Diseases. A Review. J. Gastrointest. Liver Dis. 2018, 27, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Tefas, C.; Marginean, R.; Toma, V.; Petrushev, B.; Fischer, P.; Tantau, M.; Stiufiuc, R. Surface-enhanced Raman scattering for the diagnosis of ulcerative colitis: Will it change the rules of the game? Anal. Bioanal. Chem. 2021, 413, 827–838. [Google Scholar] [CrossRef] [PubMed]
- Kuk, N.; Correia, J.; Alhomrani, M.; Lim, R.; Sievert, W.; Hodge, A.; Moore, G. Human Amnion Epithelial Cells and Their Conditioned Media Reduces Intestinal Inflammation and Fibrosis in a Murine Model of Chronic Colitis, in European Crohn’s and Colitis Organisation-ECCO; Oxford University Press: Vienna, Austria, 2018; p. S072. [Google Scholar]
- Toplak, M.; Birarda, G.; Read, S.; Sandt, C.; Rosendahl, S.M.; Vaccari, L.; Demšar, J.; Borondics, F. Infrared Orange: Connecting Hyperspectral Data with Machine Learning. Synchrotron Radiat. News 2017, 30, 40–45. [Google Scholar] [CrossRef]
- Morais, C.L.M.; Lima, K.M.G.; Singh, M.; Martin, F.L. Tutorial: Multivariate classification for vibrational spectroscopy in biological samples. Nat. Protoc. 2020, 15, 2143–2162. [Google Scholar] [CrossRef] [PubMed]
- Morais, C.L.M.; Paraskevaidi, M.; Cui, L.; Fullwood, N.J.; Isabelle, M.; Lima, K.M.G.; Martin-Hirsch, P.L.; Sreedhar, H.; Trevisan, J.; Walsh, M.J.; et al. Standardization of complex biologically derived spectrochemical datasets. Nat. Protoc. 2019, 14, 1546–1577. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wavenumber Values (cm−1) | Band Assignment |
|---|---|
| ~1743 | Ester carbonyl (lipid) [10] |
| ~1685 | Amide I anti-parallel β-pleated sheet protein secondary structure [12] |
| ~1646 | Amide I α-helix protein secondary structure [10] |
| ~1639 | Amide I β-pleated sheet protein secondary structure [15] |
| ~1539 | Amide II β-pleated sheet [15] |
| ~1515 | Amide II [16] |
| ~1450 | Carboxylate group (proteins) [17] |
| ~1390 | Lipids [16] |
| ~1310 | Amide III [10] |
| ~1280 | Collagen [15] |
| ~1230 | Collagen, nucleic acids [15] |
| ~1200 | Collagen [15] |
| ~1151 | Carbohydrates and glycogen [18] |
| ~1115 | RNA [12] |
| ~1076 | Mannose and glycoproteins, nucleic acids [12] |
| ~1053 | Glycogen and other carbohydrates [16] |
| ~1028 | Glycoproteins including glycogen [19] |
| ~999 | RNA [17] |
| ~964 | Deoxyribose (mainly DNA) [8] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keung, C.; Heraud, P.; Kuk, N.; Lim, R.; Sievert, W.; Moore, G.; Wood, B. Fourier-Transform Infra-Red Microspectroscopy Can Accurately Diagnose Colitis and Assess Severity of Inflammation. Int. J. Mol. Sci. 2022, 23, 2849. https://doi.org/10.3390/ijms23052849
Keung C, Heraud P, Kuk N, Lim R, Sievert W, Moore G, Wood B. Fourier-Transform Infra-Red Microspectroscopy Can Accurately Diagnose Colitis and Assess Severity of Inflammation. International Journal of Molecular Sciences. 2022; 23(5):2849. https://doi.org/10.3390/ijms23052849
Chicago/Turabian StyleKeung, Charlotte, Philip Heraud, Nathan Kuk, Rebecca Lim, William Sievert, Gregory Moore, and Bayden Wood. 2022. "Fourier-Transform Infra-Red Microspectroscopy Can Accurately Diagnose Colitis and Assess Severity of Inflammation" International Journal of Molecular Sciences 23, no. 5: 2849. https://doi.org/10.3390/ijms23052849