
Genetic Biomarkers of Antipsychotic-Induced Prolongation of the QT Interval in Patients with Schizophrenia

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Genetic Predictors of Long QT Syndrome
2.1. Causal Genes for Familial Long QT Syndrome
2.2. Candidate Genes Responsible for Prolongation of the QT Interval
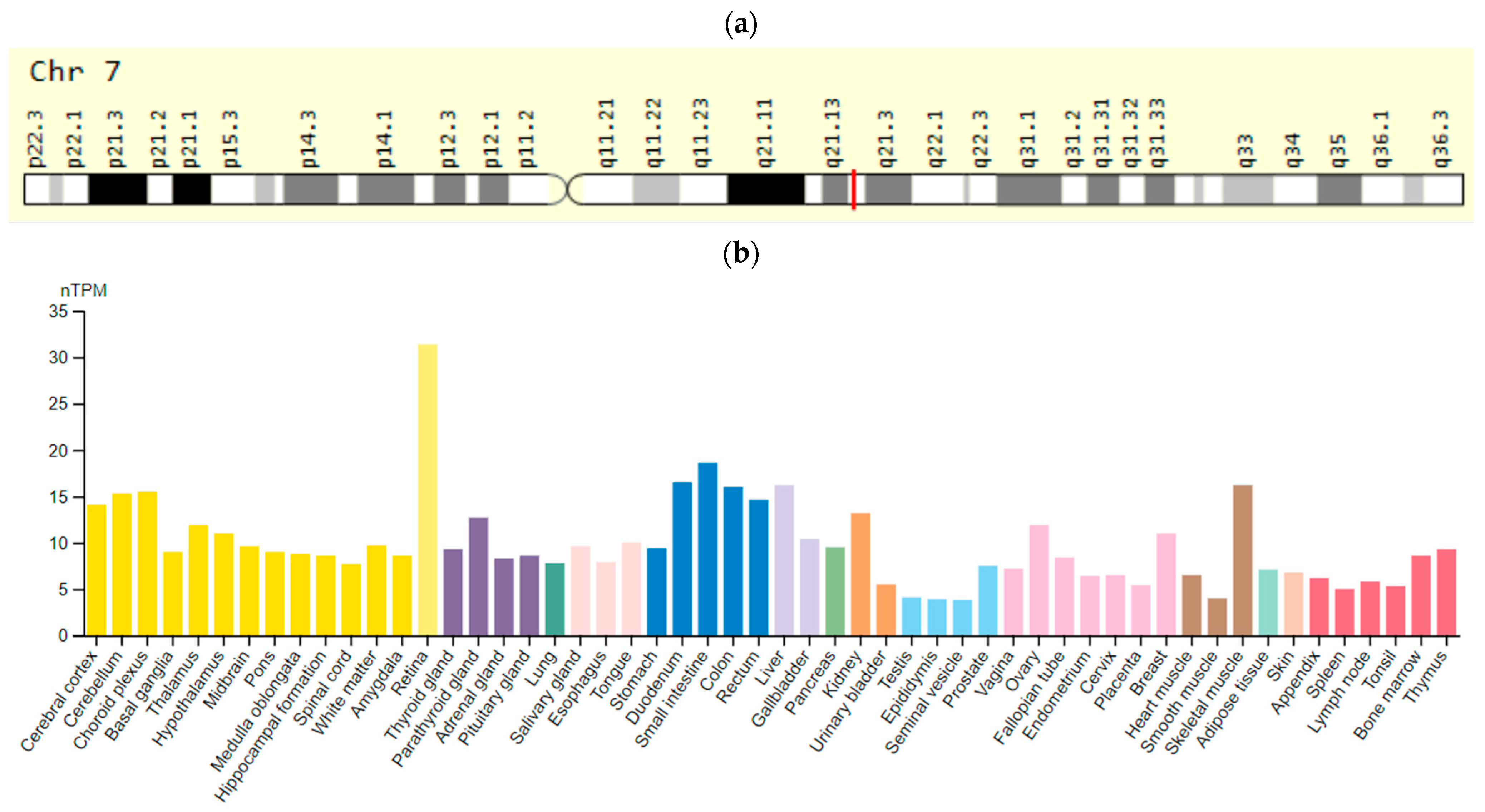
2.2.1. The KCNH2 (HERG) Gene
2.2.2. The SCN5A Gene
2.2.3. The KCNE1 (MiRP1) Gene
2.2.4. The AKAP9 (KCNQ1) Gene
2.3. Candidate Genes Responsible for Poor Metabolism of Antipsychotics
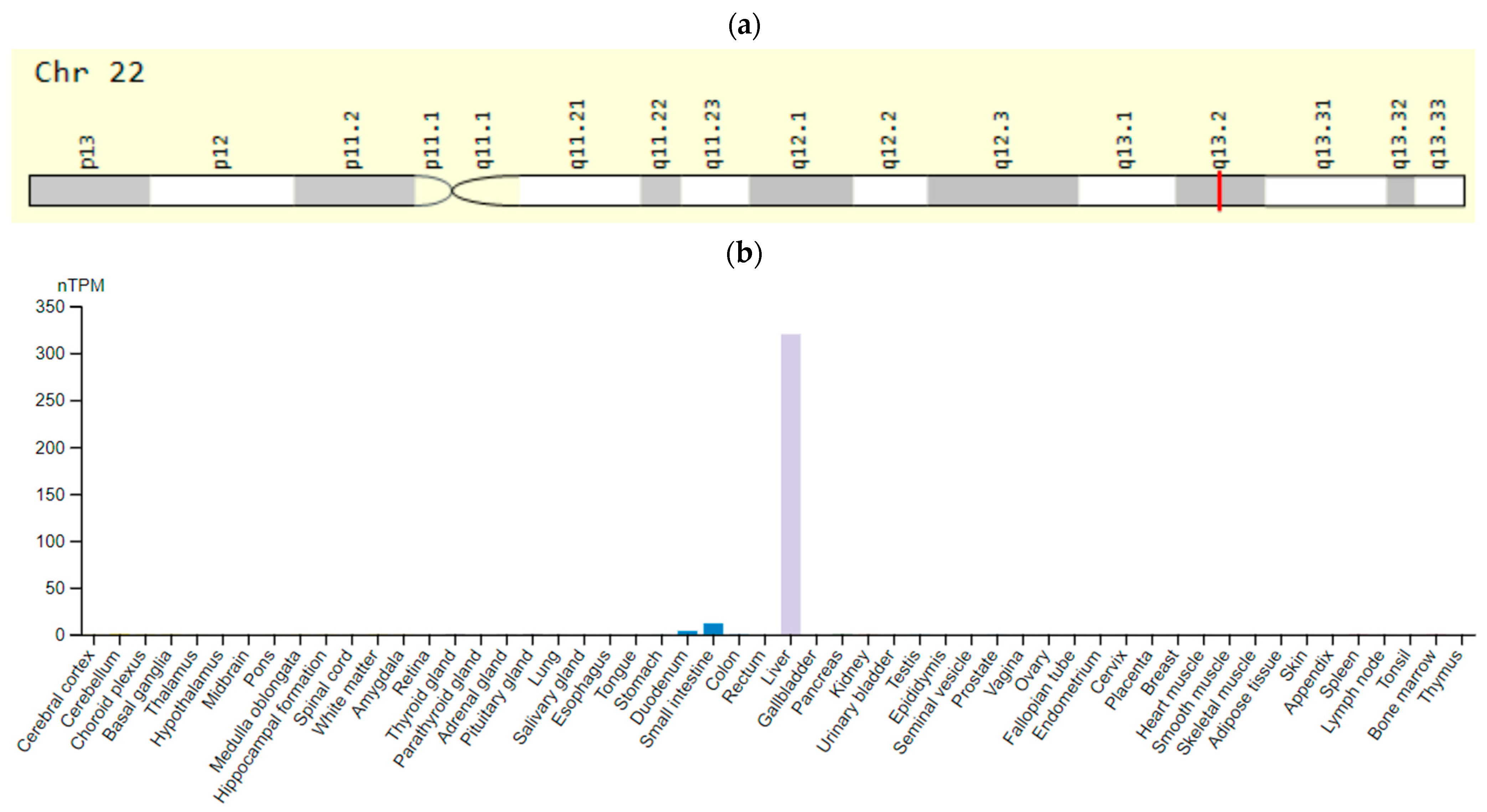
2.3.1. The CYP2D6 Gene
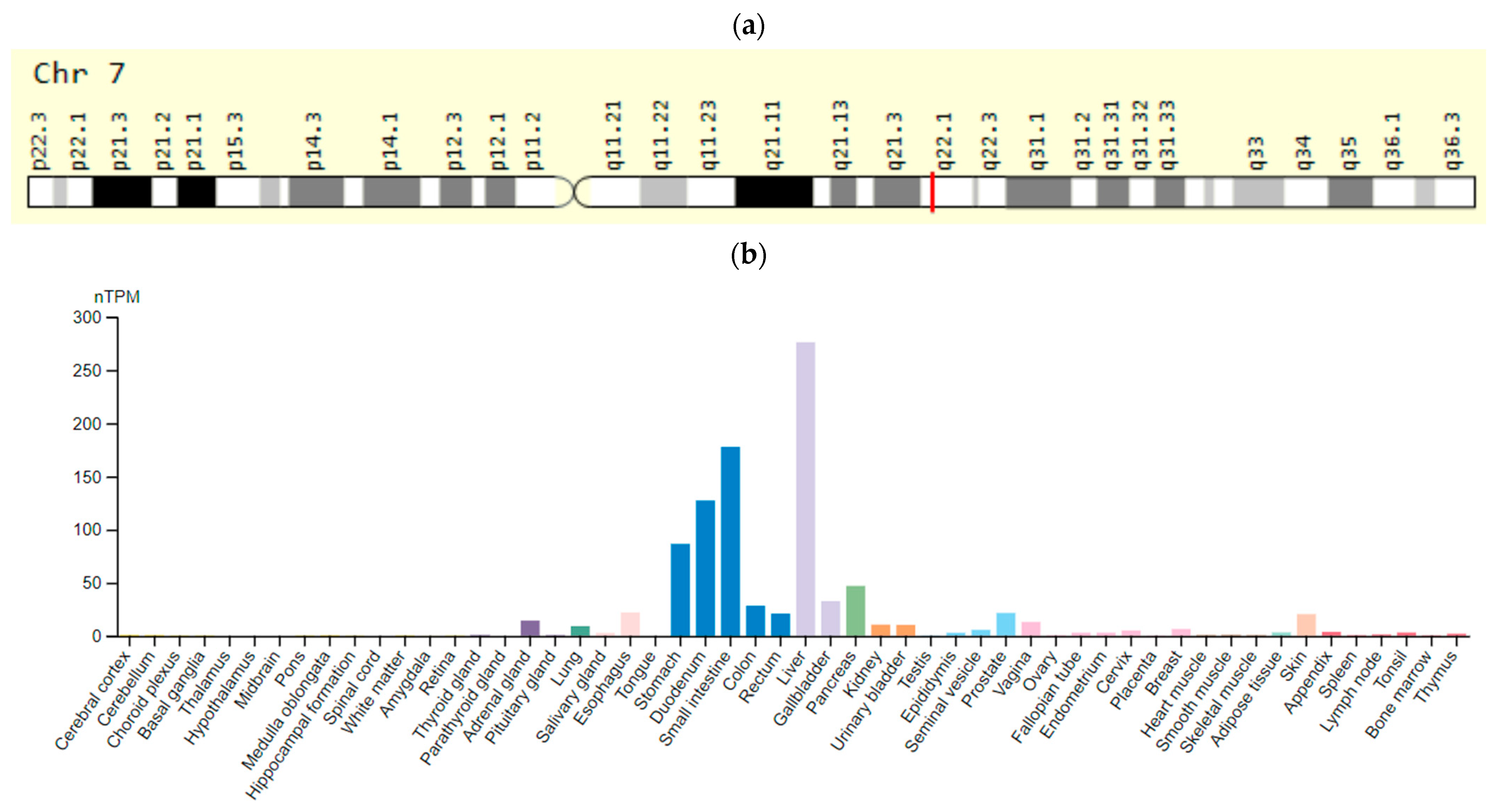
2.3.2. The CYP3A5 Gene
2.3.3. The CYP1A2 Gene
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Laursen, T.M.; Wahlbeck, K.; Hallgren, J.; Westman, J.; Ösby, U.; Alinaghizadeh, H.; Gissler, M.; Nordentoft, M. Life expectancy and death by diseases of the circulatory system in patients with bipolar disorder or schizophrenia in the Nordic countries. PLoS ONE 2013, 8, e67133. [Google Scholar] [CrossRef] [Green Version]
- Dobrodeeva, V.S.; Abdyrahmanova, A.K.; Nasyrova, R.F. Personalized approach to antipsychotic-induced weight gain prognosis. Pers. Psychiatry Neurol. 2021, 1, 3–10. [Google Scholar] [CrossRef]
- Taylor, D.M. Antipsychoticsand QT prolongation. Acta Psychiatr. Scand. 2003, 107, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Hollister, L.E.; Koesk, J.C. Sudden death during treatment with phenothiazine derivatives. JAMA 1965, 192, 1035–1038. [Google Scholar] [CrossRef] [PubMed]
- Huston, J.R.; Bell, G.E. The effect of thioridazine hydrochloride and chlorpromazine on the electrocardiogram. JAMA 1966, 198, 134–138. [Google Scholar] [CrossRef]
- Kelly, H.G.; Fay, J.E.; Laverty, S.G. Thioridazine hydrochloride (Mellaril): Its effect on the electrocardiogram and a report on two fatalities with electrocardiographic abnormalities. Can. Med. Assoc. J. 1963, 89, 546–554. [Google Scholar]
- Leestma, J.E.; Koenig, K.L. Sudden death and phenothiazines: A current controversy. Arch. Gen. Psychiatry 1968, 18, 137–148. [Google Scholar] [CrossRef]
- Roman, M.; Farmer, S.Y. Antipsychotic medications and cardiac conduction risks. Issues Ment. Health Nurs. 2010, 31, 68–70. [Google Scholar] [CrossRef]
- Committee for Proprietary Medicinal Products (CPMP). Points to Consider: The Assessment of the Potential for QT Interval Prolongation by Non-Cardiovascular Medicinal Products; Committee for Proprietary Medicinal Products (CPMP): London, UK, 1997. [Google Scholar]
- Ryzhenko, I.M. Side Effects associated with the peculiarities of the use of antipsychotic drugs. J. Pharm. 2003, 15, 28. Available online: http://provisor.com.ua/archive/2003/N15/art_28.php?part_code=1&art_code=3771 (accessed on 10 February 2022). (In Russian).
- Correll, C.U.; Rubio, J.M.; Kane, J.M. What is the risk-benefit ratio of long-term antipsychotic treatment in people with schizophrenia? World Psychiatry 2018, 17, 149–160. [Google Scholar] [CrossRef] [Green Version]
- D’Urso, G.; Anastasia, A.; Toscano, E.; Patti, S.; de Bartolomeis, A. Aripiprazole-induced atrial fibrillation in a patient with concomitant risk factors. Exp. Clin. Psychopharmacol. 2018, 26, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Parks, K.A.; Parks, C.G.; Yost, J.P.; Bennett, J.I.; Onwuameze, O.E. Acute blood pressure changes associated with antipsychotic administration to psychiatric inpatients. Prim. Care Companion CNS Disord. 2018, 20, 26587. [Google Scholar] [CrossRef] [PubMed]
- Stroup, T.S.; Gray, N. Management of common adverse effects of antipsychotic medications. World Psychiatry 2018, 17, 341–356. [Google Scholar] [CrossRef]
- Haddad, P.M.; Anderson, I.M. Antipsychotic-related QTc prolongation, torsade de pointes and sudden death. Drugs 2002, 62, 1649–1671. [Google Scholar] [CrossRef] [PubMed]
- Jusic, N.; Lader, M. Post-Mortem antipsychotic drug concentrations and unexplained deaths. Br. J. Psychiatry 1994, 165, 787–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehtonen, O.P.; Aranko, K.; Mälkonen, L.; Vapaatalo, H. A survey of sudden death associated with the use of antipsychotic or antidepressant drugs: 49 cases in Finland. Acta Psychiatr. Scand. 1991, 84, 5864. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.G.; Ayis, S.A.; Ferrier, I.N.; Jones, S.J.; Thomas, S.H. QTc-interval abnormalities and psychotropic drug therapy in psychiatric patients. Lancet 2000, 355, 1048–1052. [Google Scholar] [CrossRef] [PubMed]
- Sisakova, M.; Toman, O.; Spinar, J. Monitoring of QT interval in patients treated with psychotropic drugs. Int. J. Cardiol. 2007, 117, 329–332. [Google Scholar] [CrossRef]
- Priori, S.G.; Schwartz, P.J.; Napolitano, C.; Bloise, R.; Ronchetti, E.; Grillo, M.; Vicentini, A.; Spazzolini, C.; Nastoli, J.; Bottelli, G.; et al. Risk stratification in the long-QT syndrome. N. Engl. J. Med. 2003, 348, 1866–1874. [Google Scholar] [CrossRef]
- Mahida, S.; Hogarth, A.J.; Cowan, C.; Tayebjee, M.H.; Graham, L.N.; Pepper, C.B. Genetics of congenital and drug-induced long QT syndromes: Current evidence and future research perspectives. J. Interv. Card. Electrophysiol. 2013, 37, 9–19. [Google Scholar] [CrossRef]
- Hong, Y.; Rautaharju, P.M.; Hopkins, P.N.; Arnett, D.K.; Djoussé, L.; Pankow, J.S.; Sholinsky, P.; Rao, D.C.; Province, M.A. Familial aggregation of QT-interval variability in a general population: Results from the NHLBI Family Heart Study. Clin. Genet. 2001, 59, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Newton-Cheh, C.; Larson, M.G.; Corey, D.C.; Benjamin, E.J.; Herbert, A.G.; Levy, D.; D’Agostino, R.B.; O’Donnell, C.J. QT interval is a heritable quantitative trait with evidence of linkage to chromosome 3 in a genome-wide linkage analysis: The Framingham Heart Study. Heart Rhythm 2005, 2, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Kannankeril, P.J.; Roden, D.M.; Norris, K.J.; Whalen, S.P.; George, A.L., Jr.; Murray, K.T. Genetic susceptibility to acquired long QT syndrome: Pharmacologic challenge in first-degree relatives. Heart Rhythm 2005, 2, 134–140. [Google Scholar] [CrossRef] [PubMed]
- OMIM. Online Mendelian Inheritance in Man. An Online Catalog of Human Genes and Genetic Disorders. (Updated 3 September 2021). Available online: https://www.omim.org/ (accessed on 10 February 2022).
- Gurovich, I.; Vempaty, A.; Lippmann, S. QTc Prolongation: Chlorpromazine and High-Dosage Olanzapine. Can. J. Psychiatry 2003, 48, 348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, D.; Wu, K.; Kathöfer, S.; Katus, H.A.; Schoels, W.; Kiehn, J.; Karle, C.A. The antipsychotic drug chlorpromazine inhibits HERG potassium channels. Br. J. Pharmacol. 2003, 139, 567–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.S.; Kim, E.J. The phenothiazine drugs inhibit hERG potassium channels. Drug Chem. Toxicol. 2005, 28, 303–313. [Google Scholar] [CrossRef]
- Suessbrich, H.; Schönherr, R.; Heinemann, S.H.; Attali, B.; Lang, F.; Busch, A.E. The inhibitory effect of the antipsychotic drug haloperidol on HERG potassium channels expressed in Xenopus oocytes. Br. J. Pharmacol. 1997, 120, 968–974. [Google Scholar] [CrossRef] [Green Version]
- Vesely, P.; Stracina, T.; Hlavacova, M.; Halamek, J.; Kolarova, J.; Olejnickova, V.; Mrkvicova, V.; Paulova, H.; Novakova, M. Haloperidol affects coupling between QT and RR intervals in guinea pig isolated heart. J. Pharmacol. Sci. 2019, 139, 23–28. [Google Scholar] [CrossRef]
- Blom, M.T.; Bardai, A.; van Munster, B.C.; Nieuwland, M.I.; de Jong, H.; van Hoeijen, D.A.; Spanjaart, A.M.; de Boer, A.; de Rooij, S.E.; Tan, H.L. Differential changes in QTc duration during in-hospital haloperidol use. PLoS ONE 2011, 6, e23728. [Google Scholar] [CrossRef]
- Zareba, W.; Lin, D.A. Antipsychotic drugs and QT interval prolongation. Psychiatr. Q. 2003, 74, 291–306. [Google Scholar] [CrossRef]
- Nachimuthu, S.; Assar, M.D.; Schussler, J.M. Drug-induced QT interval prolongation: Mechanisms and clinical management. Ther. Adv. Drug Saf. 2012, 3, 241–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, B.; Wang, C.; Xu, X.; Lyu, H.; Ma, C.; Cheng, G. Risk of Prolonged Corrected QT Interval With Amisulpride Therapy for Renal Function Management in Patients With Schizophrenia. J. Clin. Psychopharmacol. 2020, 40, 482–486. [Google Scholar] [CrossRef] [PubMed]
- Täubel, J.; Ferber, G.; Fox, G.; Fernandes, S.; Lorch, U.; Camm, A.J. Thorough QT study of the effect of intravenous amisulpride on QTc interval in Caucasian and Japanese healthy subjects. Br. J. Clin. Pharmacol. 2017, 83, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, R.; Bastiampillai, T.; Tee, K.; Vanlint, A. Clozapine and associated QTC prolongation. Aust. N. Z. J. Psychiatry 2011, 45, 1098–1099. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Kim, Y.J.; Kim, K.T.; Choe, H.; Jo, S.H. Blockade of HERG human K+ channels and IKr of guinea-pig cardiomyocytes by the antipsychotic drug clozapine. Br. J. Pharmacol. 2006, 148, 499–509. [Google Scholar] [CrossRef] [Green Version]
- Zhu, J.; Hou, W.; Xu, Y.; Ji, F.; Wang, G.; Chen, C.; Lin, C.; Lin, X.; Li, J.; Zhuo, C.; et al. Antipsychotic drugs and sudden cardiac death: A literature review of the challenges in the prediction, management, and future steps. Psychiatry Res. 2019, 281, 112598. [Google Scholar] [CrossRef]
- Dineen, S.; Withrow, K.; Voronovitch, L.; Munshi, F.; Nawbary, M.W.; Lippmann, S. QTc prolongation and high-dose olanzapine. Psychosomatics 2009, 44, 174–175. [Google Scholar] [CrossRef]
- Calderone, V.; Testai, L.; Martinotti, E.; Del Tacca, M.; Breschi, M.C. Drug-induced block of cardiac HERG potassium channels and development of torsade de pointes arrhythmias: The case of antipsychotics. J. Pharm. Pharmacol. 2005, 57, 151–161. [Google Scholar] [CrossRef]
- Kang, J.; Wang, L.; Cai, F.; Rampe, D. High affinity blockade of the HERG cardiac K(+) channel by the neuroleptic pimozide. Eur. J. Pharmacol. 2000, 392, 137–140. [Google Scholar] [CrossRef]
- Hasnain, M.; Vieweg, W.V.; Howland, R.H.; Kogut, C.; Crouse, E.L.B.; Koneru, J.N.; Hancox, J.C.; Digby, G.C.; Baranchuk, A.; Deshmukh, A.; et al. Quetiapine QTc interval prolongation, and torsade de pointes: A review of case reports. Ther. Adv. Psychopharmacol. 2014, 4, 130–138. [Google Scholar] [CrossRef] [Green Version]
- Milnes, J.T.; Witchel, H.J.; Leaney, J.L.; Leishman, D.J.; Hancox, J.C. hERG K+ channel blockade by the antipsychotic drug thioridazine: An obligatory role for the S6 helix residue F656. Biochem. Biophys. Res. Commun. 2006, 351, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Beach, S.R.; Celano, C.M.; Noseworthy, P.A.; Januzzi, J.L.; Huffman, J.C. QTc prolongation, torsades de pointes, and psychotropic medications. Psychosomatics 2013, 54, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Torres-Yaghi, Y.; Carwin, A.; Carolan, J.; Nakano, S.; Amjad, F.; Pagan, F. QTc Interval Prolongation with Therapies Used to Treat Patients with Parkinson’s Disease Psychosis: A Narrative Review. Neuropsychiatr. Dis. Treat. 2021, 17, 3791–3818. [Google Scholar] [CrossRef]
- Guidelines for the Management of QTc Prolongation in Adults Prescribed Antipsychotics. Available online: https://www.england.nhs.uk/north/wp-content/uploads/sites/5/2018/12/QTc-flow-diagram-with-medications-final-Dec-17-A3-with-logos.pdf (accessed on 10 February 2022).
- Khera, A.V.; Mason-Suares, H.; Brockman, D.; Wang, M.; Van Denburgh, M.J.; Senol-Cosar, O.; Patterson, C.; Newton-Cheh, C.; Zekavat, S.M.; Pester, J.; et al. Rare Genetic Variants Associated with Sudden Cardiac Death in Adults. J. Am. Coll. Cardiol. 2019, 74, 2623–2634. [Google Scholar] [CrossRef] [PubMed]
- Spellmann, I.; Reinhard, M.A.; Veverka, D.; Zill, P.; Obermeier, M.; Dehning, S.; Schennach, R.; Müller, N.; Möller, H.J.; Riedel, M.; et al. QTc prolongation in short- term treatment of schizophrenia patients: Effects of different antipsychotics and genetic factors. Eur. Arch. Psychiatry Clin. Neurosci. 2018, 268, 383–390. [Google Scholar] [CrossRef]
- Akyol, M.; Jalilzadeh, S.; Sinner, M.F.; Perz, S.; Beckmann, B.M.; Gieger, C.; Illig, T.; Wichmann, H.E.; Meitinger, T.; Kääb, S.; et al. The common non-synonymous variant G38S of the KCNE1-(minK)-gene is not associated to QT interval in Central European Caucasians: Results from the KORA study. Eur. Heart J. 2007, 28, 305–309. [Google Scholar] [CrossRef] [Green Version]
- de Villiers, C.P.; van der Merwe, L.; Crotti, L.; Goosen, A.; George, A.L.J.; Schwartz, P.J.; Brink, P.A.; Moolman-Smook, J.C.; Corfield, V.A. AKAP9 is a genetic modifier of congenital long-QT syndrome type 1. Circ. Cardiovasc. Genet. 2014, 7, 599–606. [Google Scholar] [CrossRef] [Green Version]
- Vincent, G.M. The molecular genetics of the long QT syndrome: Genes causing fainting and sudden death. Annu. Rev. Med. 1998, 49, 263–274. [Google Scholar] [CrossRef]
- Gene KCNH2. The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000055118-KCNH2 (accessed on 10 October 2022).
- Gene KCNH2. Gene Cards: The Human Gene Database. Available online: https://www.genecards.org/cgi-bin/carddisp.pl?gene=KCNH2&keywords=KCNH2 (accessed on 10 October 2022).
- Chen, L.; Zhang, W.; Fang, C.; Jiang, S.; Shu, C.; Cheng, H.; Li, F.; Li, H. Polymorphism H558R in the human cardiac sodium channel SCN5A gene is associated with atrial fibrillation. J. Int. Med. Res. 2011, 39, 1908–1916. [Google Scholar] [CrossRef]
- Gene SCN5A. The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000183873-SCN5A (accessed on 10 October 2022).
- Gene SCN5A. Gene Cards: The Human Gene Database. Available online: https://www.genecards.org/cgi-bin/carddisp.pl?gene=SCN5A&keywords=SCN5A (accessed on 10 October 2022).
- Gouas, L.; Nicaud, V.; Berthet, M.; Forhan, A.; Tiret, L.; Balkau, B.; Guicheney, P. Association of KCNQ1, KCNE1, KCNH2 and SCN5A polymorphisms with QTc interval length in a healthy population. Eur. J. Hum. Genet. 2005, 13, 1213–1222. [Google Scholar] [CrossRef]
- Hobday, P.M.; Mahoney, D.W.; Urban, L.; Jacobsen, S.J.; Makielski, J.M.; Olson, T.M.; Rodeheffer, R.; Ackerman, M.J. Influence of the common H558R-SCN5A sodium channel polymorphism on the electrocardiographic phenotype in a population-based study. Heart Rhythm 2005, 3, S279–S280. [Google Scholar] [CrossRef]
- Lehtinen, A.B.; Daniel, K.R.; Shah, S.A.; Nelson, M.R.; Ziegler, J.T.; Freedman, B.I.; Carr, J.J.; Herrington, D.M.; Langefeld, C.D.; Bowden, D.W. Relationship between genetic variants in myocardial sodium and potassium channel genes and QT interval duration in diabetics: The Diabetes Heart Study. Ann. Noninvasive Electrocardiol. 2009, 14, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Pfeufer, A.; Sanna, S.; Arking, D.E.; Müller, M.; Gateva, V.; Fuchsberger, C.; Ehret, G.B.; Orrú, M.; Pattaro, C.; Köttgen, A.; et al. Common variants at ten loci modulate the QT interval duration in the QTSCD Study. Nat. Genet. 2009, 41, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.E.; Roden, D.M. The long QT syndromes: Genetic basis and clinical implications. J. Am. Coll. Cardiol. 2000, 36, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Gene KCNE1. The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000180509-KCNE1 (accessed on 10 October 2022).
- Gene KCNE1. Gene Cards: The Human Gene Database. Available online: https://www.genecards.org/cgi-bin/carddisp.pl?gene=KCNE1&keywords=KCNE1 (accessed on 10 October 2022).
- Koskela, J.; Kähönen, M.; Fan, M.; Nieminen, T.; Lehtinen, R.; Viik, J.; Nikus, K.; Niemelä, K.; Kööbi, T.; Turjanmaa, V.; et al. Effect of common KCNE1 and SCN5A ion channel gene variants on T-wave alternans, a marker of cardiac repolarization, during clinical exercise stress test: The Finnish Cardiovascular Study. Transl. Res. 2008, 152, 49–58. [Google Scholar] [CrossRef]
- Barhanin, J.; Lesage, F.; Guillemare, E.; Fink, M.; Lazdunski, M.; Romey, G. KvLQT1 and IsK (minK) proteins associate to form the IKS cardiac potassium current. Nature 1996, 384, 78–80. [Google Scholar] [CrossRef] [PubMed]
- Marx, S.O.; Kurokawa, J.; Reiken, S.; Motoike, H.; D’Armiento, J.; Marks, A.R.; Kass, R.S. Requirement of a macromolecular signaling complex for beta adrenergic receptor modulation of the KCNQ1-KCNE1 potassium channel. Science 2002, 295, 496–499. [Google Scholar] [CrossRef] [Green Version]
- Gene AKAP9. The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000127914-AKAP9 (accessed on 10 October 2022).
- Gene AKAP9. Gene Cards: The Human Gene Database. Available online: https://www.genecards.org/cgi-bin/carddisp.pl?gene=AKAP9&keywords=AKAP9 (accessed on 10 October 2022).
- Shnayder, N.A.; Abdyrakhmanova, A.K.; Nasyrova, R.F. Oxidation of antipsychotics. Encyclopedia 2022, 2, 974–989. [Google Scholar] [CrossRef]
- Shnayder, N.A.; Abdyrakhmanova, A.K.; Nasyrova, R.F. Phase I of antipsychotics metabolism and its pharmacogenetic testing. Pers. Psychiatry Neurol. 2022, 2, 4–21. [Google Scholar] [CrossRef]
- Shnayder, N.A.; Vaiman, E.E.; Neznanov, N.G.; Nasyrova, R.F. Pharmacogenetics of Antipsychotic-Induced Extrapyramidal Disorders; DEAN Publishing House: Macedon, Australia, 2021; p. 288. ISBN 978-5-6046354-7-6. (In Russian) [Google Scholar]
- Kagimoto, M.; Heim, M.; Kagimoto, K.; Zeugin, T.; Meyer, U.A. Multiple mutations of the human cytochrome P450IID6 gene (CYP2D6) in poor metabolizers of debrisoquine. Study of the functional significance of individual mutations by expression of chimeric genes. J. Biol. Chem. 1990, 265, 17209–17214. [Google Scholar] [CrossRef]
- Ranjbar, F.; Akbarzadeh, F.; Ahmadi, N.M.; Abbasnejhad, M. Risperidone and corrected QT-interval prolongation in surface electrocardiogram. Pak. J. Biol. Sci. 2012, 15, 496–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoja, S.S.; Fallah, J.P. Olanzapine induced Q-Tc shortening. Ther. Adv. Psychopharmacol. 2014, 4, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Niemeijer, M.N.; vanden Berg, M.E.; Eijgelsheim, M.; Rijnbeek, P.R.; Stricker, B.H. Pharmacogenetics of Drug-Induced QT Interval Prolongation: An Update. Drug Saf. 2015, 38, 855–867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gene CYP2D6. The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000100197-CYP2D6 (accessed on 10 October 2022).
- Gene CYP2D6. Gene Cards: The Human Gene Database. Available online: https://www.genecards.org/cgi-bin/carddisp.pl?gene=CYP2D6&keywords=CYP2D6 (accessed on 10 October 2022).
- von Bahr, C.; Movin, G.; Nordin, C.; Lidén, A.; Hammarlund-Udenaes, M.; Hedberg, A.; Ring, H.; Sjöqvist, F. Plasma levels of thioridazine and metabolites are influenced by the debrisoquin hydroxylation phenotype. Clin. Pharmacol. Ther. 1991, 49, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Lerena, A.; Berecz, R.; De La Rubia, A.; Norberto, M.J.; Benítez, J. The use of the mesoridazine/thioridazine ratio as a marker for CYP2D6 enzyme activity. Ther. Drug Monit. 2000, 22, 397–401. [Google Scholar] [CrossRef]
- Lerena, A.; Cobaleda, J.; Martínez, C.; Benítez, J. Interethnic differences in drug metabolism: Influence of sex-relatedand environmental factors on debrisoquine hydroxylation phenotype. Eur. J. Drug Metab. Pharmacokinet. 1996, 21, 129–138. [Google Scholar] [CrossRef]
- Mazer-Amirshahi, M.; Porter, R.; Dewey, K. Prolonged QRS Widening After Aripiprazole Overdose. Pediatric Emerg. Care 2019, 35, e209–e212. [Google Scholar] [CrossRef]
- Gene CYP3A5. The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000106258-CYP3A5 (accessed on 10 October 2022).
- Gene CYP3A5. Gene Cards: The Human Gene Database. Available online: https://www.genecards.org/Search/Keyword?queryString=CYP3A5 (accessed on 10 October 2022).
- Gene CYP1A2. The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000140505-CYP1A2 (accessed on 10 October 2022).
- Gene CYP1A2. Gene Cards: The Human Gene Database. Available online: https://www.genecards.org/cgi-bin/carddisp.pl?gene=CYP1A2&keywords=CYP1A2 (accessed on 10 October 2022).
- Food and Drug Administration, HHS. International Conference on Harmonisation; guidance on E14 Clinical Evaluation of QT/QTc Interval Prolongation and Proarrhythmic Potential for Non-Antiarrhythmic Drugs; availability. Notice. Fed. Regist. 2005, 70, 61134–61135. [Google Scholar]
- Shnayder, N.A.; Petrova, M.M.; Petrov, K.V.; Nasyrova, R.F. Pharmacological predictors of heart rate and conductivity disorders in juvenile myoclonic epilepsy. Epilepsy Paroxysmal Cond. 2021, 13, 168–179. [Google Scholar] [CrossRef]
- Fanoe, S.; Kristensen, D.; Fink-Jensen, A.; Jensen, H.K.; Toft, E.; Nielsen, J.; Videbech, P.; Pehrson, S.; Bundgaard, H. Risk of arrhythmia induced by psychotropic medications: A proposal for clinical management. Eur. Heart J. 2014, 35, 1306–1315. [Google Scholar] [CrossRef] [Green Version]
- Mladěnka, P.; Applová, L.; Patočka, J.; Costa, V.M.; Remiao, F.; Pourová, J.; Mladěnka, A.; Karlíčková, J.; Jahodář, L.; Vopršalová, M.; et al. Comprehensive review of cardiovascular toxicity of drugs and related agents. Med. Res. Rev. 2018, 38, 1332–1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, P.; Warner, B. ArehERG channel inhibition and QT interval prolongation all there is in drug-induced torsadogenesis? A review of emerging trends. J. Pharmacol. Toxicol. Methods 2006, 53, 87–105. [Google Scholar] [CrossRef] [PubMed]
- Roden, D.M. Drug-induced prolongation of the QT interval. N. Engl. J. Med. 2004, 350, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.R. Drug-induced QT interval prolongation: Regulatory perspectives and drug development. Ann. Med. 2004, 36, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Nogawa, H.; Kawai, T. hERG trafficking inhibition in drug-induced lethal cardiac arrhythmia. Eur. J. Pharmacol. 2014, 741, 336–339. [Google Scholar] [CrossRef]
- Vaiman, E.E.; Novitsky, M.A.; Nasyrova, R.F. Pharmacogenetics of chlorpromazine and its role in the development of antipsychotic-induced parkinsonism. Pers. Psychiatry Neurol. 2021, 1, 11–17. [Google Scholar] [CrossRef]
- Nasyrova, R.F.; Neznanov, N.G. (Eds.) Clinical Psychopharmacogenetics; DEAN Publishing House: Saint-Petersburg, Russia, 2019; 405p. [Google Scholar]
- Neznanov, N.G. A paradigm shift to treat psychoneurological disorders. Pers. Psychiatry Neurol. 2021, 1, 1–2. [Google Scholar]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene (OMIM Number) | Protein | Chromosome Location | Inheritance | Phenotype (OMIM Number) |
|---|---|---|---|---|
| KCNQ1 (607542) | Potassium voltage-gated channel subfamily Q member 1 | 11p15.5-p15.4 | AR | JLNS1 (220400) |
| AD | LQT1 (192500) | |||
| KCNH2/HERG (152427) | Potential-dependent potassium channel H2 type | 7q36.1 | AD | LQT2 (613688) |
| ALG10B (603313) | Asparagine-associated glycosylation of 10 homologue B | 12q22 | AD | LQT2 (613688) |
| SCN5A (600163) | Alpha subunit of voltage-gated type 5 sodium channel | 3p22 | AD | LQT3 (603830) |
| ANK2 (106410) | Ancrinin 2 | 4q25-q26 | AD | LQT4 (600919) |
| KCNE1/MIRP1 (176261) | Potential-dependent potassium channel E1 type | 22q22.12 | AR | LQT5 (613695) JLNS2 (612347) |
| KCNE2 (603796) | Potential-dependent potassium channel E2 type | 21q22.11 | AD | LQT6 (613693) |
| KCNJ2 (600681) | Voltage-gated potassium channel J2 type | 17q24 | AD | ATS or LQT7 (170390) |
| CACNAIC (114205) | Potential-dependent potassium channel alpha 1C subunit | 12p13.33 | - | BS or LQT8 (618447) |
| CAV3 (601253) | Caveolin 3 | 3p25.3 | AD | LQT9 (611818) |
| SCN4B (608256) | Voltage-dependent sodium channel beta 4 subunit | 11q23.3 | AD | LQT10 (611819) |
| AKAP9/KCNQ1 (604001) | Anchor protein A-kinase 9 type | 7q21.2 | AD | LQT11 (611820) |
| SNTA1 (601017) | Syntrophin alpha 1 | 20q11.21 | AD | LQT12 (612955) |
| KCNJ5 (600734) | Potential-dependent potassium channel J5 type | 11q24.3 | AD | LQT13 (613485) |
| CALM1 (114180) | Calmodulin 1 | 14q32.11 | AD | LQT14 (616247) |
| CALM2 (114182) | Calmodulin 2 | 2p21 | AD | LQT15 (616249) |
| CALM3 (114183) | Calmodulin 3 | 19q13.32 | AD | LQT16 (618782) |
| Antipsychotics | Mechanism of Action | Effect | References |
|---|---|---|---|
| High risk | |||
| Chlorpromazine | Blocking IKr channels | QTc prolongation | [26,27,28] |
| Haloperidol | [29,30,31,32] | ||
| Ziprasidone | [32,33] | ||
| Moderate risk | |||
| Amisulpride (oral) | Blocking IKr channels | QTc prolongation | [34,35] |
| Clozapine | [36,37] | ||
| Flupentixol | [38] | ||
| Haloperidol (oral) | [29,30,31,32] | ||
| Olanzapine | [26,39,40] | ||
| Pimozide | [32,40,41] | ||
| Quetiapine | [32,40,42] | ||
| Risperidone | [32,40] | ||
| Thioridazine | [28,32,40,43] | ||
| Mesoridazine | [32,33] | ||
| Perphenazine | [28] | ||
| Trifluoperazine | [28] | ||
| Sertindole | [40] | ||
| Sulpiride | [40] | ||
| Low risk | |||
| Asenapine | Blocking IKr channels | QTc prolongation | [44] |
| Iloperidone | [44] | ||
| Paliperidone | [44] | ||
| Pimavanserin | [45] | ||
| Aripiprazole | [44] | ||
| No effect | |||
| Aripiprazole | N/A | Do not cause QTc prolongation | [46] |
| Zuclopenthixol | [46] | ||
| Lurasidone | [46] | ||
| Gene (OMIM Number) | Protein | Chromosome Location | rsID | Effect | References |
|---|---|---|---|---|---|
| KCNH2 (152427) | Potential-dependent potassium channel H2 | 7q36.1 | rs189014161 | Susceptibility to QT interval prolongation | [47] |
| SCN5A (600163) | Alpha subunit of voltage-gated type 5 sodium channel | 3p22.2 | rs1805124 | Susceptibility to QT interval prolongation | [48] |
| KCNE1/MIRP1 (176261) | Potential-dependent potassium channel E1 type | 21q22.12 | rs1805127 | Susceptibility to QT interval prolongation | [49] |
| AKAP9/KCNQ1 (604001) | Type 9 alpha kinase anchor protein | 7q21.2 | rs11772585 | The T allele is associated with the risk of QT interval prolongation | [50] |
| rs7808587 | The GG genotype is associated with the risk of QT interval prolongation | [50] | |||
| rs2282972 | The T allele is associated with reducing the risk of QT interval prolongation | [50] | |||
| rs2961024 | The GG genotype is associated with the risk of QT interval prolongation | [50] |
| Gene (OMIM Number) | Protein | Chromosome Location | rsID | Effect | References |
|---|---|---|---|---|---|
| CYP2D6 (124030) | Isoenzyme 2D6 of cytochrome P450 | 22q13.2 | rs16947, rs1135840, rs35742686, rs1135824, rs35742686, rs3892097, rs3892097, i4001456, rs3892097, i4001467 rs3892097, rs28371733, rs5030655, rs5030867, rs5030865, rs5030863, rs5030862, rs5030865, rs72549354 | Risk of prolongation QT interval while taking chlorpromazine, haloperidol, perphenazine, thioridosine, aripiprazil, olanzapine, risperidone. | [72] |
| CYP3A5 (605325) | Isoenzyme 3A5 of cytochrome P450 | 7q22.1 | rs28365083, rs776746, rs10264272, rs41303343, rs55817950, rs28383479, rs41279854, rs72552791, rs56244447, rs28365085, rs28383468, rs41279857 | Risk of prolongation QT interval while taking haloperidol, aripiprazole, risperidone. | [73] |
| CYP1A2 (124060) | Isoenzyme 1A2 of cytochrome P450 | 15q24.1 | rs2069514, rs12720461, rs2069526, rs56276455, rs72547516, rs28399424 | Risk prolongation QT interval while taking olanzapine, clozapine, thioridazine, chlorpromazine. | [74] |
| Category | Characteristic |
|---|---|
| Class A | Drug without the risk of QT interval or TdP |
| Class B | Drug capable of QT interval prolongation |
| Class C | Drug with marked QT interval prolongation, reported cases of TdP or other serious arrhythmia |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaiman, E.E.; Shnayder, N.A.; Zhuravlev, N.M.; Petrova, M.M.; Asadullin, A.R.; Al-Zamil, M.; Garganeeva, N.P.; Shipulin, G.A.; Cumming, P.; Nasyrova, R.F. Genetic Biomarkers of Antipsychotic-Induced Prolongation of the QT Interval in Patients with Schizophrenia. Int. J. Mol. Sci. 2022, 23, 15786. https://doi.org/10.3390/ijms232415786
Vaiman EE, Shnayder NA, Zhuravlev NM, Petrova MM, Asadullin AR, Al-Zamil M, Garganeeva NP, Shipulin GA, Cumming P, Nasyrova RF. Genetic Biomarkers of Antipsychotic-Induced Prolongation of the QT Interval in Patients with Schizophrenia. International Journal of Molecular Sciences. 2022; 23(24):15786. https://doi.org/10.3390/ijms232415786
Chicago/Turabian StyleVaiman, Elena E., Natalia A. Shnayder, Nikita M. Zhuravlev, Marina M. Petrova, Azat R. Asadullin, Mustafa Al-Zamil, Natalia P. Garganeeva, German A. Shipulin, Paul Cumming, and Regina F. Nasyrova. 2022. "Genetic Biomarkers of Antipsychotic-Induced Prolongation of the QT Interval in Patients with Schizophrenia" International Journal of Molecular Sciences 23, no. 24: 15786. https://doi.org/10.3390/ijms232415786