
Mitochondrial DNA as a Candidate Marker of Multiple Organ Failure after Cardiac Surgery
 , ,
, ,
Abstract
:1. Introduction
2. Results
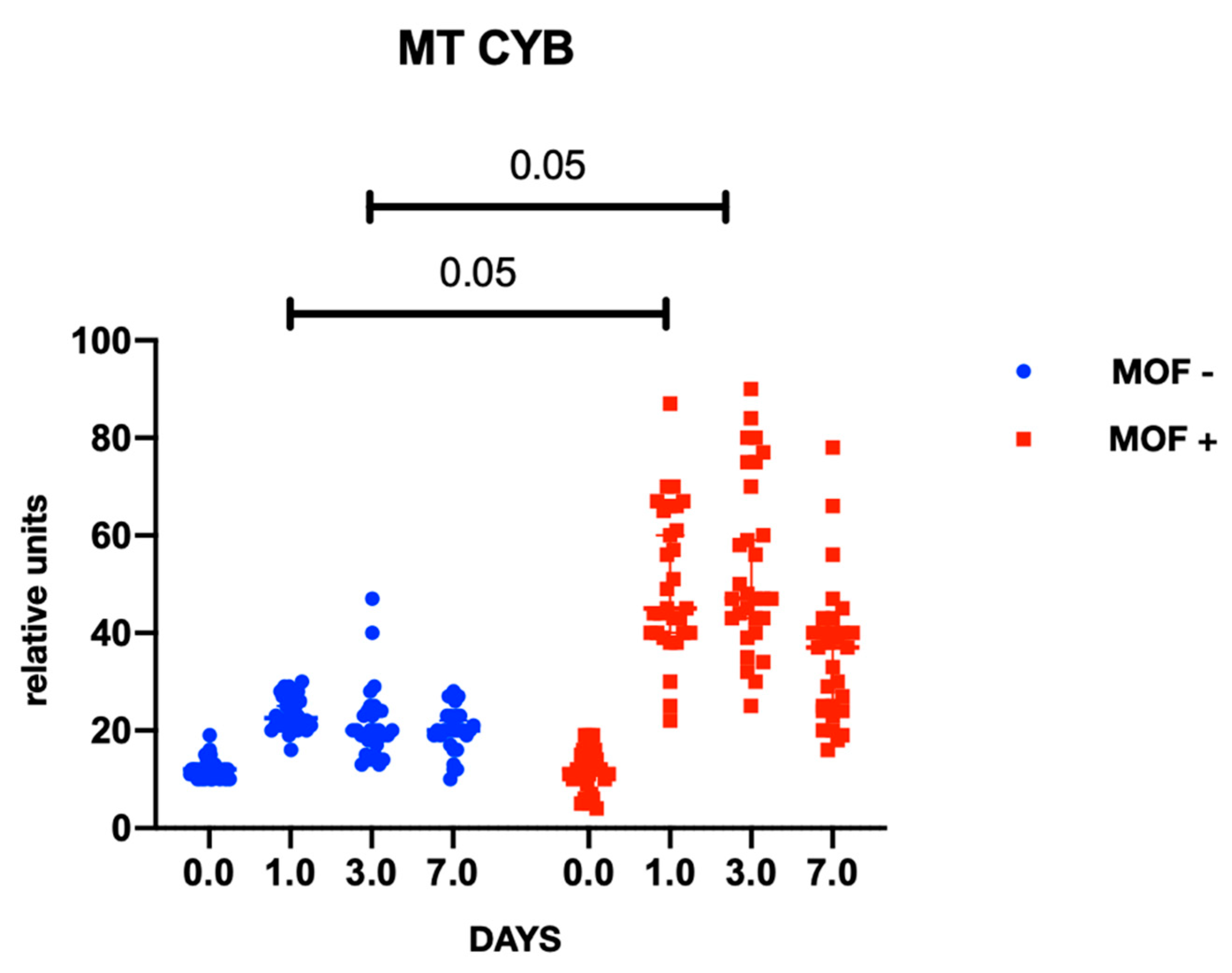
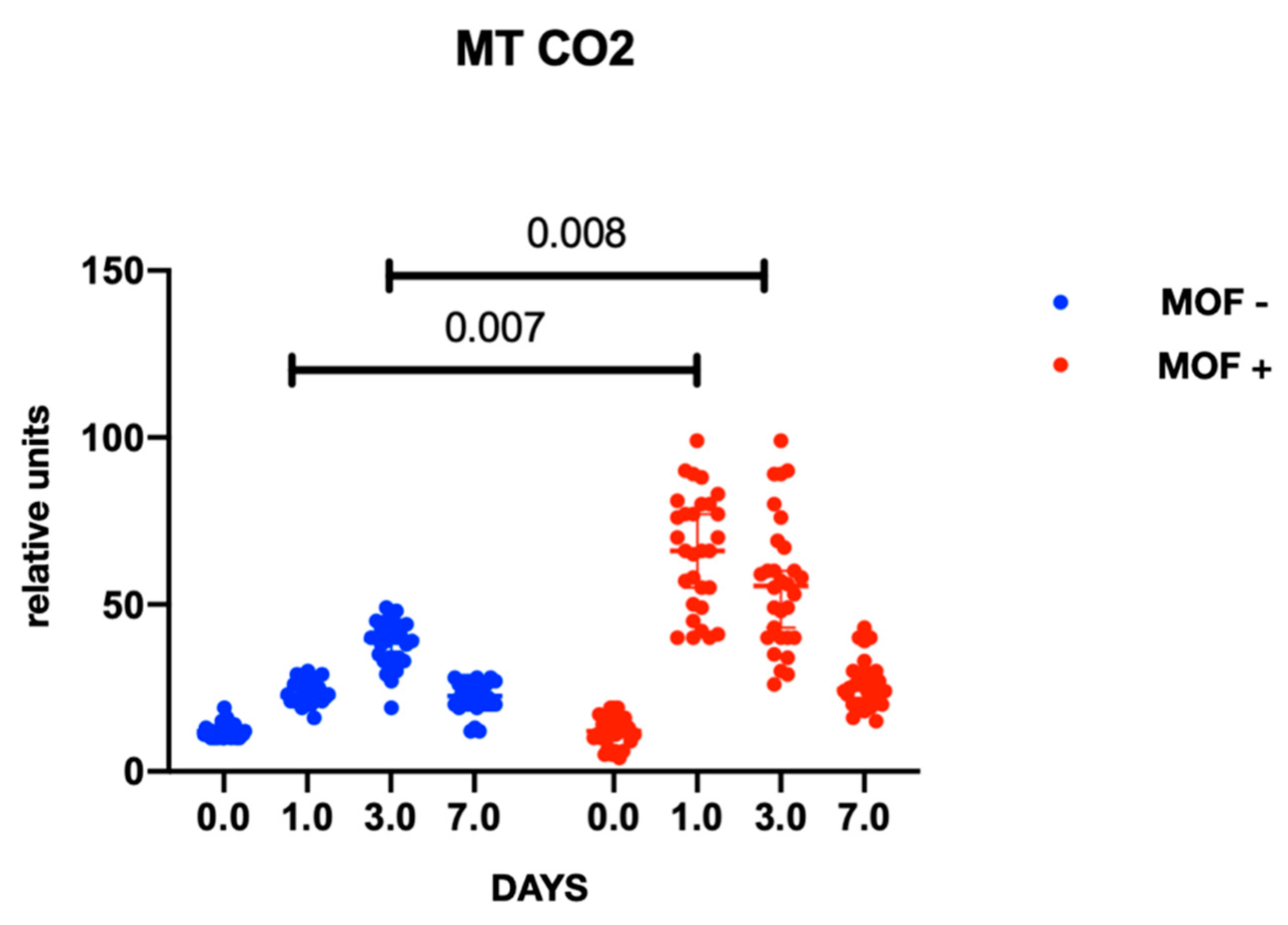
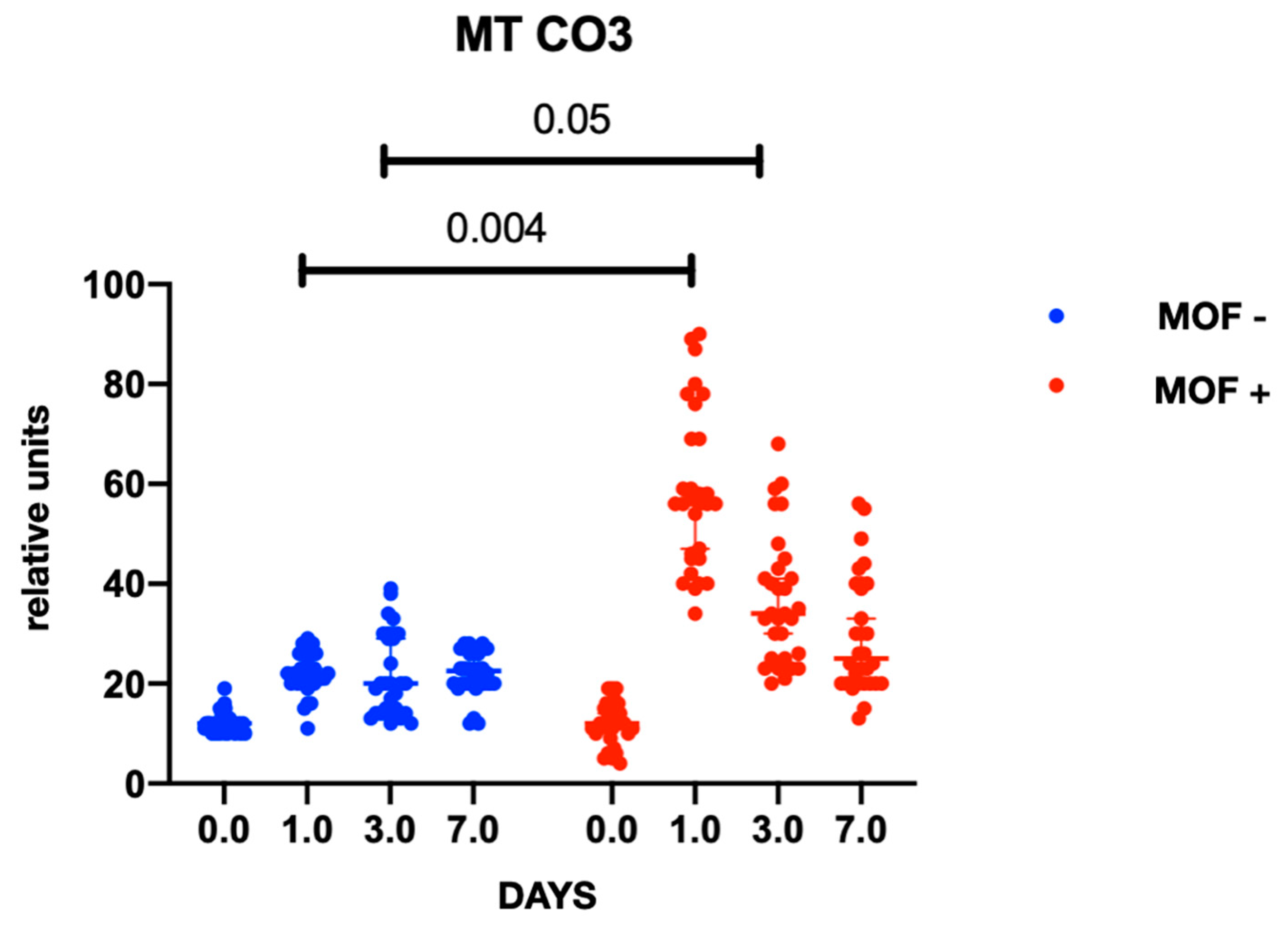
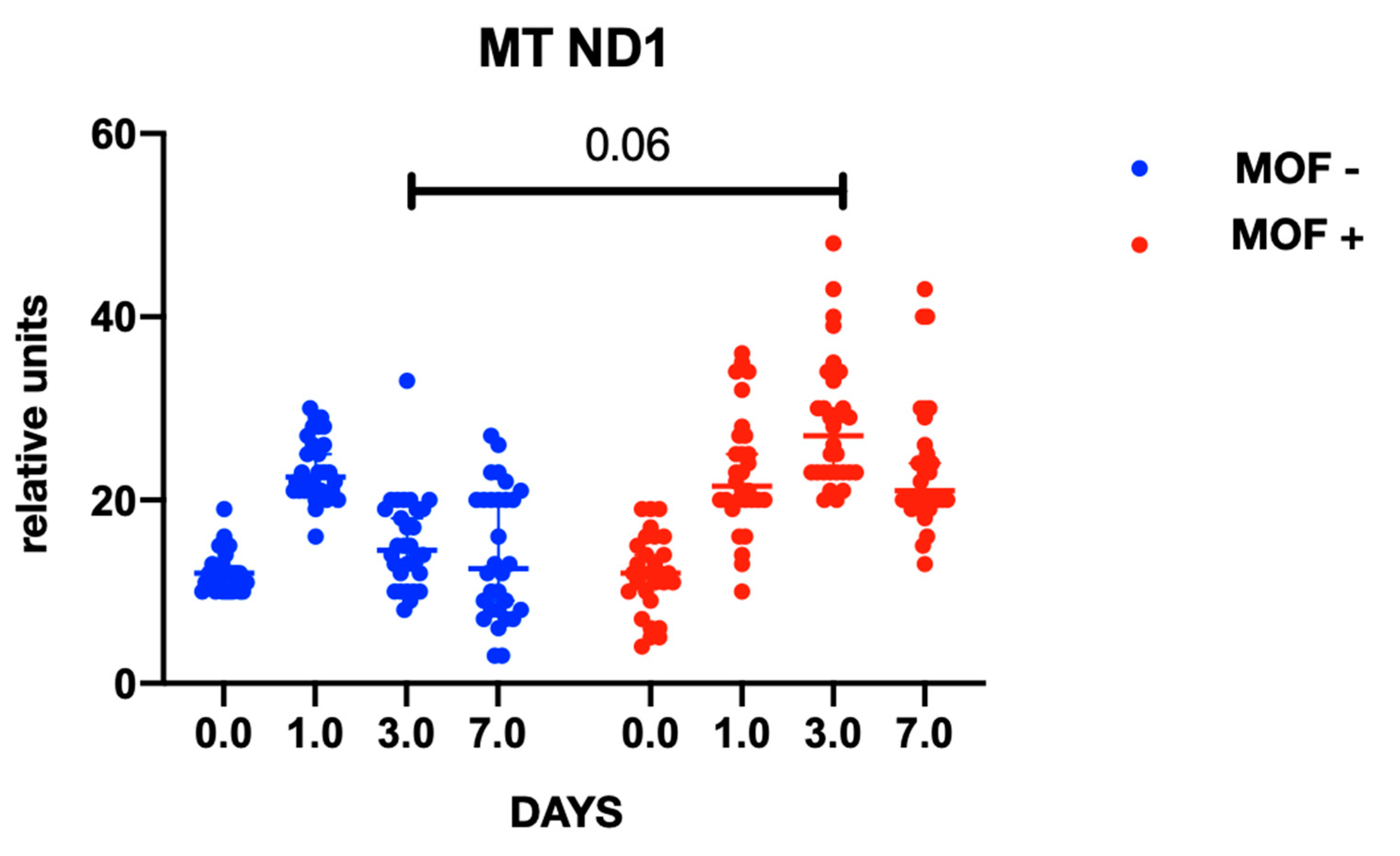
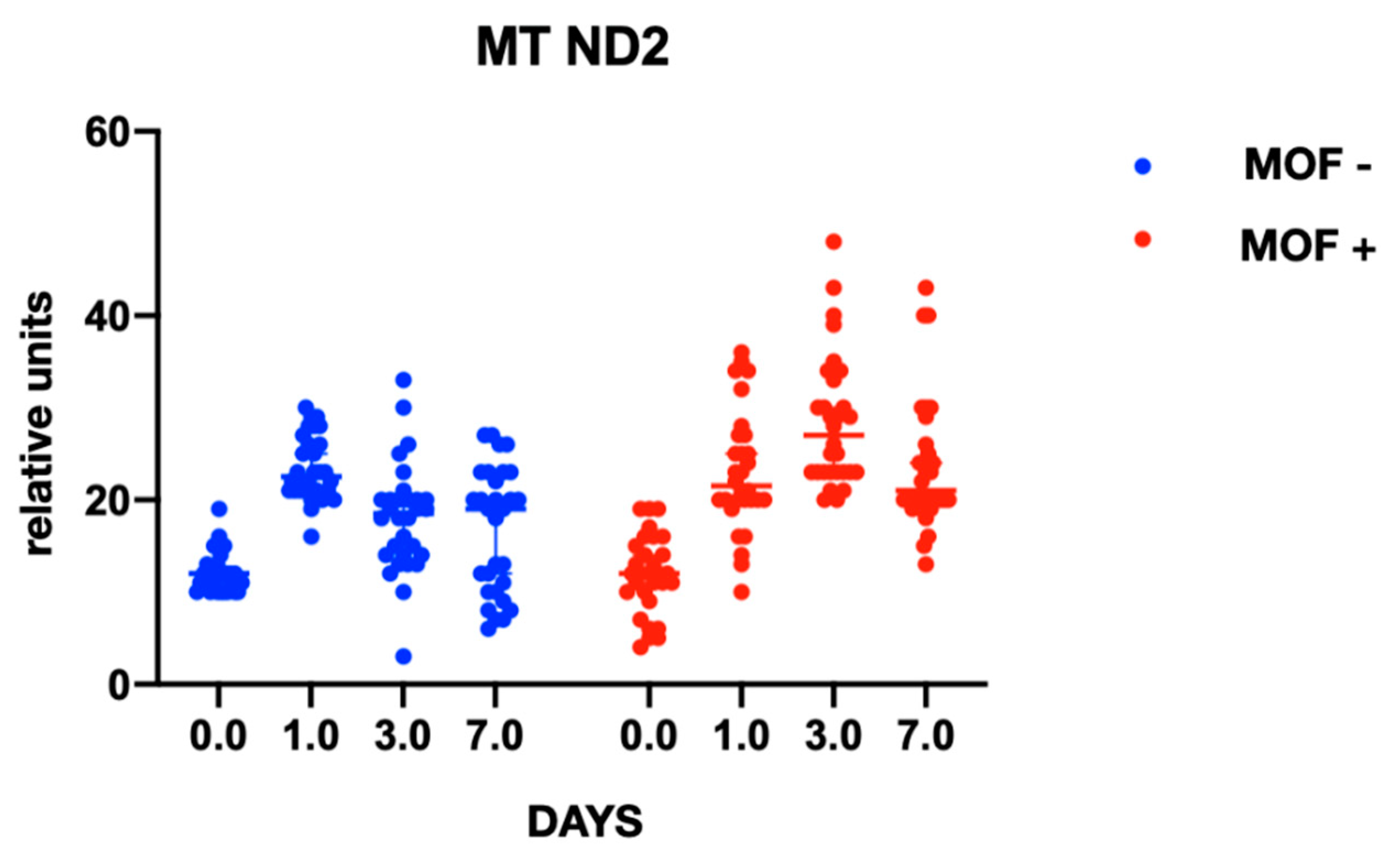
2.1. MtDNA Levels in Patients
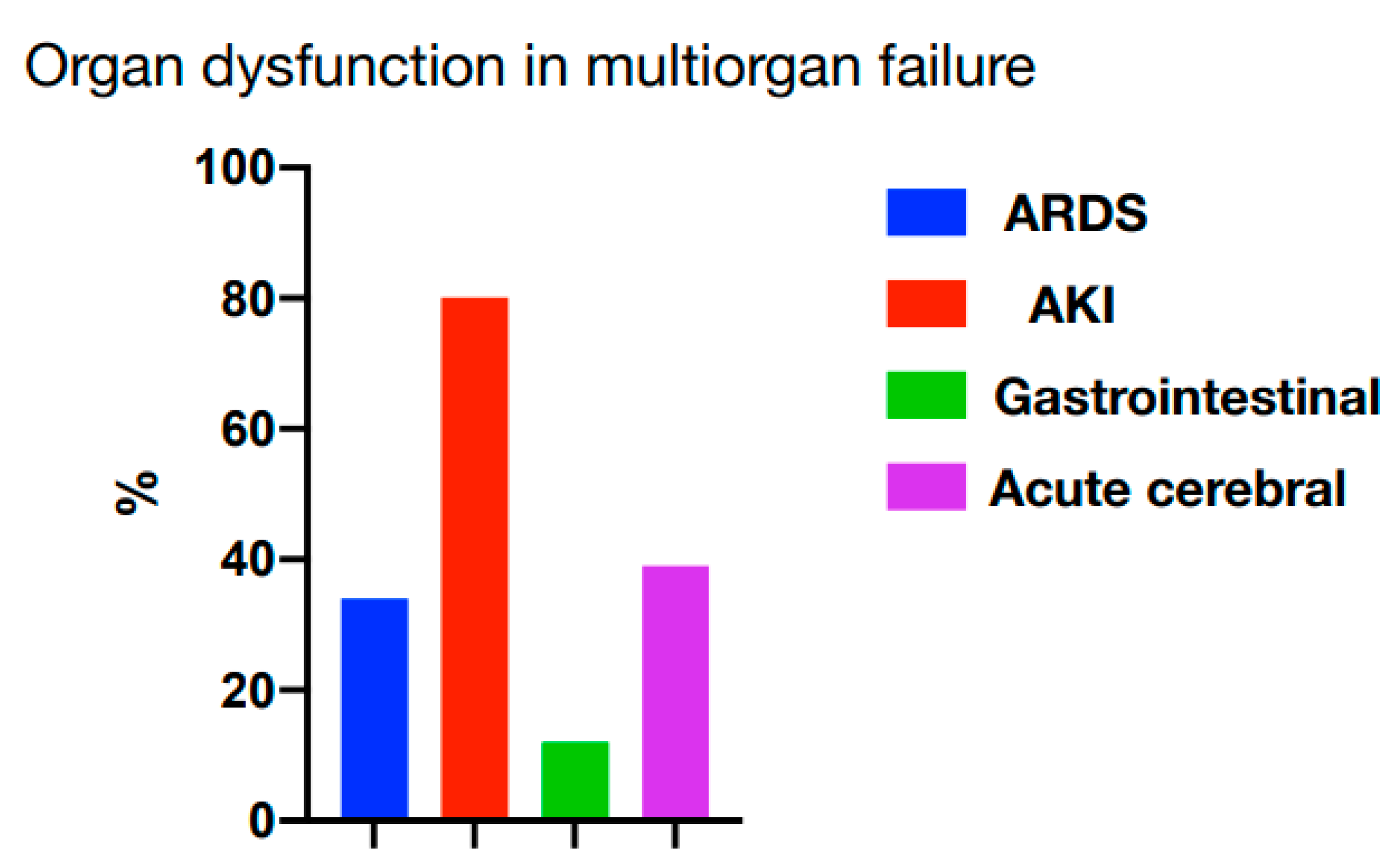
2.2. Features of MOF in Patients with Complications
3. Discussion
4. Material and Methods
4.1. Cohort Description
4.2. Blood Sampling
4.3. DNA Isolation and Quantitative mtDNA Analysis
4.4. Statistical Data Processing
5. Conclusions
- The level of mtDNA significantly increases in case of the development of MOF, regardless of its cause, in a small cohort of cardiac surgery patients.
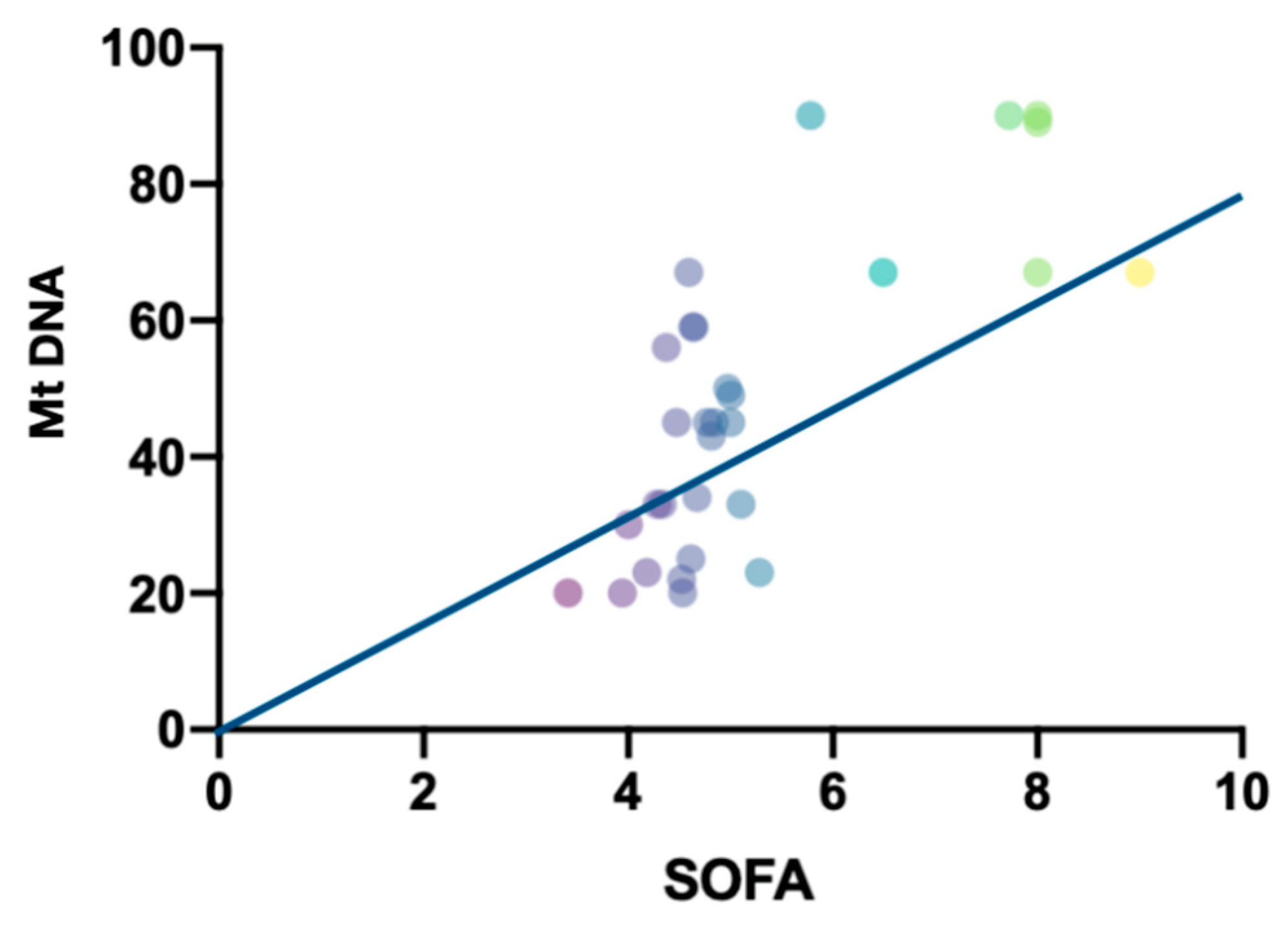
- The level of mtDNA correlates with the severity of MOF on the SOFA score.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| ADQI | Acute dialysis quality initiative |
| CAM-ICU | Confusion Assessment Method for Intensive Care Unit |
| SIRS | Systemic Inflammatory Response Syndrome |
| COX | Cytochrome oxidase |
| DAMP | Danger-associated molecular patterns |
| GAPDH | Glyceraldehyde 3-phosphate dehydrogenase |
| NADH | Nicotinamide adenine dinucleotide hydrogen |
| PAMP | Pathogen-associated molecular patterns |
| SOFA | Sequential Organ Failure Assessment |
References
- Bowdish, M.E.; D’Agostino, R.S.; Thourani, V.H.; Desai, N.; Shahian, D.M.; Fernandez, F.G.; Badhwar, V. The Society of Thoracic Surgeons Adult Cardiac Surgery Database: 2020 Update on Outcomes and Research. Ann. Thorac. Surg. 2020, 109, 1646–1655. [Google Scholar] [CrossRef]
- Golovkin, A.S.; Matveeva, V.G.; Khutornaya, M.V.; Ponasenko, A.V.; Shukevich, D.L.; Grigoryev, E.V. The role of serum cytokines in the pathogenesis of the systemic inflammatory response after coronary artery bypass grafting under extracorporeal circulation. Czitokiny’ I Vospal. 2015, 2, 48–55. (In Russian) [Google Scholar]
- Matveeva, V.G.; Golovkin, A.S.; Grigoryev, E.V.; Ponasenko, A.V. The role of a trigger receptor expressed on myeloid cells in the activation of innate immunity. Gen. Reanimatol. 2011, 3, 70–74. [Google Scholar] [CrossRef] [Green Version]
- Adzhigaliev, R.R.; Bautin, A.E.; Pasyuga, V.V. Influence of the components of general anesthesia on the systemic inflammatory response during cardiac surgery. Complex Issues Cardiovasc. Dis. 2019, 8, 145–152. [Google Scholar] [CrossRef] [Green Version]
- Riley, J.S.; Tait, S.W. Mitochondrial DNA in inflammation and immunity. EMBO Rep. 2020, 21, e49799. [Google Scholar] [CrossRef] [PubMed]
- Nakahira, K.; Hisata, S.; Choi, A.M. The roles of mitochondrial damage-associated molecular patterns in diseases. Antioxid. Redox Signal. 2015, 23, 1329–1350. [Google Scholar] [CrossRef] [Green Version]
- Knez, J.; Cauwenberghs, N.; Thijs, L.; Winckelmans, E.; Brguljan-Hitij, J.; Yang, W.Y.; Staessen, J.A.; Nawrot, T.S.; Kuznetsova, T. Association of left ventricular structure and function with peripheral blood mitochondrial DNA content in a general population. Int. J. Cardiol. 2016, 214, 180–188. [Google Scholar] [CrossRef]
- Ashar, F.N.; Zhang, Y.; Longchamps, R.J.; Lane, J.; Moes, A.; Grove, M.L.; Mychaleckyj, J.C.; Taylor, K.D.; Coresh, J.; Rotter, J.I.; et al. Association of Mitochondrial DNA Copy Number with Cardiovascular Disease. JAMA Cardiol. 2017, 2, 1247–1255. [Google Scholar] [CrossRef]
- Bayeva, M.; Gheorghiade, M.; Ardehali, H. Mitochondria as a therapeutic target in heart failure. J. Am. Coll. Cardiol. 2013, 61, 599–610. [Google Scholar] [CrossRef] [Green Version]
- Bliksøen, M.; Mariero, L.H.; Ohm, I.K.; Haugen, F.; Yndestad, A.; Solheim, S.; Seljeflot, I.; Ranheim, T.; Andersen, G.Ø.; Aukrust, P.; et al. Increased circulating mitochondrial DNA after myocardial infarction. Int. J. Cardiol. 2012, 158, 132–134. [Google Scholar] [CrossRef]
- Estevez-Cid, F.; Serrano-Teruel, M.E.; Fernandez-Rodriguez, F.; Bouzas-Mosquera, A.; Fernandez-Moreno, M.; Dieguez-Garcia, P.; Cuenca-Castillo, J.J.; Bautista-Hernandez, V. Postoperative Plasma Mitochondrial DNA and Cytokine Profiles of Elderly Patients Undergoing Minimally Invasive Aortic Valve Replacement. Thorac. Cardiovasc. Surg. 2019, 69, 034–042. [Google Scholar] [CrossRef] [PubMed]
- Ward, N.S.; Levy, M.M. (Eds.) Sepsis; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar] [CrossRef]
- Aslami, H.; Beurskens, C.J.; Tuip, A.M.; Horn, J.; Juffermans, N.P. Mitochondrial DNA A. DNA Mapp. Seq. Anal. 2018, 29, 525–528. [Google Scholar] [CrossRef]
- Gu, X.; Yao, Y.; Wu, G.; Lv, T.; Luo, L.; Song, Y. The plasma mitochondrial DNA is an independent predictor for post-traumatic systemic inflammatory response syndrome. PLoS ONE 2013, 8, e72834. [Google Scholar] [CrossRef] [PubMed]
- Barbarash, L.S.; Grigoryev, Y.V.; Plotnikov, G.P.; L, H.B.; Moiseyenkov, G.V.; Shukevich, D.L.; Ivanov, S.V.; Odarenko, Y.N. Multiple organ failure after cardiac surgery. Gen. Reanimatol. 2010, 6, 31. [Google Scholar] [CrossRef] [Green Version]
- Squiccimarro, E.; Labriola, C.; Malvindi, P.G.; Margari, V.; Guida, P.; Visicchio, G.; Kounakis, G.; Favale, A.; Dambruoso, P.; Mastrototaro, G.; et al. Prevalence and Clinical Impact of Systemic Inflammatory Reaction After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2019, 33, 1682–1690. [Google Scholar] [CrossRef]
- Khanova, M.Y.; Grigoryev, E.V. Role of PD-1 and PD-L1 receptors in the development of systemic inflammatory response and methods of immunoadjuvant therapy. Circ. Pathol. Card. Surg. 2019, 23, 76–83. [Google Scholar] [CrossRef]
- Qin, C.; Liu, R.; Gu, J.; Li, Y.; Qian, H.; Shi, Y.; Meng, W. Variation of perioperative plasma mitochondrial DNA correlate with peak inflammatory cytokines caused by cardiac surgery with cardiopulmonary bypass. J. Cardiothorac. Surg. 2015, 10, 85. [Google Scholar] [CrossRef] [Green Version]
- Gong, T.; Liu, L.; Jiang, W.; Zhou, R. DAMP-sensing receptors in sterile inflammation and inflammatory diseases. Nat. Rev. Immunol. 2020, 20, 95–112. [Google Scholar] [CrossRef]
- Khubutiya, M.S.; Shabanov, A.K.; Skulachev, M.V.; Bulava, G.V.; Savchenko, I.M.; Grebennikov, O.A.; Sergeev, A.A.; Zorov, D.B.; Zinovkin, R.A. Mitochondrial and nuclear DNA in patients with severe concomitant injury. Gen. Reanimatol. 2013, 9, 24. [Google Scholar] [CrossRef]
- Simmons, J.D.; Lee, Y.-L.; Mulekar, S.; Kuck, J.L.; Brevard, S.B.; Gonzalez, R.P.; Gillespie, M.N.; Richards, W.O. Elevated levels of plasma mitochondrial DNA DAMPs are linked to clinical outcome in severely injured human subjects. Ann. Surg. 2013, 4, 591–596. [Google Scholar] [CrossRef]
- Supinski, G.S.; Schroder, E.A.; Callahan, L.A. Mitochondria and Critical Illness. Chest 2020, 157, 310–322. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhou, W.; Wang, K.; He, S.; Chen, Y. Predictive value of circulating plasma mitochondrial DNA for Sepsis in the emergency department: Observational study based on the Sepsis-3 definition. BMC Emerg. Med. 2020, 20, 25. [Google Scholar] [CrossRef] [Green Version]
- Nakahira, K.; Kyung, S.Y.; Rogers, A.J.; Gazourian, L.; Youn, S.; Massaro, A.F.; Quintana, C.; Osorio, J.C.; Wang, Z.; Zhao, Y.; et al. Circulating mitochondrial DNA in patients in the ICU as a marker of mortality: Derivation and validation. PLoS Med. 2013, 10, e1001577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, H.P.; Li, M.; Lu, X.L.; Zhu, Y.M.; Ou-Yang, W.-X.; Xiao, Z.H.; Qiu, J.; Li, S.J. Use of plasma mitochondrial DNA levels for determining disease severity and prognosis in pediatric sepsis: A case control study. BMC Pediatr. 2018, 18, 267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneck, E.; Edinger, F.; Hecker, M.; Sommer, N.; Pak, O.; Weissmann, N.; Hecker, A.; Reichert, M.; Markmann, M.; Sander, M.; et al. Blood Levels of Free-Circulating Mitochondrial DNA in Septic Shock and Postsurgical Systemic Inflammation and Its Influence on Coagulation: A Secondary Analysis of a Prospective Observational Study. J. Clin. Med. 2020, 9, 2056. [Google Scholar] [CrossRef] [PubMed]
- Matveeva, V.G.; Khanova, M.Y.; Ivkin, A.A.; Kornelyuk, R.A.; Grigoryev, E.V. Immunosuppressive profile of patients operated on for acquired heart defects under cardiopulmonary bypass. Ann. Crit. Care 2020, 3, 74–87. [Google Scholar] [CrossRef]
- Pfeifer, R.; Kobbe, P.; Darwiche, S.S.; Billiar, T.R.; Pape, H.-C. Role of hemorrhage in the induction of systemic inflammation and remote organ damage: Analysis of combined pseudo-fracture and hemorrhagic shock. J. Orthop. Res. 2011, 29, 270–274. [Google Scholar] [CrossRef]
- Friesecke, S.; Träger, K.; Schittek, G.A.; Molnar, Z.; Bach, F.; Kogelmann, K.; Bogdanski, R.; Weyland, A.; Nierhaus, A.; Nestler, F.; et al. International registry on the use of the CytoSorb® adsorber in ICU patients. Med. Klin. Intensivmed. Notfmed. 2019, 114, 699–707. [Google Scholar] [CrossRef]
- Esteban, E.; Ferrer, R.; Alsina, L.; Artigas, A. Immunomodulation in sepsis: The role of endotoxin removal by polymyxin B-immobilized cartridge. Mediat. Inflamm. 2013, 2013, 507539. [Google Scholar] [CrossRef]
- Jansen, M.P.; Pulskens, W.P.; Butter, L.M.; Florquin, S.; Juffermans, N.P.; Roelofs, J.; Leemans, J.C. Mitochondrial DNA is released in urine of SIRS patients with acute kidney injury and correlates with severity of renal dysfunction. Shock 2018, 49, 301–310. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Patients without Complications (Group 1, n = 30) | Patients with Complications (Group 2, n = 30) | p |
|---|---|---|---|
| Age, years old | 57.2 (42.0–66.0) | 59.2 (48.0–66.9) | ns |
| Male, abs. (%) | 15 (50) | 15 (41.6) | ns |
| Body weight index, kg/m2 | 33.4 (32.1–35.2) | 36.4 (32.0–36.7) | ns |
| Comorbidity by CIRS, points | 9.6 (8.0–11.1) | 9.0 (8.9–11.5) | ns |
| Aortic valve surgery, abs (%) | 5 (16.6) | 7 (23) | ns |
| Mitral valve surgery, abs aбc. (%) | 6 (20) | 3 (10) | ns |
| Aortic + mitral valve surgery, abs (%) | 19 (63.4) | 20 (67) | ns |
| The reasons of MOF, abs (%): | |||
| Not applicable | 11 (36) 7 (23) 12 (41) | 0.0001 |
| The time of artificial circulation min | 121 (89–167) | 158 (101–201) | 0.001 |
| Aortic cross clump, min | 98 (90–122) | 108 (99–145) | ns |
| The need for transfusion after surgery, % | 0 | 100% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grigoriev, E.; Ponasenko, A.V.; Sinitskaya, A.V.; Ivkin, A.A.; Kornelyuk, R.A. Mitochondrial DNA as a Candidate Marker of Multiple Organ Failure after Cardiac Surgery. Int. J. Mol. Sci. 2022, 23, 14748. https://doi.org/10.3390/ijms232314748
Grigoriev E, Ponasenko AV, Sinitskaya AV, Ivkin AA, Kornelyuk RA. Mitochondrial DNA as a Candidate Marker of Multiple Organ Failure after Cardiac Surgery. International Journal of Molecular Sciences. 2022; 23(23):14748. https://doi.org/10.3390/ijms232314748
Chicago/Turabian StyleGrigoriev, Evgeny, Anastasia V. Ponasenko, Anna V. Sinitskaya, Artem A. Ivkin, and Roman A. Kornelyuk. 2022. "Mitochondrial DNA as a Candidate Marker of Multiple Organ Failure after Cardiac Surgery" International Journal of Molecular Sciences 23, no. 23: 14748. https://doi.org/10.3390/ijms232314748