
Serum Level of MMP-3 and MMP-9 in Patients with Diabetes Mellitus Type 2 Infected with Epstein-Barr Virus

 ,
,
Abstract
:1. Introduction
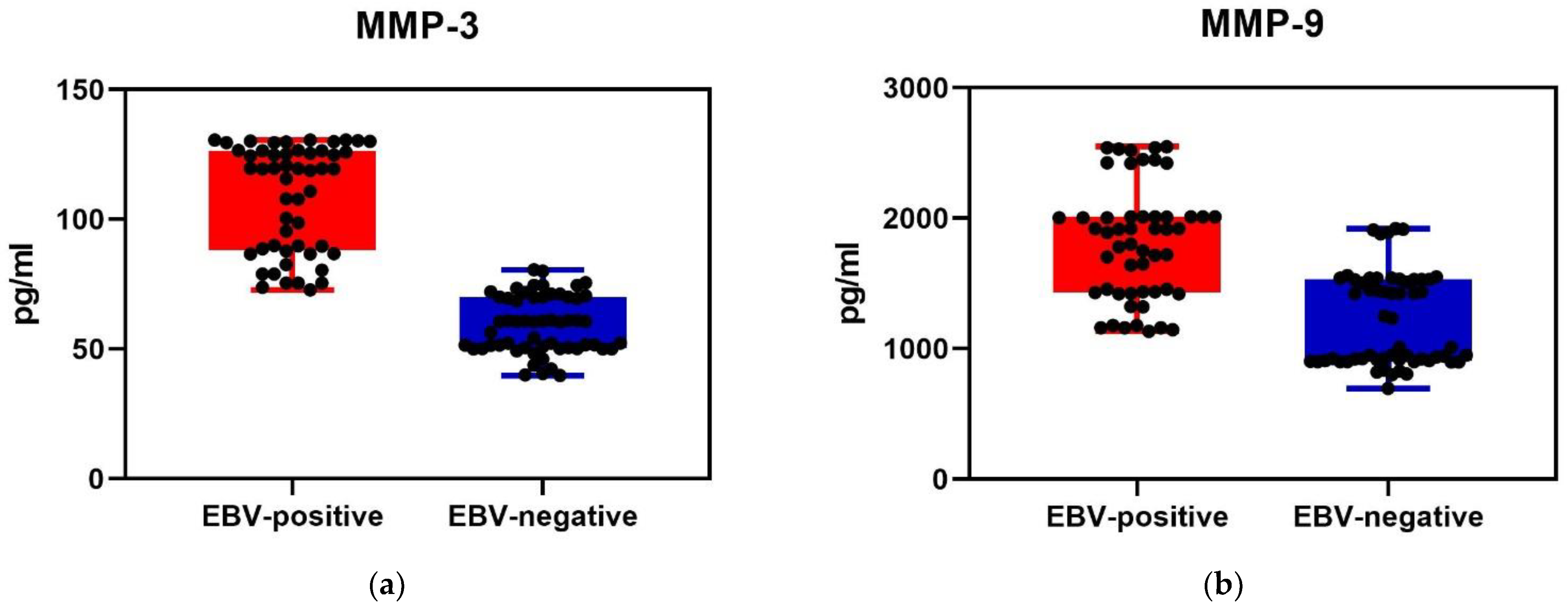
2. Results
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Clinical Specimens
4.3. Saliva Collection
4.4. Serum Collection
4.5. Molecular Methods
4.5.1. DNA Extraction from Saliva
4.5.2. EBV DNA Detection
4.5.3. MMP-3 and MMP-9
4.6. Statistical Analysis
4.7. Ethics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ogurtsova, K.; da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Guariguata, L.; Whiting, D.R.; Hambleton, I.; Beagley, J.; Linnenkamp, U.; Shaw, J.E. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res. Clin. Pract. 2014, 103, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Sonne, D.P.; Hemmingsen, B. Comment on American Diabetes Association. Standards of Medical Care in Diabetes—2017. Diabetes Care 2017; 40 (Suppl. 1): S1–S135. Diabetes Care 2017, 40, e92–e93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Handley, S.A. The virome: A missing component of biological interaction networks in health and disease. Genome Med. 2016, 8, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houghton, D.; Hardy, T.; Stewart, C.; Errington, L.; Day, C.P.; Trenell, M.I.; Avery, L. Systematic review assessing the effectiveness of dietary intervention on gut microbiota in adults with type 2 diabetes. Diabetologia 2018, 61, 1700–1711. [Google Scholar] [CrossRef] [Green Version]
- Nikolich-Zugich, J.; Goodrum, F.; Knox, K.; Smithey, M.J. Known unknowns: How might the persistent herpesvirome shape immunity and aging? Curr. Opin. Immunol. 2017, 48, 23–30. [Google Scholar] [CrossRef]
- Dworzański, J.; Drop, B.; Kliszczewska, E.; Strycharz-Dudziak, M.; Polz-Dacewicz, M. Prevalence of Epstein-Barr virus, human papillomavirus, cytomegalovirus and herpes simplex virus type 1 in patients with diabetes mellitus type 2 in south-eastern Poland. PLoS ONE 2019, 14, e0222607. [Google Scholar] [CrossRef]
- Casquiero, J.; Casquiero, J.; Alves, C. Infections in patients with diabete mellitus; A review of pathogenesis. Indian J. Endocrinol. Metab. 2012, 1, S27–S36. [Google Scholar]
- Cabral-Pacheco, G.A.; Garza-Veloz, I.; Castruita-De la Rosa, C.; Ramirez-Acuña, J.; Perez-Romero, B.A.; Guerrero-Rodriguez, J.F.; Martinez-Avila, N.; Martinez-Fierro, M.L. The Roles of Matrix Metalloproteinases and Their Inhibitors in Human Diseases. Int. J. Mol. Sci. 2020, 21, 9739. [Google Scholar] [CrossRef]
- Nagase, H.; Visse, R.; Murphy, G. Structure and function of matrix metalloproteinases and TIMPs. Cardiovasc. Res. 2006, 69, 562–573. [Google Scholar] [CrossRef] [Green Version]
- Caley, M.P.; Martins, V.L.; O’Toole, E.A. Metalloproteinases and wound healing. Adv. Wound Care 2015, 4, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Piskór, B.M.; Przylipiak, A.; Dąbrowska, E.; Niczyporuk, M.; Ławicki, S. Matrilysins and Stromelysins in Pathogenesis and Diagnostics of Cancers. Cancer Manag. Res. 2020, 12, 10949–10964. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, C.; Vaidya, S.; Wadhwan, V.; Kaur, G.; Pathak, A. Seesaw of matrix metalloproteinases (MMPs). J. Cancer Res. Ther. 2016, 12, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Barrichello, T.; Generoso, J.S.; Michelin, C.M.; Simões, L.R.; Elias, S.G.; Vuolo, F.; Comim, C.M.; Dal-Pizzol, F.; Quevedo, J. Inhibition of matrix metalloproteinases-2 and -9 prevents cognitive impairment caused by pneumococcal meningitis in Wistar rats. Exp. Biol. Med. 2014, 239, 225–231. [Google Scholar] [CrossRef]
- Overall, C.M. Regulation of tissue inhibitor of metalloproteinase expression. Ann. N. Y. Acad. Sci. 1994, 732, 51–64. [Google Scholar] [CrossRef]
- Papazafiropoulou, A.; Perrea, D.; Moyssakis, I.; Kokkinos, A.; Katsilambros, N.; Tentolouris, N. Plasma levels of MMP-2, MMP-9 and TIMP-1 are not associated with arterial stiffness in subjects with type 2 diabetes mellitus. J. Diabetes Complicat. 2010, 24, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Nagase, H.; Woessner, J.F., Jr. Matrix metalloproteinases. J. Biol. Chem. 1999, 274, 21491–21494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kupczyk, D.; Bilski, R.; Studzińska, R.; Woźniak, A. Assessment of the concentration of selected metalloproteinases (MMP-2, MMP-3, MMP-9 and MMP-13) in patients with ulcers as a complication of type 2 diabetes. Adv. Dermatol. Allergol. 2022, 39, 59–65. [Google Scholar] [CrossRef]
- Quintero-Fabián, S.; Arreola, R.; Becerril-Villanueva, E.; Torres-Romero, J.C.; Arana-Argáez, V.; Lara-Riegos, J.; Ramírez-Camacho, M.A.; Alvarez-Sánchez, M.E. Role of Matrix Metalloproteinases in Angiogenesis and Cancer. Front. Oncol. 2019, 9, 1370. [Google Scholar] [CrossRef] [Green Version]
- Gkouveris, I.; Nikitakis, N.G.; Aseervatham, J.; Rao, N.; Ogbureke, K.U.E. Matrix metalloproteinases in head and neck cancer: Current perspectives. Met. Med. 2017, 4, 47–61. [Google Scholar] [CrossRef] [Green Version]
- Niland, S.; Riscanevo, A.X.; Eble, J.A. Matrix Metalloproteinases Shape the Tumor Microenvironment in Cancer Progression. Int. J. Mol. Sci. 2021, 23, 146. [Google Scholar] [CrossRef] [PubMed]
- Lan, Y.Y.; Yeh, T.H.; Lin, W.H.; Wu, S.Y.; Lai, H.C.; Chang, F.H.; Takada, K.; Chang, Y. Epstein-Barr virus Zta upregulates matrix metalloproteinases 3 and 9 that synergistically promote cell invasion in vitro. PLoS ONE 2013, 8, e56121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshizaki, T.; Sato, H.; Furukawa, M.; Pagano, J.S. The expression of matrix metalloproteinase 9 is enhanced by Epstein–Barr virus latent membrane protein 1. Biol. Sci. 1998, 95, 3621–3626. [Google Scholar] [CrossRef] [Green Version]
- Uemura, S.; Matsushita, H.; Li, W.; Glassford, A.J.; Asagami, T.; Lee, K.H.; Harrison, D.G.; Tsao, P.S. Diabetes mellitus enhances vascular matrix metalloproteinase activity: Role of oxidative stress. Circ. Res. 2001, 88, 1291–1298. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.; Chen, Z.; Wang, L.; Wang, G.; Wang, Z.; Dong, X.B.; Wen, B.; Zhang, Z. The Pathogenesis of Diabetes Mellitus by Oxidative Stress and Inflammation: Its Inhibition by Berberine. Front. Pharmacol. 2018, 9, 782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oguntibeju, O.O. Type 2 diabetes mellitus, oxidative stress and inflammation: Examining the links. Int. J. Physiol. Pathophysiol. Pharmacol. 2019, 11, 45–63. [Google Scholar]
- Yang, Y.; Yin, L.; Liu, Q.; Sun, J.; Adami, H.O.; Ye, W.; Zhang, Z.; Fang, F. Hospital-Treated Infections and Increased Risk of Two EBV-Related Malignancies: A Nested Case-Control Study. Cancers 2022, 14, 3804. [Google Scholar] [CrossRef]
- Giovanuci, E.; Harlen, D.M.; Archer, M.C.; Bergenstal, R.M.; Gapstur, S.M.; Habel, L.; Pollak, M.; Regensteiner, J.G.; Yee, D. Diabetes and cancer. A consensus report. Diabetes Care 2010, 33, 1674–1685. [Google Scholar] [CrossRef] [Green Version]
- Yu, J. Introduction. In Obesity, Fatty Liver and Liver Cancer; Wong, C.C., Yu, J., Eds.; Advances in Experimental Medicine and Biology; Springer Nature: Singapore, 2018; pp. 1–2. [Google Scholar]
- Signorelli, S.S.; Malaponte, G.; Libra, M.; Di Pino, L.; Celotta, G.; Bevelacqua, V.; Petrina, M.; Nicotra, G.S.; Indelicato, M.; Navolanic, P.M.; et al. Plasma levels and zymographic activities of matrix metalloproteinases 2 and 9 in type II diabetics with peripheral arterial disease. Vasc. Med. 2005, 10, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Derosa, G.; D’Angelo, A.; Tinelli, C.; Devangelio, E.; Consoli, A.; Miccoli, R.; Penno, G.; Del Prato, S.; Paniga, S.; Cicero, A.F.G. Evaluation of metalloproteinase 2 and 9 levels and their inhibitors in diabetic and healthy subjects. Diabetes Metab. 2007, 33, 129–134. [Google Scholar] [CrossRef]
- Sampson, M.; Davies, I.; Gavrilovic, J.; Sussams, B.; Brown, J.; Astley, S.; Hughes, D.A. Plasma matrix metalloproteinases, low density lipoprotein oxidisability and soluble adhesion molecules after a glucose load in Type 2 diabetes. Cardiovasc. Diabetol. 2004, 3, 7. [Google Scholar] [CrossRef] [Green Version]
- Ritter, A.M.V.; de Faria, A.P.; Barbaro, N.; Sabbatini, A.R.; Corrêa, N.B.; Brunelli, V.; Amorim, R.; Modolo, R.; Moreno, H. Crosstalk between obesity and MMP-9 in cardiac remodelling -a cross-sectional study in apparent treatment-resistant hypertension. Blood Press 2017, 26, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Chavey, C.; Mari, B.; Monthouel, M.-N.; Bonnafous, S.; Anglard, P.; Van Obberghen, E.; Tartare-Deckert, S. Matrix metalloproteinases are differentially expressed in adipose tissue during obesity and modulate adipocyte differentiation. J. Biol. Chem. 2003, 278, 11888–11896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derosa, G.; Ferrari, I.; D’Angelo, A.; Tinelli, C.; Salvadeo, S.A.T.; Ciccarelli, L.; Piccinni, M.N.; Gravina, A.; Ramondetti, F.; Maffioli, P.; et al. Matrix metalloproteinase-2 and -9 levels in obese patients. Endothélium 2008, 15, 219–224. [Google Scholar] [CrossRef]
- Śliwowska, I.; Kopczyński, Z. Matrix metalloproteinases—Biochemical characteristics and clinical value determination in breast cancer patients. Contemp. Oncol. 2005, 9, 327–335. [Google Scholar]
- Galliera, E.; Tacchini, L.; Corsi Romanelli, M.M. Matrix metalloproteinases as biomarkers of disease: Updates and new insights. Clin. Chem. Lab. Med. 2015, 53, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.; Wu, G.; Li, S.; Weinberg, E.M.; Kumthip, K.; Peng, L.F.; Méndez-Navarro, J.; Chen, W.-C.; Jilg, N.; Zhaoet, H.; et al. HIV and HCV cooperatively promote hepatic fibrogenesis via induction of reactive oxygen species and NFkappaB. J. Biol. Chem. 2011, 286, 2665–2674. [Google Scholar] [CrossRef] [Green Version]
- Zuo, X.; Pan, W.; Feng, T.; Shi, X.; Dai, J. Matrix metalloproteinase 3 promotes cellular anti-dengue virus response via interaction with transcription factor NFkappaB in cell nucleus. PLoS ONE 2014, 9, e84748. [Google Scholar] [CrossRef]
- Li, Y.; Feng, Z.; Xing, S.; Liu, W.; Zhang, G. Combination of serum matrix metalloproteinase-3 activity and EBV antibodies improves the diagnostic performance of nasopharyngeal carcinoma. J. Cancer 2020, 11, 6009–6018. [Google Scholar] [CrossRef]
- Polz-Dacewicz, M.; Strycharz-Dudziak, M.; Dworzanski, J.; Stec, A.; Kocot, J. Salivary and serum IL-10, TNF-α, TGF-β, VEGF levels in oropharyngeal squamous cell carcinoma and correlation with HPV and EBV infection. Infect. Agent Cancer 2016, 11, 45. [Google Scholar] [CrossRef] [Green Version]
- Foltyn, S.; Strycharz-Dudziak, M.; Drop, B.; Boguszewska, A.; Polz-Dacewicz, M. Serum EBV antibodies and LMP-1 in Polish patients with oropharyngeal and laryngeal cancer. Infect. Agents Cancer 2017, 12, 31. [Google Scholar] [CrossRef] [PubMed]
- Polz-Dacewicz, M.; Macieląg, P.; Kliszczewska, E.; Rolniak, Ł. Serum and saliva levels of matrix metalloproteinase 3 and 9 in pharynx and larynx cancer. J. Pre-Clin. Clin. Res. 2017, 11, 106–110. [Google Scholar] [CrossRef]


{kind=link}
| EBV-Positive N = 55 | EBV-Negative N = 60 | p | |||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Sex | |||||
| Male | 23 | 41.8 | 24 | 40.0 | >0.05 |
| Female | 32 | 58.2 | 36 | 60.0 | |
| Age | |||||
| 20–39 | 7 | 12.7 | 8 | 13.3 | >0.05 |
| 40–59 | 20 | 36.4 | 22 | 36.7 | |
| 60+ | 28 | 50.9 | 30 | 50.0 | |
| Place of residence | |||||
| Urban | 23 | 41.8 | 24 | 40.0 | >0.05 |
| Rural | 32 | 58.2 | 36 | 60.0 | |
| Smoking | |||||
| Yes | 34 | 61.8 | 38 | 63.3 | >0.05 |
| No | 21 | 38.2 | 22 | 36.7 | |
| Alcohol abuse | |||||
| Yes | 35 | 63.6 | 36 | 60.0 | >0.05 |
| No | 20 | 36.4 | 24 | 40.0 | |
| BMI | |||||
| 18.5–24.9 | 9 | 16.4 | 11 | 18.3 | >0.05 |
| 25–29.9 | 14 | 25.5 | 16 | 26.7 | |
| 30–39.9 | 32 | 58.1 | 33 | 55.0 | |
| Duration of diabetes (years) | |||||
| 1–5 | 11 | 20.0 | 13 | 21.7 | >0.05 |
| 6–10 | 14 | 25.5 | 15 | 25.0 | |
| >10 | 30 | 54.5 | 32 | 53.3 | |
| BMI | MMP-3 [pg/mL] | MMP-9 [pg/mL] |
|---|---|---|
| 18.5–24.9 | 82.3 +/− 5.9 | 1303.0 +/− 128.7 |
| 25.0–29.9 | 108.5 +/− 16.3 | 1741.5 +/− 255.2 |
| 30.0–39.9 | 128.6 +/− 2.0 | 2307.5 +/− 240.9 |
| p value * | 10−4 | 10−4 |
| Duration of diabetes (years) | ||
| 6–10 | 90.3 +/− 13.7 | 1440.4 +/− 226.5 |
| >10 | 125.7 +/− 4.3 | 2160.9 +/− 258.4 |
| p value ** | 10−6 | 10−6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stępień, E.; Dworzański, J.; Dworzańska, A.; Drop, B.; Polz-Dacewicz, M. Serum Level of MMP-3 and MMP-9 in Patients with Diabetes Mellitus Type 2 Infected with Epstein-Barr Virus. Int. J. Mol. Sci. 2022, 23, 13599. https://doi.org/10.3390/ijms232113599
Stępień E, Dworzański J, Dworzańska A, Drop B, Polz-Dacewicz M. Serum Level of MMP-3 and MMP-9 in Patients with Diabetes Mellitus Type 2 Infected with Epstein-Barr Virus. International Journal of Molecular Sciences. 2022; 23(21):13599. https://doi.org/10.3390/ijms232113599
Chicago/Turabian StyleStępień, Ewa, Jakub Dworzański, Anna Dworzańska, Bartłomiej Drop, and Małgorzata Polz-Dacewicz. 2022. "Serum Level of MMP-3 and MMP-9 in Patients with Diabetes Mellitus Type 2 Infected with Epstein-Barr Virus" International Journal of Molecular Sciences 23, no. 21: 13599. https://doi.org/10.3390/ijms232113599