
Cyclic Nigerosyl-Nigerose as Oxygen Nanocarrier to Protect Cellular Models from Hypoxia/Reoxygenation Injury: Implications from an In Vitro Model

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Results
2.1. In Vitro Oxygen Release Kinetics
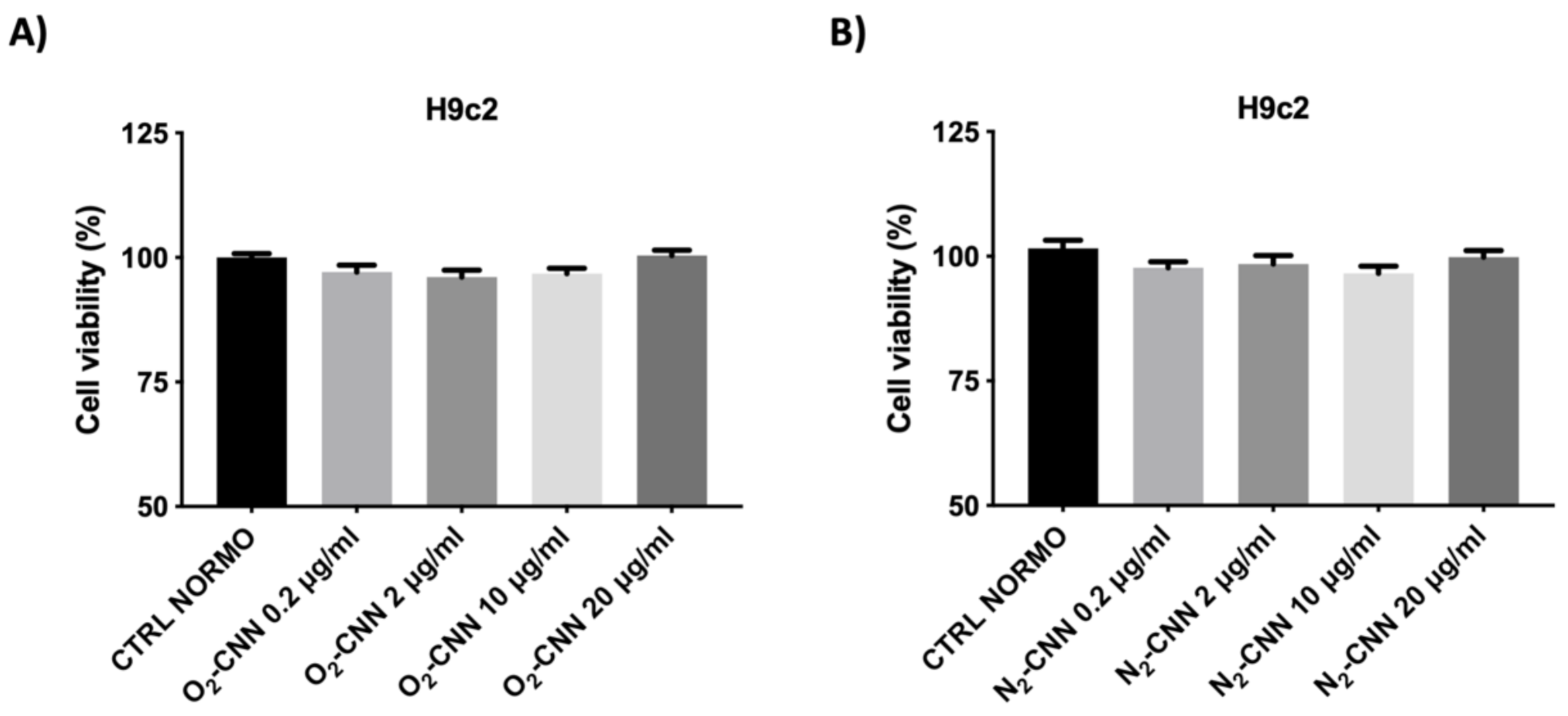
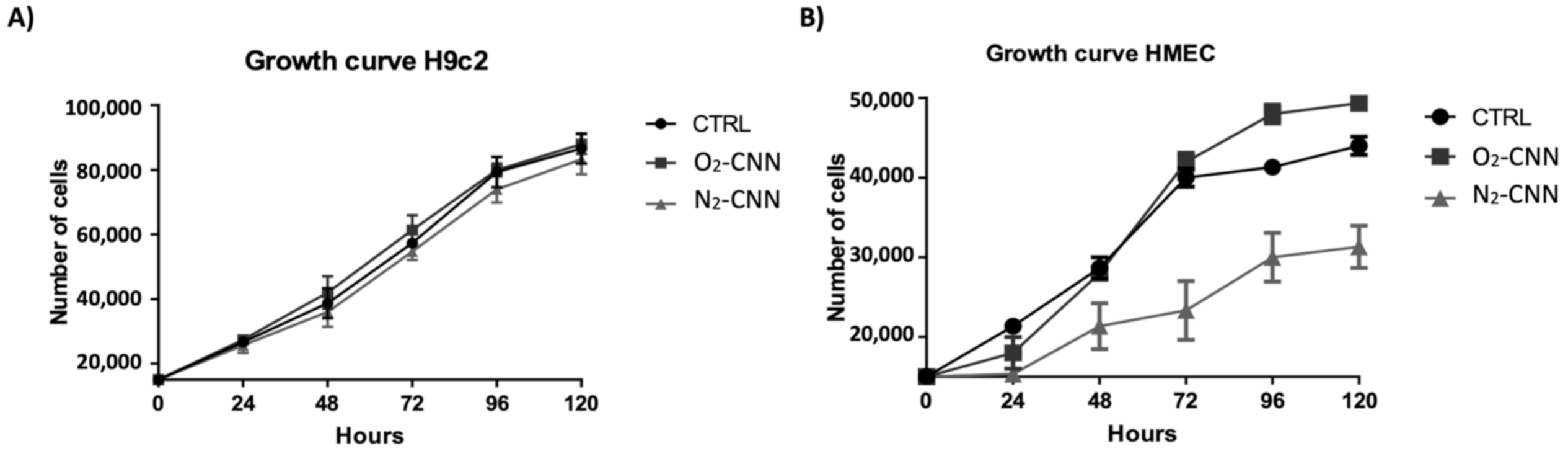
2.2. Dose–Response and Growth Curve in Normoxic Conditions
2.3. Untreated Cells: Normoxic and H/R Conditions
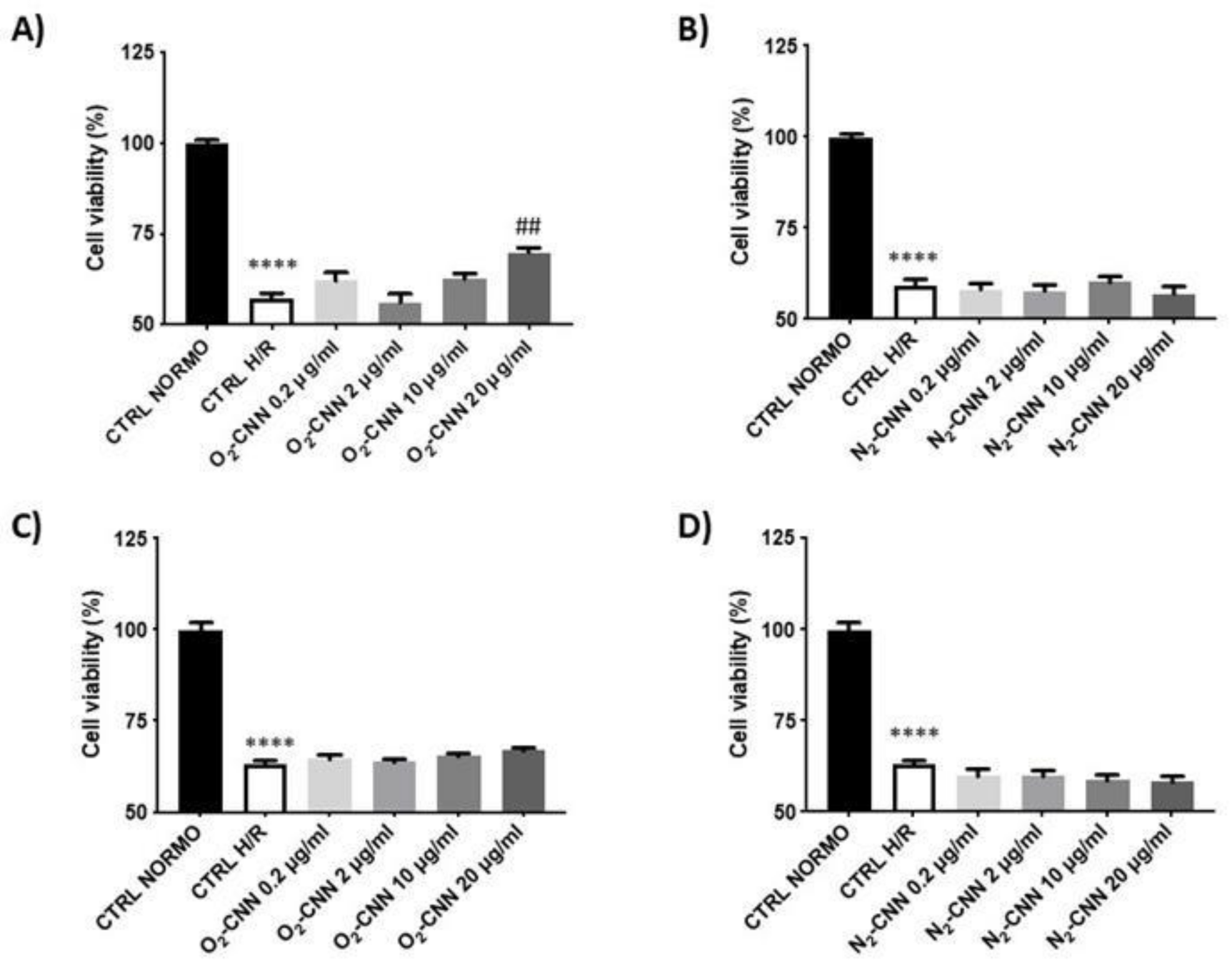
2.4. CNN-Pre-Treated Cells in H/R Conditions
2.5. CNN Post-Treated Cells in H/R Conditions
3. Discussion
4. Materials and Methods
4.1. Preparation and Characterization of Oxygen-Loaded Cyclic Nigerosyl-Nigerose Solution
4.2. Hemolytic Activity Determination
4.3. In Vitro Oxygen Release Kinetics from Oxygen-Loaded Nigerose Solution
4.4. Cellular Model
4.5. Protocols
4.5.1. Normoxic Experimental Conditions (Dose–Response Studies and Growth Curve)
4.5.2. Experimental Conditions of Untreated, and Pre- and Post-Treated, Cells in Hypoxia/Reoxygenation
4.6. MTT Assay
4.7. Western Blot Analysis 346
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HF | Heart failure |
| MI | Myocardial ischemia |
| IRI | Ischemia/reperfusion injury |
| CNN | Cyclic nigerosyl-nigerose |
| O2-CNN | Oxygen CNN |
| N2-CNN | Nitrogen CNN |
| H9c2 | Cardiomyoblast |
| HMEC | Human microvascular endothelial cells |
| H/R | Hypoxia/reoxygenation |
| MTT | 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide |
| IB | Ischemic buffer |
| ROS | Radical oxygen species |
| AMI | Acute myocardial infarction |
References
- Su, S.; Kang, P.M. Recent Advances in Nanocarrier-Assisted Therapeutics Delivery Systems. Pharmaceutics 2020, 12, E837. [Google Scholar] [CrossRef] [PubMed]
- Pagliaro, P.; Penna, C. Redox signaling and cardioprotection: Translatability and mechanism. Br. J. Pharmacol. 2015, 172, 1974–1995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hausenloy, D.J.; Yellon, D.M. Ischaemic conditioning and reperfusion injury. Nat. Rev. Cardiol. 2016, 13, 193–209. [Google Scholar] [CrossRef] [PubMed]
- Pagliaro, P.; Moro, F.; Tullio, F.; Perrelli, M.G.; Penna, C. Cardioprotective pathways during reperfusion: Focus on redox signaling and other modalities of cell signaling. Antioxid. Redox Signal. 2011, 14, 833–850. [Google Scholar] [CrossRef] [Green Version]
- Tullio, F.; Angotti, C.; Perrelli, M.G.; Penna, C.; Pagliaro, P. Redox balance, and cardioprotection. Basic Res. Cardiol. 2013, 108, 392. [Google Scholar] [CrossRef] [Green Version]
- Evans, C.W.; Iyer, K.S.; Hool, L.C. The potential for nanotechnology to improve delivery of therapy to the acute ischemic heart. Nanomedicine 2016, 11, 817–832. [Google Scholar] [CrossRef] [Green Version]
- Penna, C.; Rastaldo, R.; Mancardi, D.; Raimondo, S.; Cappello, S.; Gattullo, D.; Losano, G.; Pagliaro, P. Post–conditioning induced cardioprotection requires signaling through a redox-sensitive mechanism, mitochondrial ATP–sensitive K+ channel and protein kinase C activation. Basic Res. Cardiol. 2006, 101, 180–189. [Google Scholar] [CrossRef]
- Tsutsumi, Y.M.; Yokoyama, T.; Horikawa, Y.; Roth, D.M.; Patel, H.H. Reactive oxygen species trigger ischemic and pharmacological postconditioning: In vivo and in vitro characterization. Life Sci. 2007, 81, 1223–1227. [Google Scholar] [CrossRef] [Green Version]
- Vinten-Johansen, J.; Granfeldt, A.; Mykytenko, J.; Undyala, V.V.; Dong, Y.; Przyklenk, K. The multidimensional physiological responses to postconditioning. Antioxid. Redox Signal. 2011, 14, 791–810. [Google Scholar] [CrossRef]
- Martins-Marques, T.; Hausenloy, D.J.; Sluijter, J.P.G.; Leybaert, L.; Girao, H. Intercellular Communication in the Heart: Therapeutic Opportunities for Cardiac Ischemia. Trends Mol. Med. 2020, 27, 248–262. [Google Scholar] [CrossRef]
- Serviddio, G.; Bellanti, F.; Sastre, J.; Vendemiale, G.; Altomare, E. Targeting mitochondria: A new promising approach for the treatment of liver diseases. Curr. Med. Chem. 2010, 17, 2325–2337. [Google Scholar] [CrossRef]
- Lakshmanan, R.; Ukani, G.; Rishi, M.T.; Maulik, N. Trimodal rescue of hind limb ischemia with growth factors, cells, and nanocarriers: Fundamentals to clinical trials. Can. J. Physiol. Pharmacol. 2017, 95, 1125–1140. [Google Scholar] [CrossRef] [Green Version]
- Bar, A.; Cohen, S. Inducing Endogenous Cardiac Regeneration: Can Biomaterials Connect the Dots? Front. Bioeng. Biotechnol. 2020, 8, 126. [Google Scholar] [CrossRef] [Green Version]
- Davidson, S.M.; Andreadou, I.; Barile, L.; Birnbaum, Y.; Cabrera-Fuentes, H.A.; Cohen, M.V.; Downey, J.M.; Girao, H.; Pagliaro, P.; Penna, C.; et al. Circulating blood cells and extracellular vesicles in acute cardioprotection. Cardiovasc. Res. 2019, 115, 1156–1166. [Google Scholar] [CrossRef]
- Femminò, S.; Penna, C.; Bessone, F.; Caldera, F.; Dhakar, N.; Cau, D.; Pagliaro, P.; Cavalli, R.; Trotta, F. α-Cyclodextrin and α-Cyclodextrin Polymers as Oxygen Nanocarriers to Limit Hypoxia/Reoxygenation Injury: Implications from an In Vitro Model. Polymers 2018, 10, 211. [Google Scholar] [CrossRef] [Green Version]
- Caldera, F.; Argenziano, M.; Trotta, F.; Dianzani, C.; Gigliotti, L.; Tannous, M.; Pastero, L.; Aquilano, D.; Nishimoto, T.; Higashiyama, T.; et al. Cyclic nigerosyl-1,6-nigerose-based nanosponges: An innovative pH and time-controlled nanocarrier for improving cancer treatment. Carbohydr. Polym. 2018, 194, 111–121. [Google Scholar] [CrossRef]
- Sezer, M.; van Royen, N.; Umman, B.; Bugra, Z.; Bulluck, H.; Hausenloy, D.J.; Umman, S. Coronary Microvascular Injury in Reperfused Acute Myocardial Infarction: A View from an Integrative Perspective. J. Am. Heart Assoc. 2018, 7, e009949. [Google Scholar] [CrossRef] [Green Version]
- Bøtker, H.E.; Hausenloy, D.; Andreadou, I.; Antonucci, S.; Boengler, K.; Davidson, S.M.; Deshwal, S.; Devaux, Y.; Di Lisa, F.; Di Sante, M.; et al. Practical guidelines for rigor and reproducibility in preclinical and clinical studies on cardioprotection. Basic Res. Cardiol. 2018, 113, 39. [Google Scholar] [CrossRef] [Green Version]
- Cavalli, R.; Akhter, A.K.; Bisazza, A.; Giustetto, P.; Trotta, F.; Vavia, P. Nanosponge formulations as oxygen delivery systems. Int. J. Pharm. 2010, 402, 254–257. [Google Scholar] [CrossRef]
- Cavalli, R.; Bisazza, A.; Giustetto, P.; Civra, A.; Lembo, D.; Trotta, G.; Guiot, C.; Trotta, M. Preparation and characterization of dextran nanobubbles for oxygen delivery. Int. J. Pharm. 2009, 381, 160–165. [Google Scholar] [CrossRef] [Green Version]
- Cavalli, R.; Bisazza, A.; Rolfo, A.; Balbis, S.; Madonnaripa, D.; Caniggia, I.; Guiot, C. Ultrasound-mediated oxygen delivery from chitosan nanobubbles. Int. J. Pharm. 2009, 378, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Magnetto, C.; Prato, M.; Khadjavi, A.; Giribaldi, G.; Fenoglio, I.; Jose, J.; Gulino, G.R.; Cavallo, F.; Quaglino, E.; Benintende, E.; et al. Ultrasound-activated decafluoropentane-cored and chitosan-shelled nanodroplets for oxygen delivery to hypoxic cutaneous tissues. RCS Adv. 2014, 4, 38433–38441. [Google Scholar] [CrossRef]
- Prato, M.; Magnetto, C.; Jose, J.; Khadjavi, A.; Cavallo, F.; Quaglino, E.; Panariti, A.; Rivolta, I.; Benintende, E.; Varetto, G.; et al. 2H, 3H-decafluoropentane-based nanodroplets: New perspectives for oxygen delivery to hypoxic cutaneous tissues. PLoS ONE 2015, 10, e0119769. [Google Scholar] [CrossRef] [PubMed]
- Doyle, B. There will be blood. JACC Cardiovasc. Interv. 2009, 2, 54–55. [Google Scholar] [CrossRef] [Green Version]
- Tullio, F.; Penna, C.; Cabiale, K.; Femminò, S.; Galloni, M.; Pagliaro, P. Cardioprotective effects of calcitonin gene-related peptide in isolated rat heart and in H9c2 cells via redox signaling. Biomed. Pharmacother. 2017, 90, 194–202. [Google Scholar] [CrossRef]
- Pasqua, T.; Tota, B.; Penna, C.; Corti, A.; Cerra, M.C.; Loh, Y.P.; Angelone, T. pGlu-serpinin protects the normotensive and hypertensive heart from ischemic injury. J. Endocrinol. 2015, 227, 167–178. [Google Scholar] [CrossRef] [Green Version]
- Basilico, N.; Mondani, M.; Parapini, S.; Speciale, L.; Ferrante, P.; Taramelli, D. Plasmodium falciparum parasitized red blood cells modulate the production of endothelin-1 by human endothelial cells. Minerva Med. 2004, 95, 153–158. [Google Scholar]
- Penna, C.; Femminò, S.; Tapparo, M.; Lopatina, T.; Fladmark, K.E.; Ravera, F.; Comità, S.; Alloatti, G.; Giusti, I.; Dolo, V.; et al. The Inflammatory Cytokine IL-3 Hampers Cardioprotection Mediated by Endothelial Cell-Derived Extracellular Vesicles Possibly via Their Protein Cargo. Cells 2020, 10, 13. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cyclic Nigerosyl-Nigerose (4% w/v) in NaCl (0.9% w/v) | Cyclic Nigerosyl-Nigerose (4% w/v) in Glycerol (2% w/v) + Dextran-70 (6% w/v) | Glucose (5% w/v) + Dextran-70 (6% w/v) | |
|---|---|---|---|
| pH | 6.00 | 6.05 | 5.85 |
| Osmolarity (mOsm) | 310 | 300 | 280 |
| Viscosity (cP) | 1.07 | 2.30 | 3.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Penna, C.; Femminò, S.; Caldera, F.; Rubin Pedrazzo, A.; Cecone, C.; Alfì, E.; Comità, S.; Higashiyama, T.; Trotta, F.; Pagliaro, P.; et al. Cyclic Nigerosyl-Nigerose as Oxygen Nanocarrier to Protect Cellular Models from Hypoxia/Reoxygenation Injury: Implications from an In Vitro Model. Int. J. Mol. Sci. 2021, 22, 4208. https://doi.org/10.3390/ijms22084208
Penna C, Femminò S, Caldera F, Rubin Pedrazzo A, Cecone C, Alfì E, Comità S, Higashiyama T, Trotta F, Pagliaro P, et al. Cyclic Nigerosyl-Nigerose as Oxygen Nanocarrier to Protect Cellular Models from Hypoxia/Reoxygenation Injury: Implications from an In Vitro Model. International Journal of Molecular Sciences. 2021; 22(8):4208. https://doi.org/10.3390/ijms22084208
Chicago/Turabian StylePenna, Claudia, Saveria Femminò, Fabrizio Caldera, Alberto Rubin Pedrazzo, Claudio Cecone, Edoardo Alfì, Stefano Comità, Takanobu Higashiyama, Francesco Trotta, Pasquale Pagliaro, and et al. 2021. "Cyclic Nigerosyl-Nigerose as Oxygen Nanocarrier to Protect Cellular Models from Hypoxia/Reoxygenation Injury: Implications from an In Vitro Model" International Journal of Molecular Sciences 22, no. 8: 4208. https://doi.org/10.3390/ijms22084208