
Propolis and Diet Rich in Polyphenols as Cariostatic Agents Reducing Accumulation of Dental Plaque

 , ,
, ,
Abstract
:1. Introduction
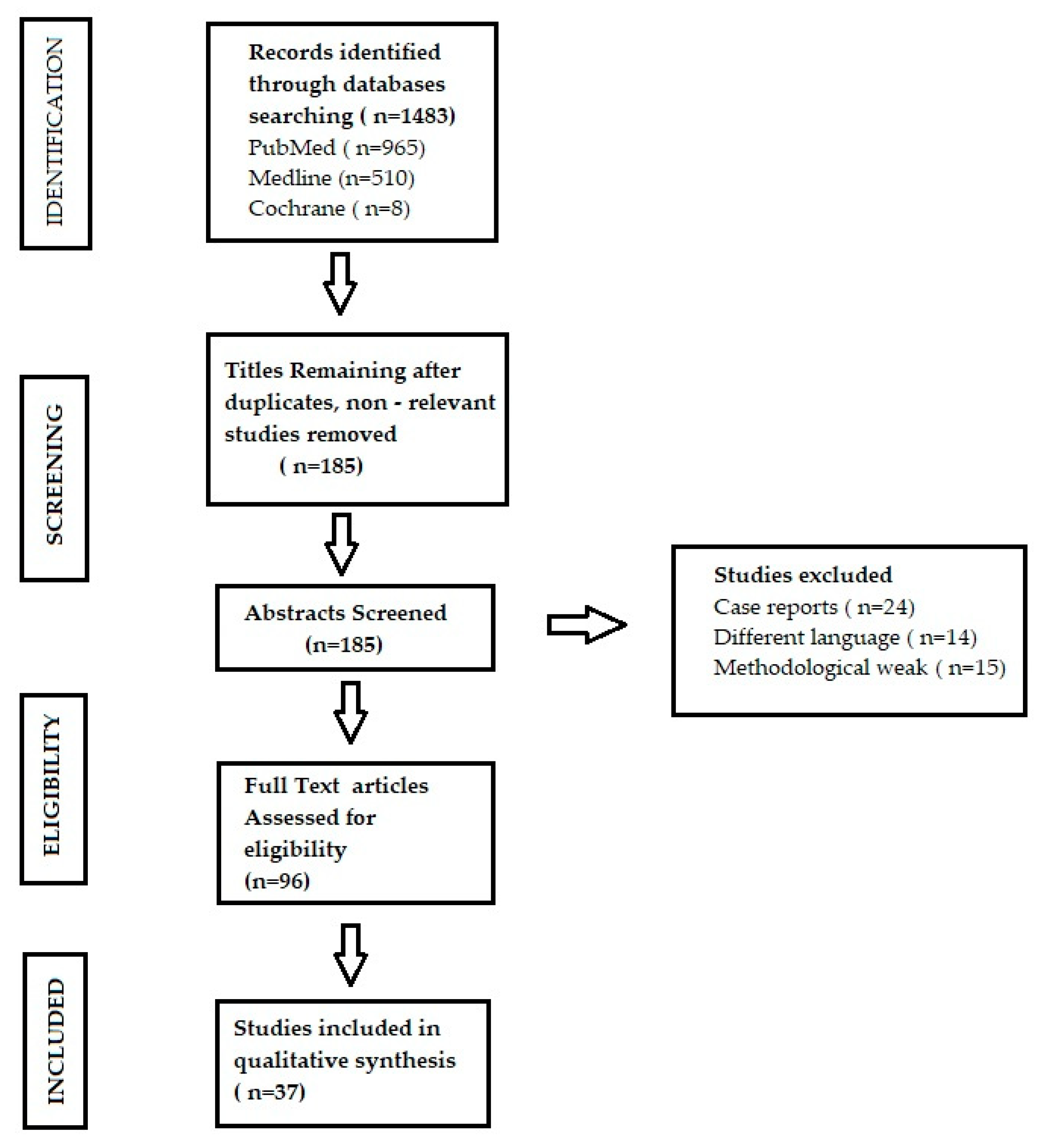
2. Materials and Methods
- observational studies evaluating the association between dental plaque and systemic diseases
- randomized clinical trials (RCTs) and observational studies evaluating the impact of propolis on hygiene of oral cavity
- randomized clinical trials (RCTs) and reviews presenting the impact of food rich in polyphenols in prophylaxis of dental plaque accumulation
- case reports
- articles published in other languages than Polish and English.
- Is there an association between dental plaque and systemic diseases?
- Can propolis play a role as a cariostatic agent?
- What is the impact of diet containing polyphenols on oral cavity microbiome?
3. The Results
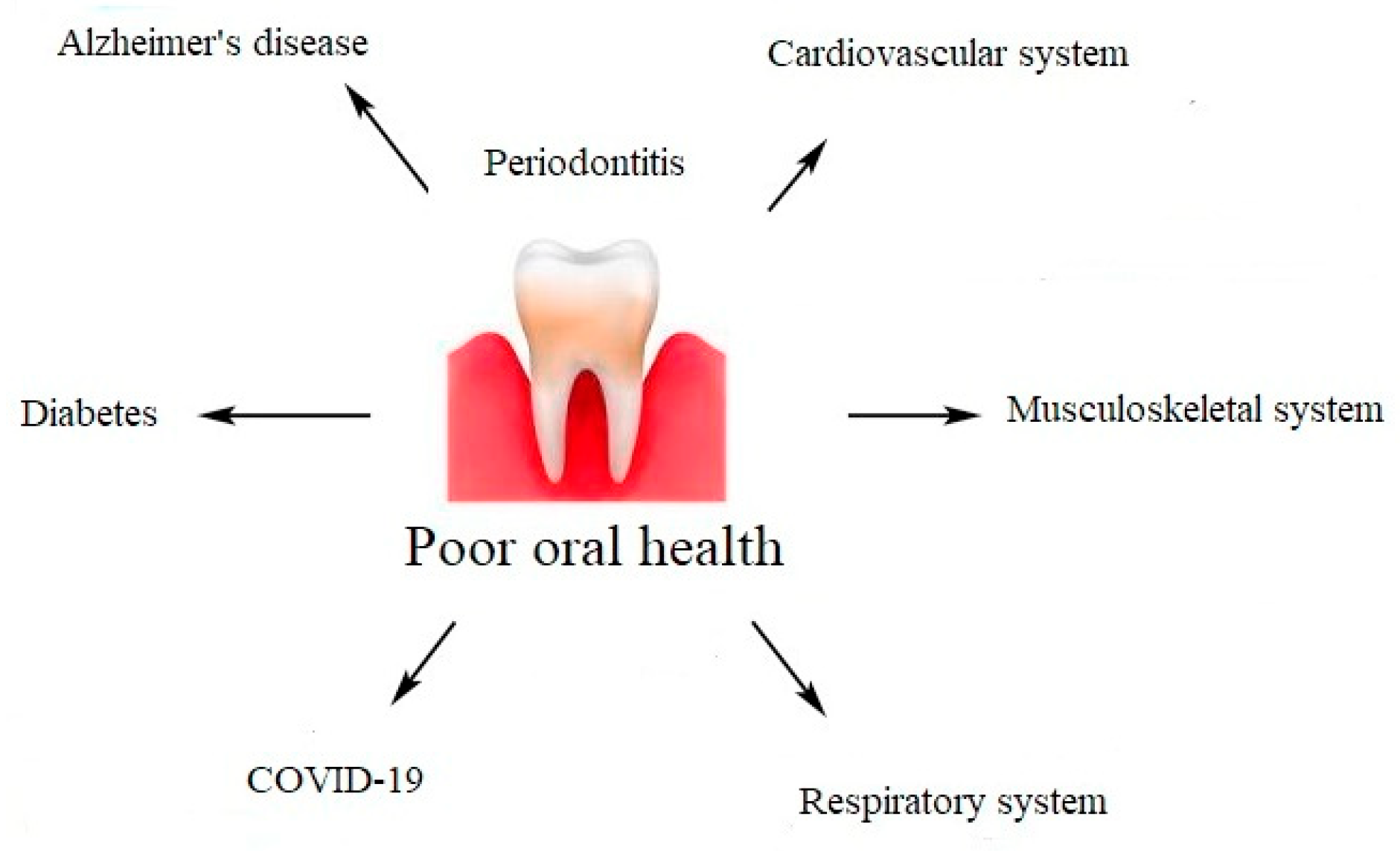
3.1. The Role of Dental Plaque in the Course of Systemic Diseases and SARS-CoV-2 Infection
3.1.1. Cardiovascular System
3.1.2. Musculoskeletal System
3.1.3. Respiratory System and SARS-CoV-2 Infection
3.1.4. Diabetes
3.1.5. Alzheimer’s Disease

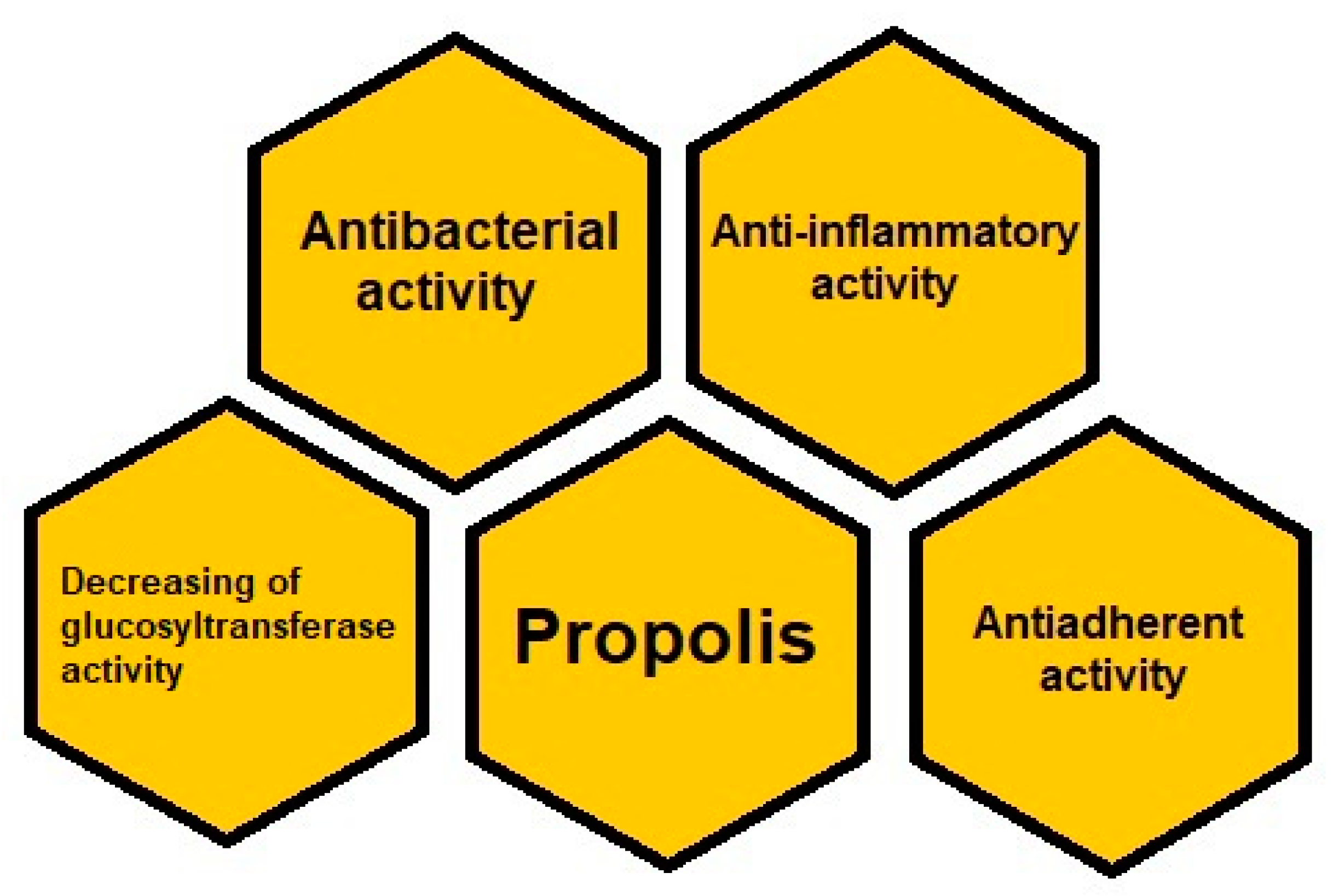
3.2. Propolis as a Therapeutic Agent in Dentistry
3.3. The Role of a Diet in the Reduction of the Dental Plaque Development
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Graves, D.; Corrêa, J.; Silva, T. The oral microbiota is modified by systemic diseases. J. Dent. Res. 2018, 98, 148–156. [Google Scholar] [CrossRef]
- Yumoto, H.; Hirota, K.; Hirao, K.; Ninomiya, M.; Murakami, K.; Fujii, H.; Miyake, Y. The pathogenic factors from oral streptococci for systemic diseases. Int. J. Mol. Sci. 2019, 20, 4571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health. Sci. 2017, 11, 72–80. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5426403/ (accessed on 16 October 2020).
- Kleinstein, S.; Nelson, K.; Freire, M. Inflammatory networks linking oral microbiome with systemic health and disease. J. Dent. Res. 2020, 99, 1131–1139. [Google Scholar] [CrossRef] [PubMed]
- Baeza, M.; Morales, A.; Cisterna, C.; Cavalla, F.; Jara, G.; Isamitt, Y.; Pino, P.; Gamonal, J. Effect of periodontal treatment in patients with periodontitis and diabetes: Systematic review and meta-analysis. J. Appl. Oral Sci. 2020, 28, 20190248. [Google Scholar] [CrossRef]
- Cecoro, G.; Annunziata, M.; Iuorio, M.T.; Nastri, L.; Guida, L. Periodontitis, low-grade inflammation and systemic health: A scoping review. Medicina 2020, 56, 272. [Google Scholar] [CrossRef]
- Parolia, A.; Thomas, M.S.; Kundabala, M.; Mohan, M. Propolis and its potential uses in oral health. Int. J. Med. Med. Sci. 2010, 2, 210–215. Available online: http://eprints.manipal.edu/1932/1/14._Int_J_Med_and_Med_Sci%2C_2010_proplis_use.pdf (accessed on 21 July 2020).
- Sforcin, J.M. Biological properties and therapeutic applications of propolis. Phytother. Res. 2016, 30, 894–905. [Google Scholar] [CrossRef]
- Özan, F.; Sümer, Z.; Polat, Z.A.; Er, K.; Özan, Ü.; Deḡer, O. Effect of mouthrinse containing propolis on oral microorganisms and human gingival fibroblasts. Eur. J. Dent. 2007, 1, 195–201. Available online: https://europepmc.org/article/med/19212467#free-full-text (accessed on 1 August 2020). [CrossRef] [PubMed] [Green Version]
- Listyasari, N.A.; Santoso, O. Inhibition of dental plaque formation by toothpaste containing propolis. Dent. J. 2012, 45, 208–211. [Google Scholar] [CrossRef] [Green Version]
- Lisbona-González, M.J.; Muñoz-Soto, E.; Reyes-Botella, C.; Olmedo-Gaya, M.V.; Diaz-Castro, J.; Moreno-Fernandez, J. Study of the antimicrobial effect of an ethanolic extract of propolis in periodontal disease. Appl. Sci. 2021, 11, 7463. [Google Scholar] [CrossRef]
- Anjum, S.I.; Ullah, A.; Ali Khan, K.; Attaullah, M.; Khan, H.; Ali, H.; Bashir, M.A.; Tahir, M.; Ansari, M.J. Composition and functional properties of propolis (bee glue): A review. Saudi J. Biol. Sci. 2019, 16, 1695–1703. [Google Scholar] [CrossRef]
- Kurek-Górecka, A.; Walczyńska-Dragon, K.; Felitti, R.; Nitecka, A.; Baron, S.; Olczyk, P. the influence of propolis on dental plaque reduction and the correlation between dental plaque and severity of COVID-19 complications—A literature review. Molecules 2021, 26, 5516. [Google Scholar] [CrossRef] [PubMed]
- Lim, G.; Janu, U.; Chiou, L.L.; Gandhi, K.K.; Palomo, L.; John, V. Periodontal health and systemic conditions. Dent. J. 2020, 8, 130. [Google Scholar] [CrossRef]
- Pan, W.; Wang, Q.; Chen, Q. The cytokine network involved in the host immune response to periodontitis. Int. J. Oral Sci. 2019, 11, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajishengallis, G.; Chavakis, T. Local and systemic mechanisms linking periodontal disease and inflammatory comorbidities. Nat. Rev. Immunol. 2021, 21, 426–440. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, S.; Caton, J.G.; Albandar, J.M.; Bissada, N.F.; Bouchard, P.; Cortellini, P.; Demirel, K.; de Sanctis, M.; Ercoli, C.; Fan, J.; et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S237–S248. [Google Scholar] [CrossRef] [PubMed]
- Wojtkowska, A.A.; Wysokinski, A. Periodontitis and prevalence of cardiovascular diseases. Chor. Serca Naczyń 2015, 12, 289–294. (In Polish) [Google Scholar]
- Kaur, N.; Kaur, N.; Sarangal, V. A study to evaluate the correlation of serum albumin levels with chronic periodontitis. Ind. J. Dent. Res. 2015, 26, 11–14. Available online: https://www.ijdr.in/article.asp?issn=0970-9290;year=2015;volume=26;issue=1;spage=11;epage=14;aulast=Kaur (accessed on 2 October 2020). [CrossRef]
- Knypl, K. Pharmacotherapy of arterial hypertension: Antagonists of angiotensin receptors AT1. Med. Rodz. 2001, 2, 58–60. (In Polish) [Google Scholar]
- Liccardo, D.; Cannavo, A.; Spagnuolo, G.; Ferrara, N.; Cittadini, A.; Rengo, C.; Rengo, G. Periodontal disease: A risk factor for diabetes and cardiovascular disease. Int. J. Mol. Sci. 2019, 20, 1414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yiqiang, Q.; Zao, W.; Yafang, L.; Yafei, H.; Yanheng, Z.; Xuanping, C. Rheumatoid arthritis risk in periodontitis patients: A systematic review and meta-analysis. Jt. Bone Spine 2020, 87, 556–564. [Google Scholar] [CrossRef]
- Ceccarelli, F.; Saccucci, M.; Di Carlo, G.; Lucchetti, R.; Pilloni, A.; Pranno, N.; Luzzi, V.; Valesini, G.; Polimeni, A. Periodontitis and rheumatoid arthritis: The same inflammatory mediators? Mediat. Inflamm. 2019, 2019, 6034546. [Google Scholar] [CrossRef] [PubMed]
- Mercado, F.; Marshall, R.I.; Klestov, A.C.; Bartold, P.M. Is there a relationship between rheumatoid arthritis and periodontal disease? J. Clin. Periodontol. 2000, 27, 267–272. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Northwell COVID-19 Research Consortium. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Li, T. COVID-19: Towards understanding of pathogenesis. Cell Res. 2020, 30, 367–369. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Zhong, L.; Deng, J.; Peng, J.; Dan, H.; Zeng, X.; Li, T.; Chen, Q. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int. J. Oral Sci. 2020, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Watanabe, N.; Kamio, N.; Kobayashi, R.; Iinuma, T.; Imai, K. Aspiration of periodontopathic bacteria due to poor oral hygiene potentially contributes to the aggravation of COVID-19. J. Oral Sci. 2021, 63, 1–3. [Google Scholar] [CrossRef]
- Takahashi, Y.; Watanabe, N.; Kamio, N.; Yokoe, S.; Suzuki, R.; Sato, S.; Iinuma, T.; Imai, K. Expression of the SARS-CoV-2 receptor ACE2 and proinflammatory cytokines induced by the periodontopathic bacterium fusobacterium nucleatum in human respiratory epithelial cells. Int. J. Mol. Sci. 2021, 22, 1352. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Mohindra, R.; Chauhan, P.; Singla, V.; Goyal, K.; Sahni, V.; Gaur, R.; Verma, D.K.; Ghosh, A.; Soni, R.K.; et al. SARS-CoV-2 detection in gingival crevicular fluid. J. Dent. Res. 2021, 100, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Hojyo, S.; Uchida, M.; Tanaka, K.; Hasebe, R.; Tanaka, Y.; Murakami, M.; Hirano, T. How COVID-19 induces cytokine storm with high mortality. Inflamm. Regen. 2020, 40, 1–7. [Google Scholar] [CrossRef]
- Sampson, V.; Kamona, N.; Sampson, A. Could there be a link between oral hygiene and the severity of SARS-CoV-2 infections? Brit. Dent. J. 2020, 228, 971–975. [Google Scholar] [CrossRef] [PubMed]
- Stanko, P.; Izakovicova; Holla, L. Bidirectional association between diabetes mellitus and inflammatory periodontal disease. A review. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 2014, 158, 35–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bui, F.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed J. 2019, 42, 27–35. [Google Scholar] [CrossRef]
- Chapple, I.L.; Genco, R.; Working Group 2 of the Joint EFP/AAP Workshop. Diabetes and periodontal diseases: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, S106–S112. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, A.; Zafar, S.; Sharma, A.; Quaranta, A. Diabetes mellitus and periodontal disease: The call for interprofessional education and interprofessional collaborative care—A systematic review of the literature. J. Interprof. Care 2020, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Dicembrini, I.; Serni, L.; Monami, M.; Caliri, M.; Barbato, L.; Cairo, F.; Mannucci, E. Type 1 diabetes and periodontitis: Prevalence and periodontal destruction-a systematic review. Acta Diabetol. 2020, 57, 1405–1412. [Google Scholar] [CrossRef]
- Grigoriadis, A.; Räisänen, I.T.; Pärnänen, P.; Tervahartiala, T.; Sorsa, T.; Sakellari, D. Prediabetes/diabetes screening strategy at the periodontal clinic. Clin. Exp. Dent. Res. 2021, 7, 85–92. [Google Scholar] [CrossRef]
- Borsa, L.; Dubois, M.; Sacco, G.; Lupi, L. Analysis the link between periodontal diseases and Alzheimer’s disease: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 9312. [Google Scholar] [CrossRef] [PubMed]
- Poole, S.; Singhrao, S.K.; Kesavalu, L.; Curtis, M.A.; Crean, S. Determining the presence of periodontopathic virulence factors in short-term postmortem Alzheimer’s disease brain tissue. J. Alzheim. Dis. 2013, 36, 665–677. [Google Scholar] [CrossRef] [PubMed]
- Sansores-España, D.; Carrillo-Avila, A.; Melgar-Rodriguez, S.; Díaz-Zuñiga, J.; Martínez-Aguilar, V. Periodontitis and Alzheimer’s disease. Med. Oral. Patol. Oral. Cir. Bucal. 2021, 26, 43–48. [Google Scholar] [CrossRef]
- Kanagasingam, S.; Chukkapalli, S.S.; Welbury, R.; Singhrao, S.K. Porphyromonas gingivalis is a strong risk factor for Alzheimer’s disease. J Alzheimers Dis. Rep. 2020, 4, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Ahangari, Z.; Naseri, M.; Vatandoost, F. Propolis: Chemical composition and its applications in endodontics. Iran Endod. J. 2018, 13, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Libério, S.A.; Pereira, A.L.A.; Araújo, M.J.A.; Dutra, R.P.; Nascimento, F.R.; Monteiro-Neto, V.; Ribeiro, M.N.S.; Gonçalves, A.G.; Guerra, R.N. The potential use of propolis as a cariostatic agent and its actions on mutans group streptococci. J. Ethnopharmacol. 2009, 125, 1–9. [Google Scholar] [CrossRef]
- Eroglu, N.; Akkus, S.; Yaman, M.; Asci, B.; Silici, S. Amino acid and vitamin content of propolis collected by native Caucasican honeybees. J. Apic. Sci. 2016, 60, 101–110. [Google Scholar] [CrossRef] [Green Version]
- Shahinozzaman, M.; Basak, B.; Emran, R.; Rozario, P.; Obanda, D.N. Artepillin C: A comprehensive review of its chemistry, bioavailability, and pharmacological properties. Phytotherapy 2020, 147, 104775. [Google Scholar] [CrossRef]
- Paulino, N.; Abreu, S.R.L.; Uto, Y.; Koyama, D.; Nagasawa, H.; Hori, H.; Dirsch, V.; Vollmar, A.M.; Paulino, A.S.; Bretz, W. Anti-inflammatory effects of a bioavailable compound, Artepillin C, in Brazilian propolis. Eur. J. Pharmacol. 2008, 587, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Veloz, J.J.; Alvear, M.; Salazar, L.A. Antimicrobial and antibiofilm activity against Streptococcus mutans of individual and mixtures of the main polyphenolic compounds found in Chilean propolis. BioMed. Res. Int. 2019, 2019, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.; Zhang, C.-P.; Wang, K.; Li, G.Q.; Hu, F.-L. Recent advances in the chemical composition of propolis. Molecules 2014, 19, 19610–19632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, H.; Gomes, B.P.F.A.; Rosalen, P.L.; Ambrosano, G.M.B.; Par, K.Y.K.; Cury, J.A. In vitro antimicrobial activity of propolis and Arnica montana against oral pathogens. Arch. Oral Bio. 2000, 45, 141–148. [Google Scholar] [CrossRef]
- Botros, N.; Iyer, P.; Ojcius, D.M. Is there an association between oral health and severity of COVID-19 complications? Biomed. J. 2020, 43, 325–327. [Google Scholar] [CrossRef] [PubMed]
- Lofty, M. Biological activity of bee propolis in health and disease. Asian Pac. J. Cancer Prev. 2006, 7, 22–31. Available online: http://journal.waocp.org/article_24421_e27f12cfb64e899d4a0ee2f315f985bf.pdf (accessed on 21 October 2020).
- Elbaz, G.; Elsayad, I. Comparison if the antimicrobial effect of Egyptian propolis vs. New Zealand propolis on Streptococcus mutans and Lactobacilli in saliva. Oral Health Prev. Dent. 2012, 10, 155–160. Available online: http://www.quintpub.com/userhome/ohpd/ohpd_2012_02_s0155.pdf (accessed on 2 October 2020).
- Koo, H.; Rosalen, P.L.; Cury, J.A.; Ambrosano, G.M.; Murata, R.M.; Yatsuda, R.; Ikegaki, M.; Alencar, S.M.; Park, Y.K. Effect of a new variety of Apis mellifera propolis on Mutans streptococci. Curr. Microbiol. 2000, 41, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Duarte, S.; Koo, H.; Bowen, W.H.; Hayacibara, M.F.; Cury, J.A.; Ikegaki, M.; Rosalen, P.L. Effect of a novel type of propolis and its chemical fractions on glucosyltransferases and on growth and adherence of Mutans streptococci. Biol. Pharm. Bull. 2003, 26, 527–531. [Google Scholar] [CrossRef] [Green Version]
- Koo, H.; Rosalen, P.L.; Cury, J.A.; Park, Y.K.; Bowen, W. Effects of compounds found in propolis on Streptococcus mutans growth and on glucosyltransferase activity. Antimicrob. Agents Chemother. 2002, 46, 1302–1309. [Google Scholar] [CrossRef] [Green Version]
- Ikeno, K.; Ikeno, T.; Miyazawa, C. Effects of propolis on dental caries in rats. Caries Res. 1991, 25, 347–351. [Google Scholar] [CrossRef]
- Kędzia, B. Propolis in the treatment of dental caries. Postępy Fitoter. 2011, 2, 113–121. (In Polish) [Google Scholar]
- Koo, H.; Cury, J.A.; Rosalen, P.L.; Ambrosano, G.M.; Ikegaki, M.; Park, Y.K. Effect of a mouthrinse containing selected propolis on 3-day dental plaque accumulation and polysaccharide formation. Caries Res. 2002, 36, 445–448. [Google Scholar] [CrossRef]
- Machorowska-Pieniążek, A.; Skucha-Nowak, M.; Mertas, A.; Tanasiewicz, M.; Dziedzic, A.; Król, W. Influence of propolis on hygiene, gingival condition, and oral microflora in patients with cleft lip and palate treated with fixed orthodontic appliances. Evid. Based Complement. Altern. Med. 2013, 2013, 183915. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, C.; Colombo, F.; Biella, S.; Stockley, C.; Restani, P. polyphenols and human health: The role of bioavailability. Nutrients 2021, 13, 273. [Google Scholar] [CrossRef]
- Li, L.; Guo, L.; Wolinsky, L.; Shi, W.; Lux, R. The antimicrobial activity of pomegranate polyphenol extract (POMx) lozenges in a saliva-derived biofilm model system. Dent. Open. 2015, 2, 112–120. [Google Scholar] [CrossRef]
- Koo, H.; de Guzman, P.N.; Schobel, B.D.; Smith, A.V.; Bowen, W.H. Influence of cranberry juice on glucan-mediated processes involved in Streptococcus mutans biofilm development. Caries Res. 2006, 40, 20–27. [Google Scholar] [CrossRef]
- Williamson, G.; Carughi, A. Polyphenol content and health benefits of raisins. Nutrit. Res. 2010, 30, 511–519. [Google Scholar] [CrossRef]
- Mukherjee, M.; Bandyopadhyay, P.; Kundu, D. Exploring the role of cranberry polyphenols in periodontits: A brief review. J. Indian Soc. Periodontol. 2014, 18, 136–139. [Google Scholar] [CrossRef] [PubMed]
- Sakanaka, S.; Shimura, N.; Aizawa, M.; Kim, M.; Yamamoto, T. Preventive effect of green tea polyphenols against dental caries in conventional rats. Biosci. Biotech. Biochem. 1992, 56, 592–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arya, V.; Taneja, L. Inhibition of salivary amylase by black tea in high-caries and low-caries index children: A comparative in vivo study. Ayu 2015, 36, 278–282. [Google Scholar] [CrossRef] [Green Version]
- Namboodiripad, P.C.; Srividya, K. Can coffee prevent caries? An in vitro study. Internet J. Dent. Sci. 2009, 7, 1–6. [Google Scholar] [CrossRef]
- Daglia, M.; Tarsi, R.; Papetti, A.; Grisoli, P.; Dacarro, C.; Pruzzo, C.; Gazzani, G. Antiadhesive effect of green and roasted coffee on Streptococcus mutans’ adhesive properties on saliva-coated hydroxyapatite beads. J. Agric. Food Chem. 2002, 50, 1225–1229. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Nakamura, Y.; Tokunaga, T.; Iijima, D.; Fukushima, K. Anti-cariogenic properties of a water-soluble extract from cacao. Biosci. Biotechnol. Biocem. 2003, 67, 2567–2573. [Google Scholar] [CrossRef] [Green Version]
- Olczak-Kowalczyk, D.; Grzebieluch, W.; Turkowski, M.; Kaczmarek, U. Food and dental caries. Part 2. Nutrition containing polyphenols. Nowa Stomatol. 2017, 2, 80–88. (In Polish) [Google Scholar]
- Uju, D.E.; Obioma, N.P. Anticariogenic potentials of clove, tobacco and bitter kola. Asian Pac. J. Trop. Med. 2011, 4, 814–818. [Google Scholar] [CrossRef] [Green Version]
- He, Z.; Huang, Z.; Jiang, W.; Zhou, W. Antimicrobial activity of cinnamaldehyde on Streptococcus mutans biofilms. Front. Microbiol. 2019, 10, 2241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yanakiev, S. Effects of cinnamon (Cinnamomum spp.) in dentistry: A review. Molecules 2020, 25, 4184. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, Y.; Shi, Y.Q.; Pan, X.H.; Lu, Y.H.; Cao, P. Antibacterial effects of cinnamon (Cinnamomum zeylanicum) bark essential oil on Porphyromonas gingivalis. Microb. Pathog. 2018, 116, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.S.; Li, Y.; Cao, X.; Cui, Y. The effect of eugenol on the cariogenic properties of Streptococcus mutans and dental caries development in rats. Exp. Ther. Med. 2013, 5, 1667–1670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, J.Y.; Choo, J.H.; Lee, M.H.; Hwang, J.K. Anticariogenic activity of macelignan isolated from Myristica fragrans (nutmeg) against Streptococcus mutans. Phytomedicine 2006, 13, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Bae, J.; Lee, D.S. Antibacterial activity of [10]-gingerol and [12]-gingerol isolated from ginger rhizome against periodontal bacteria. Phytother. Res. 2008, 22, 1446–1449. [Google Scholar] [CrossRef]
- Patel, R.V.; Thaker, V.T.; Patel, V.K. Antimicrobial activity of ginger and honey on isolates of extracted carious teeth during orthodontic treatment. Asian Pac. J. Trop. Biomed. 2011, 1, S58–S61. [Google Scholar] [CrossRef]
- Ahn, S.J.; Song, Y.D.; Mah, S.J.; Cho, E.J.; Kook, J.K. Determination of optimal concentration of deglycyrrhizinated licorice root extract for preventing dental caries using a bacterial model system. J. Dent. Sci. 2014, 9, 214–220. [Google Scholar] [CrossRef] [Green Version]
- Ovaskainen, M.L.; Torronen, R.; Koponen, J.M.; Sinkko, H.; Hellstrom, J.; Reinivuo, H.; Mattila, P. Dietary intake and major food sources of polyphenols in Finnish adults. J. Nutr. 2008, 138, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Perez-Jimenez, J.; Fezeu, L.; Touvier, M.; Arnault, N.; Manach, C.; Hercberg, S.; Galan, P.; Scalbert, A. Dietary intake of 337 polyphenols in French adults. Am. J. Clin. Nutr. 2011, 93, 1220–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tresserra-Rimbau, A.; Medina-Remon, A.; Perez-Jimenez, J.; Martinez-Gonzalez, M.A.; Covas, M.I.; Corella, D.; Salas-Salvado, J.; Gómez-Gracia, E.; Lapetra, J.; Arós, F.; et al. Dietary intake and major food sources of polyphenols in a Spanish population at high cardiovascular risk: The PREDIMED study. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Stepaniak, U.; Topor-Madry, R.; Szafraniec, K.; Pajak, A. Estimated dietary intake and major food sources of polyphenols in the Polish arm of the HAPIEE study. Nutrition 2014, 30, 1398–1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scalbert, A.; Williamson, G. Dietary Intake and Bioavailability of Polyphenols. J. Nutr. 2000, 130, 2073–2085. [Google Scholar] [CrossRef] [PubMed]
- Wilczyńska, A.; Retel, M. Evaluation of polyphenol dietary intake considering participation of honey. Probl. Hig. Epidemiol. 2011, 92, 709–712. (In Polish) [Google Scholar]
- Zulhendri, F.; Felitti, R.; Fearnley, J.; Ravalia, M. The use of propolis in dentistry, oral health, and medicine: A review. J. Oral. Biosci. 2021, 63, 23–34. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Active | Action | Literature |
|---|---|---|
| Apigenin Kaempherol Cinnamic acid | Inhibition of the Glucosyltransferase activity | [58,59] |
| Galangin Chrysin Pinobanksin Quercetin Naringenin Apigenin TT-farnesol Phenolic acids like caffeic acid, benzoic acid, cinnamic acid, gallic acid Artepillin C (3,5-diprenyl-p-coumaric acid) Catechins Ursolic acid Bacarin | Antibacterial action | [7,8,9,10,11] |
| Not identified | Antiadherent action | |
| Galangin Caffeic acid phenethyl ester (CAPE) | Anti-inflammatory action | [12] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurek-Górecka, A.; Walczyńska-Dragon, K.; Felitti, R.; Baron, S.; Olczyk, P. Propolis and Diet Rich in Polyphenols as Cariostatic Agents Reducing Accumulation of Dental Plaque. Molecules 2022, 27, 271. https://doi.org/10.3390/molecules27010271
Kurek-Górecka A, Walczyńska-Dragon K, Felitti R, Baron S, Olczyk P. Propolis and Diet Rich in Polyphenols as Cariostatic Agents Reducing Accumulation of Dental Plaque. Molecules. 2022; 27(1):271. https://doi.org/10.3390/molecules27010271
Chicago/Turabian StyleKurek-Górecka, Anna, Karolina Walczyńska-Dragon, Rafael Felitti, Stefan Baron, and Paweł Olczyk. 2022. "Propolis and Diet Rich in Polyphenols as Cariostatic Agents Reducing Accumulation of Dental Plaque" Molecules 27, no. 1: 271. https://doi.org/10.3390/molecules27010271