
Recent Advances in Polymeric Nanoparticle-Encapsulated Drugs against Intracellular Infections



Abstract
:1. Introduction
2. Polymeric Nanocarriers against Intracellular Infections: General Aspects
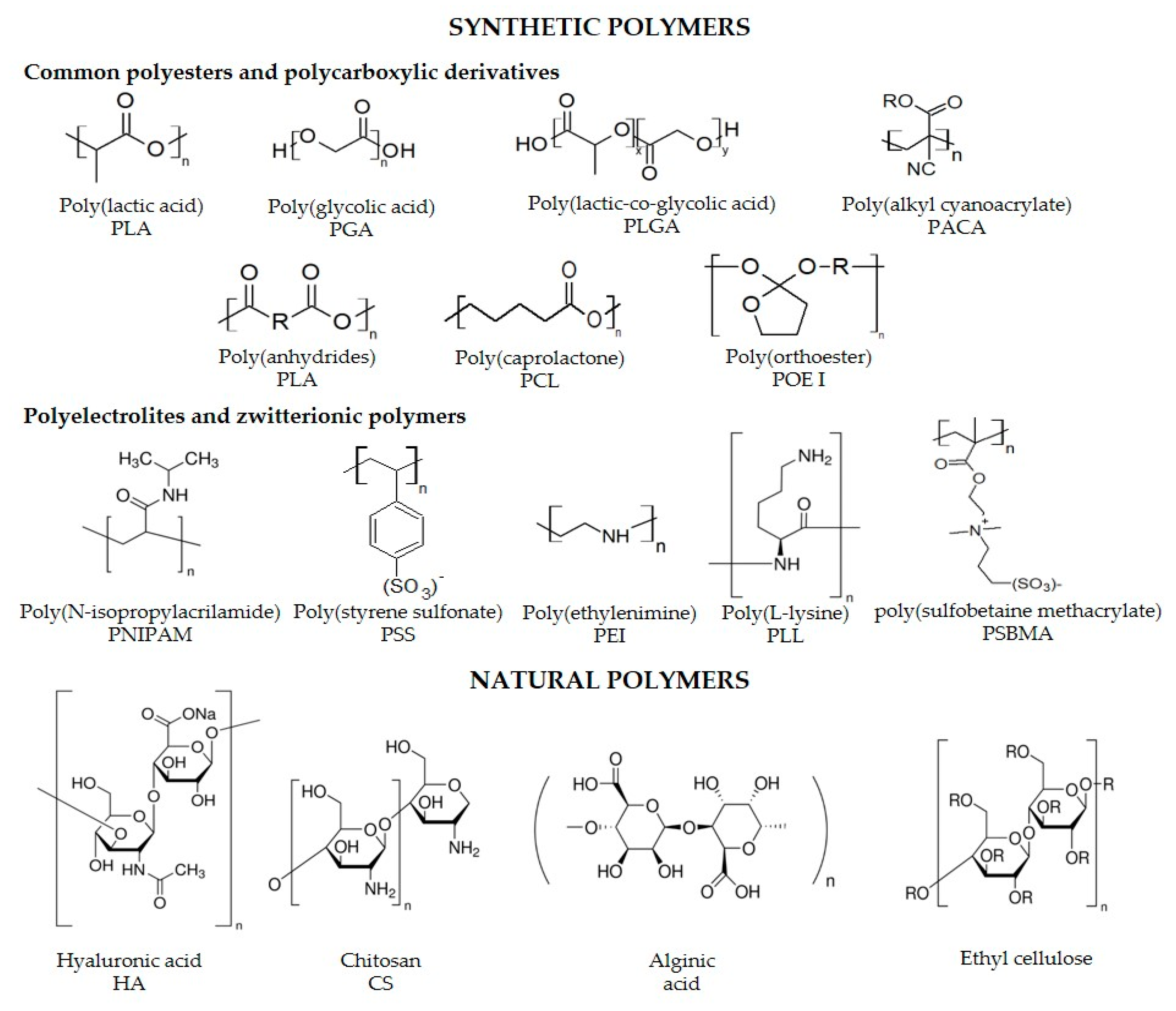
2.1. Chemical Nature of the Polymer, Physicochemical Properties and Interactions
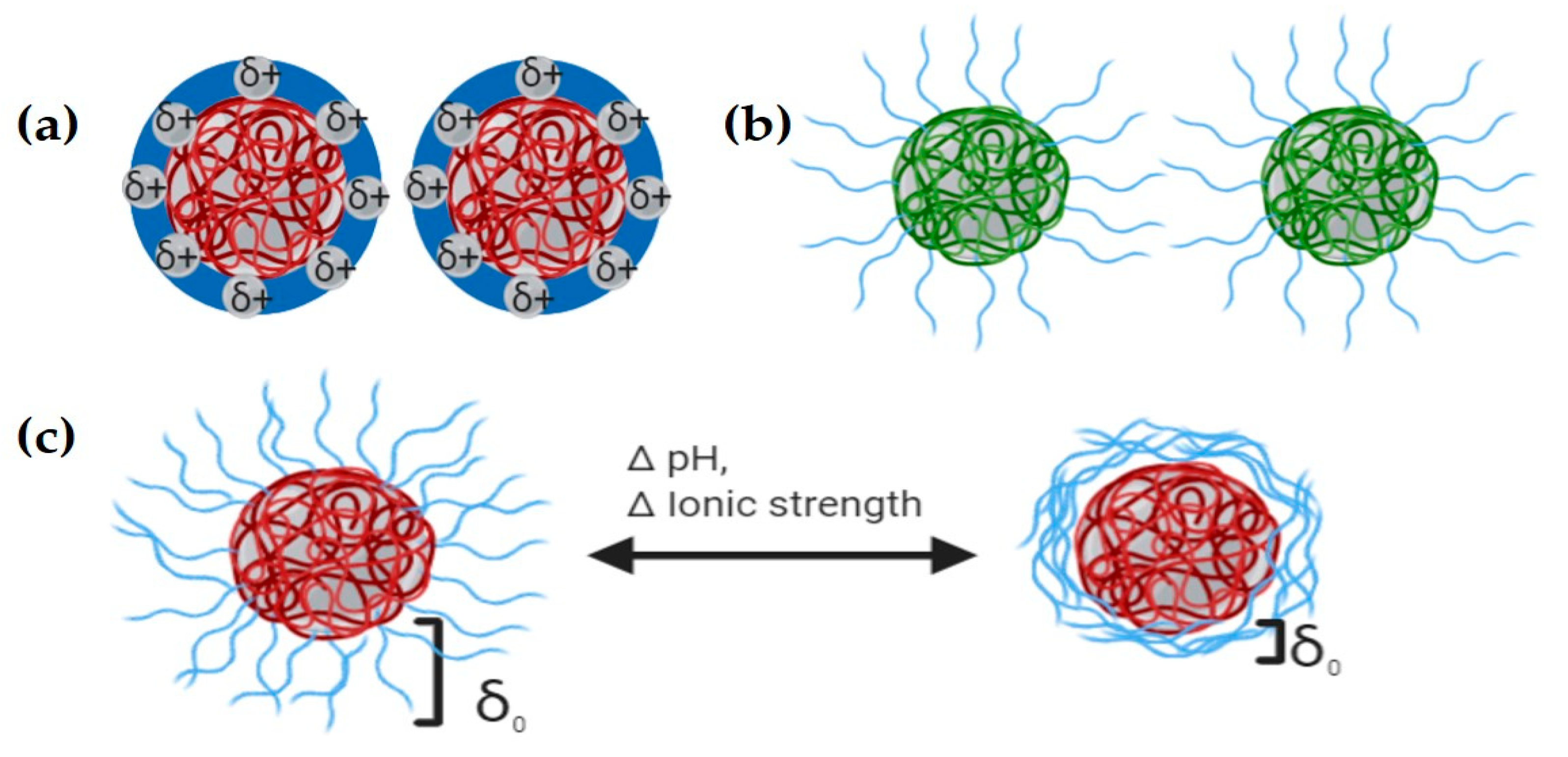
2.2. Colloidal Properties of PNs for Intracellular Therapy
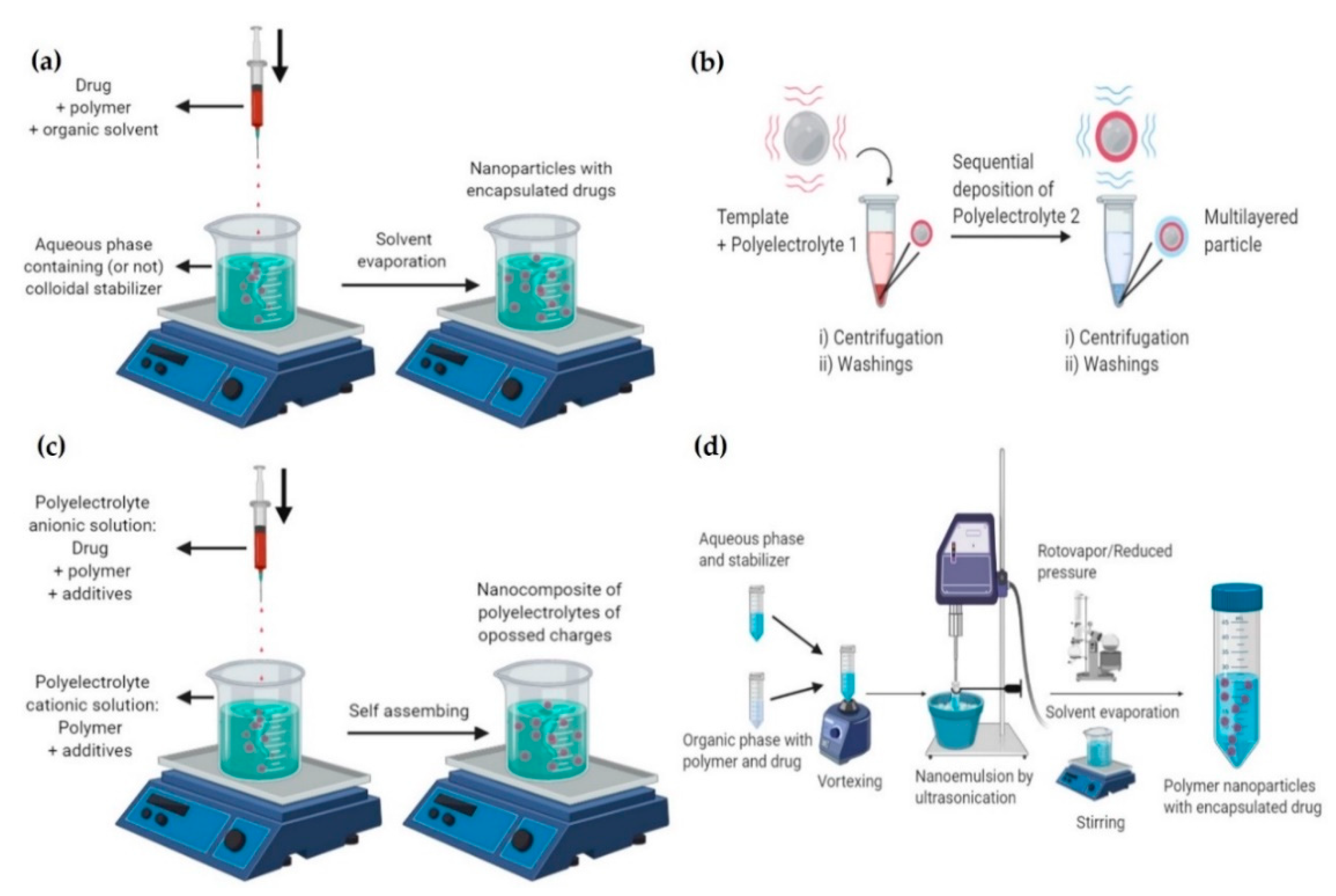
2.3. Nanoparticle Fabrication Methods
2.3.1. Nanoprecipitation
2.3.2. Layer-by-Layer (LbL)
2.3.3. Ionic Gelation
2.3.4. Emulsification-Evaporation
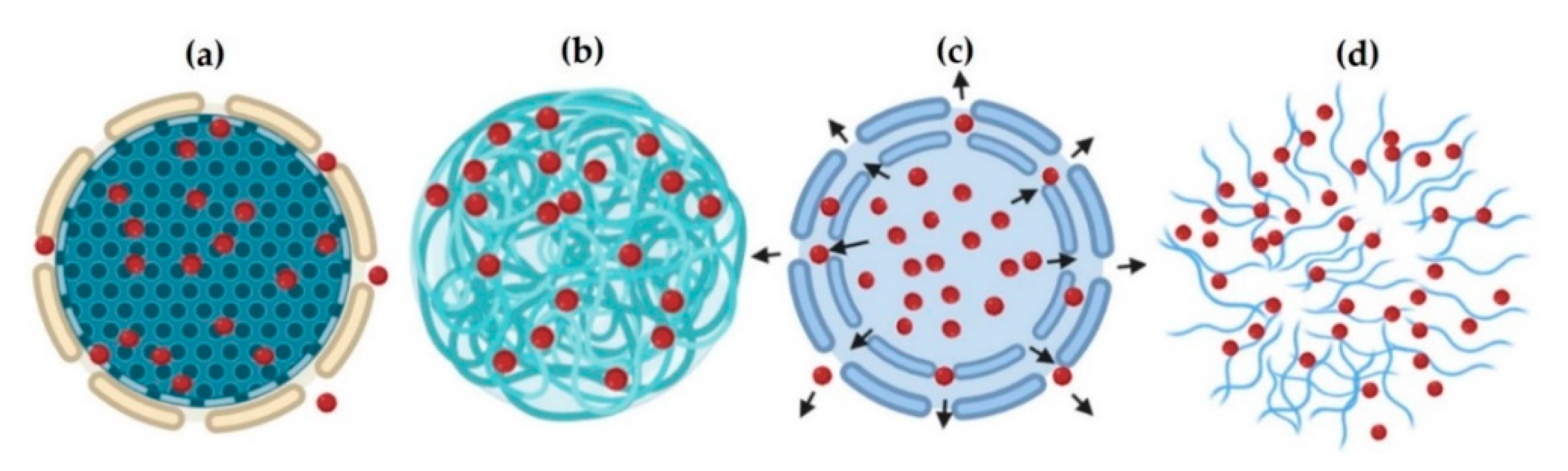
2.4. Nanoparticles Drug Release
3. Challenges and Opportunities of Polymeric Nanoparticles in Treating Intracellular Pathogens
3.1. Intracellular Pathogens
3.2. Biological Barriers
3.2.1. Intravenous Administration
3.2.2. Oral Administration
3.2.3. Intranasal Administration
3.2.4. Topical Administration
3.3. Therapeutic Challenges
4. Recent Advances of PNs in the Treatment of Intracellular Infections
5. Pharmacokinetics, Biodistribution and Nanotoxicology
5.1. Pharmacokinetics
5.2. Biodistribution
5.3. Nanotoxicology
6. Future Outlooks
Author Contributions
Funding
Conflicts of Interest
References
- Dodds Ashley, E.; Lewis, R.; Lewis, J.; Martin, C.; Andes, D. Pharmacology of Systemic Antifungal Agents. Clin. Infect. Dis. 2006, 43. [Google Scholar] [CrossRef] [Green Version]
- Jayaraman, R. Antibiotic resistance: An overview of mechanisms and a paradigm shift. Curr. Sci. 2009, 96, 1475–1484. [Google Scholar]
- Ladaviere, C.; Gref, R. Toward an optimized treatment of intracellular bacterial infections: Input of nanoparticulate drug delivery systems. Nanomedicine (Lond) 2015, 10, 3033–3055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zazo, H.; Colino, C.I.; Lanao, J.M. Current applications of nanoparticles in infectious diseases. J. Control. Release 2016, 224, 86–102. [Google Scholar] [CrossRef] [PubMed]
- Costa-Gouveia, J.; Aínsa, J.A.; Brodin, P.; Lucía, A. How can nanoparticles contribute to antituberculosis therapy? Drug Discov. Today 2017, 22, 600–607. [Google Scholar] [CrossRef]
- Lee, N.-Y.; Ko, W.-C.; Hsueh, P.-R. Nanoparticles in the Treatment of Infections Caused by Multidrug-Resistant Organisms. Front. Pharmacol. 2019, 10, 1153. [Google Scholar] [CrossRef] [Green Version]
- Tukulula, M.; Gouveia, L.; Paixao, P.; Hayeshi, R.; Naicker, B.; Dube, A. Functionalization of PLGA Nanoparticles with 1,3-beta-glucan Enhances the Intracellular Pharmacokinetics of Rifampicin in Macrophages. Pharm. Res. 2018, 35, 111. [Google Scholar] [CrossRef]
- Jahagirdar, P.S.; Gupta, P.K.; Kulkarni, S.P.; Devarajan, P.V. Polymeric curcumin nanoparticles by a facile in situ method for macrophage targeted delivery. Bioeng. Transl. Med. 2019, 4, 141–151. [Google Scholar] [CrossRef]
- Singh, L.; Kruger, H.G.; Maguire, G.E.M.; Govender, T.; Parboosing, R. The role of nanotechnology in the treatment of viral infections. Ther. Adv. Infect. Dis. 2017, 4, 105–131. [Google Scholar] [CrossRef]
- Biswaro, L.S.; Garcia, M.P.; da Silva, J.R.; Neira Fuentes, L.F.; Vera, A.; Escobar, P.; Azevedo, R.B. Itraconazole encapsulated PLGA-nanoparticles covered with mannose as potential candidates against leishmaniasis. J. Biomed. Mater. Res. B. Appl. Biomater. 2019, 107, 680–687. [Google Scholar] [CrossRef]
- Hu, J.; Wei, P.; Seeberger, P.H.; Yin, J. Mannose-Functionalized Nanoscaffolds for Targeted Delivery in Biomedical Applications. Chem. Asian J. 2018, 13, 3448–3459. [Google Scholar] [CrossRef] [PubMed]
- Gao, W.; Chen, Y.; Zhang, Y.; Zhang, Q.; Zhang, L. Nanoparticle-based local antimicrobial drug delivery. Adv. Drug Deliv. Rev. 2018, 127, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Mir, M.; Ahmed, N.; ur Rehman, A. Recent applications of PLGA based nanostructures in drug delivery. Colloids Surf. B Biointerfaces 2017, 159, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Kim, C.-S.; Saylor, D.M.; Koo, D. Polymer degradation and drug delivery in PLGA-based drug-polymer applications: A review of experiments and theories. J. Biomed. Mater. Res. B. Appl. Biomater. 2017, 105, 1692–1716. [Google Scholar] [CrossRef] [PubMed]
- Kamaly, N.; Yameen, B.; Wu, J.; Farokhzad, O.C. Degradable controlled-release polymers and polymeric nanoparticles: Mechanisms of controlling drug release. Chem. Rev. 2016, 116, 2602–2663. [Google Scholar] [CrossRef] [Green Version]
- Bentz, K.C.; Savin, D.A. Hollow polymer nanocapsules: Synthesis, properties, and applications. Polym. Chem. 2018, 9, 2059–2081. [Google Scholar] [CrossRef]
- Gao, M.; Yang, Y.; Bergfel, A.; Huang, L.; Zheng, L.; Bowden, T.M. Self-assembly of cholesterol end-capped polymer micelles for controlled drug delivery. J. Nanobiotechnol. 2020, 18, 13. [Google Scholar] [CrossRef] [Green Version]
- Ganda, I.S.; Zhong, Q.; Hali, M.; Albuquerque, R.L.C.; Padilha, F.F.; da Rocha, S.R.P.; Whittum-Hudson, J.A. Dendrimer-conjugated peptide vaccine enhances clearance of Chlamydia trachomatis genital infection. Int. J. Pharm. 2017, 527, 79–91. [Google Scholar] [CrossRef]
- Zhu, Y.; Yang, B.; Chen, S.; Du, J. Polymer vesicles: Mechanism, preparation, application, and responsive behavior. Prog. Polym. Sci. 2017, 64, 1–22. [Google Scholar] [CrossRef]
- Zhao, Y.; Li, X.; Zhao, X.; Yang, Y.; Li, H.; Zhou, X.; Yuan, W. Asymmetrical Polymer Vesicles for Drug delivery and Other Applications. Front. Pharmacol. 2017, 8, 374. [Google Scholar] [CrossRef] [Green Version]
- Letchford, K.; Burt, H. A review of the formation and classification of amphiphilic block copolymer nanoparticulate structures: Micelles, nanospheres, nanocapsules and polymersomes. Eur. J. Pharm. Biopharm. 2007, 65, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Colorado, D.; Fernandez, M.; Orozco, J.; Lopera, Y.; Muñoz, D.L.; Acín, S.; Balcazar, N. Metabolic Activity of Anthocyanin Extracts Loaded into Non-ionic Niosomes in Diet-Induced Obese Mice. Pharm. Res. 2020, 37, 152. [Google Scholar] [CrossRef]
- Hickey, J.W.; Santos, J.L.; Williford, J.-M.; Mao, H.-Q. Control of polymeric nanoparticle size to improve therapeutic delivery. J. Control. Release 2015, 219, 536–547. [Google Scholar] [CrossRef] [Green Version]
- Rezvantalab, S.; Drude, N.I.; Moraveji, M.K.; Guvener, N.; Koons, E.K.; Shi, Y.; Lammers, T.; Kiessling, F. PLGA-Based Nanoparticles in Cancer Treatment. Front. Pharmacol. 2018, 9, 1260. [Google Scholar] [CrossRef] [Green Version]
- Cowen, T.; Karim, K.; Piletsky, S.A. Solubility and size of polymer nanoparticles. Polym. Chem. 2018, 9, 4566–4573. [Google Scholar] [CrossRef] [Green Version]
- Ekladious, I.; Colson, Y.L.; Grinstaff, M.W. Polymer–drug conjugate therapeutics: Advances, insights and prospects. Nat. Rev. Drug Discov. 2019, 18, 273–294. [Google Scholar] [CrossRef] [PubMed]
- Girase, M.L.; Patil, P.G.; Ige, P.P. Polymer-drug conjugates as nanomedicine: A review. Int. J. Polym. Mater. Polym. Biomater. 2019, 1–25. [Google Scholar] [CrossRef]
- Shirure, V.S.; George, S.C. Design considerations to minimize the impact of drug absorption in polymer-based organ-on-a-chip platforms. Lab Chip 2017, 17, 681–690. [Google Scholar] [CrossRef]
- Sun, Y.; Chen, D.; Pan, Y.; Qu, W.; Hao, H.; Wang, X.; Liu, Z.; Xie, S. Nanoparticles for antiparasitic drug delivery. Drug Deliv. 2019, 26, 1206–1221. [Google Scholar] [CrossRef]
- Batalha, I.L.; Bernut, A.; Schiebler, M.; Ouberai, M.M.; Passemar, C.; Klapholz, C.; Kinna, S.; Michel, S.; Sader, K.; Castro-Hartmann, P.; et al. Polymeric nanobiotics as a novel treatment for mycobacterial infections. J. Control. Release 2019, 314, 116–124. [Google Scholar] [CrossRef]
- Reynolds, N.; Dearnley, M.; Hinton, T.M. Polymers in the Delivery of siRNA for the Treatment of Virus Infections. Top. Curr. Chem. 2017, 375, 38. [Google Scholar] [CrossRef] [PubMed]
- Mena-Giraldo, P.; Pérez-Buitrago, S.; Londoño-Berrío, M.; Ortiz-Trujillo, I.C.; Hoyos-Palacio, L.M.; Orozco, J. Photosensitive nanocarriers for specific delivery of cargo into cells. Sci. Rep. 2020, 10, 2110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trousil, J.; Syrova, Z.; Dal, N.-J.K.; Rak, D.; Konefal, R.; Pavlova, E.; Matejkova, J.; Cmarko, D.; Kubickova, P.; Pavlis, O.; et al. Rifampicin Nanoformulation Enhances Treatment of Tuberculosis in Zebrafish. Biomacromolecules 2019, 20, 1798–1815. [Google Scholar] [CrossRef] [PubMed]
- Tropical Diseases 3rd International Conference on Tropical and Infectious Diseases. Available online: https://tropicaldiseases.infectiousconferences.com/ (accessed on 18 July 2020).
- Briones, E.; Colino, C.I.; Lanao, J.M. Delivery systems to increase the selectivity of antibiotics in phagocytic cells. J. Control. Release 2008, 125, 210–227. [Google Scholar] [CrossRef]
- Zaioncz, S.; Khalil, N.M.; Mainardes, R.M. Exploring the Role of Nanoparticles in Amphotericin B Delivery. Curr. Pharm. Des. 2017, 23, 509–521. [Google Scholar] [CrossRef]
- Hakkimane, S.S.; Shenoy, V.P.; Gaonkar, S.L.; Bairy, I.; Guru, B.R. Antimycobacterial susceptibility evaluation of rifampicin and isoniazid benz-hydrazone in biodegradable polymeric nanoparticles against Mycobacterium tuberculosis H37Rv strain. Int. J. Nanomed. 2018, 13, 4303–4318. [Google Scholar] [CrossRef] [Green Version]
- Patra, J.K.; Das, G.; Fraceto, L.F.; Campos, E.V.R.; Rodriguez-Torres, M.D.P.; Acosta-Torres, L.S.; Diaz-Torres, L.A.; Grillo, R.; Swamy, M.K.; Sharma, S.; et al. Nano based drug delivery systems: Recent developments and future prospects. J. Nanobiotechnol. 2018, 16, 71. [Google Scholar] [CrossRef] [Green Version]
- Cunha-Azevedo, E.P.; Py-Daniel, K.R.; Siqueira-Moura, M.P.; Bocca, A.L.; Felipe, M.S.S.; Tedesco, A.C.; Pires Junior, O.R.; Lucci, C.M.; Azevedo, R.B. In vivo evaluation of the efficacy, toxicity and biodistribution of PLGA-DMSA nanoparticles loaded with itraconazole for treatment of paracoccidioidomycosis. J. Drug Deliv. Sci. Technol. 2018, 45, 135–141. [Google Scholar] [CrossRef]
- World Health Organization Antibiotic Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 29 April 2020).
- Thakur, A.; Mikkelsen, H.; Jungersen, G. Intracellular pathogens: Host immunity and microbial persistence strategies. J. Immunol. Res. 2019, 2019. [Google Scholar] [CrossRef]
- Maurin, M.; Raoult, D. Use of aminoglycosides in treatment of infections due to intracellular bacteria. Antimicrob. Agents Chemother. 2001, 45, 2977–2986. [Google Scholar] [CrossRef] [Green Version]
- Xie, S.; Tao, Y.; Pan, Y.; Qu, W.; Cheng, G.; Huang, L.; Chen, D.; Wang, X.; Liu, Z.; Yuan, Z. Biodegradable nanoparticles for intracellular delivery of antimicrobial agents. J. Control. Release 2014, 187, 101–117. [Google Scholar] [CrossRef] [PubMed]
- Ficai, A.; Grumezescu, A.M. Nanostructures for Antimicrobial Therapy; Elsevier: Amsterdam, The Netherlands, 2017; ISBN 0323461514. [Google Scholar]
- Aderibigbe, B.A. Polymeric therapeutic delivery systems for the treatment of infectious diseases. Ther. Deliv. 2017, 8, 557–576. [Google Scholar] [CrossRef] [PubMed]
- Abed, N.; Couvreur, P. Nanocarriers for antibiotics: A promising solution to treat intracellular bacterial infections. Int. J. Antimicrob. Agents 2014, 43, 485–496. [Google Scholar] [CrossRef]
- Khalid, M.; El-Sawy, H.S. Polymeric nanoparticles: Promising platform for drug delivery. Int. J. Pharm. 2017, 528, 675–691. [Google Scholar]
- Donahue, N.D.; Acar, H.; Wilhelm, S. Concepts of nanoparticle cellular uptake, intracellular trafficking, and kinetics in nanomedicine. Adv. Drug Deliv. Rev. 2019, 143, 68–96. [Google Scholar] [CrossRef]
- Kamaly, N.; He, J.C.; Ausiello, D.A.; Farokhzad, O.C. Nanomedicines for renal disease: Current status and future applications. Nat. Rev. Nephrol. 2016, 12, 738. [Google Scholar] [CrossRef] [Green Version]
- Devarajan, P.V.; Jain, S. Targeted Drug Delivery: Concepts and Design; Springer: Berlin/Heidelberg, Germany, 2016; ISBN 331937625X. [Google Scholar]
- Lakkireddy, H.R.; Bazile, D. Building the design, translation and development principles of polymeric nanomedicines using the case of clinically advanced poly (lactide (glycolide))–poly (ethylene glycol) nanotechnology as a model: An industrial viewpoint. Adv. Drug Deliv. Rev. 2016, 107, 289–332. [Google Scholar] [CrossRef]
- Zhang, Y.; Chan, H.F.; Leong, K.W. Advanced materials and processing for drug delivery: The past and the future. Adv. Drug Deliv. Rev. 2013, 65, 104–120. [Google Scholar] [CrossRef] [Green Version]
- Farokhzad, O.C.; Langer, R. Impact of Nanotechnology on Drug Delivery. ACS Nano 2009, 3, 16–20. [Google Scholar] [CrossRef]
- Amgoth, C.; Phan, C.; Banavoth, M.; Rompivalasa, S.; Tang, G. Polymer Properties: Functionalization and Surface Modified Nanoparticles. In Role of Novel Drug Delivery Vehicles in Nanobiomedicine; IntechOpen: London, UK, 2019. [Google Scholar]
- Koo, O.M.; Rubinstein, I.; Onyuksel, H. Role of nanotechnology in targeted drug delivery and imaging: A concise review. Nanomed. Nanotechnol. Biol. Med. 2005, 1, 193–212. [Google Scholar] [CrossRef]
- Binnemars-Postma, K.; Storm, G.; Prakash, J. Nanomedicine strategies to target tumor-associated macrophages. Int. J. Mol. Sci. 2017, 18, 979. [Google Scholar] [CrossRef] [PubMed]
- Dinarvand, R.; Sepehri, N.; Manoochehri, S.; Rouhani, H.; Atyabi, F. Polylactide-co-glycolide nanoparticles for controlled delivery of anticancer agents. Int. J. Nanomed. 2011, 6, 877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canaparo, R.; Foglietta, F.; Giuntini, F.; Della Pepa, C.; Dosio, F.; Serpe, L. Recent developments in antibacterial therapy: Focus on stimuli-responsive drug-delivery systems and therapeutic nanoparticles. Molecules 2019, 24, 1991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suhail, M.; Rosenholm, J.M.; Minhas, M.U.; Badshah, S.F.; Naeem, A.; Khan, K.U.; Fahad, M. Nanogels as drug-delivery systems: A comprehensive overview. Ther. Deliv. 2019, 10, 697–717. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; van Nostrum, C.F.; Mastrobattista, E.; Vermonden, T.; Hennink, W.E. Nanogels for intracellular delivery of biotherapeutics. J. Control. Release 2017, 259, 16–28. [Google Scholar] [CrossRef]
- Ye, Y.; Yu, J.; Gu, Z. Versatile protein nanogels prepared by in situ polymerization. Macromol. Chem. Phys. 2016, 217, 333–343. [Google Scholar] [CrossRef]
- Vauthier, C.; Ponchel, G. Polymer Nanoparticles for Nanomedicines; Springer: Berlin/Heidelberg, Germany, 2017; ISBN 3319414194. [Google Scholar]
- Ramos, J.; Forcada, J.; Hidalgo-Alvarez, R. Cationic polymer nanoparticles and nanogels: From synthesis to biotechnological applications. Chem. Rev. 2014, 114, 367–428. [Google Scholar] [CrossRef]
- Nelemans, L.C.; Gurevich, L. Drug Delivery with Polymeric Nanocarriers—Cellular Uptake Mechanisms. Materials (Basel) 2020, 13, 366. [Google Scholar] [CrossRef] [Green Version]
- Chaubey, P.; Momin, M.; Sawarkar, S. Significance of Ligand-Anchored Polymers for Drug Targeting in the Treatment of Colonic Disorders. Front. Pharmacol. 2019, 10, 1628. [Google Scholar] [CrossRef] [Green Version]
- Bolhassani, A.; Javanzad, S.; Saleh, T.; Hashemi, M.; Aghasadeghi, M.R.; Sadat, S.M. Polymeric nanoparticles: Potent vectors for vaccine delivery targeting cancer and infectious diseases. Hum. Vaccin. Immunother. 2014, 10, 321–332. [Google Scholar] [CrossRef] [Green Version]
- George, A.; Shah, P.A.; Shrivastav, P.S. Natural biodegradable polymers based nano-formulations for drug delivery: A review. Int. J. Pharm. 2019, 561, 244–264. [Google Scholar] [CrossRef] [PubMed]
- Raveendran, S.; Rochani, A.K.; Maekawa, T.; Kumar, D.S. Smart carriers and nanohealers: A nanomedical insight on natural polymers. Materials (Basel) 2017, 10, 929. [Google Scholar] [CrossRef] [PubMed]
- Jana, S.; Jana, S. Natural polymeric biodegradable nanoblend for macromolecules delivery. In Recent Developments in Polymer Macro, Micro and Nano Blends; Elsevier: Amsterdam, The Netherlands, 2017; pp. 289–312. [Google Scholar]
- Peres, C.; Matos, A.I.; Conniot, J.; Sainz, V.; Zupančič, E.; Silva, J.M.; Graça, L.; Gaspar, R.S.; Préat, V.; Florindo, H.F. Poly (lactic acid)-based particulate systems are promising tools for immune modulation. Acta Biomater. 2017, 48, 41–57. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Parmar, A.; Kori, S.; Sandhir, R. PLGA-based nanoparticles: A new paradigm in biomedical applications. TrAC Trends Anal. Chem. 2016, 80, 30–40. [Google Scholar] [CrossRef]
- Jones, R.A.; Cheung, C.Y.; Black, F.E.; Zia, J.K.; Stayton, P.S.; Hoffman, A.S.; Wilson, M.R. Poly (2-alkylacrylic acid) polymers deliver molecules to the cytosol by pH-sensitive disruption of endosomal vesicles. Biochem. J. 2003, 372, 65–75. [Google Scholar] [CrossRef] [Green Version]
- Kusonwiriyawong, C.; Van De Wetering, P.; Hubbell, J.A.; Merkle, H.P.; Walter, E. Evaluation of pH-dependent membrane-disruptive properties of poly (acrylic acid) derived polymers. Eur. J. Pharm. Biopharm. 2003, 56, 237–246. [Google Scholar] [CrossRef]
- Foster, S.; Duvall, C.L.; Crownover, E.F.; Hoffman, A.S.; Stayton, P.S. Intracellular delivery of a protein antigen with an endosomal-releasing polymer enhances CD8 T-cell production and prophylactic vaccine efficacy. Bioconjug. Chem. 2010, 21, 2205–2212. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, T.A.; Aljaeid, B.M. Preparation, characterization, and potential application of chitosan, chitosan derivatives, and chitosan metal nanoparticles in pharmaceutical drug delivery. Drug Des. Devel. Ther. 2016, 10, 483. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Li, J.; Jiang, Z.; Tong, R.; Duan, X.; Bai, L.; Shi, J.-Y. Chitosan, N, N, N-trimethyl chitosan (TMC) and 2-hydroxypropyltrimethyl ammonium chloride chitosan (HTCC): The potential immune adjuvants and nano carriers. Int. J. Biol. Macromol. 2020, 154, 339–348. [Google Scholar] [CrossRef]
- Contreras Lancheros, C.A.; Pelegrino, M.T.; Kian, D.; Tavares, E.R.; Hiraiwa, P.M.; Goldenberg, S.; Nakamura, C.V.; Yamauchi, L.M.; Pinge-Filho, P.; Seabra, A.B. Selective antiprotozoal activity of nitric oxide-releasing chitosan nanoparticles against Trypanosoma cruzi: Toxicity and mechanisms of action. Curr. Pharm. Des. 2018, 24, 830–839. [Google Scholar] [CrossRef]
- Szymańska, E.; Winnicka, K. Stability of chitosan—A challenge for pharmaceutical and biomedical applications. Mar. Drugs 2015, 13, 1819–1846. [Google Scholar] [CrossRef] [PubMed]
- Coya, J.M.; De Matteis, L.; Giraud-Gatineau, A.; Biton, A.; Serrano-Sevilla, I.; Danckaert, A.; Dillies, M.-A.; Gicquel, B.; Jesus, M.; Tailleux, L. Tri-mannose grafting of chitosan nanocarriers remodels the macrophage response to bacterial infection. J. Nanobiotechnol. 2019, 17, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gan, Q.; Wang, T. Chitosan nanoparticle as protein delivery carrier—Systematic examination of fabrication conditions for efficient loading and release. Colloids Surf. B Biointerfaces 2007, 59, 24–34. [Google Scholar] [CrossRef] [PubMed]
- He, Z.; Santos, J.L.; Tian, H.; Huang, H.; Hu, Y.; Liu, L.; Leong, K.W.; Chen, Y.; Mao, H.-Q. Scalable fabrication of size-controlled chitosan nanoparticles for oral delivery of insulin. Biomaterials 2017, 130, 28–41. [Google Scholar] [CrossRef]
- Zhang, S.; Gao, H.; Bao, G. Physical principles of nanoparticle cellular endocytosis. ACS Nano 2015, 9, 8655–8671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, R.; Roy, K. Intracellular delivery of polymeric nanocarriers: A matter of size, shape, charge, elasticity and surface composition. Ther. Deliv. 2013, 4, 705–723. [Google Scholar] [CrossRef] [PubMed]
- Blanco, E.; Shen, H.; Ferrari, M. Principles of nanoparticle design for overcoming biological barriers to drug delivery. Nat. Biotechnol. 2015, 33, 941. [Google Scholar] [CrossRef] [PubMed]
- Behzadi, S.; Serpooshan, V.; Tao, W.; Hamaly, M.A.; Alkawareek, M.Y.; Dreaden, E.C.; Brown, D.; Alkilany, A.M.; Farokhzad, O.C.; Mahmoudi, M. Cellular uptake of nanoparticles: Journey inside the cell. Chem. Soc. Rev. 2017, 46, 4218–4244. [Google Scholar] [CrossRef]
- Bobo, D.; Robinson, K.J.; Islam, J.; Thurecht, K.J.; Corrie, S.R. Nanoparticle-based medicines: A review of FDA-approved materials and clinical trials to date. Pharm. Res. 2016, 33, 2373–2387. [Google Scholar] [CrossRef]
- Zhao, Z.; Ukidve, A.; Krishnan, V.; Mitragotri, S. Effect of physicochemical and surface properties on in vivo fate of drug nanocarriers. Adv. Drug Deliv. Rev. 2019, 143, 3–21. [Google Scholar] [CrossRef]
- Sahin, A.; Esendagli, G.; Yerlikaya, F.; Caban-Toktas, S.; Yoyen-Ermis, D.; Horzum, U.; Aktas, Y.; Khan, M.; Couvreur, P.; Capan, Y. A small variation in average particle size of PLGA nanoparticles prepared by nanoprecipitation leads to considerable change in nanoparticles’ characteristics and efficacy of intracellular delivery. Artif. cells Nanomed. Biotechnol. 2017, 45, 1657–1664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattacharjee, S. DLS and zeta potential–what they are and what they are not? J. Control. Release 2016, 235, 337–351. [Google Scholar] [CrossRef] [PubMed]
- Toti, U.S.; Guru, B.R.; Hali, M.; McPharlin, C.M.; Wykes, S.M.; Panyam, J.; Whittum-Hudson, J.A. Targeted delivery of antibiotics to intracellular chlamydial infections using PLGA nanoparticles. Biomaterials 2011, 32, 6606–6613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenwood, R. Review of the measurement of zeta potentials in concentrated aqueous suspensions using electroacoustics. Adv. Colloid Interface Sci. 2003, 106, 55–81. [Google Scholar] [CrossRef]
- Verma, A.; Stellacci, F. Effect of surface properties on nanoparticle–cell interactions. Small 2010, 6, 12–21. [Google Scholar] [CrossRef]
- Yue, Z.-G.; Wei, W.; Lv, P.-P.; Yue, H.; Wang, L.-Y.; Su, Z.-G.; Ma, G.-H. Surface charge affects cellular uptake and intracellular trafficking of chitosan-based nanoparticles. Biomacromolecules 2011, 12, 2440–2446. [Google Scholar] [CrossRef]
- Yuan, Y.; Mao, C.; Du, X.; Du, J.; Wang, F.; Wang, J. Surface charge switchable nanoparticles based on zwitterionic polymer for enhanced drug delivery to tumor. Adv. Mater. 2012, 24, 5476–5480. [Google Scholar] [CrossRef]
- Reis, C.P.; Neufeld, R.J.; Ribeiro, A.J.; Veiga, F.; Nanoencapsulation, I. Methods for preparation of drug-loaded polymeric nanoparticles. Nanomed. Nanotechnol. Biol. Med. 2006, 2, 8–21. [Google Scholar] [CrossRef] [Green Version]
- Lepeltier, E.; Bourgaux, C.; Couvreur, P. Nanoprecipitation and the “Ouzo effect”: Application to drug delivery devices. Adv. Drug Deliv. Rev. 2014, 71, 86–97. [Google Scholar] [CrossRef]
- Santos, A.C.; Caldas, M.; Pattekari, P.; Ribeiro, C.F.; Ribeiro, A.J.; Lvov, Y.; Veiga, F. Layer-by-Layer coated drug-core nanoparticles as versatile delivery platforms. In Design and Development of New Nanocarriers; Elsevier: Amsterdam, The Netherlands, 2018; pp. 595–635. [Google Scholar]
- Salaün, F. Microencapsulation technology for smart textile coatings. In Active Coatings for Smart Textiles; Elsevier: Amsterdam, The Netherlands, 2016; pp. 179–220. [Google Scholar]
- Sundar, S.; Kundu, J.; Kundu, S.C. Biopolymeric nanoparticles. Sci. Technol. Adv. Mater. 2010, 11, 14104. [Google Scholar] [CrossRef]
- Masotti, A.; Ortaggi, G. Chitosan micro-and nanospheres: Fabrication and applications for drug and DNA delivery. Mini Rev. Med. Chem. 2009, 9, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Muñoz, N.; Alcalá-Alcala, S.; Quintanar-Guerrero, D. Preparation of Polymer Nanoparticles by the Emulsification-Solvent Evaporation Method: From Vanderhoff’s Pioneer Approach to Recent Adaptations. In Polymer Nanoparticles for Nanomedicines; Vauthier, C., Ponchel, G., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 87–121. [Google Scholar]
- Anton, N.; Benoit, J.-P.; Saulnier, P. Design and production of nanoparticles formulated from nano-emulsion templates—A review. J. Control. Release 2008, 128, 185–199. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Eral, H.B.; Hatton, T.A.; Doyle, P.S. Nanoemulsions: Formation, properties and applications. Soft Matter 2016, 12, 2826–2841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birnbaum, D.T.; Kosmala, J.D.; Brannon-Peppas, L. Optimization of preparation techniques for poly (lactic acid-co-glycolic acid) nanoparticles. J. Nanopart. Res. 2000, 2, 173–181. [Google Scholar] [CrossRef]
- Dalwadi, G.; Benson, H.A.E.; Chen, Y. Comparison of diafiltration and tangential flow filtration for purification of nanoparticle suspensions. Pharm. Res. 2005, 22, 2152–2162. [Google Scholar] [CrossRef]
- Hederström, I. Purification and Surface Modification of Polymeric Nanoparticles for Medical Applications. Master’s Thesis, Linköping University, Linköping, Sweden, 2008. [Google Scholar]
- Ahmad, N.; Gopinath, P.; Dutta, R. 3D Printing Technology in Nanomedicine; Elsevier: Amsterdam, The Netherlands, 2019; ISBN 0128158913. [Google Scholar]
- Zhao, D.; Han, A.; Qiu, M. Ice lithography for 3D nanofabrication. Sci. Bull. 2019, 64, 865–871. [Google Scholar] [CrossRef] [Green Version]
- Sur, S.; Rathore, A.; Dave, V.; Reddy, K.R.; Chouhan, R.S.; Sadhu, V. Recent developments in functionalized polymer nanoparticles for efficient drug delivery system. Nano Struct. Nano Objects 2019, 20, 100397. [Google Scholar] [CrossRef]
- Wan, K.Y.; Wong, K.W.; Chow, A.H.L.; Chow, S.F. Impact of molecular rearrangement of amphiphilic stabilizers on physical stability of itraconazole nanoparticles prepared by flash nanoprecipitation. Int. J. Pharm. 2018, 542, 221–231. [Google Scholar] [CrossRef] [Green Version]
- Rai, P.; Gautam, N.; Chandra, H.; Kumar, V. Generation of Micro/Nano Scale Particles and Capsules by Electro hydrodynamic Atomization (EHDA) Process. Mater. Today Proc. 2019, 18, 4374–4383. [Google Scholar] [CrossRef]
- Bruschi, M.L. Strategies to Modify the Drug Release from Pharmaceutical Systems; Woodhead Publishing: Cambridge, UK, 2015; Chapter 5; ISBN 0081001126. [Google Scholar]
- Fredenberg, S.; Wahlgren, M.; Reslow, M.; Axelsson, A. The mechanisms of drug release in poly (lactic-co-glycolic acid)-based drug delivery systems—A review. Int. J. Pharm. 2011, 415, 34–52. [Google Scholar] [CrossRef]
- Jäger, E.; Venturini, C.G.; Poletto, F.S.; Colomé, L.M.; Pohlmann, J.P.U.; Bernardi, A.; Battastini, A.M.O.; Guterres, S.S.; Pohlmann, A.R. Sustained release from lipid-core nanocapsules by varying the core viscosity and the particle surface area. J. Biomed. Nanotechnol. 2009, 5, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Wu, J.; Ding, C.; Cui, Y.; Zhou, Y.; Li, Y.; Deng, M.; Wang, C.; Xu, K.; Ren, J.; et al. Epidemiological features of and changes in incidence of infectious diseases in China in the first decade after the SARS outbreak: An observational trend study. Lancet Infect. Dis. 2017, 17, 716–725. [Google Scholar] [CrossRef]
- Qasim, M.; Lim, D.-J.; Park, H.; Na, D. Nanotechnology for Diagnosis and Treatment of Infectious Diseases. J. Nanosci. Nanotechnol. 2014, 14, 7374–7387. [Google Scholar] [CrossRef] [PubMed]
- Sundar, S.; Prajapati, V.K. Drug targeting to infectious diseases by nanoparticles surface functionalized with special biomolecules. Curr. Med. Chem. 2012, 19, 3196–3202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garg, A.; Bhalala, K.; Tomar, D.S.; Wahajuddin, M. Nanomedicine: Emerging Trends in Treatment of Malaria. In Antimicrobial Nanoarchitectonics; Elsevier: Amsterdam, The Netherlands, 2017; pp. 475–509. [Google Scholar]
- Hill, L.E.; Taylor, T.M.; Gomes, C. Antimicrobial efficacy of poly (DL-lactide-co-glycolide) (PLGA) nanoparticles with entrapped cinnamon bark extract against Listeria monocytogenes and Salmonella typhimurium. J. Food Sci. 2013, 78, N626–N632. [Google Scholar] [CrossRef]
- Bruni, N.; Stella, B.; Giraudo, L.; Della Pepa, C.; Gastaldi, D.; Dosio, F. Nanostructured delivery systems with improved leishmanicidal activity: A critical review. Int. J. Nanomed. 2017, 12, 5289–5311. [Google Scholar] [CrossRef] [Green Version]
- Casadevall, A. Evolution of Intracellular Pathogens. Annu. Rev. Microbiol. 2008, 62, 19–33. [Google Scholar] [CrossRef] [Green Version]
- Darville, T.; Hiltke, T.J. Pathogenesis of genital tract disease due to Chlamydia trachomatis. J. Infect. Dis. 2010, 201 (Suppl. 2), S114–S125. [Google Scholar] [CrossRef] [Green Version]
- Witkin, S.S.; Minis, E.; Athanasiou, A.; Leizer, J.; Linhares, I.M. Chlamydia trachomatis: The Persistent Pathogen. Clin. Vaccine Immunol. 2017, 24. [Google Scholar] [CrossRef] [Green Version]
- Garfoot, A.L.; Rappleye, C.A. Histoplasma capsulatum surmounts obstacles to intracellular pathogenesis. FEBS J. 2016, 283, 619–633. [Google Scholar] [CrossRef] [Green Version]
- Boucher, H.W.; Talbot, G.H.; Benjamin, D.K.; Bradley, J.; Guidos, R.J.; Jones, R.N.; Murray, B.E.; Bonomo, R.A.; Gilbert, D. 10 × ’20 Progress—Development of New Drugs Active Against Gram-Negative Bacilli: An Update From the Infectious Diseases Society of America. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2013, 56, 1685–1694. [Google Scholar] [CrossRef] [Green Version]
- Andrei, S.; Valeanu, L.; Chirvasuta, R.; Stefan, M.-G. New FDA approved antibacterial drugs: 2015–2017. Discoveries (Craiova, Rom.) 2018, 6, e81. [Google Scholar] [CrossRef] [PubMed]
- Huh, A.J.; Kwon, Y.J. “Nanoantibiotics”: A new paradigm for treating infectious diseases using nanomaterials in the antibiotics resistant era. J. Control. Release 2011, 156, 128–145. [Google Scholar] [CrossRef] [PubMed]
- Alonso, A.; Garcia-del Portillo, F. Hijacking of eukaryotic functions by intracellular bacterial pathogens. Int. Microbiol. 2004, 7, 181–191. [Google Scholar] [PubMed]
- Ventola, C.L. The antibiotic resistance crisis: Part 1: Causes and threats. P T 2015, 40, 277–283. [Google Scholar] [PubMed]
- Nagle, A.S.; Khare, S.; Kumar, A.B.; Supek, F.; Buchynskyy, A.; Mathison, C.J.N.; Chennamaneni, N.K.; Pendem, N.; Buckner, F.S.; Gelb, M.H.; et al. Recent developments in drug discovery for leishmaniasis and human African trypanosomiasis. Chem. Rev. 2014, 114, 11305–11347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volpedo, G.; Costa, L.; Ryan, N.; Halsey, G.; Satoskar, A.; Oghumu, S. Nanoparticulate drug delivery systems for the treatment of neglected tropical protozoan diseases. J. Venom. Anim. Toxins Incl. Trop. Dis. 2019, 25. [Google Scholar] [CrossRef] [PubMed]
- Abushaheen, M.A.; Muzaheed; Fatani, A.J.; Alosaimi, M.; Mansy, W.; George, M.; Acharya, S.; Rathod, S.; Divakar, D.D.; Jhugroo, C.; et al. Antimicrobial resistance, mechanisms and its clinical significance. Dis. Month 2020, 100971. [Google Scholar] [CrossRef]
- Li, B.; Webster, T.J. Bacteria antibiotic resistance: New challenges and opportunities for implant-associated orthopedic infections. J. Orthop. Res. 2018, 36, 22–32. [Google Scholar] [CrossRef] [Green Version]
- Munita, J.M.; Arias, C.A. Mechanisms of Antibiotic Resistance. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef] [Green Version]
- Pelgrift, R.Y.; Friedman, A.J. Nanotechnology as a therapeutic tool to combat microbial resistance. Adv. Drug Deliv. Rev. 2013, 65, 1803–1815. [Google Scholar] [CrossRef] [PubMed]
- Justo, J.A.; Bosso, J. Adverse Reactions Associated with Systemic Polymyxin Therapy. Pharm. J. Hum. Pharmacol. Drug Ther. 2014, 35. [Google Scholar] [CrossRef] [PubMed]
- Piddock, L.J.; Jin, Y.F.; Griggs, D.J. Effect of hydrophobicity and molecular mass on the accumulation of fluoroquinolones by Staphylococcus aureus. J. Antimicrob. Chemother. 2001, 47, 261–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchant, J. When antibiotics turn toxic. Nature 2018, 555, 431–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razonable, R.R. Antiviral drugs for viruses other than human immunodeficiency virus. Mayo Clin. Proc. 2011, 86, 1009–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Center for Biotechnology Information. PubChem Database. Enfuvirtide, CID=16130199. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/16130199 (accessed on 20 July 2020).
- Ryu, W.-S. Antiviral Therapy. In Molecular Virology of Human Pathogenic Viruses; Academic Press: Boston, MA, USA, 2017; pp. 367–381. ISBN 978-0-12-800838-6. [Google Scholar]
- De Clercq, E.; Li, G. Approved Antiviral Drugs over the Past 50 Years. Clin. Microbiol. Rev. 2016, 29, 695–747. [Google Scholar] [CrossRef] [Green Version]
- Fiandra, L.; Colombo, M.; Mazzucchelli, S.; Truffi, M.; Santini, B.; Allevi, R.; Nebuloni, M.; Capetti, A.; Rizzardini, G.; Prosperi, D.; et al. Nanoformulation of antiretroviral drugs enhances their penetration across the blood brain barrier in mice. Nanomedicine 2015, 11, 1387–1397. [Google Scholar] [CrossRef] [Green Version]
- Kapishon, V.; Allison-Logan, S.; Whitney, R.; Cunningham, M.; Szewczuk, M.; Neufeld, R. Oseltamivir-conjugated polymeric micelles prepared by RAFT living radical polymerization as a new active tumor targeting drug delivery platform. Biomater. Sci. 2016, 4. [Google Scholar] [CrossRef] [Green Version]
- Giri, N.; Tomar, P.; Karwasara, V.; Pandey, R.; Dixit, V. Targeted novel surface-modified nanoparticles for interferon delivery for the treatment of hepatitis B. Acta Biochim. Biophys. Sin. (Shanghai) 2011, 43, 877–883. [Google Scholar] [CrossRef] [Green Version]
- Imperiale, J.; Schlachet, I.; Lewicki, M.; Sosnik, A.; Biglione, M. Oral Pharmacokinetics of a Chitosan-Based Nano- Drug Delivery System of Interferon Alpha. Polymers 2019, 11, 1862. [Google Scholar] [CrossRef] [Green Version]
- Kenedi, C.A.; Goforth, H.W. A systematic review of the psychiatric side-effects of efavirenz. AIDS Behav. 2011, 15, 1803–1818. [Google Scholar] [CrossRef] [PubMed]
- National Center for Biotechnology Information. PubChem Database. Efavirenz, CID=64139. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/64139 (accessed on 20 July 2020).
- Rocha, L.M.; Baldan, D.C.d.S.; de Souza, A.L.; Chaim, E.A.; Pavin, E.J.; Alegre, S.M. Body composition and metabolic profile in adults with vitamin D deficiency. Rev. Nutr. 2017, 30, 419–430. [Google Scholar] [CrossRef] [Green Version]
- Nett, J.E.; Andes, D.R. Antifungal Agents: Spectrum of Activity, Pharmacology, and Clinical Indications. Infect. Dis. Clin. North Am. 2016, 30, 51–83. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Sequeda, N.; Torres, R.; Ortiz, C. Synthesis, characterization, and in vitro activity against Candida spp. of fluconazole encapsulated on cationic and conventional nanoparticles of poly(lactic-co-glycolic acid). Nanotechnol. Sci. Appl. 2017, 10, 95–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parente, J.; Bailao, A.; Amaral, A.; Taborda, C.; Paccez, J.; Borges, C.; Pereira, M. Antifungal Resistance, Metabolic Routes as Drug Targets, and New Antifungal Agents: An Overview about Endemic Dimorphic Fungi. Mediat. Inflamm. 2017, 2017, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Souza, A.C.O.; Amaral, A.C. Antifungal Therapy for Systemic Mycosis and the Nanobiotechnology Era: Improving Efficacy, Biodistribution and Toxicity. Front. Microbiol. 2017, 8, 336. [Google Scholar] [CrossRef] [Green Version]
- Wolfram, J.; Nizzero, S.; Liu, H.; Li, F.; Zhang, G.; Li, Z.; Shen, H.; Blanco, E.; Ferrari, M. A chloroquine-induced macrophage-preconditioning strategy for improved nanodelivery. Sci. Rep. 2017, 7. [Google Scholar] [CrossRef] [Green Version]
- Lima, T.L.C.; Feitosa, R.D.C.; Santos-Silva, D.; Santos-Silva, D.; Maria, A.; Siqueira, E.M.D.S.; Machado, P.R.L.; Cornélio, A.M.; Do Egito, E.S.T.; Fernandes-Pedrosa, M.D.F.; et al. Improving Encapsulation of Hydrophilic Chloroquine Diphosphate into Biodegradable Nanoparticles: A Promising Approach against Herpes Virus Simplex-1 Infection. Pharmaceutics 2018, 10, 255. [Google Scholar] [CrossRef] [Green Version]
- Jana, S.S.; Jana, S.S.; Eleraky, N.E.; Allam, A.; Hassan, S.B.; Omar, M.M.; Gao, F.; Xu, L.; Yang, B.B.; Fan, F.; et al. PubChem Database. Chloroquine, CID = 2719. Int. J. Pharm. 2019, 10, 3–21. [Google Scholar] [CrossRef] [Green Version]
- Sangshetti, J.; Khan, F.; Kulkarni, A.; Arote, R.; Patil, R. Antileishmanial drug discovery: Comprehensive review of the last 10 years. RSC Adv. 2015, 5. [Google Scholar] [CrossRef]
- Hoagland, D.T.; Liu, J.; Lee, R.B.; Lee, R.E. New agents for the treatment of drug-resistant Mycobacterium tuberculosis. Adv. Drug Deliv. Rev. 2016, 102, 55–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Tuberculosis Report 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization. HIV Drug Resistance Report 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Wheat, J.; Marichal, P.; Vanden Bossche, H.; Le Monte, A.; Connolly, P. Hypothesis on the mechanism of resistance to fluconazole in Histoplasma capsulatum. Antimicrob. Agents Chemother 1997, 41, 410–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakai, J.B. Pharmacokinetics: The Absorption, Distribution, and Excretion of Drugs. Pract. Pharmacol. Pharm. Tech. 2008, 27–40. [Google Scholar]
- Blaschke, T. Pharmacokinetics: Absorption, Distribution, Metabolism, Excretion Overview Chapter. In Principles of Pharmacogenetics and Pharmacogenomics; Flockhart, D., Goldstein, D.B., Altman, R.B., Eds.; Cambridge University Press: Cambridge, UK, 2012; pp. 21–26. ISBN 9780521885379. [Google Scholar]
- Romero, E.L.; Morilla, M.J. Drug delivery systems against leishmaniasis? Still an open question. Expert Opin. Drug Deliv. 2008, 5, 805–823. [Google Scholar] [CrossRef] [PubMed]
- Cai, R.; Chen, C. The Crown and the Scepter: Roles of the Protein Corona in Nanomedicine. Adv. Mater. 2019, 31, e1805740. [Google Scholar] [CrossRef]
- Nehoff, H.; Parayath, N.N.; Domanovitch, L.; Taurin, S.; Greish, K. Nanomedicine for drug targeting: Strategies beyond the enhanced permeability and retention effect. Int. J. Nanomed. 2014, 9, 2539–2555. [Google Scholar] [CrossRef] [Green Version]
- Chu, D.; Gao, J.; Wang, Z. Neutrophil-Mediated Delivery of Therapeutic Nanoparticles across Blood Vessel Barrier for Treatment of Inflammation and Infection. ACS Nano 2015, 9, 11800–11811. [Google Scholar] [CrossRef] [Green Version]
- Le Roy, C.; Wrana, J.L. Clathrin-and non-clathrin-mediated endocytic regulation of cell signalling. Nat. Rev. Mol. Cell Biol. 2005, 6, 112–126. [Google Scholar] [CrossRef]
- Homayun, B.; Lin, X.; Choi, H.-J. Challenges and Recent Progress in Oral Drug Delivery Systems for Biopharmaceuticals. Pharmaceutics 2019, 11, 129. [Google Scholar] [CrossRef] [Green Version]
- Reinholz, J.; Landfester, K.; Mailander, V. The challenges of oral drug delivery via nanocarriers. Drug Deliv. 2018, 25, 1694–1705. [Google Scholar] [CrossRef]
- Leal, J.; Smyth, H.D.C.; Ghosh, D. Physicochemical properties of mucus and their impact on transmucosal drug delivery. Int. J. Pharm. 2017, 532, 555–572. [Google Scholar] [CrossRef] [PubMed]
- Newman, S.P. Drug delivery to the lungs: Challenges and opportunities. Ther. Deliv. 2017, 8, 647–661. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.H.; Tiemann, K.M.; Hunstad, D.A.; Elsabahy, M.; Wooley, K.L. Polymeric nanoparticles in development for treatment of pulmonary infectious diseases. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2016, 8, 842–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, B.C.; DeLouise, L.A. Nanoparticle-Enabled Transdermal Drug Delivery Systems for Enhanced Dose Control and Tissue Targeting. Molecules 2016, 21. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.W.; Xu, Z.P.; Grice, J.; Zvyagin, A.V.; Roberts, M.S.; Liu, X. Penetration of nanoparticles into human skin. Curr. Pharm. Des. 2013, 19, 6353–6366. [Google Scholar] [CrossRef]
- Portnoy, D.A.; Auerbuch, V.; Glomski, I.J. The cell biology of Listeria monocytogenes infection: The intersection of bacterial pathogenesis and cell-mediated immunity. J. Cell Biol. 2002, 158, 409–414. [Google Scholar] [CrossRef] [Green Version]
- MacGurn, J.A.; Cox, J.S. A Genetic Screen for Mycobacterium tuberculosis Mutants Defective for Phagosome Maturation Arrest Identifies Components of the ESX-1 Secretion System. Infect. Immun. 2007, 75, 2668–2678. [Google Scholar] [CrossRef] [Green Version]
- Vergne, I.; Chua, J.; Lee, H.-H.; Lucas, M.; Belisle, J.; Deretic, V. Mechanism of phagolysosome biogenesis block by viable Mycobacterium tuberculosis. Proc. Natl. Acad. Sci. USA 2005, 102, 4033–4038. [Google Scholar] [CrossRef] [Green Version]
- Méresse, S.; Steele-Mortimer, O.; Finlay, B.B.; Gorvel, J.-P. The rab7 GTPase controls the maturation of Salmonella typhimurium-containing vacuoles in HeLa cells. EMBO J. 1999, 18, 4394–4403. [Google Scholar] [CrossRef] [Green Version]
- Newton, H.J.; McDonough, J.A.; Roy, C.R. Effector Protein Translocation by the Coxiella burnetii Dot/Icm Type IV Secretion System Requires Endocytic Maturation of the Pathogen-Occupied Vacuole. PLoS ONE 2013, 8, e54566. [Google Scholar] [CrossRef] [Green Version]
- Panyam, J.; Labhasetwar, V. Dynamics of endocytosis and exocytosis of poly (D, L-lactide-co-glycolide) nanoparticles in vascular smooth muscle cells. Pharm. Res. 2003, 20, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Panyam, J.; Zhou, W.-Z.; Prabha, S.; Sahoo, S.K.; Labhasetwar, V. Rapid endo-lysosomal escape of poly(DL-lactide-co-glycolide) nanoparticles: Implications for drug and gene delivery. FASEB J. 2002, 16, 1217–1226. [Google Scholar] [CrossRef] [PubMed]
- Parodi, A.; Corbo, C.; Cevenini, A.; Molinaro, R.; Palomba, R.; Pandolfi, L.; Agostini, M.; Salvatore, F.; Tasciotti, E. Enabling cytoplasmic delivery and organelle targeting by surface modification of nanocarriers. Nanomedicine (Lond) 2015, 10, 1923–1940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandgren, S.; Cheng, F.; Belting, M. Nuclear targeting of macromolecular polyanions by an HIV-Tat derived peptide. Role for cell-surface proteoglycans. J. Biol. Chem. 2002, 277, 38877–38883. [Google Scholar] [CrossRef] [Green Version]
- Tiku, V.; Tan, M.-W.; Dikic, I. Mitochondrial Functions in Infection and Immunity. Trends Cell Biol. 2020, 30, 263–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, D.; Joglekar, A.P.; Williams, A.L.; Hay, J.C. Subunit structure of a mammalian ER/Golgi SNARE complex. J. Biol. Chem. 2000, 275, 39631–39639. [Google Scholar] [CrossRef] [Green Version]
- Glingston, R.S.; Deb, R.; Kumar, S.; Nagotu, S. Organelle dynamics and viral infections: At cross roads. Microbes Infect. 2019, 21, 20–32. [Google Scholar] [CrossRef]
- Novoa, R.R.; Calderita, G.; Arranz, R.; Fontana, J.; Granzow, H.; Risco, C. Virus factories: Associations of cell organelles for viral replication and morphogenesis. Biol. Cell 2005, 97, 147–172. [Google Scholar] [CrossRef]
- Capitani, M.; Sallese, M. The KDEL receptor: New functions for an old protein. FEBS Lett. 2009, 583, 3863–3871. [Google Scholar] [CrossRef] [Green Version]
- Jahagirdar, P.; Lokhande, A.S.; Dandekar, P.; Devarajan, P.V. Mannose Receptor and Targeting Strategies. In Targeted Intracellular Drug Delivery by Receptor Mediated Endocytosis; Springer: Berlin/Heidelberg, Germany, 2019; pp. 433–456. [Google Scholar]
- Kamaruzzaman, N.F.; Tan, L.P.; Hamdan, R.H.; Choong, S.S.; Wong, W.K.; Gibson, A.J.; Chivu, A.; de Fatima Pina, M. Antimicrobial polymers: The potential replacement of existing antibiotics? Int. J. Mol. Sci. 2019, 20, 2747. [Google Scholar] [CrossRef] [Green Version]
- Masri, A.; Anwar, A.; Khan, N.A.; Siddiqui, R. The Use of Nanomedicine for Targeted Therapy against Bacterial Infections. Antibiotics 2019, 8, 260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, F.; Wern, J.E.; Gavins, F.; Andersen, P.; Follmann, F.; Foged, C. A strong adjuvant based on glycol-chitosan-coated lipid-polymer hybrid nanoparticles potentiates mucosal immune responses against the recombinant Chlamydia trachomatis fusion antigen CTH522. J. Control. Release 2018, 271, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Xu, L.; Yang, B.; Fan, F.; Yang, L. Kill the Real with the Fake: Eliminate Intracellular Staphylococcus aureus Using Nanoparticle Coated with Its Extracellular Vesicle Membrane as Active-Targeting Drug Carrier. ACS Infect. Dis. 2018, 5, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Tariq, S.; Rahim, A.; Muhammad, N.; Rahman, S.U.; Azhar, U.; Sultana, K.; Sharif, F.; Siddiqi, S.A.; Zaman, M.; Rehman, F. Controllable delivery from gentamicin loaded polycaprolactone/grafted silica nanoparticles composite mats. J. Mol. Liq. 2019, 290, 111205. [Google Scholar] [CrossRef]
- Eleraky, N.E.; Allam, A.; Hassan, S.B.; Omar, M.M. Nanomedicine Fight against Antibacterial Resistance: An Overview of the Recent Pharmaceutical Innovations. Pharmaceutics 2020, 12, 142. [Google Scholar] [CrossRef] [Green Version]
- Lakshminarayanan, R.; Ye, E.; Young, D.J.; Li, Z.; Loh, X.J. Recent advances in the development of antimicrobial nanoparticles for combating resistant pathogens. Adv. Healthc. Mater. 2018, 7, 1701400. [Google Scholar] [CrossRef] [Green Version]
- Date, A.A.; Hanes, J.; Ensign, L.M. Nanoparticles for oral delivery: Design, evaluation and state-of-the-art. J. Control. Release 2016, 240, 504–526. [Google Scholar] [CrossRef] [Green Version]
- Martins, J.P.; D’Auria, R.; Liu, D.; Fontana, F.; Ferreira, M.P.A.; Correia, A.; Kemell, M.; Moslova, K.; Mäkilä, E.; Salonen, J. Engineered Multifunctional Albumin-Decorated Porous Silicon Nanoparticles for FcRn Translocation of Insulin. Small 2018, 14, 1800462. [Google Scholar] [CrossRef]
- Gulfam, M.; Sahle, F.F.; Lowe, T.L. Design strategies for chemical-stimuli-responsive programmable nanotherapeutics. Drug Discov. Today 2019, 24, 129–147. [Google Scholar] [CrossRef]
- Mosaiab, T.; Farr, D.C.; Kiefel, M.J.; Houston, T.A. Carbohydrate-based nanocarriers and their application to target macrophages and deliver antimicrobial agents. Adv. Drug Deliv. Rev. 2019, 151, 94–129. [Google Scholar] [CrossRef]
- Malik, E.; Dennison, S.R.; Harris, F.; Phoenix, D.A. pH dependent antimicrobial peptides and proteins, their mechanisms of action and potential as therapeutic agents. Pharmaceuticals 2016, 9, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pazos-Ortiz, E.; Roque-Ruiz, J.H.; Hinojos-Márquez, E.A.; López-Esparza, J.; Donohué-Cornejo, A.; Cuevas-González, J.C.; Espinosa-Cristóbal, L.F.; Reyes-López, S.Y. Dose-dependent antimicrobial activity of silver nanoparticles on polycaprolactone fibers against gram-positive and gram-negative bacteria. J. Nanomater. 2017, 2017, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Benhacine, F.; siham Hadj-Hamou, A.; Habi, A. Development of long-term antimicrobial poly (ε-caprolactone)/silver exchanged montmorillonite nanocomposite films with silver ion release property for active packaging use. Polym. Bull. 2016, 73, 1207–1227. [Google Scholar] [CrossRef]
- Jiang, L.; Greene, M.K.; Insua, J.L.; Pessoa, J.S.; Small, D.M.; Smyth, P.; McCann, A.P.; Cogo, F.; Bengoechea, J.A.; Taggart, C.C. Clearance of intracellular Klebsiella pneumoniae infection using gentamicin-loaded nanoparticles. J. Control. Release 2018, 279, 316–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abkar, M.; Fasihi-Ramandi, M.; Kooshki, H.; Lotfi, A.S. Intraperitoneal immunization with Urease loaded N-trimethyl Chitosan nanoparticles elicits high protection against Brucella melitensis and Brucella abortus infections. Immunol. Lett. 2018, 199, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Salzano, G.; Wankar, J.; Ottani, S.; Villemagne, B.; Baulard, A.R.; Willand, N.; Brodin, P.; Manet, I.; Gref, R. Cyclodextrin-based nanocarriers containing a synergic drug combination: A potential formulation for pulmonary administration of antitubercular drugs. Int. J. Pharm. 2017, 531, 577–587. [Google Scholar] [CrossRef]
- Puig-Rigall, J.; Fernández-Rubio, C.; González-Benito, J.; Houston, J.E.; Radulescu, A.; Nguewa, P.; González-Gaitano, G. Structural characterization by scattering and spectroscopic methods and biological evaluation of polymeric micelles of poloxamines and TPGS as nanocarriers for miltefosine delivery. Int. J. Pharm. 2020, 578, 119057. [Google Scholar] [CrossRef]
- Leporati, A.; Gupta, S.; Bolotin, E.; Castillo, G.; Alfaro, J.; Gottikh, M.B.; Bogdanov, A.A., Jr. Antiretroviral Hydrophobic Core Graft-Copolymer Nanoparticles: The Effectiveness against Mutant HIV-1 Strains and in Vivo Distribution after Topical Application. Pharm. Res. 2019, 36, 73. [Google Scholar] [CrossRef]
- Chen, P.; Zhang, X.; Venosa, A.; Lee, I.H.; Myers, D.; Holloway, J.A.; Prud’homme, R.K.; Gao, D.; Szekely, Z.; Laskin, J.D. A Novel Bivalent Mannosylated Targeting Ligand Displayed on Nanoparticles Selectively Targets Anti-Inflammatory M2 Macrophages. Pharmaceutics 2020, 12, 243. [Google Scholar] [CrossRef] [Green Version]
- Shang, S.; Kats, D.; Cao, L.; Morgun, E.; Velluto, D.; He, Y.; Xu, Q.; Wang, C.-R.; Scott, E.A. Induction of mycobacterium tuberculosis lipid-specific T cell responses by pulmonary delivery of mycolic acid-loaded polymeric micellar Nanocarriers. Front. Immunol. 2018, 9, 2709. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Liang, R.; Xu, J.; Shen, L.; Gao, J.; Wang, X.; Wang, N.; Shou, D.; Hu, Y. Efficient induction of antimicrobial activity with vancomycin nanoparticle-loaded poly (trimethylene carbonate) localized drug delivery system. Int. J. Nanomed. 2017, 12, 1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pei, Y.; Mohamed, M.F.; Seleem, M.N.; Yeo, Y. Particle engineering for intracellular delivery of vancomycin to methicillin-resistant Staphylococcus aureus (MRSA)-infected macrophages. J. Control. Release 2017, 267, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Güncüm, E.; Işıklan, N.; Anlaş, C.; Ünal, N.; Bulut, E.; Bakırel, T. Development and characterization of polymeric-based nanoparticles for sustained release of amoxicillin–an antimicrobial drug. Artif. Cells Nanomed. Biotechnol. 2018, 46, 964–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gámez, E.; Elizondo-Castillo, H.; Tascon, J.; García-Salinas, S.; Navascues, N.; Mendoza, G.; Arruebo, M.; Irusta, S. Antibacterial Effect of Thymol Loaded SBA-15 Nanorods Incorporated in PCL Electrospun Fibers. Nanomaterials 2020, 10, 616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palza, H. Antimicrobial polymers with metal nanoparticles. Int. J. Mol. Sci. 2015, 16, 2099–2116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, I.H.; Palombo, M.S.; Zhang, X.; Szekely, Z.; Sinko, P.J. Design and evaluation of a CXCR4 targeting peptide 4DV3 as an HIV entry inhibitor and a ligand for targeted drug delivery. Eur. J. Pharm. Biopharm. 2019, 138, 11–22. [Google Scholar]
- Mahmood, K.; Zia, K.M.; Zuber, M.; Salman, M.; Anjum, M.N. Recent developments in curcumin and curcumin based polymeric materials for biomedical applications: A review. Int. J. Biol. Macromol. 2015, 81, 877–890. [Google Scholar] [CrossRef]
- Yallapu, M.M.; Nagesh, P.K.B.; Jaggi, M.; Chauhan, S.C. Therapeutic applications of curcumin nanoformulations. AAPS J. 2015, 17, 1341–1356. [Google Scholar] [CrossRef] [Green Version]
- Zorofchian Moghadamtousi, S.; Abdul Kadir, H.; Hassandarvish, P.; Tajik, H.; Abubakar, S.; Zandi, K. A review on antibacterial, antiviral, and antifungal activity of curcumin. Biomed Res. Int. 2014, 2014, 186864. [Google Scholar] [CrossRef]
- Santovito, E.; das Neves, J.; Greco, D.; D’Ascanio, V.; Sarmento, B.; Logrieco, A.F.; Avantaggiato, G. Antimicrobial properties of rosin acids-loaded nanoparticles against antibiotic-sensitive and antibiotic-resistant foodborne pathogens. Artif. cells Nanomed. Biotechnol. 2018, 46, S414–S422. [Google Scholar] [CrossRef] [Green Version]
- Tripodo, G.; Trapani, A.; Torre, M.L.; Giammona, G.; Trapani, G.; Mandracchia, D. Hyaluronic acid and its derivatives in drug delivery and imaging: Recent advances and challenges. Eur. J. Pharm. Biopharm. 2015, 97, 400–416. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Huang, H. Application of hyaluronic acid as carriers in drug delivery. Drug Deliv. 2018, 25, 766–772. [Google Scholar] [CrossRef] [PubMed]
- Sladek, Z.; Rysanek, D. Expression of macrophage CD44 receptor in the course of experimental inflammatory response of bovine mammary gland induced by lipopolysaccharide and muramyl dipeptide. Res. Vet. Sci. 2009, 86, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.P.; Gonçalves, C.; Costa, C.; Sousa, J.; Silva-Gomes, R.; Castro, A.G.; Pedrosa, J.; Appelberg, R.; Gama, F.M. Delivery of LLKKK18 loaded into self-assembling hyaluronic acid nanogel for tuberculosis treatment. J. Control. Release 2016, 235, 112–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahiner, N.; Sagbas, S.; Sahiner, M.; Ayyala, R.S. Polyethyleneimine modified poly (Hyaluronic acid) particles with controllable antimicrobial and anticancer effects. Carbohydr. Polym. 2017, 159, 29–38. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, J.; Chen, W.; Angsantikul, P.; Spiekermann, K.A.; Fang, R.H.; Gao, W.; Zhang, L. Erythrocyte membrane-coated nanogel for combinatorial antivirulence and responsive antimicrobial delivery against Staphylococcus aureus infection. J. Control. Release 2017, 263, 185–191. [Google Scholar] [CrossRef]
- Senanayake, T.H.; Gorantla, S.; Makarov, E.; Lu, Y.; Warren, G.; Vinogradov, S.V. Nanogel-conjugated reverse transcriptase inhibitors and their combinations as novel antiviral agents with increased efficacy against HIV-1 infection. Mol. Pharm. 2015, 12, 4226–4236. [Google Scholar] [CrossRef] [Green Version]
- Akram, M.; Hussain, R. Nanohydrogels: History, development, and applications in drug delivery. Nanocell. Nanohydrogel Matrices Biotechnol. Biomed. Appl. 2017, 297–330. [Google Scholar]
- Vashist, A.; Ghosal, A.; Sharmin, E.; Vashist, A.; Dua, R.; Bhardwaj, V.; Tomatika, A.; Jayant, R.D.; Uthaman, S.; Calderon, M. Nanogels for Biomedical Applications; Royal Society of Chemistry: London, UK, 2017; ISBN 1788012526. [Google Scholar]
- Barros, D.; Costa Lima, S.A.; Cordeiro-da-Silva, A. Surface functionalization of polymeric nanospheres modulates macrophage activation: Relevance in leishmaniasis therapy. Nanomedicine 2015, 10, 387–403. [Google Scholar] [CrossRef] [Green Version]
- Asthana, S.; Gupta, P.K.; Jaiswal, A.K.; Dube, A.; Chourasia, M.K. Overexpressed macrophage mannose receptor targeted nanocapsules-mediated cargo delivery approach for eradication of resident parasite: In vitro and in vivo studies. Pharm. Res. 2015, 32, 2663–2677. [Google Scholar] [CrossRef]
- Chaubey, P.; Mishra, B.; Mudavath, S.L.; Patel, R.R.; Chaurasia, S.; Sundar, S.; Suvarna, V.; Monteiro, M. Mannose-conjugated curcumin-chitosan nanoparticles: Efficacy and toxicity assessments against Leishmania donovani. Int. J. Biol. Macromol. 2018, 111, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Sockolosky, J.T.; Szoka, F.C. The neonatal Fc receptor, FcRn, as a target for drug delivery and therapy. Adv. Drug Deliv. Rev. 2015, 91, 109–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, S.-Y.; Pegu, A.; Rudicell, R.S.; Yang, Z.; Joyce, M.G.; Chen, X.; Wang, K.; Bao, S.; Kraemer, T.D.; Rath, T. Enhanced neonatal Fc receptor function improves protection against primate SHIV infection. Nature 2014, 514, 642–645. [Google Scholar] [CrossRef] [Green Version]
- de Souza, A.; Marins, D.S.S.; Mathias, S.L.; Monteiro, L.M.; Yukuyama, M.N.; Scarim, C.B.; Löbenberg, R.; Bou-Chacra, N.A. Promising nanotherapy in treating leishmaniasis. Int. J. Pharm. 2018, 547, 421–431. [Google Scholar] [CrossRef] [Green Version]
- Saleem, K.; Khursheed, Z.; Hano, C.; Anjum, I.; Anjum, S. Applications of Nanomaterials in Leishmaniasis: A Focus on Recent Advances and Challenges. Nanomaterials 2019, 9, 1749. [Google Scholar] [CrossRef] [Green Version]
- Donnellan, S.; Giardiello, M. Nanomedicines towards targeting intracellular Mtb for the treatment of tuberculosis. J. Interdiscip. Nanomed. 2019, 4, 76–85. [Google Scholar] [CrossRef] [Green Version]
- Patil, T.S.; Deshpande, A.S.; Deshpande, S.; Shende, P. Targeting pulmonary tuberculosis using nanocarrier-based dry powder inhalation: Current status and futuristic need. J. Drug Target. 2019, 27, 12–27. [Google Scholar] [CrossRef]
- Mignani, S.; Tripathi, R.P.; Chen, L.; Caminade, A.-M.; Shi, X.; Majoral, J.-P. New ways to treat tuberculosis using dendrimers as nanocarriers. Pharmaceutics 2018, 10, 105. [Google Scholar] [CrossRef] [Green Version]
- Costa, A.; Pinheiro, M.; Magalhães, J.; Ribeiro, R.; Seabra, V.; Reis, S.; Sarmento, B. The formulation of nanomedicines for treating tuberculosis. Adv. Drug Deliv. Rev. 2016, 102, 102–115. [Google Scholar] [CrossRef]
- Minakshi, P.; Ghosh, M.; Brar, B.; Kumar, R.; Lambe, U.P.; Ranjan, K.; Manoj, J.; Prasad, G. Nano-antimicrobials: A new paradigm for combating mycobacterial resistance. Curr. Pharm. Des. 2019, 25, 1554–1579. [Google Scholar] [CrossRef]
- Singh, K.; Mishra, A.; Sharma, D.; Singh, K. Antiviral and antimicrobial potentiality of nano drugs. In Applications of Targeted Nano Drugs and Delivery Systems; Elsevier: Amsterdam, The Netherlands, 2019; pp. 343–356. [Google Scholar]
- de Souza, M.E.; Verdi, C.M.; de Andrade, E.N.C.; Santos, R.C.V. Antiviral and antimicrobial (antibacterial) potentiality of nano drugs. In Applications of Targeted Nano Drugs and Delivery Systems; Elsevier: Amsterdam, The Netherlands, 2019; pp. 327–342. [Google Scholar]
- Sued, O.; Figueroa, M.I.; Cahn, P. Clinical challenges in HIV/AIDS: Hints for advancing prevention and patient management strategies. Adv. Drug Deliv. Rev. 2016, 103, 5–19. [Google Scholar] [CrossRef] [PubMed]
- Lenjisa, J.L.; Woldu, M.A.; Satessa, G.D. New hope for eradication of HIV from the body: The role of polymeric nanomedicines in HIV/AIDS pharmacotherapy. J. Nanobiotechnol. 2014, 12, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, Y.; Wijewardhana, C.; Mann, J.F.S. Virus-like particle, liposome, and polymeric particle-based vaccines against HIV-1. Front. Immunol. 2018, 9, 345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saravanan, M.; Asmalash, T.; Gebrekidan, A.; Gebreegziabiher, D.; Araya, T.; Hilekiros, H.; Barabadi, H.; Ramanathan, K. Nano-medicine as a newly emerging approach to combat human immunodeficiency virus (HIV). Pharm. Nanotechnol. 2018, 6, 17–27. [Google Scholar] [CrossRef]
- Khandalavala, K.; Mandal, S.; Pham, R.; Destache, C.J.; Shibata, A. Nanoparticle Encapsulation for Antiretroviral Pre-Exposure Prophylaxis. J. Nanotechnol. Mater. Sci. 2017, 4, 53. [Google Scholar]
- Gnanadesigan, M.; Nandagopalan, V.; Kapildev, G.; Gundappa, M. Nano Drugs for Curing Malaria: The Plausibility. In Applications of Targeted Nano Drugs and Delivery Systems; Elsevier: Amsterdam, The Netherlands, 2019; pp. 451–467. [Google Scholar]
- Mvango, S.; Matshe, W.M.R.; Balogun, A.O.; Pilcher, L.A.; Balogun, M.O. Nanomedicines for malaria chemotherapy: Encapsulation vs. polymer therapeutics. Pharm. Res. 2018, 35, 237. [Google Scholar] [CrossRef] [Green Version]
- Alven, S.; Aderibigbe, B. Combination Therapy Strategies for the Treatment of Malaria. Molecules 2019, 24, 3601. [Google Scholar] [CrossRef] [Green Version]
- Van Giau, V.; An, S.S.A.; Hulme, J. Recent advances in the treatment of pathogenic infections using antibiotics and nano-drug delivery vehicles. Drug Des. Devel. Ther. 2019, 13, 327. [Google Scholar] [CrossRef] [Green Version]
- Ranjan, A.; Pothayee, N.; Seleem, M.N.; Boyle, S.M.; Kasimanickam, R.; Riffle, J.S.; Sriranganathan, N. Nanomedicine for intracellular therapy. FEMS Microbiol. Lett. 2012, 332, 1–9. [Google Scholar] [CrossRef]
- Armstead, A.L.; Li, B. Nanomedicine as an emerging approach against intracellular pathogens. Int. J. Nanomed. 2011, 6, 3281. [Google Scholar]
- Chifiriuc, M.C.; Holban, A.M.; Curutiu, C.; Ditu, L.-M.; Mihaescu, G.; Oprea, A.E.; Grumezescu, A.M.; Lazar, V. Antibiotic drug delivery systems for the intracellular targeting of bacterial pathogens. In Smart Drug Delivery System; IntechOpen: London, UK, 2016. [Google Scholar]
- Gao, W.; Thamphiwatana, S.; Angsantikul, P.; Zhang, L. Nanoparticle approaches against bacterial infections. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2014, 6, 532–547. [Google Scholar] [CrossRef] [PubMed]
- Algharib, S.A.; Dawood, A.; Xie, S. Nanoparticles for treatment of bovine Staphylococcus aureus mastitis. Drug Deliv. 2020, 27, 292–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fasihi Ramandi, M.; Panahi, Y. Application of nanoparticles drug delivery systems in the treatment of intracellular bacterial infections. Minerva Biotecnol. 2017, 29, 156–165. [Google Scholar]
- Bansal, A.; Zhang, Y. Photocontrolled nanoparticle delivery systems for biomedical applications. Acc. Chem. Res. 2014, 47, 3052–3060. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Lorenzo, C.; Garcia-Gonzalez, C.A.; Bucio, E.; Concheiro, A. Stimuli-responsive polymers for antimicrobial therapy: Drug targeting, contact-killing surfaces and competitive release. Expert Opin. Drug Deliv. 2016, 13, 1109–1119. [Google Scholar] [CrossRef]
- Qin, X.; Li, Y. Strategies to Design and Synthesize Polymer-Based Stimuli-Responsive Drug Delivery Nanosystems. Chem. Bio. Chem. 2019. [Google Scholar] [CrossRef]
- Geng, Y.; Dalhaimer, P.; Cai, S.; Tsai, R.; Tewari, M.; Minko, T.; Discher, D.E. Shape effects of filaments versus spherical particles in flow and drug delivery. Nat. Nanotechnol. 2007, 2, 249–255. [Google Scholar] [CrossRef]
- Shah, S.R.; Henslee, A.M.; Spicer, P.P.; Yokota, S.; Petrichenko, S.; Allahabadi, S.; Bennett, G.N.; Wong, M.E.; Kasper, F.K.; Mikos, A.G. Effects of antibiotic physicochemical properties on their release kinetics from biodegradable polymer microparticles. Pharm. Res. 2014, 31, 3379–3389. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.-P.; Pei, Y.-Y.; Zhang, X.-Y.; Gu, Z.-H.; Zhou, Z.-H.; Yuan, W.-F.; Zhou, J.-J.; Zhu, J.-H.; Gao, X.-J. PEGylated PLGA nanoparticles as protein carriers: Synthesis, preparation and biodistribution in rats. J. Control. Release 2001, 71, 203–211. [Google Scholar] [CrossRef]
- Zolnik, B.S.; Burgess, D.J. Effect of acidic pH on PLGA microsphere degradation and release. J. Control. Release 2007, 122, 338–344. [Google Scholar] [CrossRef]
- Faisant, N.; Siepmann, J.; Richard, J.; Benoit, J.P. Mathematical modeling of drug release from bioerodible microparticles: Effect of gamma-irradiation. Eur. J. Pharm. Biopharm. 2003, 56, 271–279. [Google Scholar] [CrossRef]
- Duan, X.; Li, Y. Physicochemical characteristics of nanoparticles affect circulation, biodistribution, cellular internalization, and trafficking. Small 2013, 9, 1521–1532. [Google Scholar] [CrossRef] [PubMed]
- Konduru, N.V.; Molina, R.M.; Swami, A.; Damiani, F.; Pyrgiotakis, G.; Lin, P.; Andreozzi, P.; Donaghey, T.C.; Demokritou, P.; Krol, S.; et al. Protein corona: Implications for nanoparticle interactions with pulmonary cells. Part. Fibre Toxicol. 2017, 14, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, H.; Zhang, H.; Ye, H.; Zheng, Y. Receptor-Mediated Endocytosis of Nanoparticles: Roles of Shapes, Orientations, and Rotations of Nanoparticles. J. Phys. Chem. B 2018, 122, 171–180. [Google Scholar] [CrossRef]
- Ungaro, F.; d’Angelo, I.; Coletta, C.; d’Emmanuele di Villa Bianca, R.; Sorrentino, R.; Perfetto, B.; Tufano, M.A.; Miro, A.; La Rotonda, M.I.; Quaglia, F. Dry powders based on PLGA nanoparticles for pulmonary delivery of antibiotics: Modulation of encapsulation efficiency, release rate and lung deposition pattern by hydrophilic polymers. J. Control. Release 2012, 157, 149–159. [Google Scholar] [CrossRef]
- Win, K.Y.; Feng, S.-S. Effects of particle size and surface coating on cellular uptake of polymeric nanoparticles for oral delivery of anticancer drugs. Biomaterials 2005, 26, 2713–2722. [Google Scholar] [CrossRef]
- Alhowyan, A.A.; Altamimi, M.A.; Kalam, M.A.; Khan, A.A.; Badran, M.; Binkhathlan, Z.; Alkholief, M.; Alshamsan, A. Antifungal efficacy of Itraconazole loaded PLGA-nanoparticles stabilized by vitamin-E TPGS: In vitro and ex vivo studies. J. Microbiol. Methods 2019, 161, 87–95. [Google Scholar] [CrossRef]
- Semete, B.; Booysen, L.; Lemmer, Y.; Kalombo, L.; Katata, L.; Verschoor, J.; Swai, H.S. In vivo evaluation of the biodistribution and safety of PLGA nanoparticles as drug delivery systems. Nanomed. Nanotechnol. Biol. Med. 2010, 6, 662–671. [Google Scholar] [CrossRef]
- Gordon, S.; Plüddemann, A. Tissue macrophages: Heterogeneity and functions. BMC Biol. 2017, 15, 53. [Google Scholar] [CrossRef]
- Endsley, A.N.; Ho, R.J.Y. Enhanced anti-HIV efficacy of Indinavir after inclusion in CD4 targeted lipid nanoparticles. J. Acquir. Immune Defic. Syndr. 2012, 61, 417–424. [Google Scholar] [CrossRef] [Green Version]
- Layek, B.; Lipp, L.; Singh, J. Cell penetrating peptide conjugated chitosan for enhanced delivery of nucleic acid. Int. J. Mol. Sci. 2015, 16, 28912–28930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Ibricevic, A.; Cohen, J.A.; Cohen, J.L.; Gunsten, S.P.; Fréchet, J.M.J.; Walter, M.J.; Welch, M.J.; Brody, S.L. Impact of hydrogel nanoparticle size and functionalization on in vivo behavior for lung imaging and therapeutics. Mol. Pharm. 2009, 6, 1891–1902. [Google Scholar] [CrossRef] [PubMed]
- Tonigold, M.; Simon, J.; Estupiñán, D.; Kokkinopoulou, M.; Reinholz, J.; Kintzel, U.; Kaltbeitzel, A.; Renz, P.; Domogalla, M.P.; Steinbrink, K.; et al. Pre-adsorption of antibodies enables targeting of nanocarriers despite a biomolecular corona. Nat. Nanotechnol. 2018, 13, 862–869. [Google Scholar] [CrossRef] [PubMed]
- Tirtaatmadja, N.; Mortimer, G.; Ng, E.-P.; Ahmad, H.; Mintova, S.; Serpooshan, V.; Minchin, R.; Mahmoudi, M. Nanoparticles-induced inflammatory cytokines in human plasma concentration manner: An ignored factor at the nanobio-interface. J. Iran. Chem. Soc. 2015, 12. [Google Scholar] [CrossRef]
- Madaan, K.; Kumar, S.; Poonia, N.; Lather, V.; Pandita, D. Dendrimers in drug delivery and targeting: Drug-dendrimer interactions and toxicity issues. J. Pharm. Bioallied Sci. 2014, 6, 139–150. [Google Scholar] [CrossRef]
- Palmerston Mendes, L.; Pan, J.; Torchilin, V.P. Dendrimers as Nanocarriers for Nucleic Acid and Drug Delivery in Cancer Therapy. Molecules 2017, 22, 1401. [Google Scholar] [CrossRef] [Green Version]
- Kolhatkar, R.B.; Kitchens, K.M.; Swaan, P.W.; Ghandehari, H. Surface acetylation of polyamidoamine (PAMAM) dendrimers decreases cytotoxicity while maintaining membrane permeability. Bioconjug Chem. 2007, 18, 2054–2060. [Google Scholar] [CrossRef]
- Fuchs, A.-K.; Syrovets, T.; Haas, K.A.; Loos, C.; Musyanovych, A.; Mailänder, V.; Landfester, K.; Simmet, T. Carboxyl- and amino-functionalized polystyrene nanoparticles differentially affect the polarization profile of M1 and M2 macrophage subsets. Biomaterials 2016, 85, 78–87. [Google Scholar] [CrossRef]
- Lunov, O.; Syrovets, T.; Loos, C.; Nienhaus, G.U.; Mailänder, V.; Landfester, K.; Rouis, M.; Simmet, T. Amino-functionalized polystyrene nanoparticles activate the NLRP3 inflammasome in human macrophages. ACS Nano 2011, 5, 9648–9657. [Google Scholar] [CrossRef]
- Jones, M.-C.; Jones, S.A.; Riffo-Vasquez, Y.; Spina, D.; Hoffman, E.; Morgan, A.; Patel, A.; Page, C.; Forbes, B.; Dailey, L.A. Quantitative assessment of nanoparticle surface hydrophobicity and its influence on pulmonary biocompatibility. J. Control. Release 2014, 183, 94–104. [Google Scholar] [CrossRef]
- Yetisgin, A.A.; Cetinel, S.; Zuvin, M.; Kosar, A.; Kutlu, O. Therapeutic Nanoparticles and Their Targeted Delivery Applications. Molecules 2020, 25, 2193. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.L.; Peres, C.; Conniot, J.; Matos, A.I.; Moura, L.; Carreira, B.; Sainz, V.; Scomparin, A.; Satchi-Fainaro, R.; Préat, V.; et al. Nanoparticle impact on innate immune cell pattern-recognition receptors and inflammasomes activation. Semin. Immunol. 2017, 34, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Neun, B.W.; Barenholz, Y.; Szebeni, J.; Dobrovolskaia, M.A. Understanding the Role of Anti-PEG Antibodies in the Complement Activation by Doxil in Vitro. Molecules 2018, 23, 1700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, P.; Sun, F.; Liu, S.; Jiang, S. Anti-PEG antibodies in the clinic: Current issues and beyond PEGylation. J. Control. Release 2016, 244, 184–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abu Lila, A.S.; Shimizu, T.; Ishida, T. 3-PEGylation and anti-PEG antibodies. In Woodhead Publishing Series in Biomaterials; Parambath, A.B.T., Ed.; Woodhead Publishing: Cambridge, UK, 2018; pp. 51–68. ISBN 978-0-08-101750-0. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Classification | Example | Target | Action Mechanism | Secondary Effects | Ref. |
|---|---|---|---|---|---|
| Antibiotics | β-Lactams | Bacterial cell wall | Inhibiting bacterial cell wall synthesis. | Allergy, diarrhea/colitis, pruritic rash, abnormal coagulation, abnormal liver function. Drug-drug interaction with bacteriostatic antibiotics displaying an antagonized effect. | [136] |
| Polymixins | Bacterial cell wall | Positively charged polymyxins bind to molecules of the bacterial cell wall with negative charges, affecting the osmotic balance. | Nephotoxicity, paresthesias, apnea, nausea, vomiting, dizziness, myopathy and neuropathy. | [132,137] | |
| Quinolones and Fluoroquinolones | Enzymes | Inhibits DNA gyrase and topoisomerases enzymes. | Nausea, vomiting, dyspepsia, heartburn, abdominal pain, inflammation in tendons, musculus and joints, depression, affects memory and sleeping. | [136,138] | |
| Sulphonamides and trimetroprim | Metabolic pathways | Interferes with folic acid synthesis by preventing the addition of para-aminobenzoic acid (PABA) into the folic acid molecule. | Rashes, erythema modosum, dermatitis, photosensitivity, acute hemolytic anemia, agranulocytosis, aplastic anemia, liver injury, hepatic granuloma. Drug-drug interaction with bone marrow depressants increases the leukopenic and/or thrombocytopenic effects. | [132,136] | |
| Antivirals | Acyclovir | DNA polymerases | Chain terminator. | Pain, swelling, abdominal or stomach pain, loss appetite, nausea or vomiting and reversible nephrotoxicity. | [139] |
| Enfuvirtide | Blocks virus entry to the host cell | Inhibits glycoproteins that mediate the membrane fusion of virus. | Rash, fever, nausea, vomiting, chills, rigors, hypotension and elevation of serum liver transaminase level. | [140,141] | |
| Oseltamivir | Blocks release virions from infected cells | Inhibits glycoproteins that mediate the release of virion. | Nausea, vomiting, bronchitis, insomnia, vertigo, abdominal pain, epistaxis, optic disorder and conjunctivitis. | [142,143,144] | |
| Interferons (IFN) | Immune response | Inhibits virus replication, suppression of cell proliferation, enhancement of macrophages’ phagocytic activity. | Fever, fatigue, bone marrow suppression, influenza-like symptoms, depression, development of autoimmune illnesses, cardiovascular disorders, thyroid disorders, dyspnea and pneumonitis. | [139,145,146] | |
| Efavirenz | Inhibition of reverse transcriptase | Binds to a region that is distinct from the dNTP-binding site on the viral RT protein. | Abnormal dreams, abnormal thinking, agitation, amnesia, confusion, depersonalization, dizziness, euphoria, hallucinations, insomnia, somnolence and serum aminotransferase elevation. | [147,148] | |
| Antifungals | Amphotericin B | Fungi cell wall | Binds to ergosterol in the fungal cell membrane, disrupting cell permeability. | Nausea, fever, pulmonary toxicity, abdominal pain or leg pain, nephrotoxicity, hemolysis and liver damage. | [36,149] |
| Azole agents | Fungi cell wall | Inhibits cytochrome P-450 dependent enzymes needed to synthesize ergosterol of the fungal cell membrane. | Nausea, diarrhea, hypertension, hypokalemia, edema, liver injury and hepatotoxicity; drug-drug interaction, inhibits the cytochrome P450 (CPY450) enzymes in the liver and interacts with P-glycoproteins (P-gp) in the cell membrane involved in the absorption and distribution of drugs, affecting the therapeutic response and the interaction with other drugs. | [39,150,151] | |
| Echinocandins | Fungi cell wall | Inhibits the production of (1r3)-β-d-glucan, an essential component in the fungal cell wall. | Fever, nausea, vomiting, headache, pain, rash, anemia, abdominal pain, serum aminotransferase elevation. | [150,152,153] | |
| Antiparasitics | Chloroquine | Inhibition of metabolic pathways | Inhibits the parasitic heme detoxification and nucleic acid biosynthesis. | Apnea, nausea, vomiting, cramps, diarrhea, hepatotoxicity, cardiotoxicity. | [154,155,156] |
| Pentavalent antimonial | Parasitic cell wall | Inhibits glycolysis and b-oxidation of fatty acids of parasite. | Pancreatitis, pancytopenia, reversible peripheral neuropathy, elevation in serum aminotransferases, pain, stiff joints, gastrointestinal problems, hepatic-, renal-insufficiency (nephrotoxicity), cardiotoxicity, accumulation inside the tissues of liver and spleen. | [157] | |
| Pentamidine | Interferes with nuclear metabolism | Inhibits synthesis of DNA, RNA, phospholipids, and proteins. | Skin rash, nausea and vomiting, anxiety, headache, hypoglycemia, hypertension, myalgia, and headache. | [130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157] |
| Antimicrobial (Disease) | First-Line of Treatment | Second-Line of Treatment | Resistance Cause or Mechanism | Resistance Characteristic and Consequence | Ref. |
|---|---|---|---|---|---|
| Antibiotic (Tuberculosis) | Rifampin, Isoniazid, Pyrazinamide and Ethambutol | Fluoroquinolons, aminoglycosides, para-aminosalicylic acid, and cycloserine | Poor solubility, low plasma levels, low permeability and are rapidly metabolized by the liver, thus requiring multiple and high doses. | Multi-resistant strains appear by interruption of the treatment schedule; therapy becomes more toxic and less effective, drugs are more expensive and scarcer. Neurotoxicity and hepatotoxicity. | [30,37,158,159] |
| Antiviral (VIH) | Disoproxil fumarate, Lamivudine or Emtricitabin, Efavirenz | A boosted protease inhibitor (bPI) plus two nucleoside analogues (NRTIs) | Poor treatment compliance, variable drug pharmacokinetics, pharmacokinetic interactions and pharmacodynamics, thereof, low penetration into certain body compartments, leads to subtherapeutic levels and, therefore, to the selection of resistant viruses. | Treatment failure and further spread of drug-resistant HIV. It can compromise the effectiveness of the limited therapeutic options and further reduce HIV incidence, mortality and morbidity. | [141,142,160] |
| Antifungal | Fluconazole | Itraconazole | Drugs have poor solubility, low plasma levels, low permeability. The use of inadequate dosages, when treatment courses are not long enough. The use of fungicides in agriculture contributes to resistance. | Therapy becomes more toxic and less effective. Hepatotoxicity. | [150,152,161] |
| Antiparasitic (Leishmaniasis) | Pentavalent antimony | Pentamidine | Exposure of low concentration of arsenic leads to the emergence of parasite resistance. | Adjusting doses, frequencies and administration time to maintain its efficacy but with an increase in the severity of the side effects. | [120,157] |
| Function | Formulation | Drug/Active Principle | Targeted Microorganism or Cells | Method of Fabrication | Outcome | Ref. |
|---|---|---|---|---|---|---|
| Conventional PNs | ||||||
| Antibacterial | PLGA | Gentamicin | Klebsiella pneumoniae | Water-oil-water (w/o/w) double emulsion method | Reducing bacterial viability without concomitant stimulation of inflammatory or pyroptotic pathways in the treated cells. | [205] |
| N-trimethyl chitosan | Recombinant urease | Brucella melitensis, Brucella abortus | Ionic complexation | Intraperitoneal vaccination with TMC/urease nanoparticles provides more protection and immune response against brucellosis as compared to TMC/urease NPs’ oral administration. | [206] | |
| β-cyclodextrin | Ethionamide and BDM43266 | - | Cross-linking | Co-encapsulation of ethionamide and BDM43266 antitubercular drugs was achieved into β-CyD PNs with the possibility of pulmonary administration. | [207] | |
| Antiprotozoal | TPGS, Tetronics T904 and T1107 | Miltefosine | Leishmania major | Self-assembly | Nanoencapsulation of miltefosine in polymeric micelles of TPGS, T904 and T1107 enhanced antileishmanial activity as compared to miltefosine solutions. T904 formulation increased activity against intracellular amastigotes of L. major. | [208] |
| Antiretroviral | m-PEG-PLL | Efavirenz and Elvitegravir | TZM-bl cell line infected with HIV | Self-assembly | Enhancing of combined therapy against HIV infection was achieved by encapsulation of antiretrovirals into hydrophobic core graft-copolymer nanoparticles made of m-PEG-PLL with a hydrophobic core of fatty acids with low cytotoxicity and improved biodistribution. | [209] |
| Novel approaches on PNs | ||||||
| Macrophage targeting | PCL-PEG/MRTL (Bivalent mannose receptor targeting ligand) | - | Rat peritoneal macrophages | Flash nanoprecipitation | Macrophages of M2-type can be targeted using PNs coupled with a new bivalent mannose targeting ligand via mannose receptor, enhancing specificity and cellular uptake of PNs. | [210] |
| Antifungal | PLGA/DMSA | Itraconazole | Paracoccidioides brasiliensis | Emulsification-evaporation method | Nanoencapsulation of ITZ in functionalized PLGA/DMSA nanoparticles improved biodistribution and antifungal efficacy against Paracoccidioides brasiliensis evaluated in vivo in infected BALB/c mice as compared to free ITZ, lowering the number of administrations and side effects. | [39] |
| Antiprotozoal | PLGA/Mannose | Itraconazole | Leishmania (L) infantum | Nanoprecipitation | PLGA NPs with mannose receptor increased efficacy against Leishmania (L.) infantum amastigotes. | [10] |
| Grafted Chitosan/tri-mannose ligand | - | Human macrophages with M. tuberculosis | Nanoemulsion and Ionic gelation | CS nanocapsules grafted with tri-mannose ligands modulated cell metabolism of cells infected with M. tuberculosis, offering the possibility to reprogram immune cells improving drug therapy. | [79] | |
| PEG-PPS functionalized with acid-sensitive fluorophores (ASF) | Antigen mycolic acid | M. tuberculosis | Self-assembly | Pulmonary delivery of mycolic acid-lipid antigen encapsulated in polymeric micelles enhanced immune response of T cells in mice model hCD1Tg (humanized CD1 transgenic mice) improving immunization therapy against M. tuberculosis. | [211] | |
| N-trimethyl chitosan/poly(trimethylene carbonate) composite | Vancomycin | S. aureus | Ionotropic gelation | VCM/TMC NP-PTMC inhibits bacteria and promotes bone repair in vivo. | [212] | |
| Antibacterial | PLGA/PLGA-PEG/Zwitterionicchitosan/Eudragit E100 | Vancomycin | Methicillin-resistant S. aureus | Water-oil-water (w1/o/w2) double emulsion method | Better antimicrobial activity than free vancomycin against intracellular MRSA and other intracellular pathogens. | [213] |
| PLGA/membrane of extracellular vesicle | Vancomycin and rifampicin | S. aureus | membrane-coating technique | Membrane-coating had an active targeting capacity and the formulation improved efficacy to treat S. aureus. | [194] | |
| PVA/NaAlg | Amoxicillin | S. aureus | Coacervation | Antimicrobial activity is comparable to pure Amoxicillin. pH-controlled release of Amoxicillin. | [214] | |
| Glycol chitosan-LPNs (PLGA/DDA/TDB) | Antigen CTH522 | C. trachomatis | Single emulsion evaporation method O/W | Glycol CS-lipid polymer hybrid nanoparticles (LPNs) made of PLGA/DDA/TDB used as adjuvant of antigen CTH522 against C. trachomatis in mice model via nasal administration induced IgG/IgA responses increased in lungs and genital tract as compared to adjuvant DDA/TDB liposomal. | [193] | |
| PCL/SBA-15 | Thymol | S. aureus | Electrospinning | Antimicrobial activity is better than free thymol against S. aureus using rod-shaped particles. | [215] | |
| PCL/MCM-41 surface functionalized | Gentamicin | - | Electrospinning | Controlled release of Gentamicin and biocompatible material. | [195] | |
| Patent Name | Polymers | Therapeutic Use | Patent Number |
|---|---|---|---|
| Antiviral prodrugs and nanoformulations thereof | The prodrug, amphiphilic block copolymers, P407 | Retroviral, viral, HIV infections | WO2020086555A1 |
| Nanoparticle encapsulation to target G protein-coupled receptors in endosomes | DIPMA-DEGMA-b-PEGMA-DMAEMA; BMA-b-PEGMA-DMAEMA | Delivery of therapeutic principles | WO2020084471A1 |
| Functionalized nanoparticle formulations for oral drug delivery | Different types including polyalkenes, polyesters, functionalized with FcRn binding partner | Various uses including encapsulation of antibacterial and anticancer agents | WO2020086871A1 |
| Polymeric nanoparticles in a thermosensitive gel for coital-independent vaginal prophylaxis of HIV | PLGA, PCL, Pluronic F127, Pluronic F68 | Prevention of HIV infection | US2015/O190398A1 |
| Organosilanes for the treatment of infections | Organosilicon quaternary ammonium compounds | Bacterial, fungal, viral infections | WO2020082026A1 |
| Novel nanoparticles of antiretroviral drugs, their preparation and their use for the treatment of viral infections | Chitosan | HIV, viral infections | EP3653201A1 |
| Methods and composition for treating microbial infections | PLGA, PCL, mPEG-PLGA, PVA, PEO, PVP and combinations thereof | HIV, viral infections | WO2020097062A1 |
| Synthetic innate immune receptor ligands and uses thereof | PLGA | Vaccine therapy | WO2020082162A1 |
| Polymer-particle light-cleavable carrier systems for photodynamic therapy | Polycarbonates, polyesters, various types | Infection diseases | WO2020064701A1 |
| Small polymeric carriers for delivery of agents | Hydrophobic polymeric backbone with a plurality of pendant groups | Antiviral infections and delivery of active agents | WO2020077170A1 |
| Antimicrobial compositions and methods | Various type of block copolymers including polyethylene oxide-polyglutamic acid-phenylalanine | Antimicrobial therapy | WO2020056114A1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez, A.; Mejía, S.P.; Orozco, J. Recent Advances in Polymeric Nanoparticle-Encapsulated Drugs against Intracellular Infections. Molecules 2020, 25, 3760. https://doi.org/10.3390/molecules25163760
Sánchez A, Mejía SP, Orozco J. Recent Advances in Polymeric Nanoparticle-Encapsulated Drugs against Intracellular Infections. Molecules. 2020; 25(16):3760. https://doi.org/10.3390/molecules25163760
Chicago/Turabian StyleSánchez, Arturo, Susana P. Mejía, and Jahir Orozco. 2020. "Recent Advances in Polymeric Nanoparticle-Encapsulated Drugs against Intracellular Infections" Molecules 25, no. 16: 3760. https://doi.org/10.3390/molecules25163760