When Vessels and Sarcomas Combine: A Review of the Inferior Vena Cava Leiomyosarcoma

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Epidemiology
3. Clinical Presentation
4. Etiology and Pathogenesis
5. Imaging Diagnosis
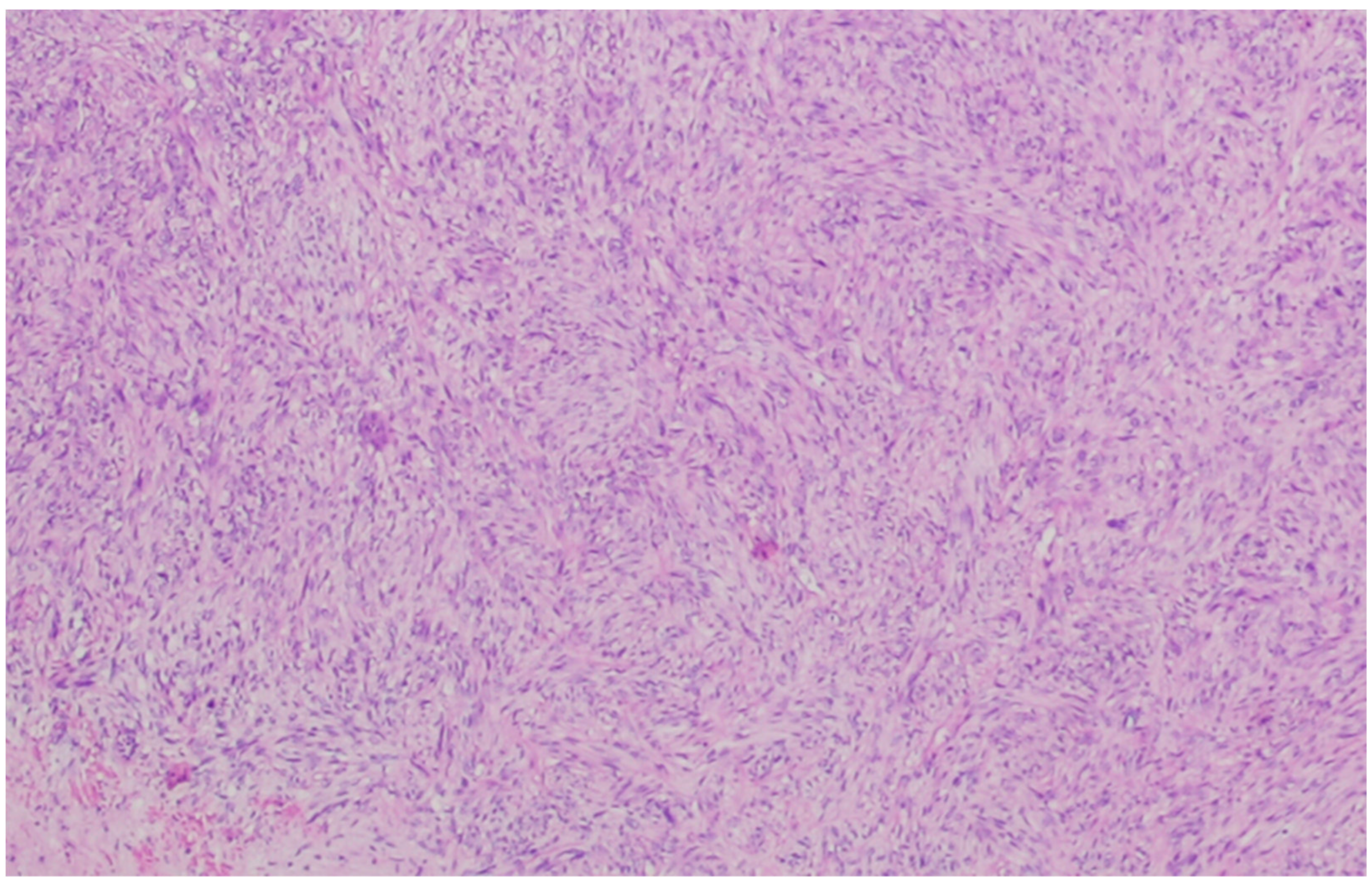
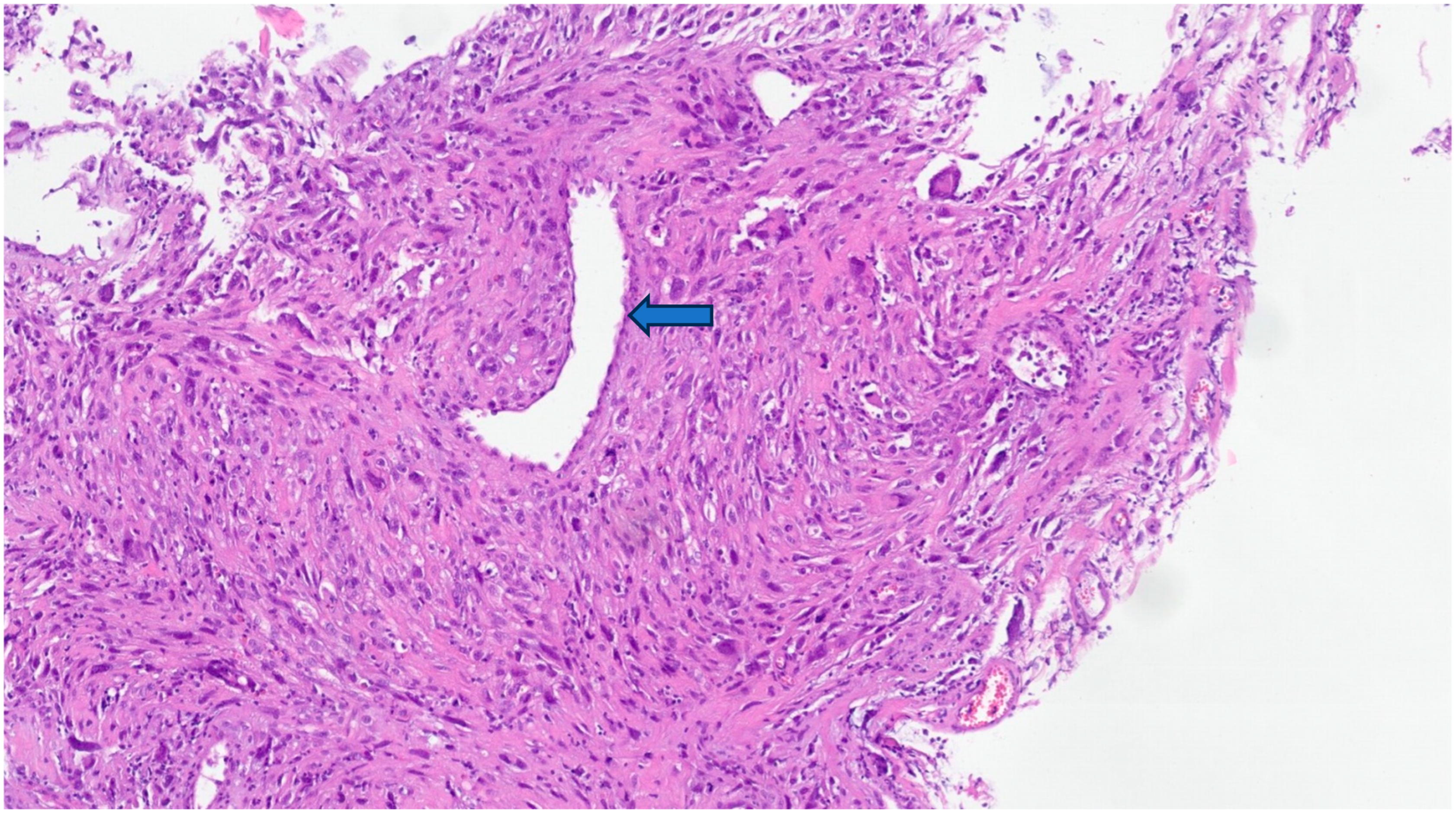
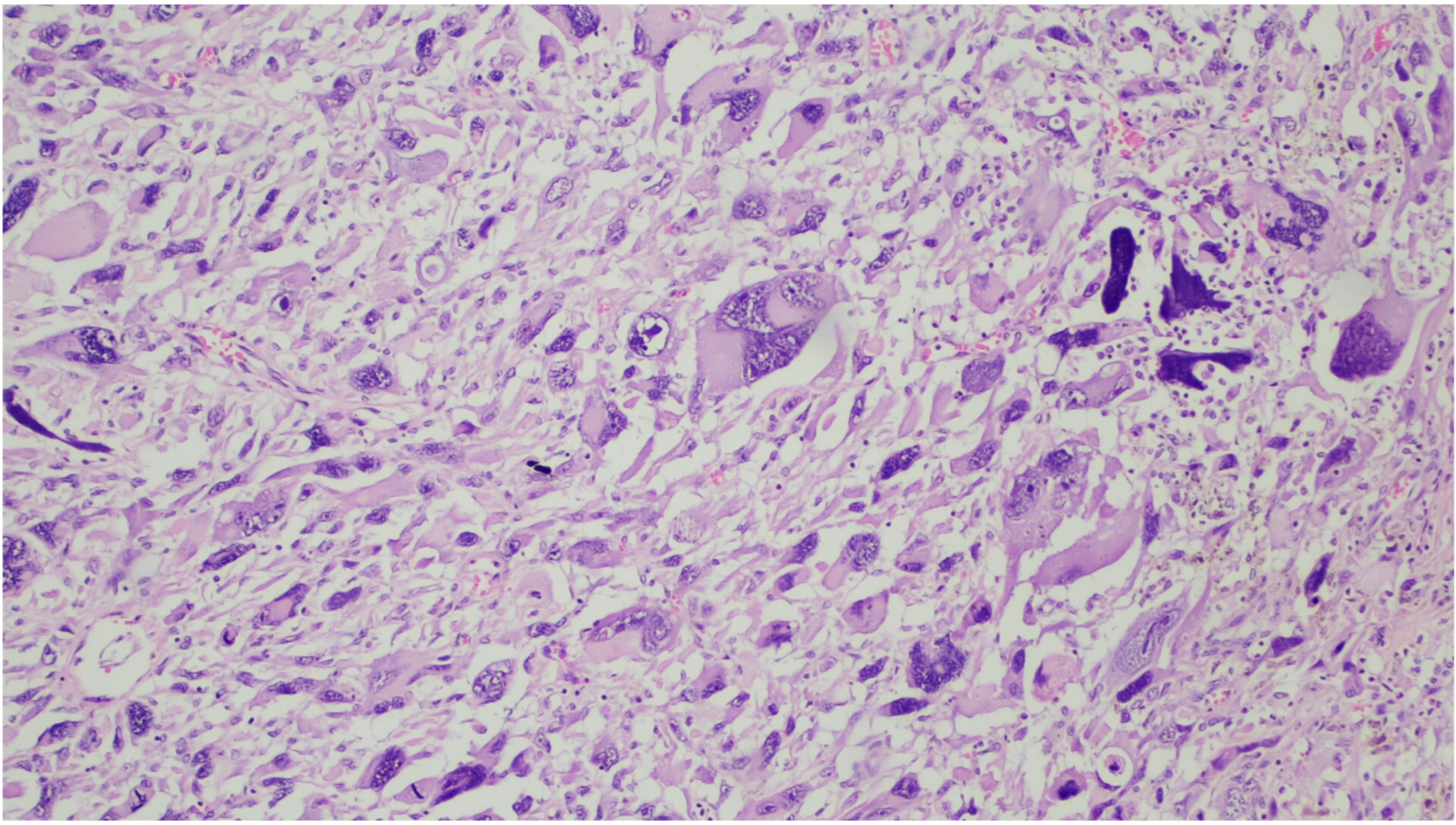
6. Gross and Histologic Features
7. Staging
8. Prognosis
9. Treatment
10. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- IARC. WHO Classification of Soft Tissue and Bone Tumours. WHO Classification of Tumours Soft Tissue and Bone Tumours. 2020. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8167394/ (accessed on 6 August 2023).
- Fletcher, C.D.M. Diagnostic Histopathology of Tumors, 5th ed.; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Roland, C.L.; Boland, G.M.; Demicco, E.G.; Lusby, K.; Ingram, D.; May, C.D.; Kivlin, C.M.; Watson, K.; Sanaa, G.A.A.; Wang, W.L.; et al. Clinical Observations and Molecular Variables of Primary Vascular Leiomyosarcoma. JAMA Surg. 2016, 151, 347–354. Available online: https://pubmed.ncbi.nlm.nih.gov/26629783/ (accessed on 31 July 2023). [CrossRef] [PubMed]
- Perl, L.; Virchow, R. Ein Fall von Sarkom der Vena cava inferior. Arch Pathol. Anat. Physiol. Klin. Med. 1871, 53, 378–383. Available online: https://link.springer.com/article/10.1007/BF01957198 (accessed on 29 July 2023). [CrossRef]
- Mastrangelo, G.; Coindre, J.M.; Ducimetière, F.; Dei Tos, A.P.; Fadda, E.; Blay, J.Y.; Buja, A.; Fedeli, U.; Cegolon, L.; Frasson, A.; et al. Incidence of soft tissue sarcoma and beyond. Cancer 2012, 118, 5339–5348. Available online: https://onlinelibrary.wiley.com/doi/full/10.1002/cncr.27555 (accessed on 31 July 2023). [CrossRef] [PubMed]
- Müller, A.M.; Chromik, A.M.; Bolik, B.; Müller, K.M.; Mittelkötter, U. Leiomyosarkom der vena cava inferior: Übersicht zu einem seltenen krankheitsbild. Pathologe 2005, 26, 153–158. Available online: https://link.springer.com/article/10.1007/s00292-004-0745-y (accessed on 29 July 2023). [CrossRef] [PubMed]
- Goldblum, J.R.; Weiss, S.W.; Folpe, A.L. Enzinger and Weiss’s Soft Tissue Tumors, 7th ed.; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Leiomyosarcoma of the Inferior Vena Cava—Hines—1999—Cancer—Wiley Online Library. Available online: https://acsjournals.onlinelibrary.wiley.com/doi/pdf/10.1002/%28SICI%291097-0142%2819990301%2985%3A5%3C1077%3A%3AAID-CNCR10%3E3.0.CO%3B2-0 (accessed on 29 July 2023).
- International Registry of Inferior Vena Cava Leiomyosarcoma: Analysis of a World Series on 218 Patients—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/8920790/ (accessed on 30 July 2023).
- Yoshizawa, K.; Ohno, Y.; Kurata, T.; Takagi, Y.; Kasai, T.; Takizawa, M.; Soyejima, Y. Primary leiomyosarcoma of the inferior vena cava in a pediatric case: A case report and literature review. Surg. Case Rep. 2023, 9, 52. Available online: https://pmc/articles/PMC10079787/ (accessed on 6 April 2023). [CrossRef] [PubMed]
- Kevorkian, J.; Cento, D.P. Leiomyosarcoma of large arteries and veins. Surgery 1973, 73, 390–400. Available online: http://www.surgjournal.com/article/0039606073903073/fulltext (accessed on 27 July 2023). [PubMed]
- Italiano, A.; Toulmonde, M.; Stoeckle, E.; Kind, M.; Kantor, G.; Coindre, J.M.; Bui, B. Clinical outcome of leiomyosarcomas of vascular origin: Comparison with leiomyosarcomas of other origin. Ann. Oncol. 2010, 21, 1915–1921. Available online: http://www.annalsofoncology.org/article/S0923753419400628/fulltext (accessed on 2 August 2023). [CrossRef]
- Weinreb, W.; Steinfeld, A.; Rodil, J.; Esparza, A.; Trebbin, W. Leiomyosarcoma Arising in an Arteriovenous Fistula. Available online: https://pubmed.ncbi.nlm.nih.gov/6861080/ (accessed on 30 July 2023).
- Hashimoto, H.; Daimaru, Y.; Tsuneyoshi, M.; Enjoji, M. Leiomyosarcoma of the External Soft Tissues A Clinicopathologic, lmmunohistochemical, and Electron Microscopic Study Materials and Methods. Available online: https://onlinelibrary.wiley.com/terms-and-conditions (accessed on 29 July 2023).
- Farshid, G.; Pradhan, M.; Goldblum, J.; Weiss, S.W. Leiomyosarcoma of somatic soft tissues: A tumor of vascular origin with multivariate analysis of outcome in 42 cases. Am. J. Surg. Pathol. 2002, 26, 14–24. Available online: https://pubmed.ncbi.nlm.nih.gov/11756765/ (accessed on 29 July 2023). [CrossRef] [PubMed]
- Gustafson, P.; Willkn, H.; Baldetorp, B.; Ferno, M.; Akerman, M.; Rydholm, A. Soft Tissue Leiomyosarcoma A Population-Based Epidemiologic and Prognostic Study of 48 Patients, Including Cellular DNA Content. Cancer 1992, 70, 114–119. [Google Scholar] [CrossRef]
- Enzinger, F.M.; Shiraki, M. Extraskeletal myxoid chondrosarcoma. An analysis of 34 cases. Hum. Pathol. 1972, 3, 421–435. [Google Scholar] [CrossRef] [PubMed]
- Mingoli, A.; Feldhaus, R.J.; Cavallaro, A.; Stipa, S. Leiomyosarcoma of the inferior vena cava: Analysis and search of world literature on 141 patients and report of three new cases. J. Vasc. Surg. 1991, 14, 688–699. [Google Scholar] [CrossRef] [PubMed]
- Gomes, J.F.; Vieira, I.; Mendes, J.; Donaire, D.; Almeida, R. Leiomyosarcoma of Inferior Vena Cava in an Immunocompetent Young-adult Female Patient. J. Coll. Physicians Surg. Pak. 2022, 32, 1353–1355. Available online: https://pubmed.ncbi.nlm.nih.gov/36205287/ (accessed on 23 September 2023). [PubMed]
- Nilbert, M.; Mandahl, N.; Heim, S.; Rydholm, A.; Helm, G.; Willén, H.; Baldetorp, B.; Mitelman, F. Complex karyotypic changes, including rearrangements of 12q13 and 14q24, in two leiomyosarcomas. Cancer Genet. Cytogenet. 1990, 48, 217–223. Available online: https://pubmed.ncbi.nlm.nih.gov/2397453/ (accessed on 31 July 2023). [CrossRef] [PubMed]
- Chudasama, P.; Mughal, S.S.; Sanders, M.A.; Hübschmann, D.; Chung, I.; Deeg, K.I.; Wong, S.H.; Rabe, S.; Hlenvjak, M.; Zapatka, M.; et al. Integrative genomic and transcriptomic analysis of leiomyosarcoma. Nat. Commun. 2018, 9, 1–15. Available online: https://www.nature.com/articles/s41467-017-02602-0 (accessed on 31 July 2023). [CrossRef] [PubMed]
- Gladdy, R.A.; Qin, L.X.; Moraco, N.; Agaram, N.P.; Brennan, M.F.; Singer, S. Predictors of Survival and Recurrence in Primary Leiomyosarcoma. Ann. Surg. Oncol. 2013, 20, 1851. Available online: https://pmc/articles/PMC3657306/ (accessed on 28 August 2023). [CrossRef] [PubMed]
- Rusu, C.B.; Gorbatâi, L.; Szatmari, L.; Koren, R.; Bungărdean, C.I.; Feciche, B.O.; Bumbulut, C.; Andras, I.M.; Rahota, R.; Telecan, T.; et al. Leiomyosarcoma of the inferior vena cava. Our experience and a review of the literature. Rom J. Morphol. Embryol. 2020, 61, 227. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7728114/ (accessed on 23 September 2023). [CrossRef] [PubMed]
- Wu, X.; Zhou, P.; Li, K. Contrast-enhanced ultrasonography of intraluminal inferior vena cava leiomyosarcoma: A case report. J. Clin. Ultrasound. 2020, 48, 357–361. Available online: https://pubmed.ncbi.nlm.nih.gov/32027023/ (accessed on 23 September 2023). [CrossRef] [PubMed]
- Webb, E.M.; Wang, Z.J.; Westphalen, A.C.; Nakakura, E.K.; Coakley, F.V.; Yeh, B.M. Can CT features differentiate between inferior vena cava leiomyosarcomas and primary retroperitoneal masses? Am. J. Roentgenol. 2013, 200, 205–209. Available online: https://www.ajronline.org/doi/10.2214/AJR.11.7476 (accessed on 23 September 2023). [CrossRef]
- Mastoraki, A.; Leotsakos, G.; Mastoraki, S.; Papanikolaou, I.S.; Danias, N.; Smyrniotis, V.; Arkadapoulos, N. Challenging diagnostic and therapeutic modalities for leiomyosarcoma of inferior vena cava. Int. J. Surg. 2015, 13, 92–95. Available online: https://pubmed.ncbi.nlm.nih.gov/25489949/ (accessed on 23 September 2023). [CrossRef]
- Sessa, B.; Iannicelli, E.; Caterino, S.; D’Angelo, F.; Milione, M.; Ziparo, V.; David, V. Imaging of leiomyosarcoma of the inferior vena cava: Comparison of 2 cases and review of the literature. Cancer Imaging 2010, 10, 80. Available online: https://pmc/articles/PMC2842181/ (accessed on 23 September 2023). [CrossRef]
- Ronchi, B.; Peña, G.A.; Sacchi, C. PET/MR: Primary inferior vena cava leiomyosarcoma. Eur. J. Hybrid Imaging 2022, 6, 1–8. Available online: https://ejhi.springeropen.com/articles/10.1186/s41824-022-00144-3 (accessed on 23 September 2023). [CrossRef] [PubMed]
- Kim, J.T.; Kwon, T.; Cho, Y.; Shin, S.; Lee, S.; Moon, D. Multidisciplinary treatment and long-term outcomes in six patients with leiomyosarcoma of the inferior vena cava. J. Korean Surg. Soc. 2012, 82, 101–109. Available online: https://pubmed.ncbi.nlm.nih.gov/22347712/ (accessed on 23 September 2023). [CrossRef] [PubMed]
- Punt, S.E.W.; Eary, J.F.; O’Sullivan, J.; Conrad, E.U. Fluorodeoxyglucose positron emission tomography in leiomyosarcoma: Imaging characteristics. Nucl. Med. Commun. 2009, 30, 546–549. Available online: https://pubmed.ncbi.nlm.nih.gov/19440162/ (accessed on 23 September 2023). [CrossRef] [PubMed]
- Gronchi, A.; Miah, A.B.; Dei Tos, A.P.; Abecassis, N.; Bajpai, J.; Bauer, S.; Biagini, R.; Bielak, S.; Blay, J.Y.; Bolle, S.; et al. Soft tissue and visceral sarcomas: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up☆. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, 32, 1348–1365. Available online: https://pubmed.ncbi.nlm.nih.gov/34303806/ (accessed on 23 September 2023). [CrossRef] [PubMed]
- Tsukada, T.; McNutt, M.A.; Ross, R.; Gown, A.M. HHF35, a muscle actin-specific monoclonal antibody. II. Reactivity in normal, reactive, and neoplastic human tissues. Am. J. Pathol. 1987, 127, 389. Available online: https://pmc/articles/PMC1899748/?report=abstract (accessed on 29 July 2023). [PubMed]
- Carvalho, J.C.; Thomas, D.G.; Lucas, D.R. Cluster analysis of immunohistochemical markers in leiomyosarcoma delineates specific anatomic and gender subgroups. Cancer 2009, 115, 4186–4195. Available online: https://pubmed.ncbi.nlm.nih.gov/19626649/ (accessed on 2 August 2023). [CrossRef] [PubMed]
- Azumi, N.; Ben-Ezra, J.; Battifora, H. Immunophenotypic diagnosis of leiomyosarcomas and rhabdomyosarcomas with monoclonal antibodies to muscle-specific actin and desmin in formalin-fixed tissue. Mod. Pathol. 1988, 1, 469–474. [Google Scholar] [PubMed]
- Pollock, L.; Rampling, D.; Greenwald, S.E.; Malone, M. Desmin expression in rhabdomyosarcoma: Influence of the desmin clone and immunohistochemical method. J. Clin. Pathol. 1995, 48, 535–538. Available online: https://jcp.bmj.com/content/48/6/535 (accessed on 29 July 2023). [CrossRef]
- Truong, L.D.; Rangdaeng, S.; Cagle, P.; Ro, J.Y.; Hawkins, H.; Font, R.L. The diagnostic utility of desmin. A study of 584 cases and review of the literature. Am. J. Clin. Pathol. 1990, 93, 305–314. Available online: https://pubmed.ncbi.nlm.nih.gov/1689936/ (accessed on 29 July 2023). [CrossRef]
- Dabbs, D.J. Diagnostic Immunohistochemistry, 6th ed.; Elsevier: Amsterdam, The Netherlands, 2022. [Google Scholar]
- Matsuyama, A.; Hisaoka, M.; Hashimoto, H. Vascular leiomyosarcoma: Clinicopathology and immunohistochemistry with special reference to a unique smooth muscle phenotype. Pathol. Int. 2010, 60, 212–216. Available online: https://pubmed.ncbi.nlm.nih.gov/20403047/ (accessed on 29 July 2023). [CrossRef]
- Iwata, J.; Fletcher, C.D.M. Immunohistochemical detection of cytokeratin and epithelial membrane antigen in leiomyosarcoma: A systematic study of 100 cases. Pathol. Int. 2000, 50, 7–14. Available online: https://onlinelibrary.wiley.com/doi/full/10.1046/j.1440-1827.2000.01001.x (accessed on 29 July 2023). [CrossRef] [PubMed]
- Traweek, S.T.; Liu, J.; Battifora, H. Keratin gene expression in non-epithelial tissues. Detection with polymerase chain reaction. Am. J. Pathol. 1993, 142, 1111. Available online: https://pmc/articles/PMC1886881/?report=abstract (accessed on 28 October 2023). [PubMed]
- Gown, A.M.; Boyd, H.C.; Chang, Y.; Ferguson, M.; Reichler, B.; Tippens, D. Smooth muscle cells can express cytokeratins of “simple” epithelium. Immunocytochemical and biochemical studies in vitro and in vivo. Am. J. Pathol. 1988, 132, 223. Available online: https://pmc/articles/PMC1880728/?report=abstract (accessed on 28 October 2023). [PubMed]
- Immunoreactivity for Cytokeratin and Epithelial Membrane Antigen in Leiomyosarcoma—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/2454091/ (accessed on 29 July 2023).
- Fisher, C. Immunohistochemistry in diagnosis of soft tissue tumours. Histopathology 2011, 58, 1001–1012. Available online: https://pubmed.ncbi.nlm.nih.gov/21143519/ (accessed on 30 July 2023). [CrossRef] [PubMed]
- Kanamori, T.; Takakura, K.; Mandai, M.; Kariya, M.; Fukuhara, K.; Sakaguchi, M.; Huh, N.H.; Saito, K.; Sakurai, T.; Fujita, J.; et al. Increased expression of calcium-binding protein S100 in human uterine smooth muscle tumours. Mol. Hum. Reprod. 2004, 10, 735–742. Available online: https://pubmed.ncbi.nlm.nih.gov/15322223/ (accessed on 30 July 2023). [CrossRef] [PubMed]
- Silva, E.G.; Bodurka, D.C.; Scouros, M.A.; Ayala, A. A uterine leiomyosarcoma that became positive for HMB45 in the metastasis. Ann. Diagn. Pathol. 2005, 9, 43–45. [Google Scholar] [CrossRef] [PubMed]
- Paal, E.; Miettinen, M. Retroperitoneal Leiomyomas: A Clinicopathologic and Immunohi: The American Journal of Surgical Pathology. Am. J. Surg. Pathol. 2001, 25, 1355–1363. Available online: https://journals.lww.com/ajsp/Abstract/2001/11000/Retroperitoneal_Leiomyomas__A_Clinicopathologic.2.aspx (accessed on 30 July 2023). [CrossRef]
- Kelley, T.W.; Borden, E.C.; Goldblum, J.R. Estrogen and progesterone receptor expression in uterine and extrauterine leiomyosarcomas: An immunohistochemical study. Appl. Immunohistochem Mol. Morphol. AIMM 2004, 12, 338–341. Available online: https://pubmed.ncbi.nlm.nih.gov/15536333/ (accessed on 30 July 2023). [CrossRef]
- Leiomyosarcoma of the Pulmonary Veins: The American Journal of Surgical Pathology. Available online: https://journals.lww.com/ajsp/Abstract/1999/09000/Leiomyosarcoma_of_the_Pulmonary_Veins.11.aspx (accessed on 30 July 2023).
- Miettinen, M.; Fetsch, J.F. Evaluation of biological potential of smooth muscle tumours. Histopathology 2006, 48, 97–105. Available online: https://pubmed.ncbi.nlm.nih.gov/16359541/ (accessed on 30 July 2023). [CrossRef]
- The Difficulty in Predicting Behavior of Smooth-Muscle Tumor: The American Journal of Surgical Pathology. Available online: https://journals.lww.com/ajsp/Citation/1995/01000/The_Difficulty_in_Predicting_Behavior_of.15.aspx (accessed on 30 July 2023).
- Billings, S.D.; Folpe, A.L.; Weiss, S.W. Do leiomyomas of deep soft tissue exist? An analysis of highly differentiated smooth muscle tumors of deep soft tissue supporting two distinct subtypes. Am. J. Surg. Pathol. 2001, 25, 1134–1142. Available online: https://pubmed.ncbi.nlm.nih.gov/11688572/ (accessed on 30 July 2023). [CrossRef]
- Trojani, M.; Contesso, G.; Coindre, J.M.; Rouesse, J.; Bui, N.B.; De Mascarel, A.; Goussot, J.F.; David, M.; Bonichon, F. Lagarde C. Soft-tissue sarcomas of adults; study of pathological prognostic variables and definition of a histopathological grading system. Int. J. Cancer 1984, 33, 37–42. Available online: https://onlinelibrary.wiley.com/doi/full/10.1002/ijc.2910330108 (accessed on 30 July 2023). [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: Chicago, IL, USA, 2018. [Google Scholar]
- Danieli, M.; Gronchi, A. Staging Systems and Nomograms for Soft Tissue Sarcoma. Curr. Oncol. 2023, 30, 3648–3671. Available online: https://www.mdpi.com/1718-7729/30/4/278/htm (accessed on 2 August 2023). [CrossRef] [PubMed]
- Székely, E.; Kulka, J.; Miklós, I.; Kaliszky, P. Leiomyosarcomas of great vessels. Pathol. Oncol. Res. 2000, 6, 233–236. Available online: https://pubmed.ncbi.nlm.nih.gov/11033466/ (accessed on 30 July 2023). [CrossRef] [PubMed]
- Penel, N.; Taieb, S.; Ceugnart, L.; Dansin, E.; Hoguet, D.; Vanseymortier, L.; Lartigau, E. Report of eight recent cases of locally advanced primary pulmonary artery sarcomas: Failure of Doxorubicin-based chemotherapy. J. Thorac. Oncol. 2008, 3, 907–911. Available online: https://pubmed.ncbi.nlm.nih.gov/18670310/ (accessed on 2 August 2023). [CrossRef] [PubMed]
- Burke, A.P.; Virmani, X. Sarcomas of the Great Vessels A Clinicopathologic Study. Available online: https://pubmed.ncbi.nlm.nih.gov/8448740/ (accessed on 30 July 2023).
- Coindre, J.M.; Terrier, P.; Guillou, L.; Le Doussal, V.; Oise Collin, F.; Ranchè, D.; Sastre, X.; Vilain, M.O.; Bonichon, F.; N’Guyen Bui, B. Predictive Value of Grade for Metastasis Development in the Main Histologic Types of Adult Soft Tissue Sarcomas A Study of 1240 Patients from the French Federation of Cancer Centers Sarcoma Group. 1999. Available online: https://pubmed.ncbi.nlm.nih.gov/11346874/ (accessed on 2 August 2023).
- Teixeira, F.J.R.; Netto SD do, C.; Perina AL de, F.; Torricelli, F.C.M.; Teixeira, L.R.; Zerati, A.E.; Ferreira, F.O.; Akaishi, E.H. Nahas W.C. Utiyama E.M. Leiomyosarcoma of the inferior vena cava: Survival rate following radical resection. Oncol. Lett. 2017, 14, 3909–3916. Available online: https://pubmed.ncbi.nlm.nih.gov/29098019/ (accessed on 23 September 2023). [CrossRef] [PubMed]
- Dew, J.; Hansen, K.; Hammon, J.; McCoy, T.; Levine, E.A.; Shen, P. Leiomyosarcoma of the inferior vena cava: Surgical management and clinical results. Am. Surg. 2005, 71, 497–501. Available online: https://pubmed.ncbi.nlm.nih.gov/16044929/ (accessed on 31 July 2023). [CrossRef] [PubMed]
- Laskin, W.B.; Fanburg-Smith, J.C.; Burke, A.P.; Kraszewska, E.; Fetsch, J.F.; Miettinen, M. Leiomyosarcoma of the inferior vena cava: Clinicopathologic study of 40 cases. Am. J. Surg. Pathol. 2010, 34, 873–881. Available online: https://pubmed.ncbi.nlm.nih.gov/20463568/ (accessed on 31 July 2023). [CrossRef] [PubMed]
- Borghese, O.; Pisani, A.; Dubrez, J.; Di Centa, I. Treatment outlines for the management of primary leiomyosarcoma of the inferior vena cava. J. Med. Vasc. 2022, 47, 65–70. Available online: https://pubmed.ncbi.nlm.nih.gov/35691665/ (accessed on 23 September 2023). [CrossRef]
- Borghi, A.; Scotto DIUccio, A.; Gronchi, A. Primary malignancy of the inferior vena cava, a review of surgical treatments and outcomes. J. Cardiovasc. Surg. 2022, 63, 649–663. Available online: https://pubmed.ncbi.nlm.nih.gov/36239928/ (accessed on 23 September 2023). [CrossRef]
- Demicco, E.G.; Boland, G.M.; Savannah, K.J.B.; Lusby, K.; Young, E.D.; Ingram, D.; Watson, K.L.; Bailey, M.; Guo, X.; Hornick, J.L.; et al. Progressive loss of myogenic differentiation in leiomyosarcoma has prognostic value. Histopathology 2015, 66, 627–638. Available online: https://pubmed.ncbi.nlm.nih.gov/24889065/ (accessed on 30 July 2023). [CrossRef]
- Miettinen, M.; Kopczynski, J.; Makhlouf, H.R.; Sarlomo-Rikala, M.; Gyorffy, H.; Burke, A.; Sobin, L.H.; Lasota, J. Gastrointestinal stromal tumors, intramural leiomyomas, and leiomyosarcomas in the duodenum: A clinicopathologic, immunohistochemical, and molecular genetic study of 167 cases. Am. J. Surg. Pathol. 2003, 27, 625–641. Available online: https://pubmed.ncbi.nlm.nih.gov/12717247/ (accessed on 28 August 2022). [CrossRef] [PubMed]
- Kawaguchi, K.I.; Oda, Y.; Saito, T.; Yamamoto, H.; Tamiya, S.; Takahira, T.; Miyajima, K.; Iwamoto, Y.; Tsuneyoshi, M. Mechanisms of inactivation of the p16INK4a gene in leiomyosarcoma of soft tissue: Decreased p16 expression correlates with promoter methylation and poor prognosis. J. Pathol. 2003, 201, 487–495. Available online: https://pubmed.ncbi.nlm.nih.gov/14595762/ (accessed on 31 July 2023). [CrossRef] [PubMed]
- Baia, M.; Naumann, D.N.; Wong, C.S.; Mahmood, F.; Parente, A.; Bissacco, D.; Almond, M.; Ford, S.J.; Tirotta, F.; Desai, A. Dealing with malignancy involving the inferior vena cava in the 21st century. J. Cardiovasc. Surg. 2022, 63, 664–673. Available online: https://pubmed.ncbi.nlm.nih.gov/36239927/ (accessed on 23 September 2023). [CrossRef] [PubMed]
- Pan, J.; Qiu, C.Y.; He, Y.Y.; Xue, X.; Li, D.L.; Tian, L.; Cheng, F.; Wu, Z.H.; Zhang, H.K. A 10-year experience of leiomyosarcoma of the inferior vena cava. Phlebology 2022, 37, 572–578. Available online: https://pubmed.ncbi.nlm.nih.gov/35570826/ (accessed on 23 September 2023). [CrossRef] [PubMed]
- Ferraris, M.; Callegaro, D.; Barretta, F.; Fiore, M.; Radaelli, S.; Stacchiotti, S.; Miceli, R.; Socrate, A.M.; Locati, P.; Gronchi, A. Outcome of iliocaval resection and reconstruction for retroperitoneal sarcoma. J. Vasc. Surg. Venous Lymphat. Disord. 2019, 7, 547–556. Available online: https://pubmed.ncbi.nlm.nih.gov/30792153/ (accessed on 23 September 2023). [CrossRef] [PubMed]
- Gaignard, E.; Bergeat, D.; Robin, F.; Corbière, L.; Rayar, M.; Meunier, B. Inferior Vena Cava Leiomyosarcoma: What Method of Reconstruction for Which Type of Resection? World J. Surg. 2020, 44, 3537–3544. Available online: https://pubmed.ncbi.nlm.nih.gov/32445073/ (accessed on 23 September 2023). [CrossRef] [PubMed]
- Silva, T.A.; Buonfiglio, V.B.; Sadi, M.V. Leiomyosarcoma of the Inferior Vena Cava and Vascular Reconstruction. Urology 2022, 168, e15–e17. Available online: https://pubmed.ncbi.nlm.nih.gov/35908743/ (accessed on 23 September 2023). [CrossRef] [PubMed]
- Goodsell, K.E.; Sharib, J.M.; Pillarisetty, V.G.; Sham, J.G. Leiomyosarcoma of the inferior vena cava: An uncommon malignancy requiring unique reconstructive approaches. Am. J. Surg. 2023, 226, 286–289. Available online: https://pubmed.ncbi.nlm.nih.gov/36959023/ (accessed on 23 September 2023). [CrossRef]
- Wachtel, H.; Jackson, B.M.; Bartlett, E.K.; Karakousis, G.C.; Roses, R.E.; Bavaria, J.E.; Fraker, D.L. Resection of primary leiomyosarcoma of the inferior vena cava (IVC) with reconstruction: A case series and review of the literature. J. Surg. Oncol. 2015, 111, 328–333. Available online: https://pubmed.ncbi.nlm.nih.gov/25297650/ (accessed on 23 September 2023). [CrossRef]
- Risaliti, M.; Fortuna, L.; Bartolini, I.; Taddei, A.; Muiesan, P. Inferior vena cava resection and reconstruction with a peritoneal patch for a leiomyosarcoma: A case report. Int. J. Surg. Case Rep. 2020, 71, 37–40. [Google Scholar] [CrossRef]
- Kunte, A.; Patkar, S.; Goel, M. Inferior Vena Cava (IVC) Resection without Reconstruction for a Large IVC Leiomyosarcoma. J. Gastrointest. Surg. 2022, 26, 2014–2018. Available online: https://pubmed.ncbi.nlm.nih.gov/35581461/ (accessed on 23 September 2023). [CrossRef] [PubMed]
- Villar, V.H.; Vögler, O.; Martínez-Serra, J.; Ramos, R.; Calabuig-Fariñas, S.; Gutiérrez, A.; Barceló, F. Martín-Broto J.; Alemany R. Nilotinib counteracts P-glycoprotein-mediated multidrug resistance and synergizes the antitumoral effect of doxorubicin in soft tissue sarcomas. PLoS ONE 2012, 7, e37735. [Google Scholar] [CrossRef] [PubMed]
- Hollenbeck, S.T.; Grobmyer, S.R.; Kent, K.C.; Brennan, M.F. Surgical treatment and outcomes of patients with primary inferior vena cava leiomyosarcoma. J. Am. Coll. Surg. 2003, 197, 575–579. Available online: https://pubmed.ncbi.nlm.nih.gov/14522326/ (accessed on 31 July 2023). [CrossRef] [PubMed]
- Ito, H.; Hornick, J.L.; Bertagnolli, M.M.; George, S.; Morgan, J.A.; Baldini, E.H.; Wagner, A.J.; Demetri, G.D.; Raut, C.P. Leiomyosarcoma of the inferior vena cava: Survival after aggressive management. Ann. Surg. Oncol. 2007, 14, 3534–3541. Available online: https://pubmed.ncbi.nlm.nih.gov/17896156/ (accessed on 2 August 2023). [CrossRef] [PubMed]
- Sakpal, S.V.; Mehta, R.; Babel, N.; Chamberlain, R.S. Peripheral artery leiomyosarcoma. J. Vasc. Surg. 2009, 49, 217–221. Available online: http://www.jvascsurg.org/article/S0741521408011750/fulltext (accessed on 31 July 2023). [CrossRef] [PubMed]
- Zhou, M.; Javadi, C.; Charville, G.W.; Bui, N.Q.; Harris, E.J.; Poultsides, G.A.; Norton, J.A.; Visser, B.; Lee, B.; Dua, M.M.; et al. Surgical resection of leiomyosarcoma of the inferior vena cava: A case series and literature review. Surg. Oncol. 2021, 39, 101670. Available online: https://pubmed.ncbi.nlm.nih.gov/34710646/ (accessed on 23 September 2023). [CrossRef]
- Saikia, J.; Rastogi, S.; Barwad, A.; Dhamija, E.; Pandey, R.; Bhoriwal, S.; Deo, S.; Kumar, S. A systematic review of the current management approaches in leiomyosarcoma of inferior vena cava-Results from analysis of 118 cases. Asian Cardiovasc. Thorac Ann. 2022, 30, 349–363. Available online: https://pubmed.ncbi.nlm.nih.gov/34672808/ (accessed on 23 September 2023). [CrossRef]
- Pautier, P.; Italiano, A.; Piperno-Neumann, S.; Chevreau, C.; Penel, N.; Firmin, N.; Boudou-Rouquette, P.; Bertucci, F.; Balleyguier, C.; Lebrun-Ly, V.; et al. Doxorubicin alone versus doxorubicin with trabectedin followed by trabectedin alone as first-line therapy for metastatic or unresectable leiomyosarcoma (LMS-04): A randomised, multicentre, open-label phase 3 trial. Lancet Oncol. 2022, 23, 1044–1054. Available online: http://www.thelancet.com/article/S1470204522003801/fulltext (accessed on 2 August 2023). [CrossRef]
- De Graaff, M.A.; De Rooij, M.A.J.; Van Den Akker, B.E.W.M.; Gelderblom, H.; Chibon, F.; Coindre, J.M.; Marino-Enriquez, A.; Fletcher, J.A.; Cleton-Jensen, A.M.; Bovée, J.V.M.G. Inhibition of Bcl-2 family members sensitises soft tissue leiomyosarcomas to chemotherapy. Br. J. Cancer 2016, 114, 1219. Available online: https://pmc/articles/PMC4891502/ (accessed on 23 September 2023). [CrossRef]
- Oliveira, R.C.; Gama, J.; Casanova, J. B-cell lymphoma 2 family members and sarcomas: A promising target in a heterogeneous disease. Explor. Target Anti-Tumor Ther. 2023, 4, 583–599. Available online: https://www.explorationpub.com/Journals/etat/Article/1002154 (accessed on 23 September 2023). [CrossRef]
- Nakamura, T.; Sudo, A. The Role of Trabectedin in Soft Tissue Sarcoma. Front. Pharmacol. 2022, 13, 777872. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, M.; Casanova, J.M.; Rodrigues, J.; Freitas, J.; Fonseca, R.; Caetano De Oliveira, R.; Tavares, P.F. Long-Term Response after 94 Cycles of Trabectedin in a Patient with Metastatic Leiomyosarcoma of the Lower Extremity. Case Rep. Oncol. 2020, 13, 113–119. Available online: https://pubmed.ncbi.nlm.nih.gov/32231532/ (accessed on 2 August 2023). [CrossRef] [PubMed]
- Le Cesne, A.; Blay, J.Y.; Cupissol, D.; Italiano, A.; Delcambre, C.; Penel, N.; Isambert, N.; Chevreau, C.; Bompas, E.; Bertucci, F.; et al. A randomized phase III trial comparing trabectedin to best supportive care in patients with pre-treated soft tissue sarcoma: T-SAR, a French Sarcoma Group trial. Ann. Oncol. 2021, 32, 1034–1044. Available online: http://www.annalsofoncology.org/article/S0923753421011716/fulltext (accessed on 2 August 2023). [CrossRef] [PubMed]
- Hatta, M.; Kaibori, M.; Matsushima, H.; Yoshida, T.; Okumura, T.; Hayashi, M.; Yoshii, K.; Todo, T.; Sekimoto, M. Efficacy of a third-generation oncolytic herpes simplex virus in refractory soft tissue sarcoma xenograft models. Mol. Ther. Oncolytics 2022, 25, 225–235. Available online: https://pubmed.ncbi.nlm.nih.gov/35615265/ (accessed on 2 August 2023). [CrossRef] [PubMed]
- Italiano, A.; Bellera, C.; D’Angelo, S. PD1/PD-L1 targeting in advanced soft-tissue sarcomas: A pooled analysis of phase II trials. J. Hematol. Oncol. 2020, 13, 55. Available online: https://pubmed.ncbi.nlm.nih.gov/32430039/ (accessed on 5 August 2023). [CrossRef] [PubMed]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; de Jesus-Acosta, A.; Delord, J.P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/mismatch repair–deficient cancer: Results from the phase II KEYNOTE-158 study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef]
- Lam, S.W.; Kostine, M.; de Miranda, N.F.C.C.; Schöffski, P.; Lee, C.J.; Morreau, H.; Bovée, J.V.M.G. Mismatch repair deficiency is rare in bone and soft tissue tumors. Histopathology 2021, 79, 509. Available online: https://pmc/articles/PMC8518745/ (accessed on 5 August 2023). [CrossRef]
- Tay, T.K.Y.; Yeong, J.P.S.; Chen, E.X.; Sam, X.X.; Lim, J.X.; Chan, J.Y. Soft Tissue Leiomyosarcoma With Microsatellite Instability, High Tumor Mutational Burden, and Programmed Death Ligand-1 Expression Showing Pathologic Complete Response to Pembrolizumab: A Case Report. JCO Precis. Oncol. 2022, 6, e2200068. Available online: https://pubmed.ncbi.nlm.nih.gov/35939769/ (accessed on 5 August 2023). [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gama, J.M.; Almeida, R.; Oliveira, R.C.; Casanova, J. When Vessels and Sarcomas Combine: A Review of the Inferior Vena Cava Leiomyosarcoma. J. Vasc. Dis. 2024, 3, 34-48. https://doi.org/10.3390/jvd3010003
Gama JM, Almeida R, Oliveira RC, Casanova J. When Vessels and Sarcomas Combine: A Review of the Inferior Vena Cava Leiomyosarcoma. Journal of Vascular Diseases. 2024; 3(1):34-48. https://doi.org/10.3390/jvd3010003
Chicago/Turabian StyleGama, João Martins, Rui Almeida, Rui Caetano Oliveira, and José Casanova. 2024. "When Vessels and Sarcomas Combine: A Review of the Inferior Vena Cava Leiomyosarcoma" Journal of Vascular Diseases 3, no. 1: 34-48. https://doi.org/10.3390/jvd3010003