1. Introduction
Healthcare in South Africa is a complex and multifaceted issue encompassing various challenges and disparities. The country’s healthcare system faces fundamental challenges, including resource constraints, inefficiencies, and disparities in access to care [
1,
2,
3,
4]. The demand for healthcare is influenced by factors such as racial differences, household size, and geographical accessibility [
4,
5,
6,
7]. Additionally, the burden of disease, the impact of the HIV epidemic, and the COVID-19 pandemic further strain the healthcare system [
8]. The disparities in healthcare access are evident in the rural–urban health divide and the persistent healthcare disparities, which are exacerbated by the historical context of apartheid policies [
9,
10].
To address some of these challenges, the government implemented National Health Insurance (NHI) to improve equity and access to healthcare for the entire population [
11,
12]. It also seeks to align policy development, resource allocation, and the integration of innovative technologies to improve quality healthcare. While some members of society embrace the NHI, there are concerns regarding its financial implications and potential impact on the healthcare system [
13].
Universities, which influence healthcare policy and train healthcare workers to serve the diverse population, have seen their medical and dental education curricula evolve considerably, adapting to global trends and local challenges [
14,
15]. While there is a growing emphasis on expanding health professionals’ training, the capacity of educational institutions remains a concern [
16]. Factors such as limited faculty numbers, inadequate infrastructure, and financial constraints hinder the expansion of training programs [
17,
18]. However, efforts are being made to increase capacity through public–private partnerships and the introduction of innovative teaching methodologies, such as simulation-based training and online learning platforms [
19].
The throughput rate of health professional programs is a critical indicator of the effectiveness of these educational systems. Studies have shown that attrition rates in health professional programs are a concern, with factors such as academic difficulty, financial challenges, and personal circumstances contributing to dropout rates [
20]. However, initiatives like student support programs and curriculum reforms aim to improve retention and graduation rates while aligning with the country’s healthcare needs [
21].
1.1. Medical and Dental Education Reforms in South Africa
Curriculum reform in South African medical and dental education has been an ongoing process, responding to the changing healthcare landscape and societal needs. The two primary drivers for this curriculum reform are ideological and curriculum reform. Ideological reform involves the transformation of the beliefs, values, and philosophies that inform education policies and practices [
22], while curriculum reform involves changes in the content, structure, and delivery of the curriculum within educational institutions [
23].
In post-apartheid South Africa, ideological reform attempts to transform higher education by addressing history-, race-, and gender-based inequalities and promoting inclusivity and equity [
24,
25]. Efforts to decolonize higher education institutions, democratize education, and promote citizenship education are evident [
26]. This transformation includes broader societal objectives like reconciliation and nation-building through higher education [
27]. Ideological reform also includes decolonizing higher education and the curriculum by reversing the hegemony of Eurocentrism in teaching, learning, and research [
28]. This includes transforming pedagogical practices, teaching, and learning [
29] and integrating and contextualizing students’ realities into curriculum designs [
30].
Curriculum reform attempts to align curriculum standards with international standards and respond to local needs [
31]. In medical and dental education, curriculum reform has shifted towards community-oriented medical and dental education, emphasizing primary healthcare and social accountability [
32]. Traditional lecture-based teaching is replaced with student-centered and work-based learning, including early clinical exposure [
33]. Interprofessional education that promotes a holistic understanding of patient care has been adopted [
34]. Furthermore, there has been an effort to incorporate ethical and humanistic components into medical training, including medical humanities, health systems science, medical ethics, patient rights, communication skills, and the social determinants of health [
35]. Alongside curriculum changes, there has been a shift in assessment strategies to emphasize work-based assessment, continuous assessment, practical examinations, and clinical skills assessment.
The challenge, however, is aligning ideological reforms and curriculum reforms into a coherent, explicit curriculum ideology. Balancing ideological and curriculum objectives while ensuring comprehensive, relevant, and equitable medical and dental education remains complex. The Health Professions Council of South Africa (HPCSA) [
36] adopted a new curriculum framework, colloquially known as AfriMEDS, to address this quagmire. The HPCSA is the statutory body established to regulate health professions in South Africa. Its mandate is derived from the Health Professions Act 56 of 1974. The primary function of the HPCSA is to set and maintain standards for education, training, and ethical practice in the healthcare sector to ensure that the public receives quality healthcare. In 2014, the HPCSA adopted the AfriMEDS curriculum framework.
1.2. The AfriMEDS Curriculum Framework
The AfriMEDS curriculum framework [
36], a pioneering initiative in South African medical and dental education, represents a significant step towards shared comprehensive curriculum reform in undergraduate medical and dental education programs. It provides “core competencies for undergraduate students in clinical associate, dentistry, and medical teaching and learning programs in South Africa” [
36] (p. 1). This framework was adapted from the CanMEDS Physician Competency Framework [
37,
38] as a collaborative effort involving various stakeholders, including educational institutions, healthcare providers, and government bodies. Its inception was driven by a critical need to address the disparities in healthcare delivery and the uneven distribution of healthcare professionals, exacerbated by the legacy of apartheid [
4,
39]. It represents an attempt to overhaul the traditional medical and dental education system, which was primarily hospital-based and specialized, to a more community-oriented and integrated approach [
40,
41].
The AfriMEDS curriculum framework establishes a comprehensive set of core competencies for undergraduate medical and dental education in South Africa. It emphasizes the role of a healthcare practitioner, which integrates graduate attributes, profession-specific knowledge, clinical skills, and professional attitudes toward providing patient/client-centered care. Additionally, it underscores the importance of acquiring and maintaining knowledge, skills, attitudes, and character appropriate for practice, involving a broad range of academic and scientific disciplines. The AfriMEDS curriculum framework also highlights the collaborator role, stressing the need for effective teamwork, respect for diversity, and leadership within healthcare teams. As leaders and managers, students are encouraged to engage in activities that enhance the functionality of healthcare organizations and systems, manage their practices and careers efficiently, and adeptly use information technology in healthcare settings. In the role of health advocates, the focus is on responding to individual health needs and broader community health issues as part of holistic care. As scholars, students are encouraged to commit to lifelong learning, critical evaluation, and the application of knowledge, including an understanding of research design and ethics. Lastly, the professional role calls for the demonstration of ethical practice, adherence to professional codes, and maintenance of professional relationships. These competencies prepare healthcare professionals for ethical, comprehensive, and patient/client-centered care across various health and social contexts in South Africa.
1.3. Problem Statement
While the AfriMEDS curriculum framework represents a pivotal shift in the approach to undergraduate medical and dental education, a notable gap exists in understanding how this framework amalgamates ideological reform and curriculum reform within the South African context. This is because the curriculum ideologies underlying this framework have not been defined in the literature. Therefore, the extent to which the AfriMEDS curriculum framework promotes standardized quality medical and dental education, which could lead to social transformation, is unclear. Given the authority of this framework in medical and dental education in South Africa, it is imperative to explore its underlying curriculum ideologies to advance its potential to cultivate the competent, empathetic, and socially responsible medical professionals that South Africa needs. Such professionals would be academically proficient and adept in responding to the diverse and complex health needs of the South African population, driven by socio-economic and political dynamics.
1.4. Aim of the Research
Considering the above discourse, this research is a preliminary effort to assess the extent to which the ideological and curriculum reforms in health professional education in South Africa are aligned. More specifically, the research aimed to qualitatively describe the curriculum ideologies underlying the AfriMEDS framework as a proxy to determine how the framework could facilitate the required training of healthcare practitioners fit to address healthcare challenges in South Africa.
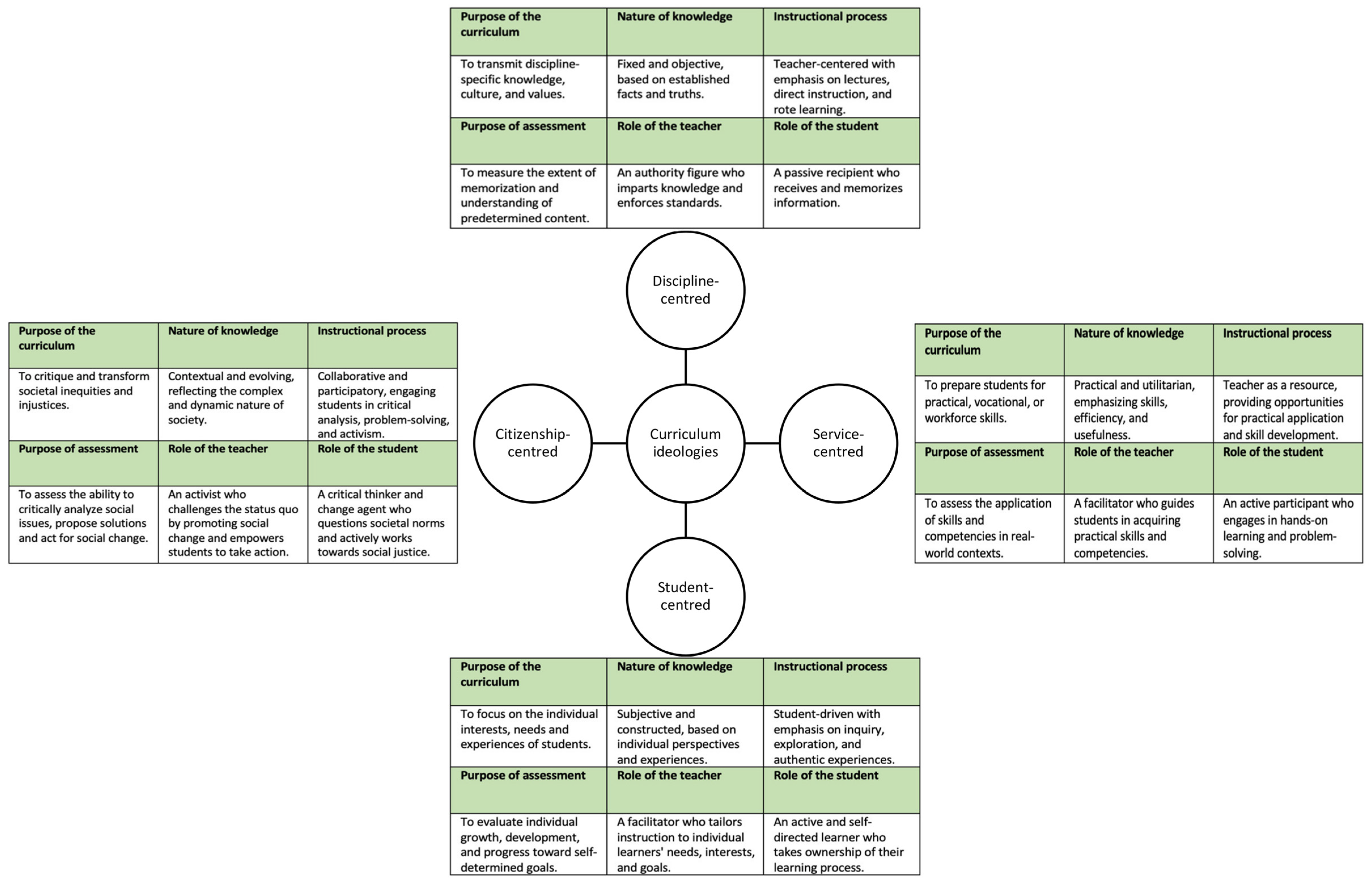
1.5. Theoretical Framework: Curriculum Ideologies
The current research adopted Schiro’s [
42] curriculum ideologies as a theoretical framework to address the research aim. A curriculum ideology refers to “the overarching aims or purposes of education, the nature of the student, the way learning must take place, the role of the teacher during instruction, the most important kind of knowledge that the curriculum is concerned with, and the approach to knowledge, and assessment” [
42] (p. 7). Curriculum ideologies, namely, discipline-centered, service-centered, student-centered, and citizenship-centered ideologies (
Figure 1), represent foundational beliefs about education and its role in society, leading to distinct approaches in curriculum design.
Curricula that adopt discipline-centered ideology are predicated on mastering discipline-specific knowledge and advocating for a rigorous, structured, and knowledge-centric education that prioritizes intellectual development and the transmission of discipline heritage [
42,
43]. Service-centered ideology requires curricula to align with society’s socio-economic and practical needs [
44,
45]. This pragmatic approach emphasizes job readiness, equipping students with skills directly applicable to the workforce and responding to market demands [
42,
46]. The student-centered ideology in curricula, championed by theorists like Beane [
47], places the individual student’s needs, interests, and experiences at the core of the educational process. This ideology supports the idea that education should be tailored to foster personal growth, self-actualization, and the construction of knowledge through active learning [
42]. The citizenship-centered ideology emphasizes cultivating civic virtues and competencies necessary for social transformation through democratic participation. This approach aims to prepare students to be informed, critical, and engaged citizens capable of contributing to the betterment of society [
24].
2. Methodology
This study used a rigorous content analysis approach to examine the AfriMEDS curriculum framework for undergraduate medical and dental education. The AfriMEDS curriculum framework was purposively selected as it is endorsed by the HPCSA and guides the accreditation of all medical and dental schools in South Africa.
A previously validated 6-item standardized document analysis protocol (
Table 1) was used to analyze the AfriMEDS curriculum framework [
43,
44,
48]. This protocol has undergone thorough validation for face, criterion-related, and content validity by a panel of experts, ensuring its suitability for the current research. It has also been used previously to determine curriculum ideologies in school curricula [
43,
44,
48]. Utilizing a standardized protocol enhances the research’s consistency, validity, credibility, and trustworthiness.
In the current research, content analysis primarily focused on responding to the six open-ended items in this protocol (
Table 1), with responses comprising verbatim extracts from the AfriMEDS curriculum framework. Specifically, in line with the theoretical framework (
Figure 1), the AfriMEDS curriculum framework was analyzed to determine the purpose of medical and dental education, the approach to knowledge taught, the instructional process, the roles of the teacher and student, and the approach to assessment (
Figure 1).
ChatGPT 4.0, set for Browsing and Advanced Data Analysis, was used to identify relevant text extracts of the AfriMEDS curriculum framework, which the researcher later analyzed. This process involved two main steps: developing prompts and extracting text from the AfriMEDS curriculum framework, as described below.
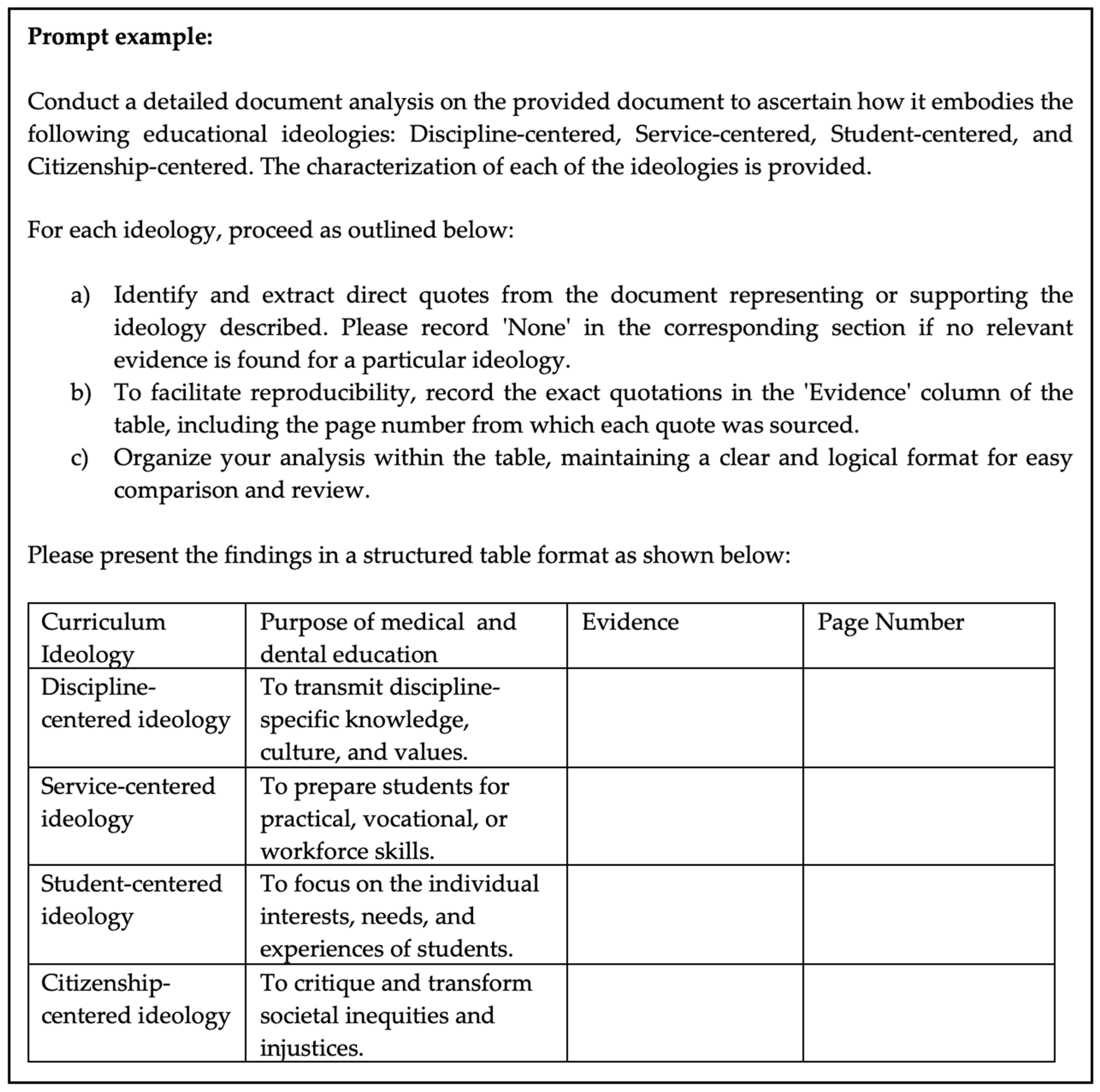
2.1. Prompt Development
A systematic approach was followed in developing effective ChatGPT prompts to ensure that they are clear, focused, and capable of analyzing the document [
49,
50,
51]. This approach, informed by Poola [
49] and White et al. [
52], involved drafting the prompts, ensuring they were clear and concise, and directly addressing the research objectives. Ambiguous language that could lead to misinterpretation was avoided. The drafted prompts were tested by running them on ChatGPT to identify the type of responses generated. This testing phase was crucial to refine the prompts for clarity and effectiveness. Based on the responses, the prompts were refined to better align with the research objectives. This involved adjusting the complexity of the language and rephrasing questions for clarity. Each version of the prompt and the rationale behind each iteration were documented. A pilot test with the final version of the prompt was carried out to ensure that the prompts consistently generated the desired type of responses. An independent panel of experts with diverse skills, including educational background, considered the prompts for face-, construct-, and criterion-related validity. Having satisfied himself with the pilot test results and feedback from the panel of experts, the researcher proceeded to use the final set of prompts in the research (e.g.,
Figure 2).
2.2. Data Extraction
ChatGPT was then prompted to extract text from the AfriMEDS curriculum framework, which describes the purpose of medical and dental education, the approach to knowledge taught, the instructional process, the roles of the teacher and student, and the approach to assessment (
Table 1). To ensure confirmability, this process was repeated until saturation was reached. Specifically, the first two rounds of data extraction were carried out. The output was then manually compared by the researcher to determine consistency. Some discrepancies were identified where the extracted text lacked depth, and the extent of the evidence was not consistent. Consequently, further rounds of extraction were conducted until the data generated were comprehensive, detailed, and consistently reliable. The researcher manually verified the output, cross-checking the extracts against the original document to ensure confirmability.
2.3. Data Analysis
Having extracted the data, the researcher performed an interpretive analysis to determine the curriculum ideologies inferred. After initial data extraction, the researcher manually examined the extracted text for underlying meanings, context, and implications, going beyond the literal content. This approach involved critically analyzing how the AfriMEDS curriculum framework reflects curriculum ideologies based on their characterization (
Figure 1). The extracted data were analyzed to determine whether they reflect any of the ideologies in
Figure 1. For example, extracts relating to the purpose of medical and dental education were analyzed to determine if the stated, implied, or inferred purpose was to:
- -
“Transmit discipline-specific knowledge, culture and values”, which is indicative of the discipline-centered ideology;
- -
“Prepare students for practical, vocational, or workforce skills”, which is indicative of the service-centered ideology;
- -
“Focus on the individual interests, needs, and experiences of students”, which is indicative of the student-centered ideology;
- -
“Critique and transform societal inequities and injustices”, which is indicative of citizenship-centered ideology.
Therefore, the researcher interpreted the data to uncover implicit assumptions, values, and beliefs in the curriculum, providing a nuanced understanding of how the AfriMEDS curriculum framework aligns with or deviates from each curriculum ideology.
An independent researcher considered the interpretive analysis generated by the primary researcher for credibility and confirmability. Specifically, the independent researcher cross-verified the primary researcher’s analysis by identifying overlooked aspects and challenging interpretations, prompting a deeper and more critical analysis. This led to the refining and strengthening of the arguments and conclusions drawn from the data. Where disagreements emerged, additional data to support either argument were manually extracted and analyzed to settle the disagreements. This way, the conclusions were reached based on the data available.
3. Presentation and Interpretation of the Results
The data provided insightful analysis of the prevalence of different educational ideologies. In some instances, evidence was extensive where aspects of the ideology are a central, recurrent theme throughout the framework. Instances of moderate evidence were also observed where aspects of the ideology were clearly acknowledged and addressed but were not a central or pervasive theme. Some of the evidence was shallow, where aspects of the ideology were barely evident or were reflected at a very basic level. In this regard, it was found that the discipline-centered ideology is predominantly evident in the purpose of medical and dental education and approach to knowledge, suggesting a strong focus on specific disciplines or subject matter. However, minimal prevalence was noted in the instructional process and role of the student. In contrast, evidence of service-centered ideology was comprehensive across most components, especially in the approach to assessment and the role of the teacher, with moderate presence in the role of the student. The student-centered ideology was notably absent in the purpose of medical and dental education and approach to knowledge. However, it is evident in the approach to assessment and the role of the student. Extensive evidence of the citizenship-centered ideology was found in the instructional process and approach to assessment, with shallow presence in the role of the teacher. Each of the components is presented in detail below.
3.1. Purpose of Medical and Dental Education
The data analysis revealed that the AfriMEDS curriculum framework adopts discipline-centered, service-centered, and citizenship-centered ideologies as reflected in the purpose of medical and dental education (
Table 2). No evidence of the student-centered ideology was found. In this regard, the emphasis on integrating “profession-specific knowledge, clinical skills, and professional attitudes” aligns with the discipline-centered ideology, which prioritizes transmitting discipline-specific knowledge and values. This ideology focuses on the mastery of a fixed body of knowledge and clinical skills essential for medical practice, underscoring the traditional view of medical and dental education to impart established facts and principles relevant to healthcare practice. Therefore, the healthcare professional’s role is predominantly as a knowledgeable authority, delivering patient/client-centered care based on established medical disciplines.
The data (
Table 2) reflect the service-centered ideology by focusing on the application of skills in patient care. The mention of “performing comprehensive assessments” and effectively using various “interventions” emphasizes preparing students for practical, vocational skills relevant to the healthcare workforce. This approach underlines the utilitarian and practical aspects of medical and dental education, where the purpose is to develop efficient and skilled practitioners capable of delivering a range of diagnostic and therapeutic procedures. The ideology here is rooted in the practical utility of education, aimed at serving the immediate needs of patients and the healthcare system.
The absence of data aligning with the student-centered ideology in the AfriMEDS curriculum framework suggests that the purpose of medical and dental education does not focus on individual student interests, needs, or experiences as a central theme. The student-centered ideology typically involves tailoring education to individual students, emphasizing inquiry and exploration and fostering self-directed learning. The lack of evidence for this ideology in the AfriMEDS curriculum framework may indicate a more traditional approach to medical and dental education, focusing less on subjective, individualized learning experiences.
Data indicative of the citizenship-centered ideology were identified (
Table 2), focusing on social responsibility and advocacy. The emphasis on acting as “advocates” for “marginalized groups” and responding to the needs of “vulnerable populations” with a commitment to equity reflects this ideology’s aim to critique and transform societal inequities. The purpose of medical and dental education here extends beyond individual patient care to include a broader social context, where healthcare professionals are seen as agents of social change, promoting equity and access to care. This perspective aligns with the idea of training healthcare professionals as clinicians who are socially responsible citizens who advocate for societal well-being.
3.2. Approach to Knowledge
Data regarding the AfriMEDS curriculum framework’s approach to knowledge revealed evidence for all ideologies except for the student-centered ideology. Specifically, some extracts from the AfriMEDS curriculum framework (e.g.,
Table 3) exemplify the discipline-centered ideology, as they emphasize the importance of “core knowledge”, which includes “academic literacy, numeracy, and information technology skills”, alongside “natural sciences and understanding normal human structure.” This focus reflects the ideology’s characteristic of valuing fixed and objective knowledge grounded in established scientific facts. The emphasis on “reflection, integration, application, and evaluation” aligns with the discipline-centered instructional process, which aims to ensure that students understand and can utilize the predetermined content.
Data aligning with the service-centered ideology were also identified (
Table 3), highlighting a focus on preparing students for practical skills necessary in healthcare. The emphasis on “consultations and facilitating clinical encounters effectively, including documentation” aligns with the ideology’s practical and utilitarian knowledge approach. Furthermore, providing compassionate and patient-centered care reflects the ideology’s focus on skills, efficiency, and usefulness in real-world contexts.
Evidence of the citizenship-centered ideology was also identified (
Table 3), including a focus on “critical analysis”, understanding “research design and ethics”, and actively engaging in the healthcare community. This reflects the ideology’s characteristic of knowledge being contextual, evolving, and aimed at critiquing and transforming societal inequities. The emphasis on playing a “constructive, critical, and creative role” in healthcare aligns with the ideology’s goal of preparing students to be change agents and critical thinkers, actively working towards social justice and community betterment.
3.3. Instructional Process Approach
Regarding the instructional process, data revealed that the discipline-centered ideology is not explicitly represented, as the AfriMEDS curriculum framework lacks direct reference to traditional pedagogical approaches (
Table 4). Instead of emphasizing lectures, direct instruction, and rote learning, the AfriMEDS curriculum framework adopts contemporary educational approaches, focusing on clinical skills and social responsibilities and aligning more closely with other curriculum ideologies.
Data reflecting the service-centered ideology were identified, emphasizing the practical application of skills in a work-based learning context (
Table 4). Learning facilitated within community settings where students interact with diverse groups, including patients, families, and professionals, aligns with this ideology. In this regard, the instructional process involves the teacher as a resource provider, guiding students in applying their skills and knowledge in practical, real-world scenarios, which is a hallmark of the service-centered approach. The emphasis on facilitation, rather than direct instruction, suggests a focus on practical skill application and utility in various contexts.
Data also suggest a strong alignment with the student-centered ideology by highlighting the importance of self-reflection and acknowledging one’s strengths and limitations. This approach fosters a student-driven instructional process, focusing on personal growth and development. The emphasis on reflection suggests an educational environment where students are encouraged to critically evaluate their learning journey, an essential aspect of the student-centered ideology. This ideology values the subjective construction of knowledge and individual experiences, promoting students as active and self-directed students.
The citizenship-centered ideology is also reflected where the AfriMEDS curriculum framework emphasizes collaboration and engagement in activities beyond individual learning, such as research, program review, and administrative tasks. The focus on collaboration for societal tasks indicates an instructional process that encourages critical thinking, problem-solving, and activism. This reflects the ideology’s goal of preparing students to critique and transform societal inequities and injustices, fostering a sense of social responsibility and activism. The collaborative nature of these activities supports the development of students as change agents and critical thinkers.
3.4. Approach to Assessment
Regarding the approach to assessment, the discipline-centered ideology was moderately represented, as the AfriMEDS curriculum framework integrates knowledge and skill acquisition within a broader context of patient-centered care. In contrast, extensive evidence for service-centered and student-centered ideologies was identified. For example, concerning discipline-centered ideology, the AfriMEDS curriculum framework states that students are expected to “acquire and maintain knowledge, skills, attitudes, and character appropriate to their practice” (p. 2). Such knowledge, skills, attitudes, and character would then be assessed to certify that students have met the required competencies. This approach to assessment reflects a discipline-centered ideology that emphasizes discipline-specific traits deemed essential for the practice. This further suggests that the assessment will likely be more traditional, emphasizing objective knowledge and skill acquisition measurements.
Regarding service-centered ideology, the AfriMEDS curriculum framework states that, on graduating, students should “function effectively as entry-level healthcare practitioners… in a plurality of health and social contexts.” (p. 2). They must also “provide compassionate empathetic and patient/client-centered care” (p. 2). These competencies would be assessed through relevant approaches. Notably, the focus on preparing students for assessable practical roles in healthcare, emphasizing effectiveness in diverse health and social contexts, and giving the ability to provide patient-centered care is typical in the service-centered ideology. Assessments in this regard would measure the application of skills in practical, real-world situations, evaluating students’ ability to adapt to different contexts and to provide compassionate and empathetic care. The hands-on approach emphasizes practical skills and their direct application in healthcare settings.
The student-centered ideology was also observed where the AfriMEDS curriculum framework states that students are expected to “Reflect on, integrate, apply, and evaluate core knowledge skills, attitudes, and character acquired during undergraduate training” (p. 2). Additionally, they must “reflect on and acknowledge the strengths and limitations of their knowledge and skills” (p. 11). This implies that self-assessment in the form of reflection forms a core competence in the AfriMEDS curriculum framework. It prioritizes the individual student’s process of reflection, integration, application, and evaluation of their learning. Assessments in this ideology would focus on personal growth and development, measuring how well students can reflect on their learning, recognize their strengths and limitations, and apply their knowledge and skills in various contexts. This approach encourages self-assessment and continuous self-improvement, focusing on the development of the student as a whole.
The AfriMEDS curriculum framework also reflects the citizenship-centered ideology. According to this framework, students are expected to “demonstrate a commitment to work in primary healthcare settings (urban and rural) and find professional and personal satisfaction in it” (p. 2). They must also “respond to the health needs of the communities that they serve” (p. 10). This approach aligned with a citizenship-centered ideology, focusing on responding to community health needs and working in various healthcare settings, including challenging environments like rural areas. Assessments would focus on students’ ability to engage with and address community health issues, demonstrating a commitment to social responsibility and the ability to find satisfaction in serving diverse populations. This approach emphasizes social consciousness, critical thinking, and the capacity to act as agents of change in healthcare.
3.5. Role of the Teacher and the Student
Concerning the role of the teacher (
Table 5), the AfriMEDS curriculum framework examined presents a multifaceted ideology, with moderate evidence supporting a discipline-centered ideology, as indicated by the recurrent theme of healthcare practitioners’ centrality, integrating graduate attributes (e.g., professional knowledge, clinical skills). For example, data suggest that the AfriMEDS framework emphasizes the need for teachers to help students integrate “profession-specific knowledge, clinical skills, and professional attitudes”, which is typical in the discipline-centered ideology. In this ideology, the teacher is viewed as an authoritative figure who imparts fixed, objective knowledge and skills relevant to healthcare. It reflects a traditional view in which the teacher imparts knowledge, and students are expected to acquire this specialized knowledge and apply it in a patient-centered manner. The focus on specific professional roles and the integration of these roles further underline the structured, discipline-specific nature of the curriculum. Notably, there was no evidence to suggest that the role of the student follows the discipline-centered ideology.
However, data were found indicating that the role of the student follows the service-centered ideology, which emphasizes that practical, utilitarian knowledge and skills are learned. Students must apply their learning to real-world scenarios, “demonstrating problem-solving abilities and judgment in clinical settings.” The focus is on applying knowledge for effective patient care, characteristic of a service-centered approach where the utility and application of skills in practical contexts are paramount. Relatedly, the role of the teacher also follows the service-centered ideology, in which the emphasis is on practical skills and attributes necessary for effective teamwork and patient care. In this context, the teacher’s role shifts to being a facilitator and resource provider, guiding students in developing practical, real-world skills such as collaboration, communication, and empathy. This utilitarian approach focuses on preparing students to serve patients and communities effectively, with the teacher supporting students in applying these skills in practical, clinical settings. The emphasis on therapeutic relationships and teamwork skills indicates a curriculum geared towards practical, service-oriented outcomes.
The student-centered ideology was also observed concerning the role of the teacher, in which the focus is on developing individual competencies like compassion, empathy, and effective communication. In this approach, the teacher’s role is to facilitate individual student growth and learning. The teacher supports students in exploring and developing these personal attributes, encouraging self-reflection and self-directed learning. The emphasis on patient/client-centered care and effective consultation points to an educational approach that values student experiences and perspectives, allowing them to construct knowledge through real-world clinical encounters and patient interactions. Similarly, the role of the student is underpinned by the student-centered ideology, where the focus is on the student’s individual growth, self-directed learning, and personal experiences. The emphasis on life-long learning, reflection, and the integration of new knowledge with practice showcases an approach in which students are active, self-motivated students. They are encouraged to continuously develop their skills, adapt to new information, and critically evaluate their practices. This ideology promotes students as constructors of their knowledge, reflecting on experiences and learning autonomously, which is essential for professional and personal development in healthcare.
Evidence of the citizenship-centered ideology concerning the role of the student was also found. Specifically, the AfriMEDS framework emphasizes critical thinking, social responsibility, and transformative action. Students are expected to advocate for vulnerable groups and engage critically with public health policies, reflecting a commitment to social justice and ethical practice. This ideology positions students as active change agents equipped to challenge and transform societal inequalities and injustices. Their role extends beyond individual patient care to include a broader societal perspective, where they are encouraged to recognize and address the social determinants of health and contribute to the well-being of diverse communities. The role of the teacher is also underpinned by the citizenship-centered ideology, in which advocacy for health and well-being at individual, community, and population levels are encouraged. The teacher is expected to act as an activist and mentor, guiding students to understand and engage with broader societal issues. The teacher empowers students to use their expertise for social change and community benefit, fostering critical thinking and social responsibility. This approach aligns with the notion of teachers preparing students as healthcare practitioners and agents of change who can address and influence public health issues and inequalities.
4. Discussion
The analysis of the AfriMEDS curriculum framework revealed a complex interplay of curriculum ideologies, each contributing uniquely to shaping medical and dental education in South Africa. These findings have critical implications for curriculum and instructional design.
The first significant finding was that the six components of curriculum ideologies—the purpose of medical and dental education, knowledge approach, instructional process, roles of teacher and student, and assessment approach—exhibit varying degrees of ideological representation. For instance, an ideology might be extensively reflected in the purpose of medical and dental education but overlooked in the approach to assessment. This lack of uniformity can significantly affect how curriculum designers and teachers at different medical schools interpret and implement the AfriMEDS framework. Variability in how these ideologies are represented across different curriculum components can lead to inconsistent interpretations and applications [
43]. For instance, a strong focus on the discipline-centered ideology in the curriculum’s purpose might not align with a student-centered approach to assessment. This disparity can create confusion and difficulties in creating a cohesive educational experience. Teachers might struggle to integrate these varied ideologies into a consistent teaching strategy, potentially leading to a fragmented and less-effective educational framework.
Such disparities indicate that there is no consensus on a guiding ideology for curriculum design in South African medical and dental education. This absence of a coherent ideological foundation can lead to educational strategies that are misaligned with the overarching goals of the AfriMEDS framework. It underscores the need for a more integrated approach, where all curriculum components—from educational purposes to assessment strategies—are informed by a consistent set of curriculum ideologies. This would ensure the uniform interpretation and application of the AfriMEDS framework, leading to a more cohesive and effective medical and dental education system in South Africa.
A second significant finding was the absence of a single dominant ideology across all components, highlighting a pluralistic approach in South African medical and dental education. While potentially enriching, this pluralism also presents challenges in achieving a cohesive educational strategy [
53]. Without a prevailing ideology across all components, the AfriMEDS framework risks lacking a unified direction, potentially leading to inconsistencies in educational outcomes across the different universities [
54]. This finding underscores the need for a more deliberate integration of ideologies to ensure a balanced and coherent curriculum [
38].
A third significant finding was that the discipline- and service-centered ideologies are the most dominant ideologies underlying the AfriMEDS curriculum framework, while the student-centered ideology is the least. This dominance is implied by the availability of recurring evidence in the framework suggesting that these ideologies significantly shape the framework’s content, approach, or perspective. The citizenship-centered ideology was moderately represented with noticeable but not extensive evidence. This finding underscores a traditional medical and dental education approach emphasizing profession-specific knowledge and practical competencies. However, the dominance of the discipline- and service-centered ideologies aligns with the global trend in medical and dental education that values domain-specific expertise and clinical skills [
55,
56]. It also aligns with reforms in South Africa, such as early clinical exposure and work-based learning. It also aligns with contemporary shifts in medical and dental education, where the applicability of knowledge in real-world contexts is increasingly valued [
57]. However, it has been argued that an excessive focus on discipline-specific knowledge may limit the holistic development of medical professionals [
58]. In particular, a discipline-specific siloed approach could frustrate efforts toward interprofessional and interdisciplinary education and the incorporation of ethical and humanistic components into medical training [
35].
The minimal representation of the student-centered ideology suggests a lack of focus on personalized and individualized learning experiences, which contrasts with recent educational trends advocating for more student-centered approaches [
59]. This minimal representation was noted as the evidence was barely mentioned or evident at a very basic level, implying that the ideology does not significantly influence or shape the overall content or approach of the framework. These approaches emphasize the importance of tailoring education to individual learning styles and needs, fostering a more engaging and effective learning environment [
60]. The minimal representation of this ideology in the AfriMEDS curriculum framework might limit the adaptability and responsiveness of the curriculum to diverse student needs. This is particularly significant in South Africa, where students come from diverse socio-economic backgrounds and could benefit from a curriculum that addresses their needs.
A moderate representation of the citizenship-centered ideology in the AfriMEDS curriculum framework suggests the promotion of advocacy and equity for vulnerable groups. This aligns with emerging trends in medical and dental education that acknowledge the importance of social responsibility and community engagement [
32]. However, the fact that the citizenship-centered ideology is not dominant in the AfriMEDS curriculum framework suggests a potential gap in fully embracing social accountability [
61]. In particular, graduates may not be fully equipped to identify and address social determinants of health through active citizenship. It also implies that the extent to which students could be active, informed, and responsible citizens who can engage with societal issues critically, understand social justice, and participate actively in community life may also be moderate and far less than envisaged in the ideological reforms in South Africa [
42,
44]. This is particularly concerning given the socio-economic determinants of health, which play a significant role in South African healthcare.
The AfriMEDS curriculum framework embodies a complex interplay of different curriculum ideologies. While it strongly favors discipline- and service-centered approaches, reflecting traditional and practical aspects of medical and dental education, it emphasizes less student-centered and citizenship-centered ideologies. This may indicate a need for greater balance to accommodate evolving educational paradigms that prioritize individualized learning experiences and social accountability in medical and dental education.
5. Recommendations
Considering that the AfriMEDS curriculum framework does not differentiate disciplines, future research should examine the curriculum ideologies reflected in the enacted curricula in medical and dental education to determine alignment with the AfriMEDS curriculum ideologies. Such research should also investigate the curriculum ideologies within and between medical and dental education disciplines, as the emphasis may vary. Determining the extent to which the underlying ideologies manifest in practice post-graduation is also important. This research will be crucial for determining the extent to which ideological reform and curriculum reform are aligned and facilitate the training of healthcare practitioners fit to address healthcare challenges in South Africa.
Furthermore, comprehensive guidelines on how curriculum ideologies should be interpreted and integrated into curricula should be developed to ensure the effective integration of curriculum ideologies in medical and dental education. These guidelines should include strategies for balancing diverse ideologies, ensuring that each component of the curriculum reflects a harmonious blend of discipline-centered, service-centered, student-centered, and citizenship-centered approaches. Additionally, there should be explicit instructions for teachers on adapting their teaching methods to align with these integrated ideologies. This approach will facilitate a more consistent and effective educational experience, accommodating the varied learning needs of students and the complex demands of medical and dental education.
6. Conclusions
The findings from the analysis of the AfriMEDS curriculum framework have significant implications for medical and dental education in South Africa. The dominance of discipline-centered and service-centered ideologies in the AfriMEDS curriculum framework suggests a robust focus on imparting technical expertise and practical skills, which are crucial in a healthcare landscape marked by diverse and complex medical challenges. Such a focus ensures that medical graduates are equipped to address the specific health needs of South African communities, particularly in resource-limited settings.
However, the minimal representation of the student-centered ideology raises concerns about future medical professionals’ adaptability and critical thinking skills. Given the rapidly evolving medical field, where personalized care and continuous learning are paramount, the lack of emphasis on student-centered approaches may limit the ability of graduates to adapt to new challenges and innovations. This gap suggests a need for curriculum reform incorporating more holistic educational strategies, fostering technical proficiency, critical analysis, problem-solving, and lifelong learning skills.
While the AfriMEDS curriculum framework is well-positioned to produce technically skilled and service-oriented practitioners, its effectiveness in nurturing well-rounded, adaptable medical professionals may be limited. Integrating a balanced representation of all curriculum ideologies would be beneficial to achieving a more comprehensive educational outcome. Such a balanced approach would ensure a well-rounded curriculum that combines discipline-specific knowledge, service orientation, student autonomy, and civic responsibility. Such a holistic educational framework is crucial in the South African context, where diverse healthcare needs demand healthcare practitioners who are clinically competent, socially aware, empathetic, and adaptable to various community and individual patient needs. This comprehensive training approach would better prepare medical professionals for the multifaceted challenges they may face in their practice.





{kind=link}
{kind=link}