
Depression Events Associated with Proton-Pump Inhibitors in Postmarketing Drug Surveillance Data
Abstract
:1. Introduction
2. Methods
2.1. FDA Adverse Event Reporting System
2.2. Data Preparation
2.3. Analysis and Control Cohort Selection
2.4. Statistical Analysis
- a = Number of cases in PPI group with depression;
- b = Number of cases in PPI group with no depression;
- c = Number of cases in H2RA group with depression;
- d = Number of cases in H2RA group with no depression.
3. Results
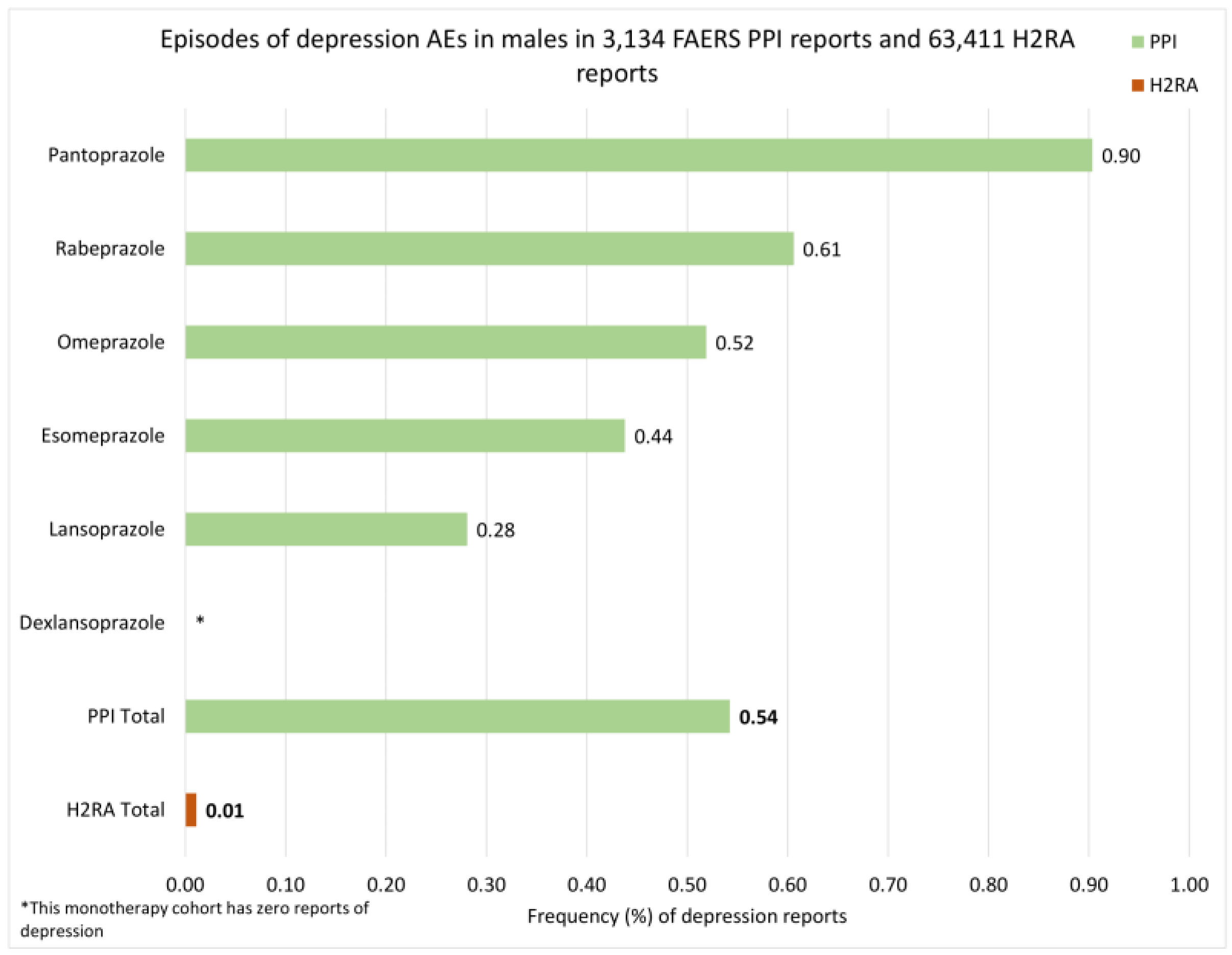
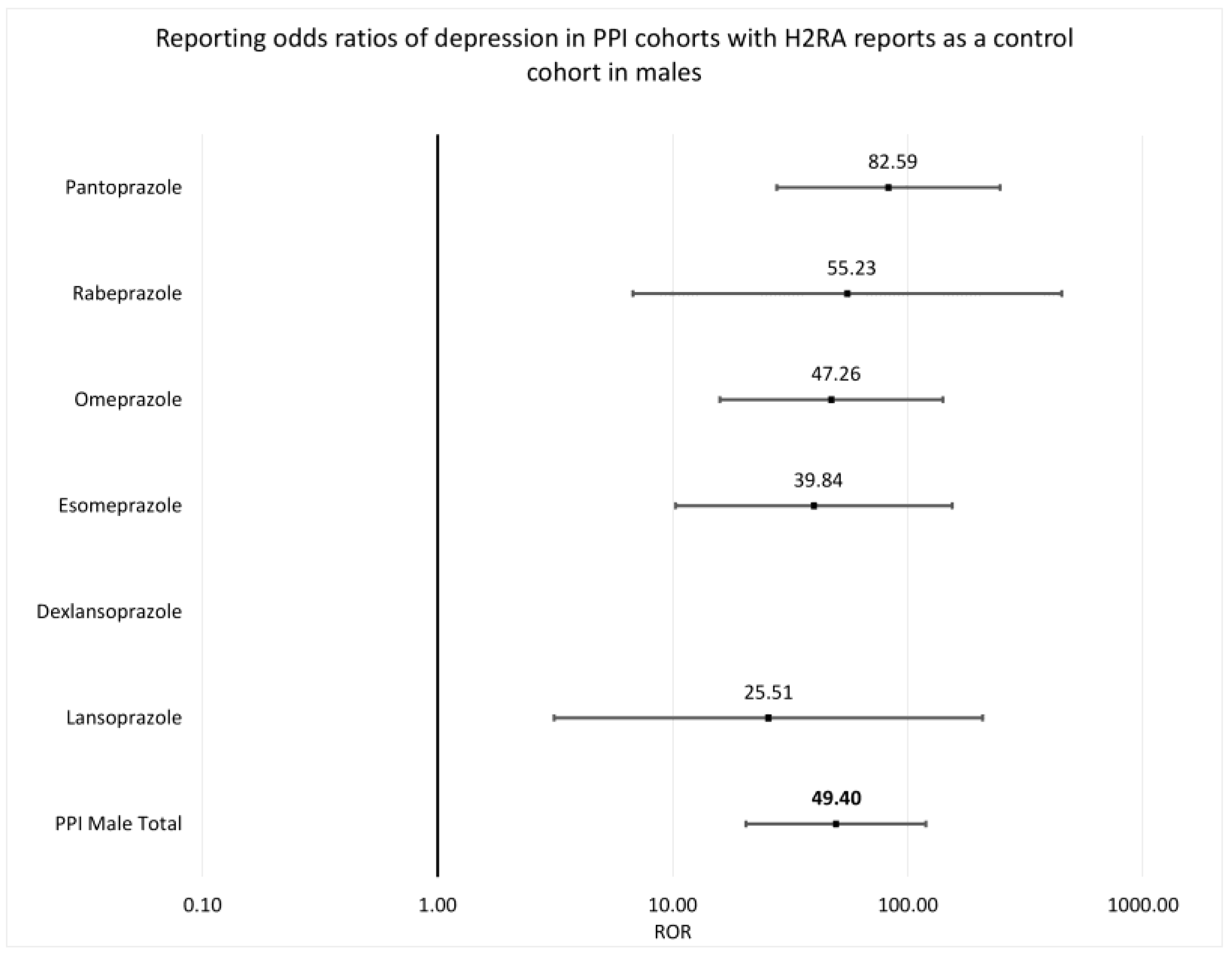
3.1. Depression Reports in Males
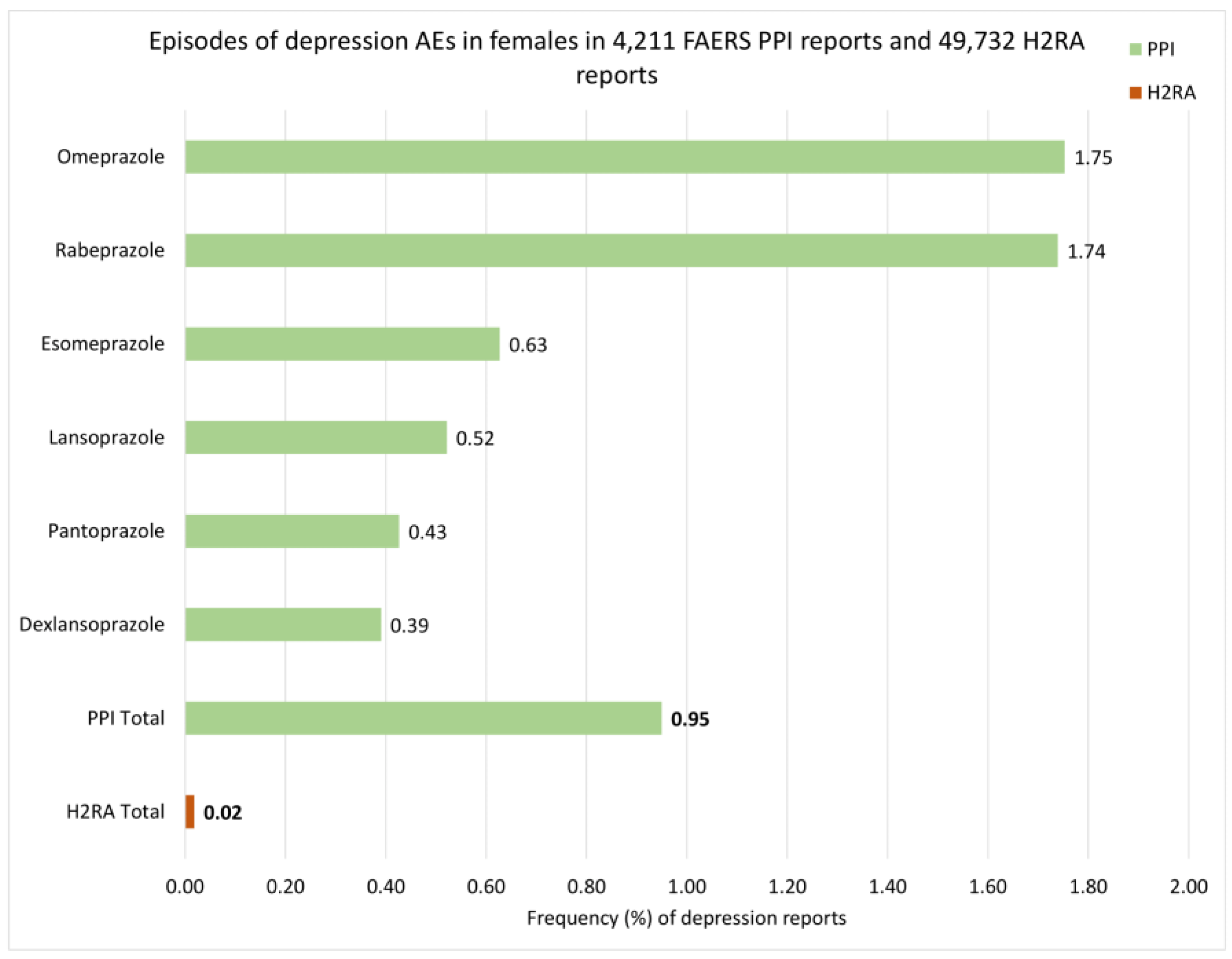
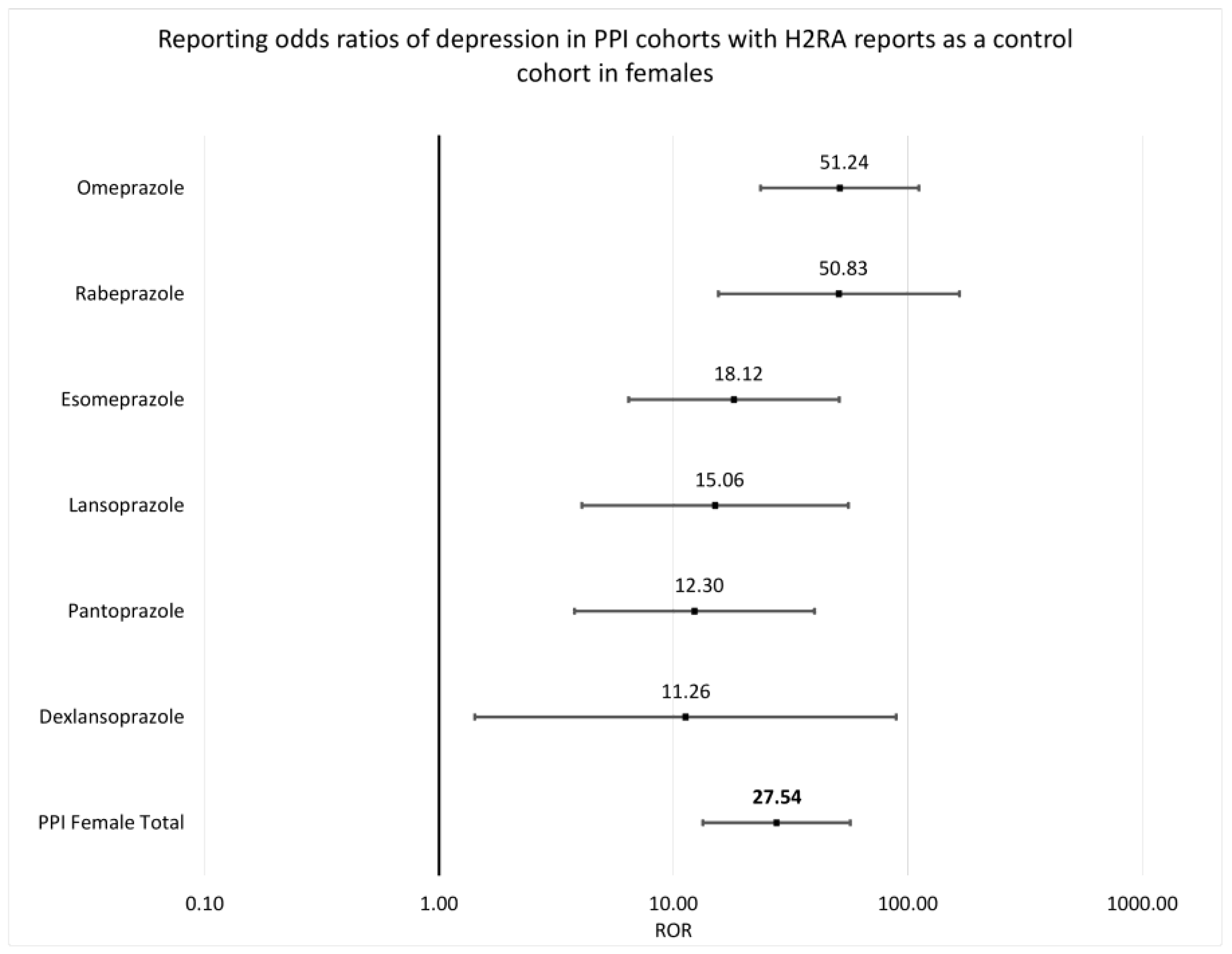
3.2. Depression Reports in Females
4. Discussion
Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Song, H.; Zhu, J.; Lu, D. Long-term proton pump inhibitor (PPI) use and the development of gastric pre-malignant lesions. Cochrane Database Syst. Rev. 2014, 12, CD010623. [Google Scholar] [CrossRef]
- Katz, P.O.; Dunbar, K.B.; Schnoll-Sussman, F.H.; Greer, K.B.; Yadlapati, R.; Spechler, S.J. ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease. Am. J. Gastroenterol. 2022, 117, 27–56. [Google Scholar] [CrossRef]
- Londong, W.; Barth, H.; Dammann, H.G.; Hengels, K.J.; Kleinert, R.; Müller, P.; Rohde, H.; Simon, B. Dose-related healing of duodenal ulcer with the proton pump inhibitor lansoprazole. Aliment. Pharmacol. Ther. 1991, 5, 245–254. [Google Scholar] [CrossRef]
- Wu, J.C.Y.; Sheu, B.S.; Wu, M.S.; Lee, Y.C.; Choi, M.G. Phase 4 Study in Patients From Asia With Gastroesophageal Reflux Disease Treated With Dexlansoprazole. J. Neurogastroenterol. Motil. 2020, 26, 85–95. [Google Scholar] [CrossRef]
- Kinoshita, Y.; Miwa, H.; Kasugai, K. Efficacy and safety of esomeprazole, compared with omeprazole, in maintenance therapy for reflux esophagitis -a phase III, multicenter, randomized, double-blind trial-. Nihon Shokakibyo Gakkai Zasshi 2013, 110, 1428–1438. [Google Scholar]
- Zhao, F.; Wang, S.; Liu, L.; Wang, Y. Comparative effectiveness of histamine-2 receptor antagonists as short-term therapy for gastro-esophageal reflux disease: A network meta-analysis. Int. J. Clin. Pharmacol. Ther. 2016, 54, 761–770. [Google Scholar] [CrossRef]
- Walan, A.; Bader, J.P.; Classen, M.; Lamers, C.B.; Piper, D.W.; Rutgersson, K.; Eriksson, S. Effect of omeprazole and ranitidine on ulcer healing and relapse rates in patients with benign gastric ulcer. N. Engl. J. Med. 1989, 320, 69–75. [Google Scholar] [CrossRef]
- Clissold, S.P.; Campoli-Richards, D.M. Omeprazole. A preliminary review of its pharmacodynamic and pharmacokinetic properties, and therapeutic potential in peptic ulcer disease and Zollinger-Ellison syndrome. Drugs 1986, 32, 15–47. [Google Scholar] [CrossRef]
- Shin, J.M.; Sachs, G. Pharmacology of proton pump inhibitors. Curr. Gastroenterol. Rep. 2008, 10, 528–534. [Google Scholar] [CrossRef]
- Shin, J.M.; Munson, K.; Vagin, O.; Sachs, G. The gastric HK-ATPase: Structure, function, and inhibition. Pflugers Arch. 2009, 457, 609–622. [Google Scholar] [CrossRef]
- Abrahami, D.; McDonald, E.G.; Schnitzer, M.; Azoulay, L. Trends in prescribing patterns of proton pump inhibitors surrounding new guidelines. Ann. Epidemiol. 2021, 55, 24–26. [Google Scholar] [CrossRef]
- Kantor, E.D.; Rehm, C.D.; Haas, J.S.; Chan, A.T.; Giovannucci, E.L. Trends in Prescription Drug Use Among Adults in the United States From 1999–2012. JAMA 2015, 314, 1818–1831. [Google Scholar] [CrossRef]
- FDA Label-Omeprazole. United States Food and Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/019810s096lbl.pdf (accessed on 1 October 2022).
- FDA Label-Esomeprazole. United States Food and Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/022101s014021957s017021153s050lbl.pdf (accessed on 1 October 2022).
- FDA Label-Rabeprazole. United States Food and Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/020973s035204736s005lbl.pdf (accessed on 1 October 2022).
- FDA Label-Pantoprazole. United States Food and Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020987s045lbl.pdf (accessed on 1 October 2022).
- FDA Label-Lansoprazole. United States Food and Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020406s078-021428s025lbl.pdf (accessed on 1 October 2022).
- FDA Label-Dexlansoprazole. United States Food and Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020406s078-021428s025lbl.pdf (accessed on 1 October 2022).
- Haenisch, B.; von Holt, K.; Wiese, B.; Prokein, J.; Lange, C.; Ernst, A.; Brettschneider, C.; König, H.H.; Werle, J.; Weyerer, S.; et al. Risk of dementia in elderly patients with the use of proton pump inhibitors. Eur. Arch. Psychiatry Clin. Neurosci. 2015, 265, 419–428. [Google Scholar] [CrossRef]
- Gomm, W.; von Holt, K.; Thomé, F.; Broich, K.; Maier, W.; Fink, A.; Doblhammer, G.; Haenisch, B. Association of Proton Pump Inhibitors With Risk of Dementia: A Pharmacoepidemiological Claims Data Analysis. JAMA Neurol. 2016, 73, 410–416. [Google Scholar] [CrossRef]
- Goldstein, F.C.; Steenland, K.; Zhao, L.; Wharton, W.; Levey, A.I.; Hajjar, I. Proton Pump Inhibitors and Risk of Mild Cognitive Impairment and Dementia. J. Am. Geriatr. Soc. 2017, 65, 1969–1974. [Google Scholar] [CrossRef]
- Makunts, T.; Cohen, I.V.; Awdishu, L.; Abagyan, R. Analysis of postmarketing safety data for proton-pump inhibitors reveals increased propensity for renal injury, electrolyte abnormalities, and nephrolithiasis. Sci. Rep. 2019, 9, 2282. [Google Scholar] [CrossRef]
- Makunts, T.; Alpatty, S.; Lee, K.C.; Atayee, R.S.; Abagyan, R. Proton-pump inhibitor use is associated with a broad spectrum of neurological adverse events including impaired hearing, vision, and memory. Sci. Rep. 2019, 9, 17280. [Google Scholar] [CrossRef]
- Melero, I.; Grimaldi, A.M.; Perez-Gracia, J.L.; Ascierto, P.A. Clinical development of immunostimulatory monoclonal antibodies and opportunities for combination. Clin. Cancer Res. 2013, 19, 997–1008. [Google Scholar] [CrossRef]
- Verghese, A. The integration of psychiatry and neurology. Indian J. Psychiatry 2016, 58, 104–105. [Google Scholar] [CrossRef]
- Rickards, H. Depression in neurological disorders: An update. Curr. Opin. Psychiatry 2006, 19, 294–298. [Google Scholar] [CrossRef]
- Makunts, T.; Abagyan, R. How can proton pump inhibitors damage central and peripheral nervous systems? Neural Regen. Res. 2020, 15, 2041–2042. [Google Scholar] [CrossRef]
- Song, T.; Jeon, H.K.; Hong, J.E.; Choi, J.J.; Kim, T.J.; Choi, C.H.; Bae, D.S.; Kim, B.G.; Lee, J.W. Proton Pump Inhibition Enhances the Cytotoxicity of Paclitaxel in Cervical Cancer. Cancer Res. Treat. 2017, 49, 595–606. [Google Scholar] [CrossRef]
- Yepuri, G.; Sukhovershin, R.; Nazari-Shafti, T.Z.; Petrascheck, M.; Ghebre, Y.T.; Cooke, J.P. Proton Pump Inhibitors Accelerate Endothelial Senescence. Circ. Res. 2016, 118, e36–e42. [Google Scholar] [CrossRef]
- Laudisio, A.; Antonelli Incalzi, R.; Gemma, A.; Giovannini, S.; Lo Monaco, M.R.; Vetrano, D.L.; Padua, L.; Bernabei, R.; Zuccalà, G. Use of proton-pump inhibitors is associated with depression: A population-based study. Int. Psychogeriatr. 2018, 30, 153–159. [Google Scholar] [CrossRef]
- Wang, Y.H.; Wintzell, V.; Ludvigsson, J.F.; Svanström, H.; Pasternak, B. Proton pump inhibitor use and risk of depression and anxiety in children: Nationwide cohort study. Clin. Transl. Sci. 2022, 15, 1112–1122. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.S.; Bai, Y.M.; Hsu, J.W.; Huang, K.L.; Tsai, C.F.; Su, T.P.; Li, C.T.; Lin, W.C.; Tsai, S.J.; Pan, T.L.; et al. Use of Proton Pump Inhibitors and Risk of Major Depressive Disorder: A Nationwide Population-Based Study. Psychother. Psychosom. 2018, 87, 62–64. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.L.; Chen, C.L.; Wen, S.H. Profile of the Change in Depression during Proton-Pump Inhibitor Therapy in Patients with Gastroesophageal Reflux Disease: Influence of the Mucosal Break. Int. J. Environ. Res. Public. Health 2021, 18, 5964. [Google Scholar] [CrossRef] [PubMed]
- WHO-Global Burden of Disease. World Health Organization. Available online: https://apps.who.int/iris/bitstream/handle/10665/43942/9789241563710_eng.pdf (accessed on 1 October 2022).
- Craigle, V. MedWatch: The FDA Safety Information and Adverse Event Reporting Program. J. Med. Libr. Assoc. 2007, 95, 224–225. [Google Scholar] [CrossRef]
- Kessler, D.A. Introducing MEDWatch. A new approach to reporting medication and device adverse effects and product problems. JAMA 1993, 269, 2765–2768. [Google Scholar] [CrossRef] [PubMed]
- Wollmer, M.A.; Makunts, T.; Krüger, T.H.C.; Abagyan, R. Postmarketing safety surveillance data reveals protective effects of botulinum toxin injections against incident anxiety. Sci. Rep. 2021, 11, 24173. [Google Scholar] [CrossRef]
- Keshishi, D.; Makunts, T.; Abagyan, R. Common osteoporosis drug associated with increased rates of depression and anxiety. Sci. Rep. 2021, 11, 23956. [Google Scholar] [CrossRef]
- Weber, F.; Knapp, G.; Ickstadt, K.; Kundt, G.; Glass, Ä. Zero-cell corrections in random-effects meta-analyses. Res. Synth. Methods 2020, 11, 913–919. [Google Scholar] [CrossRef]
- Derom, M.L.; Sayón-Orea, C.; Martínez-Ortega, J.M.; Martínez-González, M.A. Magnesium and depression: A systematic review. Nutr. Neurosci. 2013, 16, 191–206. [Google Scholar] [CrossRef] [PubMed]
- Cheungpasitporn, W.; Thongprayoon, C.; Mao, M.A.; Srivali, N.; Ungprasert, P.; Varothai, N.; Sanguankeo, A.; Kittanamongkolchai, W.; Erickson, S.B. Hypomagnesaemia linked to depression: A systematic review and meta-analysis. Intern. Med. J. 2015, 45, 436–440. [Google Scholar] [CrossRef]
- Vink, R.; Nechifor, M. Magnesium in the Central Nervous System; University of Adelaide Press: Adelaide, Australia, 2011. [Google Scholar]
- Laird, E.; O’Halloran, A.M.; Molloy, A.M.; Healy, M.; Hernandez, B.; O’Connor, D.; Kenny, R.A.; Briggs, R. Low vitamin B. Br. J. Nutr. 2021, 130, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Syed, E.U.; Wasay, M.; Awan, S. Vitamin B12 supplementation in treating major depressive disorder: A randomized controlled trial. Open Neurol. J. 2013, 7, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Almeida, O.P.; Ford, A.H.; Flicker, L. Systematic review and meta-analysis of randomized placebo-controlled trials of folate and vitamin B12 for depression. Int. Psychogeriatr. 2015, 27, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Heidelbaugh, J.J. Proton pump inhibitors and risk of vitamin and mineral deficiency: Evidence and clinical implications. Ther. Adv. Drug Saf. 2013, 4, 125–133. [Google Scholar] [CrossRef]
- Lam, J.R.; Schneider, J.L.; Zhao, W.; Corley, D.A. Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B12 deficiency. JAMA 2013, 310, 2435–2442. [Google Scholar] [CrossRef]
- Rajabally, Y.A.; Jacob, S. Neuropathy associated with lansoprazole treatment. Muscle Nerve 2005, 31, 124–125. [Google Scholar] [CrossRef]
- García Rodríguez, L.A.; Mannino, S.; Wallander, M.A. Ocular safety of antiulcer drugs. Lancet 1995, 345, 1059–1060. [Google Scholar] [CrossRef] [PubMed]
- Sáez, M.E.; González-Pérez, A.; Gaist, D.; Johansson, S.; Nagy, P.; García Rodríguez, L.A. Risk of seizure associated with use of acid-suppressive drugs: An observational cohort study. Epilepsy Behav. 2016, 62, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Maciejewski, M.; Lounkine, E.; Whitebread, S.; Farmer, P.; DuMouchel, W.; Shoichet, B.K.; Urban, L. Reverse translation of adverse event reports paves the way for de-risking preclinical off-targets. eLife 2017, 6, e25818. [Google Scholar] [CrossRef] [PubMed]
- Alatawi, Y.M.; Hansen, R.A. Empirical estimation of under-reporting in the U.S. Food and Drug Administration Adverse Event Reporting System (FAERS). Expert. Opin. Drug Saf. 2017, 16, 761–767. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PPI Monotherapy | H2RA Monotherapy | PPI Depression | H2RA Depression | |
|---|---|---|---|---|
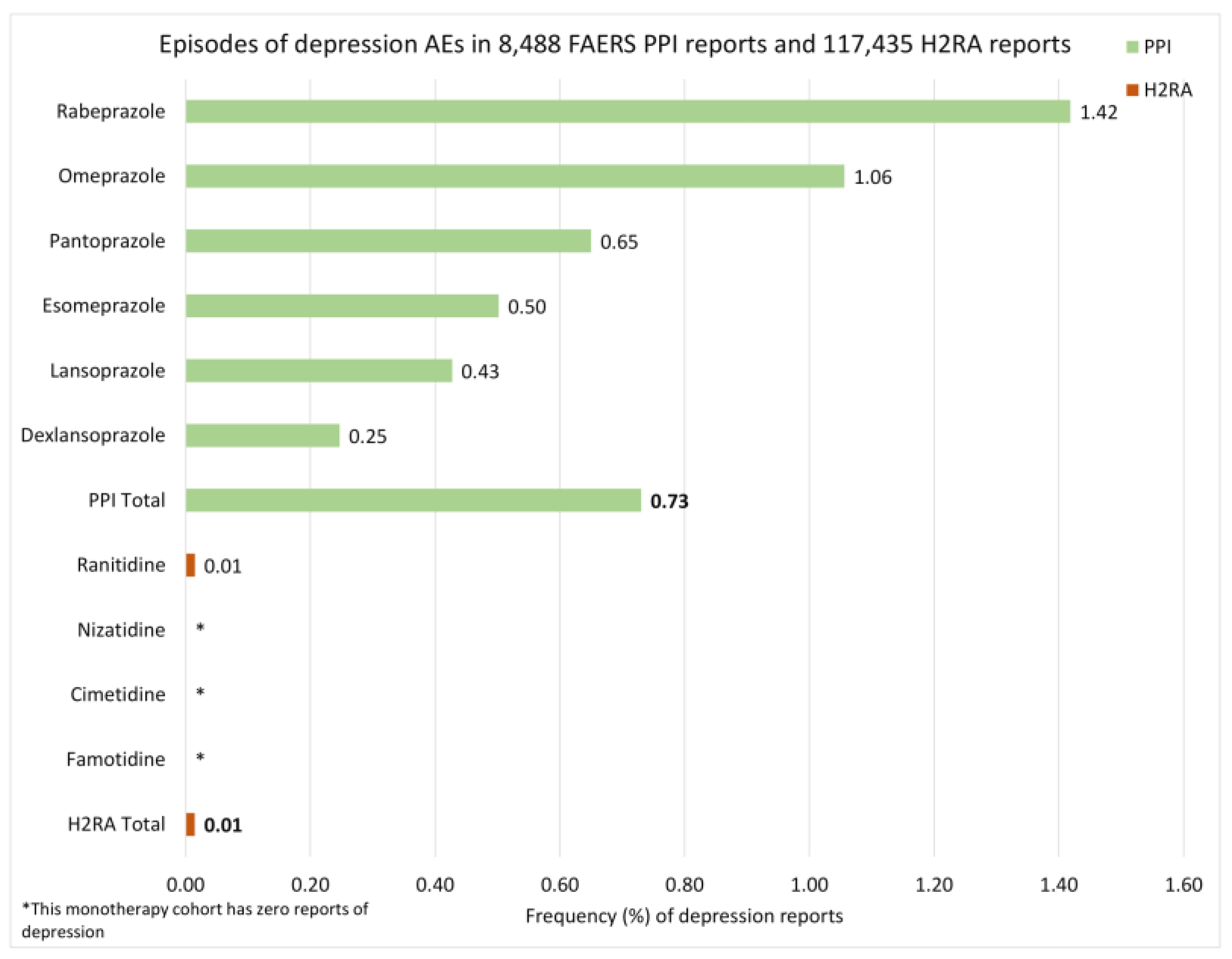
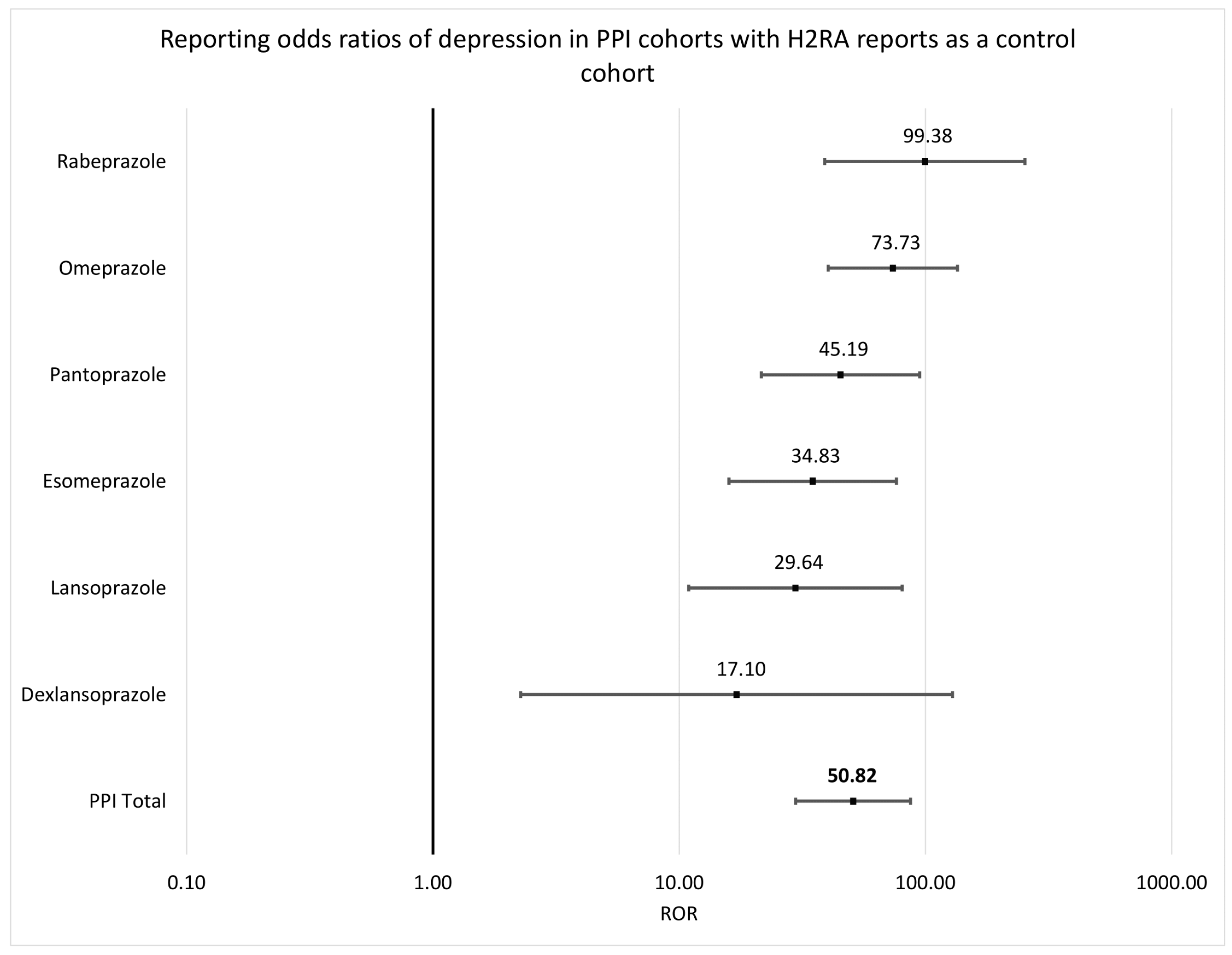
| Total reports | 100% (8488) | 100% (117,435) | 0.73% (62) | 0.01% (17) |
| Male | 36.92% (3134) | 54% (63,411) | 0.54% (17) | 0.01% (7) |
| Female | 49.61% (4211) | 42.35% (49,732) | 0.95% (40) | 0.02% (9) |
| Unspecified sex | 13.47% (1143) | 3.65% (4292) | 0.44% (5) | 0.02% (1) |
| PPI Monotherapy | H2RA Monotherapy | PPI Depression | H2RA Depression | |
|---|---|---|---|---|
| Total reports | 100% (8488) | 100% (117,435) | 0.61% (52) | 0.01% (17) |
| Invalid ages (<1 y.o.) | 1.43% (121) | 0.08% (97) | 0% (0) | 1.03% (1) |
| Unspecified ages (empty) | 32.93% (2795) | 1.08% (1267) | 0.25% (7) | 0.08% (1) |
| 1–9 y.o. | 1.35% (115) | 0.06% (76) | 0% (0) | 0% (0) |
| 10–19 y.o. | 1.93% (164) | 0.16% (185) | 1.22% (2) | 0.54% (1) |
| 20–29 y.o. | 3.13% (266) | 1.44% (1691) | 0.75% (2) | 0% (0) |
| 30–39 y.o. | 5.9% (501) | 5.54% (6508) | 1.4% (7) | 0.02% (1) |
| 40–49 y.o. | 8.14% (691) | 15.95% (18,729) | 1.01% (7) | 0.02% (3) |
| 50–59 y.o. | 12.13% (1030) | 32.08% (37,669) | 1.55% (16) | 0.02% (6) |
| 60–69 y.o. | 12.45% (1057) | 29.94% (35,165) | 1.23% (13) | 0% (1) |
| ≥70 y.o. | 20.59% (1748) | 13.67% (16,048) | 0.46% (8) | 0.02% (4) |
| PPI Monotherapy | H2RA Monotherapy | PPI Depression | H2RA Depression | |
|---|---|---|---|---|
| Total reports | 100% (8488) | 100% (117,435) | 0.61% (52) | 0.01% (17) |
| United States | 48.94% (4154) | 99.36% (116,683) | 0.7% (29) | 0.01% (16) |
| France | 9.57% (812) | 0.02% (18) | 1.63% (11) | 0% (0) |
| United Kingdom | 7.95% (675) | 0.06% (73) | 1.19% (8) | 0% (0) |
| Japan | 5.6% (475) | 0.24% (286) | 0.21% (1) | 0% (0) |
| Italy | 4.38% (372) | 0.06% (66) | 0.81% (3) | 0% (0) |
| Canada | 3.05% (259) | 0.04% (52) | 0.77% (2) | 0% (0) |
| Germany | 2.69% (228) | 0.02% (21) | 0.88% (2) | 0% (0) |
| Spain | 2.52% (214) | 0.02% (25) | 0% (0) | 0% (0) |
| Turkey | 1.73% (147) | 0% (1) | 0% (0) | 0% (0) |
| Brazil | 1.72% (146) | 0.01% (10) | 0.68% (1) | 0% (0) |
| Other countries | 11.31% (960) | 0.16% (192) | 0.1% (5) | 0.52% (1) |
| Adverse Event | n (%) |
|---|---|
| Vitamin B12 increased | 1 (0.01) |
| Vitamin B12 abnormal | 2 (0.02) |
| Anemia vitamin B12 deficiency | 13 (0.15) |
| Vitamin B12 decreased | 8 (0.09) |
| Vitamin B12 deficiency | 35 (0.41) |
| Adverse Event | n (%) |
|---|---|
| Blood magnesium increased | 1 (0.01) |
| Magnesium deficiency | 2 (0.02) |
| Blood magnesium decreased | 33 (0.39) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makunts, T.; Joulfayan, H.; Ta, K.; Abagyan, R. Depression Events Associated with Proton-Pump Inhibitors in Postmarketing Drug Surveillance Data. Pharmacoepidemiology 2023, 2, 272-282. https://doi.org/10.3390/pharma2030023
Makunts T, Joulfayan H, Ta K, Abagyan R. Depression Events Associated with Proton-Pump Inhibitors in Postmarketing Drug Surveillance Data. Pharmacoepidemiology. 2023; 2(3):272-282. https://doi.org/10.3390/pharma2030023
Chicago/Turabian StyleMakunts, Tigran, Haroutyun Joulfayan, Kenneth Ta, and Ruben Abagyan. 2023. "Depression Events Associated with Proton-Pump Inhibitors in Postmarketing Drug Surveillance Data" Pharmacoepidemiology 2, no. 3: 272-282. https://doi.org/10.3390/pharma2030023