
Spironolactone Utilization among Patients with Reduced and Preserved Ejection Fraction Heart Failure

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. HF Cohort Characteristics
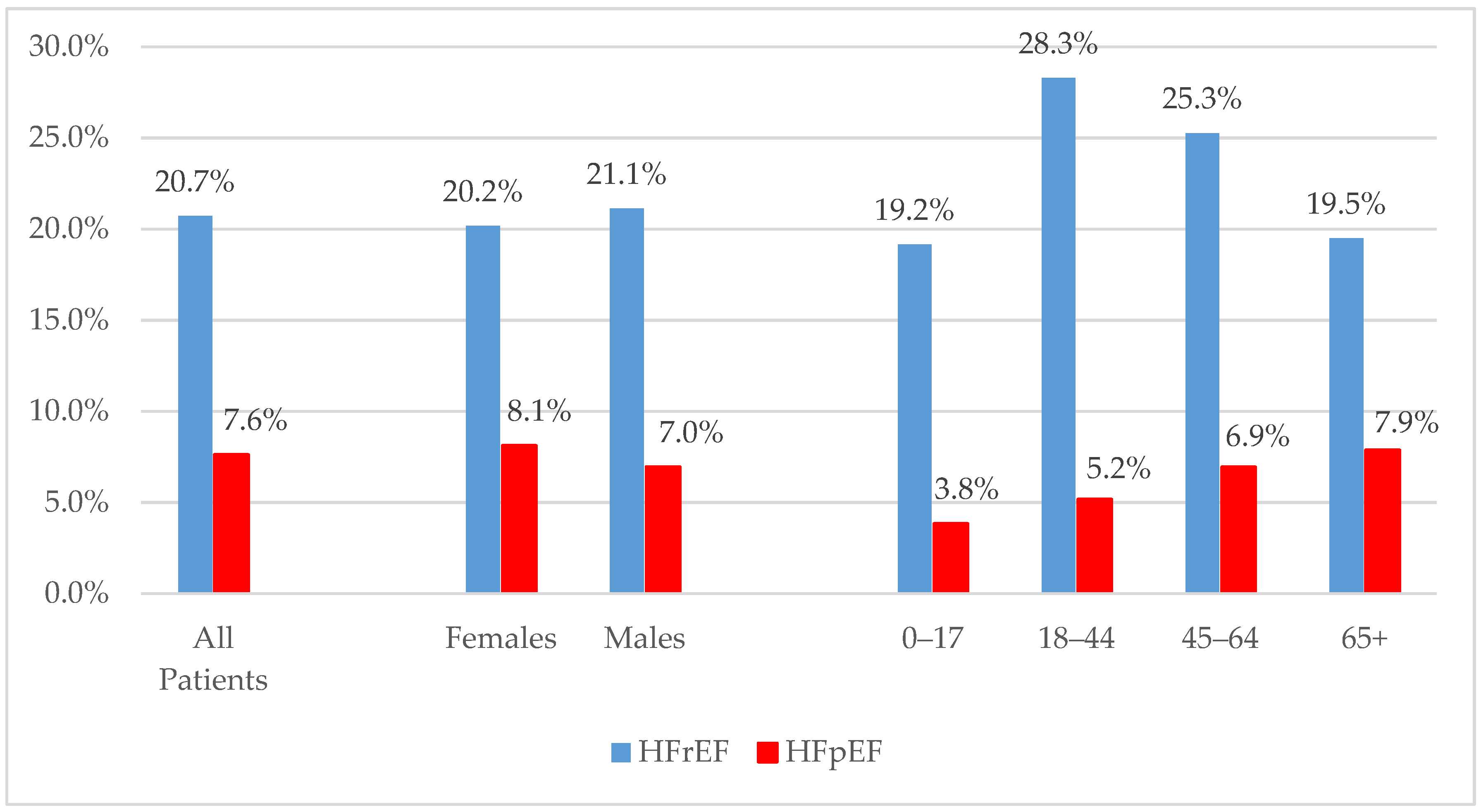
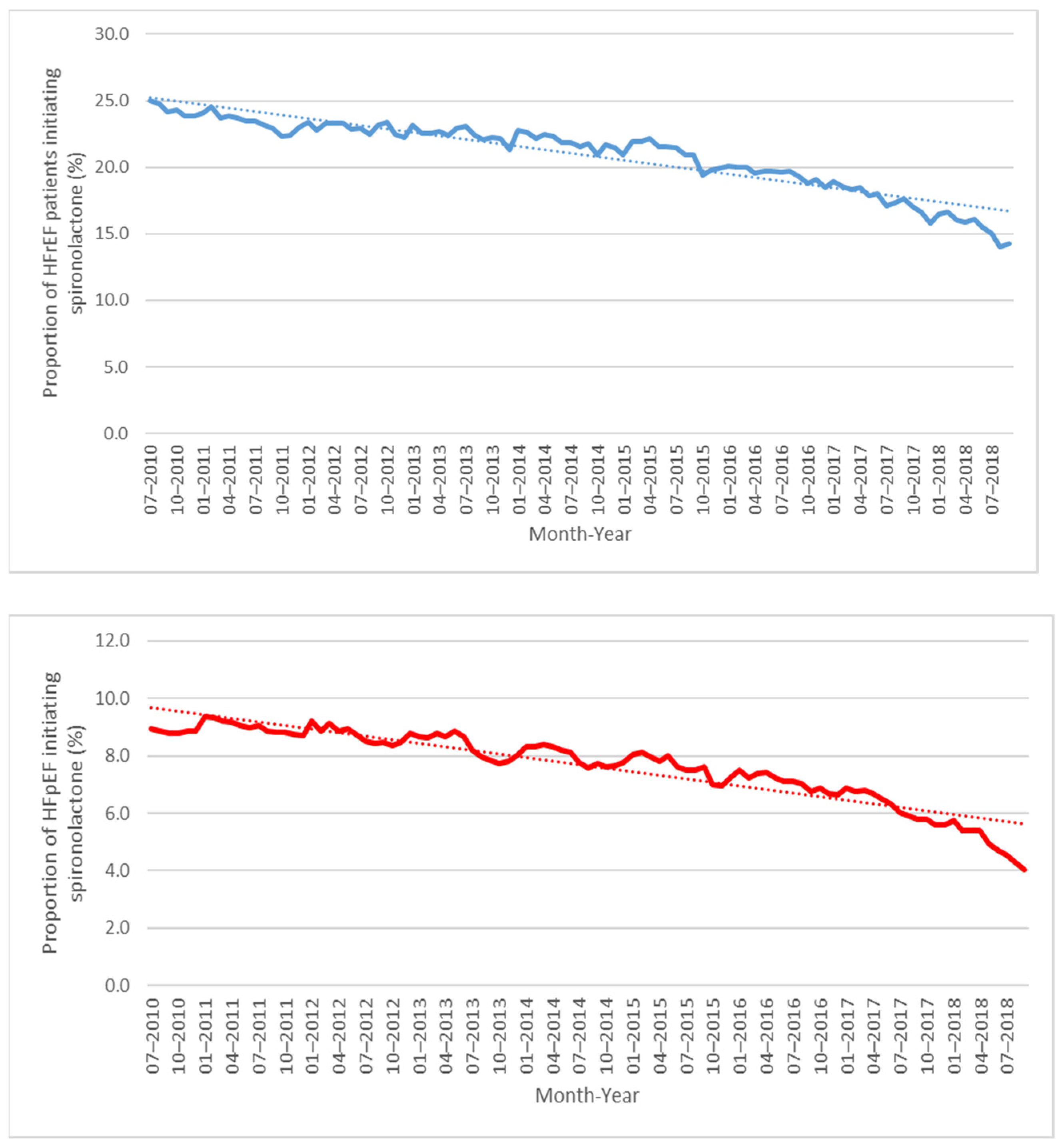
2.2. Spironolactone Use following HF Diagnosis
2.3. Time to Spironolactone Initiation following HF Diagnosis
2.4. Duration of Continuous Spironolactone Treatment following HF Diagnosis
2.5. Average Daily Dose of Spironolactone Treatment following HF Diagnosis
2.6. Sensitivity Analyses
3. Methods
3.1. Data Sources
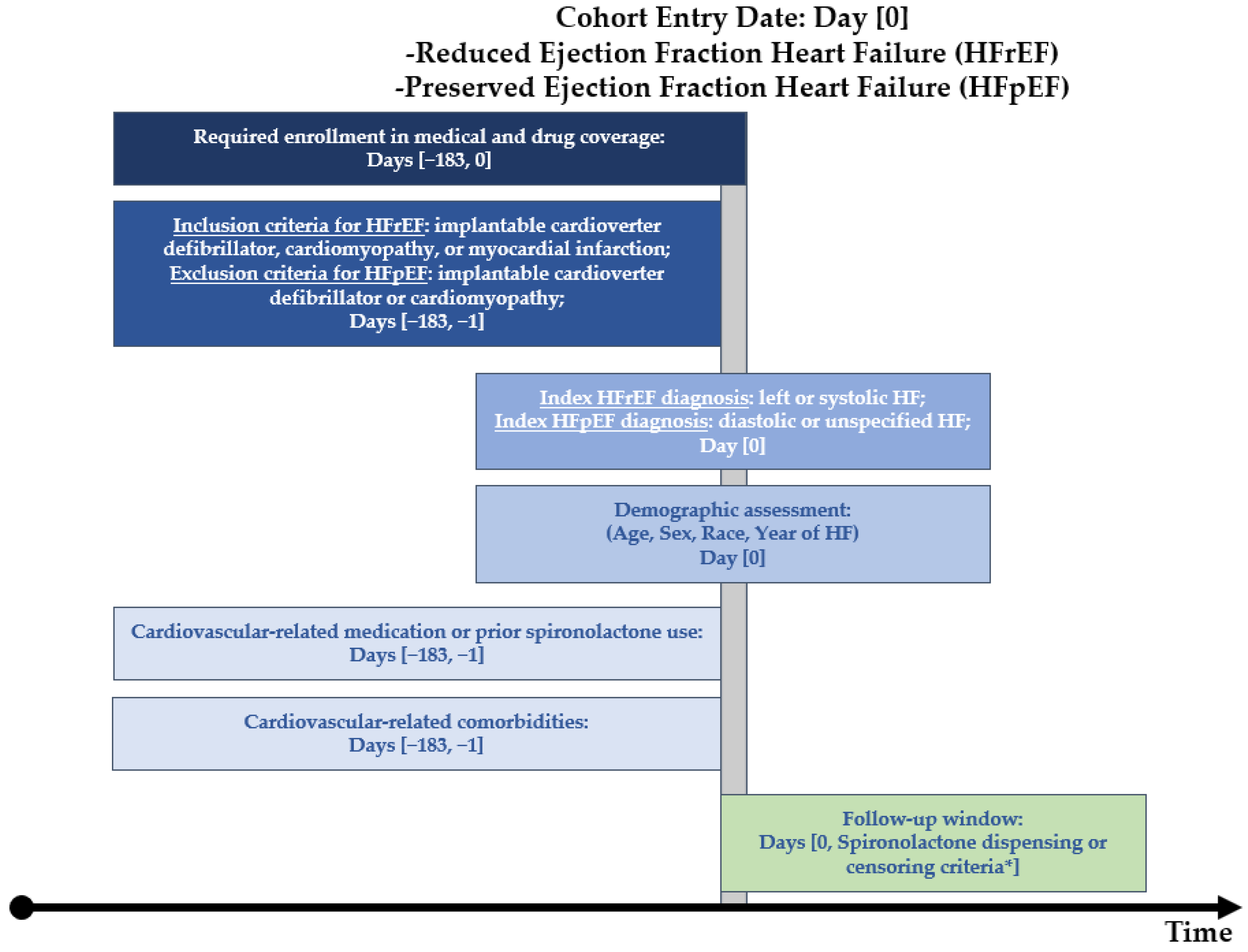
3.2. Cohort Definitions
3.3. Spironolactone Utilization
3.4. Descriptive Analyses
3.5. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Owan, T.E.; Hodge, D.O.; Herges, R.M.; Jacobsen, S.J.; Roger, V.L.; Redfield, M.M. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N. Engl. J. Med. 2006, 355, 251–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gladden, J.D.; Linke, W.A.; Redfield, M.M. Heart failure with preserved ejection fraction. Pflugers Arch. 2014, 466, 1037–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatia, R.S.; Tu, J.V.; Lee, D.S.; Austin, P.C.; Fang, J.; Haouzi, A.; Gong, Y.; Liu, P.P. Outcome of heart failure with preserved ejection fraction in a population-based study. N. Engl. J. Med. 2006, 355, 260–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitt, B.; Zannad, F.; Remme, W.J.; Cody, R.; Castaigne, A.; Perez, A.; Palensky, J.; Wittes, J. The Effect of Spironolactone on Morbidity and Mortality in Patients with Severe Heart Failure. Available online: https://www.nejm.org/doi/10.1056/NEJM199909023411001 (accessed on 12 May 2021).
- Pitt, B.; Remme, W.; Zannad, F.; Neaton, J.; Martinez, F.; Roniker, B.; Bittman, R.; Hurley, S.; Kleiman, J.; Gatlin, M.; et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N. Engl. J. Med. 2003, 348, 1309–1321. [Google Scholar] [CrossRef] [PubMed]
- Albert, N.M. Use of Aldosterone Antagonists in Heart Failure. JAMA 2009, 302, 1658. [Google Scholar] [CrossRef] [Green Version]
- Mottram, P.M.; Haluska, B.; Leano, R.; Cowley, D.; Stowasser, M.; Marwick, T.H. Effect of aldosterone antagonism on myocardial dysfunction in hypertensive patients with diastolic heart failure. Circulation 2004, 110, 558–565. [Google Scholar] [CrossRef] [Green Version]
- Edelmann, F.; Wachter, R.; Schmidt, A.G.; Kraigher-Krainer, E.; Colantonio, C.; Kamke, W.; Duvinage, A.; Stahrenberg, R.; Durstewitz, K.; Löffler, M.; et al. Effect of spironolactone on diastolic function and exercise capacity in patients with heart failure with preserved ejection fraction: The Aldo-DHF randomized controlled trial. JAMA 2013, 309, 781–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitt, B.; Pfeffer, M.A.; Assmann, S.F.; Boineau, R.; Anand, I.S.; Claggett, B.; Clausell, N.; Desai, A.S.; Diaz, R.; Fleg, J.L.; et al. Spironolactone for Heart Failure with Preserved Ejection Fraction. N. Engl. J. Med. 2014, 370, 1383–1392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, K.; Kass, D.A. Heart failure with preserved ejection fraction: Mechanisms, clinical features, and therapies. Circ. Res. 2014, 115, 79–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation 2017, 136, e137–e161. [Google Scholar] [CrossRef] [PubMed]
- Ball, R.; Robb, M.; Anderson, S.A.; Pan, G.D. The FDA’s sentinel initiative—A comprehensive approach to medical product surveillance. Clin. Pharmacol. Ther. 2016, 99, 265–268. [Google Scholar] [CrossRef]
- Curtis, L.H.; Weiner, M.G.; Boudreau, D.M.; Cooper, W.O.; Daniel, G.W.; Nair, V.P.; Raebel, M.A.; Beaulieu, N.U.; Rosofsky, R.; Woodworth, T.S.; et al. Design considerations, architecture, and use of the Mini-Sentinel distributed data system. Pharmacoepidemiol. Drug Saf. 2012, 21, 23–31. [Google Scholar] [CrossRef] [PubMed]
- McGraw, D.; Rosati, K.; Evans, B. A policy framework for public health uses of electronic health data. Pharmacoepidemiol. Drug Saf. 2012, 21, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Desai, R.J.; Lin, K.J.; Patorno, E.; Barberio, J.; Lee, M.; Levin, R.; Evers, T.; Wang, S.V.; Schneeweiss, S. Development and Preliminary Validation of a Medicare Claims-Based Model to Predict Left Ventricular Ejection Fraction Class in Patients With Heart Failure. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004700. [Google Scholar] [CrossRef] [PubMed]
- Browse Analytic Development/qrp—Sentinel Version Control System. Available online: https://dev.sentinelsystem.org/projects/AD/repos/qrp/browse (accessed on 21 September 2022).
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 62, e147–e239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dev, S.; Hoffman, T.K.; Kavalieratos, D.; Heidenreich, P.; Wu, W.; Schwenke, D.C.; Tracy, S.J. Barriers to Adoption of Mineralocorticoid Receptor Antagonists in Patients With Heart Failure: A Mixed-Methods Study. J. Am. Heart Assoc. 2016, 5, e002493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anand, I.S.; Claggett, B.; Liu, J.; Shah, A.M.; Rector, T.S.; Shah, S.J.; Desai, A.S.; O’Meara, E.; Fleg, J.L.; Pfeffer, M.A.; et al. Interaction Between Spironolactone and Natriuretic Peptides in Patients With Heart Failure and Preserved Ejection Fraction: From the TOPCAT Trial. JACC Heart Fail. 2017, 5, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wang, H.; Lu, Y.; Huang, X.; Liao, Y.; Bin, J. Effects of mineralocorticoid receptor antagonists in patients with preserved ejection fraction: A meta-analysis of randomized clinical trials. BMC Med. 2015, 13, 10. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| HFrEF | HFpEF | |
| Characteristic 1 | %/Std Dev 2 | %/Std Dev 2 |
| Number of unique patients | 2,009,529 | 9,257,514 |
| Demographics | ||
| Mean Age | 73.8 ± 12.1 | 73.0 ± 12.1 |
| Age: 0–17 | <0.1 | <0.1 |
| Age: 18–44 | 2.4 | 3.0 |
| Age: 45–64 | 17.7 | 18.2 |
| Age: 65+ | 79.9 | 78.8 |
| Gender (Female) | 42.2 | 57.3 |
| Gender (Male) | 57.8 | 42.7 |
| Race (American Indian or Alaska Native) | 0.5 | 0.4 |
| Race (Asian) | 1.5 | 2.3 |
| Race (Black or African American) | 13.5 | 12.5 |
| Race (Native Hawaiian or Other Pacific Islander) | 0.1 | 0.1 |
| Race 3 (Unknown) | 12.6 | 17.5 |
| Race (White) | 71.7 | 67.2 |
| Hispanic Origin | 2.3 | 2.9 |
| Recorded on heart failure index diagnosis: | ||
| Diastolic heart failure | -- | 33.7 |
| Left heart failure | 12.2 | -- |
| Systolic heart failure | 87.8 | -- |
| Unspecified heart failure | 11.0 | 71.6 |
| Spironolactone use in the prior 183 days: | ||
| Spironolactone dispensing | 5.7 | 1.4 |
| History of cardiovascular-related medication use in the prior 183 days: | ||
| Angiotensin-converting enzyme inhibitors | 43.0 | 33.7 |
| Angiotensin II receptor blockers | 21.1 | 23.6 |
| Antiarrhythmics | 12.8 | 4.9 |
| Beta blockers | 71.3 | 48.8 |
| Digoxin | 12.0 | 4.0 |
| Hydralazine | 7.5 | 4.2 |
| Loop diuretics | 53.9 | 27.9 |
| Mineralocorticoid receptor antagonists (eplerenone) | 0.8 | 0.1 |
| Nitrates | 20.9 | 10.0 |
| Potassium-sparing diuretics | 9.7 | 4.8 |
| Thiazide diuretics | 16.4 | 25.6 |
| History of heart failure related comorbidities in the prior 183 days: | ||
| Anemia | 45.9 | 30.4 |
| Atrial fibrillation or flutter | 47.0 | 20.9 |
| Cardiomyopathy | 66.7 | 0.0 |
| Chronic obstructive pulmonary disease | 36.1 | 21.6 |
| Coronary artery bypass graft | 2.7 | 0.5 |
| Depression | 20.5 | 16.6 |
| Diabetes mellitus | 49.9 | 40.7 |
| Endocarditis | 2.0 | 0.7 |
| Heart transplant | 0.9 | 0.3 |
| Human immunodeficiency virus | 0.5 | 0.4 |
| Hyperkalemia | 12.0 | 4.5 |
| Hyperlipidemia | 72.6 | 61.6 |
| Hypertension | 88.7 | 81.8 |
| Hypertensive nephropathy | 32.5 | 13.7 |
| Hypotension | 18.1 | 5.9 |
| Implantable cardioverter defibrillator | 20.7 | 0.0 |
| Ischemic stroke or transient ischemic attack | 23.6 | 15.9 |
| Myocardial infarction | 34.7 | 3.6 |
| Nephropathy | 54.4 | 30.0 |
| Obesity | 20.5 | 15.9 |
| Other dysrhythmias | 48.4 | 19.0 |
| Psychosis | 8.3 | 6.2 |
| Pulmonary hypertension | 17.6 | 5.3 |
| Renal disorders | 40.4 | 21.4 |
| Rheumatic heart disease | 16.4 | 4.9 |
| Sleep apnea | 15.2 | 10.2 |
| Smoking | 15.3 | 8.3 |
| Stable angina | 12.0 | 5.7 |
| Unstable angina | 18.0 | 7.2 |
| Valve disorders | 20.7 | 7.8 |
| Time to First Spironolactone Dispensing Following HF Diagnosis (in Days) | ||
|---|---|---|
| HFrEF | HFpEF | |
| Mean | 307 | 565 |
| Median | 90 (IQR: 19–385) | 286 (IQR: 57–851) |
| <1 month (%) | 30.8 | 17.4 |
| 1–<6 months | 31.4 | 24.5 |
| 6 months–<1 year (%) | 11.9 | 13.0 |
| 1–<2 years (%) | 11.9 | 16.3 |
| 2–<3 years (%) | 6.2 | 10.2 |
| 3+ years (%) | 7.8 | 18.7 |
| First Continuous Treatment Episode (in Days) of Spironolactone Dispensing | ||
| HFrEF | HFpEF | |
| Mean | 262 | 250 |
| Median | 120 (IQR: 44–321) | 114 (IQR: 32–301) |
| <1 month (%) | 5.6 | 6.4 |
| 1–<3 months (%) | 39.6 | 40.2 |
| 3–<6 months (%) | 16.1 | 16.1 |
| 6 months–<1 year (%) | 16.8 | 16.5 |
| 1+ years (%) | 22.0 | 20.7 |
| Average Daily Dose * (mg per Day) in the First Continuous Treatment Episode of Spironolactone | ||
| HFrEF | HFpEF | |
| Mean | 28 | 34 |
| Median | 25 (IQR: 25–25) | 25 (25–45) |
| <15 mg/day (%) | 18.1 | 11.3 |
| 15–<30 mg/day (%) | 64.5 | 59.3 |
| 30–<45 mg/day (%) | 3.4 | 4.3 |
| 45–<75 mg/day (%) | 11.4 | 18.7 |
| 75–<100 mg/day (%) | 0.7 | 1.5 |
| 100+ mg/day (%) | 1.9 | 4.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eworuke, E.; Cosgrove, A.; Her, Q.L.; Lyons, J.G.; Martin, D.; Adimadhyam, S. Spironolactone Utilization among Patients with Reduced and Preserved Ejection Fraction Heart Failure. Pharmacoepidemiology 2022, 1, 89-100. https://doi.org/10.3390/pharma1030009
Eworuke E, Cosgrove A, Her QL, Lyons JG, Martin D, Adimadhyam S. Spironolactone Utilization among Patients with Reduced and Preserved Ejection Fraction Heart Failure. Pharmacoepidemiology. 2022; 1(3):89-100. https://doi.org/10.3390/pharma1030009
Chicago/Turabian StyleEworuke, Efe, Austin Cosgrove, Qoua Liang Her, Jennifer G. Lyons, Dave Martin, and Sruthi Adimadhyam. 2022. "Spironolactone Utilization among Patients with Reduced and Preserved Ejection Fraction Heart Failure" Pharmacoepidemiology 1, no. 3: 89-100. https://doi.org/10.3390/pharma1030009