
Metacognition through an Iterative Anatomy AI Chatbot: An Innovative Playing Field for Educating the Future Generation of Medical Students

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Medical Education and the Gen Z Student Population
3. Incorporation of Digital Technology into Medical Education
4. Artificial Intelligence and Metacognition
4.1. Artifical Intellengence
4.2. Metacognition in Medical Education
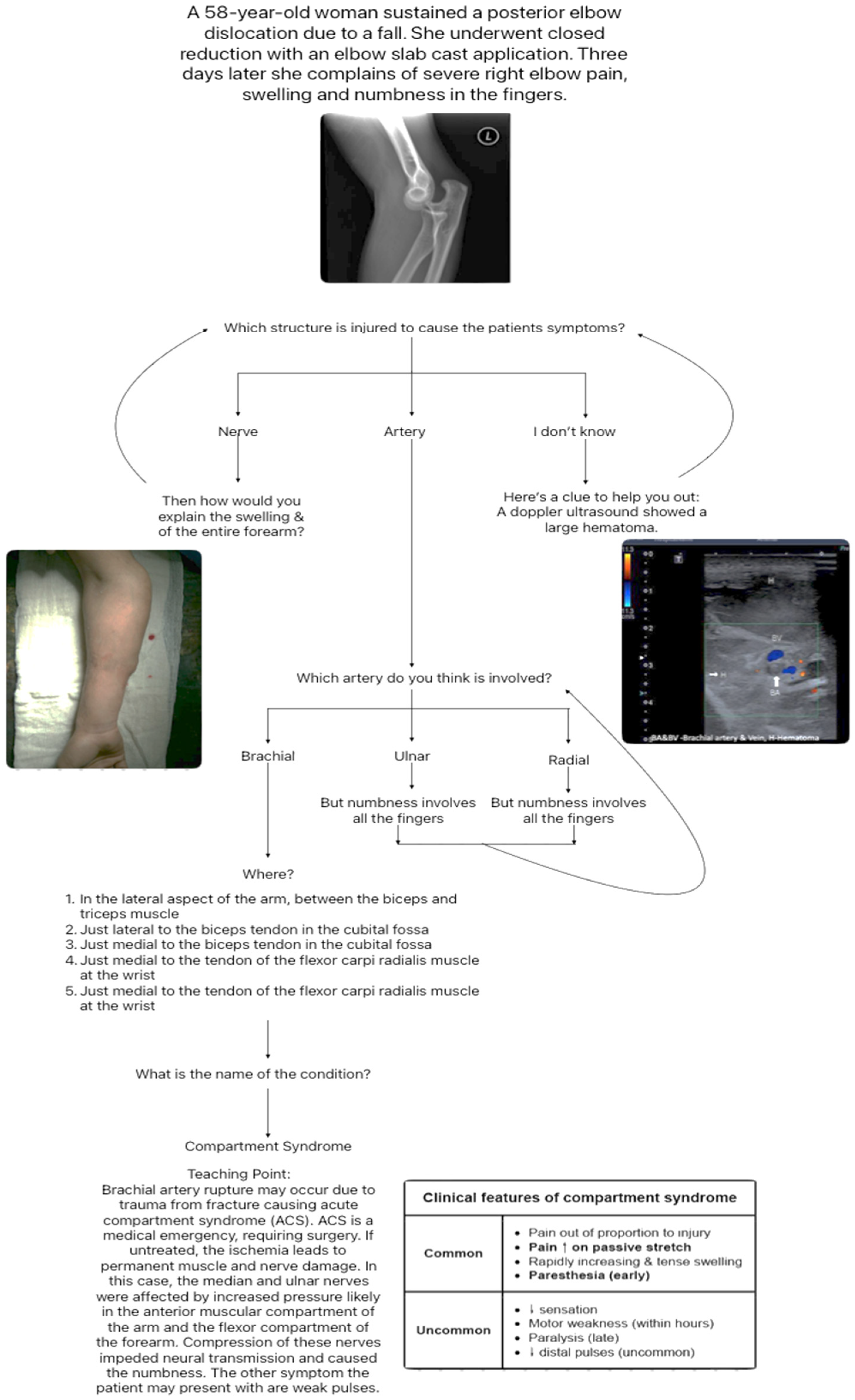
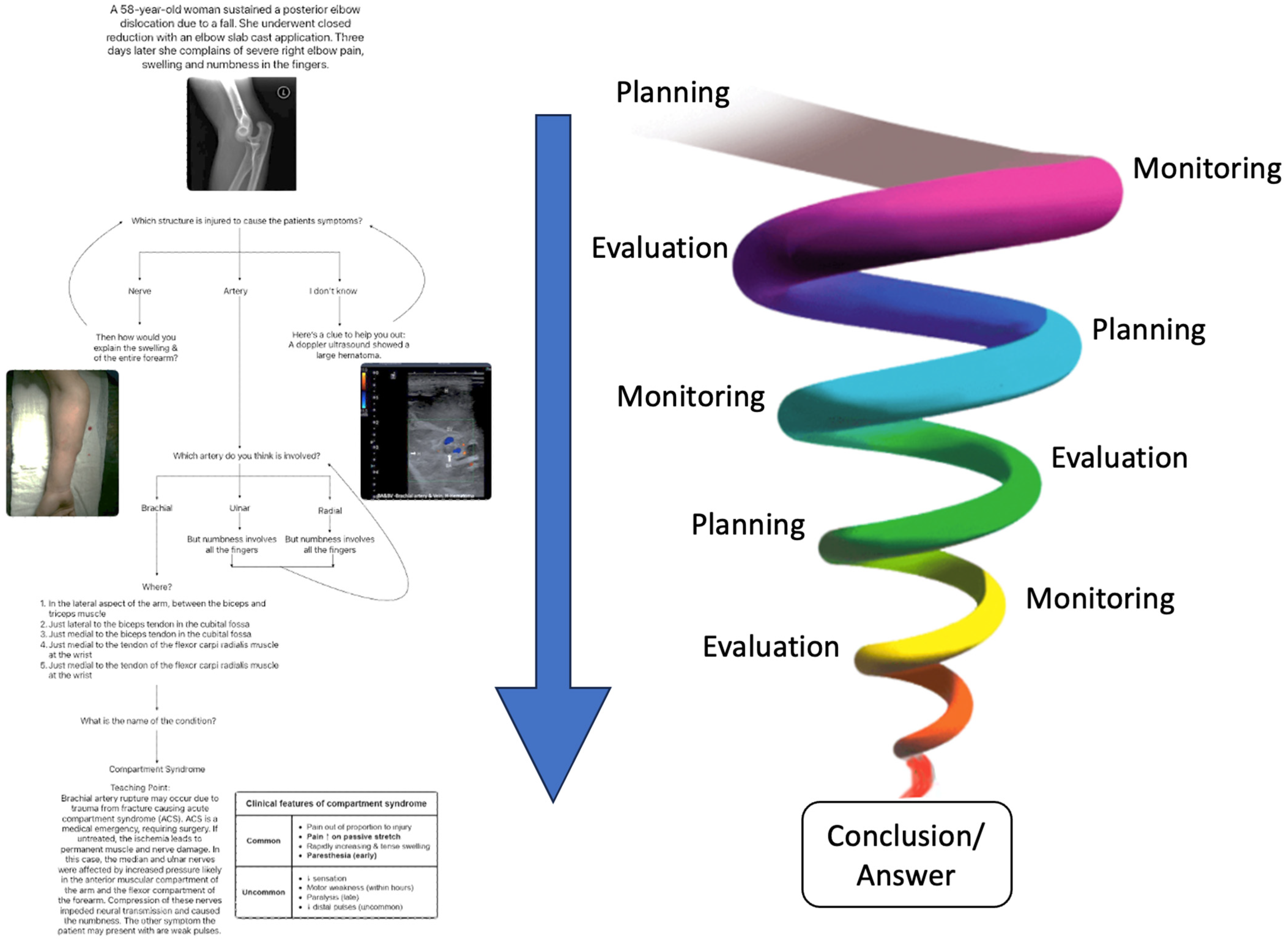
4.3. AI Case Example Using Metacognition
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Inuwa, I.M.; Tanranikanti, V.; Al-Rawahy, M.; Roychoudhry, S.; Habbal, O. “Between a Rock and a Hard Place” The discordant views among medical teachers about anatomy content in the undergraduate medical curriculum. Sultan Qaboos Univ. Med. J. 2012, 12, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Porzionato, A.; Macchi, V.; Stecco, C.; Boscolo-Berto, R.; Loukas, M.; Tubbs, R.S.; De Caro, R. Clinical Anatomy and Medical Malpractice-A Narrative Review with Methodological Implications. Healthcare 2022, 10, 1915. [Google Scholar] [CrossRef]
- Feyzi-Behnagh, R.; Azevedo, R.; Legowski, E.; Reitmeyer, K.; Tseytlin, E.; Crowley, R.S. Metacognitive Scaffolds Improve Self-Judgments of Accuracy in a Medical Intelligent Tutoring System. Instr. Sci. 2014, 42, 159–181. [Google Scholar] [CrossRef]
- Leeds, F.S.; Atwa, K.M.; Cook, A.M.; Conway, K.A.; Crawford, T.N. Teaching heuristics and mnemonics to improve generation of differential diagnoses. Med. Educ. Online 2020, 25, 1742967. [Google Scholar] [CrossRef] [PubMed]
- Zheng, B. Medical Students’ Technology Use for Self-Directed Learning: Contributing and Constraining Factors. Med. Sci. Educ. 2022, 32, 149–156. [Google Scholar] [CrossRef]
- Mukhalalati, B.A.; Taylor, A. Adult Learning Theories in Context: A Quick Guide for Healthcare Professional Educators. J. Med. Educ. Curric. Dev. 2019, 6, 2382120519840332. [Google Scholar] [CrossRef]
- Hong, W.H.; Vadivelu, J.; Daniel, E.G.; Sim, J.H. Thinking about thinking: Changes in first-year medical students’ metacognition and its relation to performance. Med. Educ. Online 2015, 20, 27561. [Google Scholar] [CrossRef] [PubMed]
- Khaine, A.A.; Adefuye, A.O.; Busari, J. Utility of Concept Mapping as a Tool to Enhance Metacognitive Teaching and learning of complex concepts in undergraduate medical education. Arch. Med. Health Sci. 2019, 7, 267–272. [Google Scholar]
- Versteeg, M.; Bressers, G.; Wijnen-Meijer, M.; Ommering, B.W.C.; de Beaufort, A.J.; Steendijk, P. What Were You Thinking? Medical Students’ Metacognition and Perceptions of Self-Regulated Learning. Teach. Learn. Med. 2021, 33, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Chytas, D.; Mitrousias, V.; Raoulis, V.; Banios, K.; Fyllos, A.; Zibis, A.H. A Review of the Outcomes of the Implementation of Case-Based Anatomy Learning. Cureus 2021, 13, e19179. [Google Scholar] [CrossRef] [PubMed]
- Burgess, A.; Bleasel, J.; Haq, I.; Roberts, C.; Garsia, R.; Robertson, T.; Mellis, C. Team-based learning (TBL) in the medical curriculum: Better than PBL? BMC Med. Educ. 2017, 17, 243. [Google Scholar] [CrossRef] [PubMed]
- Burgess, A.; Matar, E.; Roberts, C.; Haq, I.; Wynter, L.; Singer, J.; Kalman, E.; Bleasel, J. Scaffolding medical student knowledge and skills: Team-based learning (TBL) and case-based learning (CBL). BMC Med. Educ. 2021, 21, 238. [Google Scholar] [CrossRef] [PubMed]
- Stentoft, D. Problem-based projects in medical education: Extending PBL practices and broadening learning perspectives. Adv. Health Sci. Educ. Theory Pract. 2019, 24, 959–969. [Google Scholar] [CrossRef] [PubMed]
- Thistlethwaite, J.E.; Davies, D.; Ekeocha, S.; Kidd, J.M.; MacDougall, C.; Matthews, P.; Purkis, J.; Clay, D. The effectiveness of case-based learning in health professional education. A BEME systematic review: BEME Guide No. 23. Med. Teach. 2012, 34, e421–e444. [Google Scholar] [CrossRef]
- Colbert, C.Y.; Graham, L.; West, C.; White, B.A.; Arroliga, A.C.; Myers, J.D.; Ogden, P.E.; Archer, J.; Mohammad, Z.T.; Clark, J. Teaching metacognitive skills: Helping your physician trainees in the quest to ‘know what they don’t know’. Am. J. Med. 2015, 128, 318–324. [Google Scholar] [CrossRef]
- Naug, H.L.; Colson, N.J.; Donner, D.G. Promoting metacognition in first year anatomy laboratories using plasticine modeling and drawing activities: A pilot study of the “blank page” technique. Anat. Sci. Educ. 2011, 4, 231–234. [Google Scholar] [CrossRef]
- Versteeg, M.; Steendijk, P. Putting post-decision wagering to the test: A measure of self-perceived knowledge in basic sciences? Perspect. Med. Educ. 2019, 8, 9–16. [Google Scholar] [CrossRef]
- Lazaros, E.J.; Davidson, C.J. Increasing Student Retention in STEM. Acad. Exch. Q. 2014, 18, 119–124. [Google Scholar]
- Wells, T.; Fishman, E.K.; Horton, K.M.; Rowe, S.P. Meet Generation Z. Top 10 Trends of 2018. J. Am. Coll. Radiol. 2018, 15, 1791–1793. [Google Scholar] [CrossRef]
- Attardi, S.M.; Taylor, T.A.H.; Lerchenfeldt, S.; Pratt, R.L.; Sawarynski, K.E. Adapting Strategically to Changing Times in Health Professions Education: A Generational Workshop for Educators. MedEdPORTAL 2021, 17, 11084. [Google Scholar] [CrossRef]
- Taranikanti, V. Is COVID Era the Beginning of a Paradigm Shift in Anatomy Education? Med. Health 2020, 15, 1–2. [Google Scholar] [CrossRef]
- Yeh, D.D.; Park, Y.S. Improving Learning Efficiency of Factual Knowledge in Medical Education. J. Surg. Educ. 2015, 72, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Donkin, R.; Rasmussen, R. Student Perception and the Effectiveness of Kahoot!: A Scoping Review in Histology, Anatomy, and Medical Education. Anat. Sci. Educ. 2021, 14, 572–585. [Google Scholar] [CrossRef]
- Pereira, J.A.; Pleguezuelos, E.; Meri, A.; Molina-Ros, A.; Molina-Tomas, M.C.; Masdeu, C. Effectiveness of using blended learning strategies for teaching and learning human anatomy. Med. Educ. 2007, 41, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Lio, J.; Sherer, R.; Jiang, I. Some Learning Theories for Medical Educators. Med. Sci. Educ. 2021, 31, 1157–1172. [Google Scholar] [CrossRef]
- Gooding, H.C.; Mann, K.; Armstrong, E. Twelve tips for applying the science of learning to health professions education. Med. Teach. 2017, 39, 26–31. [Google Scholar] [CrossRef]
- Khodaei, S.; Hasanvand, S.; Gholami, M.; Mokhayeri, Y.; Amini, M. The effect of the online flipped classroom on self-directed learning readiness and metacognitive awareness in nursing students during the COVID-19 pandemic. BMC Nurs. 2022, 21, 22. [Google Scholar] [CrossRef]
- Lazaros, E.J.; Davidson, C.J. Asynchronous online classrooms: Success for student and teacher. Acad. Exch. Q. 2014, 18, 31. [Google Scholar]
- Gonullu, I.; Artar, M. Metacognition in medical education. Educ. Health 2014, 27, 225–226. [Google Scholar] [CrossRef]
- Rhodes, M.G. Metacognition. Teach. Psychol. 2019, 46, 168–175. [Google Scholar] [CrossRef]
- Siqueira, M.A.M.; Goncalves, J.P.; Mendonca, V.S.; Kobayasi, R.; Arantes-Costa, F.M.; Tempski, P.Z.; Martins, M.A. Relationship between metacognitive awareness and motivation to learn in medical students. BMC Med. Educ. 2020, 20, 393. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.A. Exam Wrappers: It Is Time to Adopt a Nursing Student Metacognitive Tool for Exam Review. Nurs. Educ. Perspect. 2021, 42, 51–52. [Google Scholar] [CrossRef] [PubMed]
- Hayat, A.A.; Shateri, K. The Role of Academic Self-Efficacy in Improving Students’ Metacognitive Learning Strategies. J. Adv. Med. Educ. Prof. 2019, 7, 205–212. [Google Scholar] [PubMed]
- Rahmani, M. Medical Trainees and the Dunning-Kruger Effect: When They Don’t Know What They Don’t Know. J. Grad. Med. Educ. 2020, 12, 532–534. [Google Scholar] [CrossRef] [PubMed]
- Iskander, M. Burnout, Cognitive Overload, and Metacognition in Medicine. Med. Sci. Educ. 2019, 29, 325–328. [Google Scholar] [CrossRef]
- Burke, H.; Mancuso, L. Social cognitive theory, metacognition, and simulation learning in nursing education. J. Nurs. Educ. 2012, 51, 543–548. [Google Scholar] [CrossRef]
- Wesiak, G.; Steiner, C.M.; Moore, A.; Dagger, D.; Power, G.; Berthold, M.; Albert, D.; Conlan, O. Iterative augmentation of a medical training simulator: Effects of affective metacognitive scaffolding. Comput. Educ. 2014, 76, 13–29. [Google Scholar] [CrossRef]
- Cleary, T.J.; Konopasky, A.; La Rochelle, J.S.; Neubauer, B.E.; Durning, S.J.; Artino, A.R., Jr. First-year medical students’ calibration bias and accuracy across clinical reasoning activities. Adv. Health Sci. Educ. Theory Pract. 2019, 24, 767–781. [Google Scholar] [CrossRef]
- Artino, A.R.; Dong, T., Jr.; DeZee, K.J.; Gilliland, W.R.; Waechter, D.M.; Cruess, D.; Durning, S.J. Achievement goal structures and self-regulated learning: Relationships and changes in medical school. Acad. Med. 2012, 87, 1375–1381. [Google Scholar] [CrossRef]
- Gude, T.; Finset, A.; Anvik, T.; Baerheim, A.; Fasmer, O.B.; Grimstad, H.; Vaglum, P. Do medical students and young physicians assess reliably their self-efficacy regarding communication skills? A prospective study from end of medical school until end of internship. BMC Med. Educ. 2017, 17, 107. [Google Scholar] [CrossRef]
- Madrazo, L.; Lee, C.B.; McConnell, M.; Khamisa, K. Self-assessment differences between genders in a low-stakes objective structured clinical examination (OSCE). BMC Res. Notes 2018, 11, 393. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Yasmeen, R. Practice to preach self-regulation: Use of metacognitive strategies by medical teachers in their learning practices. Pak. J. Med. Sci. 2019, 35, 1642–1646. [Google Scholar] [PubMed]
- Hayat, A.A.; Shateri, K.; Amini, M.; Shokrpour, N. Relationships between academic self-efficacy, learning-related emotions, and metacognitive learning strategies with academic performance in medical students: A structural equation model. BMC Med. Educ. 2020, 20, 76. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.; Ji, C. The correlation of metacognitive ability, self-directed learning ability and critical thinking in nursing students: A cross-sectional study. Nurs. Open 2021, 8, 936–945. [Google Scholar] [CrossRef] [PubMed]
- Kosior, K.; Wall, T.; Ferrero, S. The role of metacognition in teaching clinical reasoning: Theory to practice. Educ. Health Prof. 2019, 2, 108–114. [Google Scholar]
- Zheng, B.; Chang, C.; Lin, C.H.; Zhang, Y. Self-Efficacy, Academic Motivation, and Self-Regulation: How Do They Predict Academic Achievement for Medical Students? Med. Sci. Educ. 2021, 31, 125–130. [Google Scholar] [CrossRef]
- Chew, K.S.; Durning, S.J.; van Merrienboer, J.J. Teaching metacognition in clinical decision-making using a novel mnemonic checklist: An exploratory study. Singap. Med. J. 2016, 57, 694–700. [Google Scholar] [CrossRef]
- Gholami, M.; Moghadam, P.K.; Mohammadipoor, F.; Tarahi, M.J.; Sak, M.; Toulabi, T.; Pour, A.H. Comparing the effects of problem-based learning and the traditional lecture method on critical thinking skills and metacognitive awareness in nursing students in a critical care nursing course. Nurse Educ. Today 2016, 45, 16–21. [Google Scholar] [CrossRef]
- Chang, C.; Colon-Berlingeri, M.; Mavis, B.; Laird-Fick, H.S.; Parker, C.; Solomon, D. Medical Student Progress Examination Performance and Its Relationship with Metacognition, Critical Thinking, and Self-Regulated Learning Strategies. Acad. Med. 2021, 96, 278–284. [Google Scholar] [CrossRef]
- Mahdavi, M. An Overview: Metacognition in Education. Int. J. Multidiciplin. Curr. Res. 2014, 2, 529–535. [Google Scholar]
- Robinson, P.M.; Griffiths, E.; Watts, A.C. Simple elbow dislocation. Shoulder Elb. 2017, 9, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Gedi Ibrahim, I.; Tahtabasi, M. Doppler ultrasound diagnosis of brachial artery injury due to blunt trauma: A Case Report. Radiol. Case Rep. 2020, 15, 1207–1210. [Google Scholar] [CrossRef] [PubMed]
- Suvashis, D.; Rahul, M.; Lukesh, P. A rare cause of open acute compartment syndrome of fore arm following stab injury. Trauma Emerg. Care 2018, 3. [Google Scholar] [CrossRef]
- Rivers, M.L. Metacognition About Practice Testing: A Review of Learners’ Beliefs, Monitoring, and Control of Test-Enhanced Learning. Educ. Psychol. Rev. 2020, 33, 823–862. [Google Scholar] [CrossRef]
- Davidson, C.J.; Lazaros, E.J. How to use cognitive psychology when testing. Acad. Exch. Q. 2014, 18, 66–71. [Google Scholar]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taranikanti, V.; Davidson, C.J. Metacognition through an Iterative Anatomy AI Chatbot: An Innovative Playing Field for Educating the Future Generation of Medical Students. Anatomia 2023, 2, 271-281. https://doi.org/10.3390/anatomia2030025
Taranikanti V, Davidson CJ. Metacognition through an Iterative Anatomy AI Chatbot: An Innovative Playing Field for Educating the Future Generation of Medical Students. Anatomia. 2023; 2(3):271-281. https://doi.org/10.3390/anatomia2030025
Chicago/Turabian StyleTaranikanti, Varna, and Cameron J. Davidson. 2023. "Metacognition through an Iterative Anatomy AI Chatbot: An Innovative Playing Field for Educating the Future Generation of Medical Students" Anatomia 2, no. 3: 271-281. https://doi.org/10.3390/anatomia2030025