1. Introduction
The alterations of the musculoskeletal system are one of the causes of greater medical consultation in the different levels of health care. Within these, shoulder pain occupies an important place [
1]. The deltoid is the muscle that forms the rounded contour of the shoulder. Anatomically, it seems to be made up of three different sets of fibers. Fick [
2] and Kapandji [
3] describe seven functional portions in the deltoid muscle according to their location in relation to the abduction axis. Electromyography (EMG) studies also suggest the presence of at least seven groups that can be independently coordinated by the central nervous system to better focus the movement of the respective motor units [
4,
5]. They have been established by Positron emission tomography (PET). These seven segments are divided by muscular tendons corresponding to the functional units of the deltoid [
6]. The three anatomical portions in which the deltoid muscle has been divided classically are the anterior (clavicular), the mean (acromial), and the posterior (spinal). However, the posterior fibers of the deltoid are usually represented by being inserted directly into the spine of the scapula. Moccia et al. [
7] observed how they are first fused with the fascia of the infraspinatus muscle, and the contraction force is transmitted to the spine of the scapula. They also found a transverse fascial band from the posterior deltoid muscle belly to the infraspinatus fascia near the lateral edge of the scapula (Deltofascial Bridge). This infraspinatus fascia may be involved in compartment syndromes.
The deltoid muscle is innervated by the axillary nerve, which is a lateral terminal bouquet of the posterior fascicle of the brachial plexus [
8,
9,
10,
11,
12].
In shoulder surgeries, the separation of the deltoids is common, and there is a high risk of injuring the axillary nerve causing a functional limitation of the shoulder [
13,
14]. Cetik et al. [
15] studied the safe area of a surgical approach to avoid damaging the axillary nerve as the incisions on the deltoid are very common in arthroscopies, humeral fractures or repair of the rotator cuff [
16,
17,
18,
19,
20]. Another surgical technique used in this area is the transfer of the spinal part of the deltoid to the long head of the brachial triceps muscle to improve the extension of the glenohumeral joint in subjects with radial nerve paralysis [
21,
22].
Different variations of the deltoid muscle have been described in the literature, such as its fusion with the pectoralis major or the presence of additional bands attached to the trapezium [
23]. A bilateral separation of the posterior deltoid fibers with their fascia was described by Kayikçioglu et al. [
24]. Kamburoğlu et al. [
25] and Sawant et al. [
26] described an accessory belly to the posterior deltoid. Fraser et al. [
27] found an accessory belly of the deltoid attached to the teres minor muscle.
While the deltoid variations are rare, degenerative and/or traumatic shoulder pathologies are very common. Clinically fasciocutaneous, musculocutaneous, or muscular deltoid and posterior deltoid flaps are especially used in tetraplegia (by a transfer to triceps) [
28], posterior shoulder instability [
29] and radionecrotic defects situated over the glenohumeral joint [
30]. In addition, patients with a symptomatic rotator cuff tear show compensatory movement patterns based on the abnormal activity of the biceps brachii and posterior deltoid muscles [
31]. Considering the clinical relevance, gross anatomy of the deltoid muscle and anatomical variants should be considered to improve success of management strategies and treatments to avoid injury.
Therefore, the analysis and knowledge of these anomalies is essential for surgeons and anatomists.
2. Materials and Methods
A total of 21 specimens (12 women and 9 men) were used with a 10% formaldehyde solution. All human cadavers used in the study were derived from donors who gave their written consent, premortem, to the use of their bodies for educational and scientific purposes. The donation process as well as the procurement and use of corpses, human remains and cadaveric remains for scientific and teaching purposes at the Rey Juan Carlos University, adhered to the appropriate regulation. These regulations were approved by the Governing Council of the Rey Juan Carlos University on 28 April 2009. All specimens were dissected bilaterally. Specimens presenting deformations, injuries and/or scars on the shoulder or arm were excluded.
The classical dissection methodology was used: careful removal of the skin and subcutaneous tissue from the arm and shoulder region, preserving the fascia. The acromial end of the clavicle was accepted as a boundary between the anterior and middle bellies of the deltoid. The reference point is called the acromial angle of the scapula [
23], which is distinguishable in all cases as a palpable lump to establish the boundary between the middle and posterior belly. At this stage, it was possible to identify the connections between the deltoid fascia and adjacent structures. The origin was then dissected to visualize the axillary nerve along the internal surface of the muscle. As the muscle was dissected, the fascial connections between the deltoid and the infraspinatus were observed. Then the neurovascular package was dissected in the quadrangular space.
3. Results
In all specimens, it was possible to identify the three portions of the deltoid: the clavicular (anterior), acromial (mean) and spinal (posterior) portion.
The muscle fibers of the anterior deltoid were identified in the lateral third of the clavicle and in the anterior part of the acromion. The fibers of the middle deltoid were identified in the lateral region of the acromion, and the posterior deltoids could be followed along the spine of the scapula.
The fibers of the three muscular bellies converged in all subjects and were inserted in the proximal region of the lateral side of the humerus (deltoid tuberosity). The anterior origin of the deltoid muscle was continued with the clavicular fibers of the major pectoral muscle. These fibers are closely related and are found separated exclusively by a small chiasmatic space (the deltopectoral groove) through which the cephalic vein is observed.
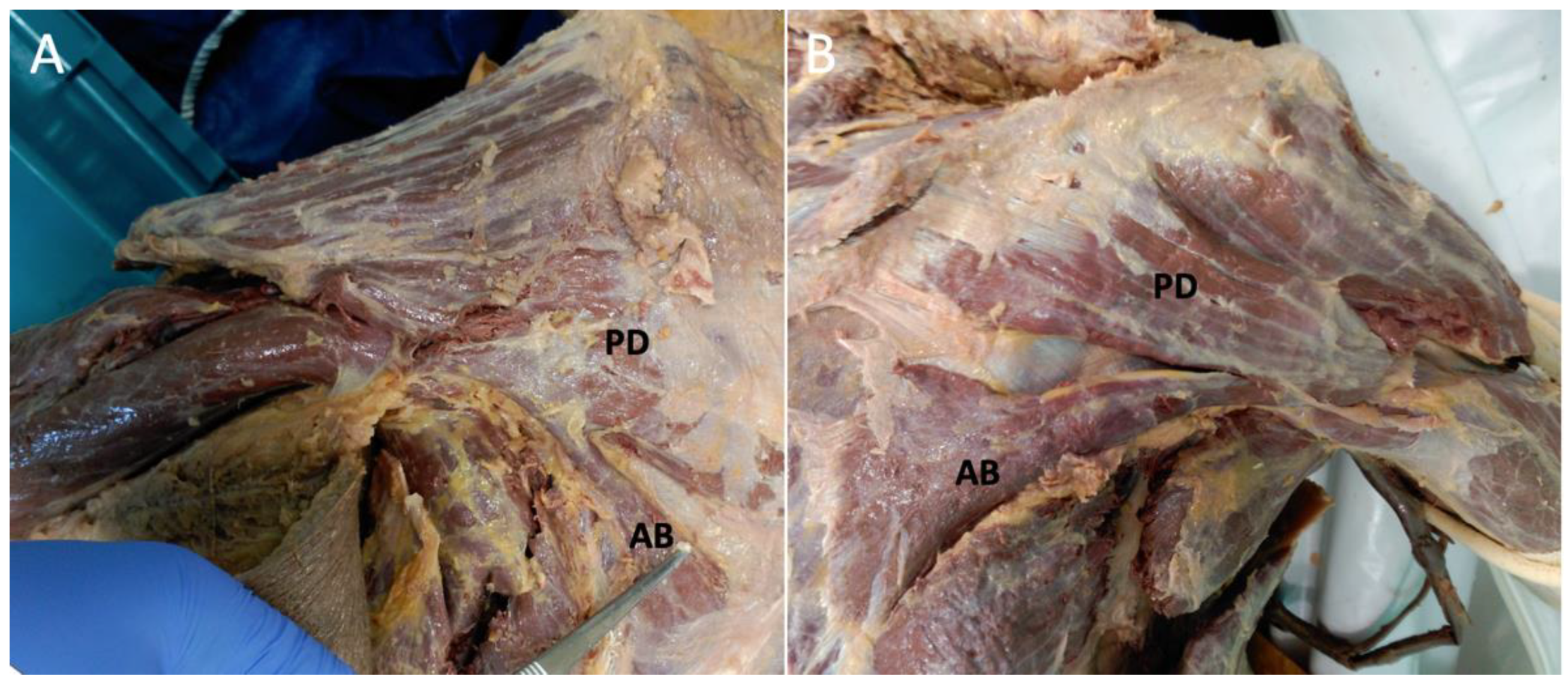
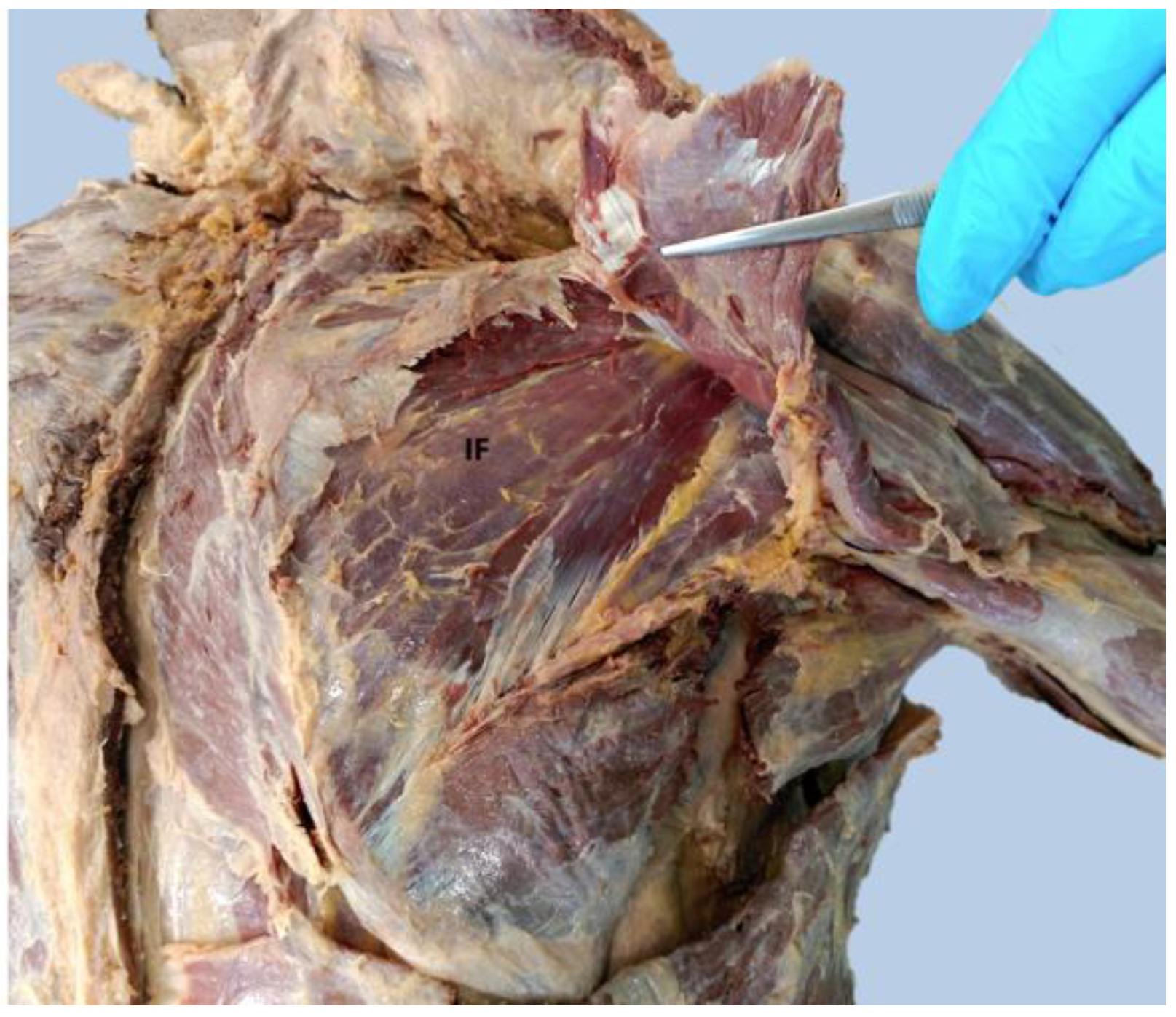
Only in one corpse, bilaterally, was found an additional belly of the deltoid muscle (
Figure 1). It was observed that this additional muscular belly was related to the fascial tissue of the deltoid muscle, and its muscle fibers take origin from the middle third of the inferomedial bands of infraspinatus fascia [
7] and attach to the posterior belly of the deltoid muscle (
Figure 2 and
Figure 3).
No abnormalities were found in terms of vascularization or innervation. The axillary nerve innervated the deltoid muscle and the additional belly. The axillar nerve is one of the terminal branches of the posterior cord of the brachial plexus and usually contains fibers from C5 and C6 ventral rami [
32]. The axillary nerve passes through the quadrilateral space from the anterior to posterior direction and splits into two branches (the anterior and the posterior branches) within the quadrilateral space. The anterior branch travels around the surgical neck of the humerus and supplies the middle and anterior portions of the deltoid.
Moreover, the sub-branches from the anterior branch supply the posterior portion. The posterior branch runs posteriorly and supplies the posterior portion of the deltoid [
11,
12]. Its blood supply was through the posterior circumflex humeral artery, which travels with the axillary nerve through the quadrilateral space. The posterior circumflex humeral artery supplies the deltoid’s middle and posterior portions. The thoracoacromial artery also supplies the deltoid muscle. The venous branches accompany the arterial branches, except the cephalic vein, which runs in the deltopectoral groove [
10].
4. Discussion
The deltoid is the only muscle of the pectoral girdle that originates in both the clavicle and the scapula (the rest originate only in the scapula). The deltoid is the largest and most superficial muscle in the shoulder region. In descriptive anatomy and clinical practice, it is accepted that the deltoid muscle is divided into three portions and is differentiated according to its origins [
23,
33,
34]. However, this same division is not carried out based on its function.
Reinhold et al. [
35] identified a different activation pattern of the three portions during shoulder movements. In 1734, Albinus was the first to describe different segments of the deltoid muscle. He was followed by Fick [
2] and Kapanji [
3], who described seven functional portions in the deltoid muscle, and considered these portions according to their location concerning the pure abduction shaft. Other authors suggested that the deltoid can be divided into segments based on the presence of intramuscular tendons [
36,
37,
38] or based on the interpretation of functional studies (EMG or PET) in living subjects [
4,
6,
39]. Sakoma et al. [
6] assumed that the seven segments in which they divide the deltoid muscle reflect the functional units of the muscle, so we cannot consider these segments as muscle anomalies. The most common variations described are the fusion with the pectoralis major, or the presence of additional bands joined to the trapezium muscle [
23]. Some studies indicate that the lateral pectoral nerve may be involved in the innervation of the deltoid muscle [
40].
The specific variation found in our study has not been described previously. A bilateral separation of the posterior deltoid fibers enclosed in a separate fascial sheath was described by Kayikçioglu et al. [
24]. Kamburoğlu et al. [
25] and Sawant et al. [
26] observed the posterior fibers of the deltoid muscle were enclosed in a distinct fascial sheet, and the deltoid muscle was seen to arise from the middle third of the vertebral border of the scapula. Both studies describe a similar case where additional muscle fibers of the posterior deltoid are enclosed in a different fascial sheath but originated in the medial scapular edge and not in the infraspinatus fascia as in our case.
Fraser et al. [
27] found a posterior deltoid accessory belly attached to the teres minor muscle.
Until now, the only relationship that had been found between the deltoid muscle and the infraspinatus was through the communication of the fascial tissue [
7]. However, in our case, we find direct communication between both muscles since a portion of the deltoid muscle originates directly from the fascia of the infraspinatus. It has been described that there are compartment syndromes associated with the supraspinatus and infraspinatus muscles [
41,
42,
43], and although there are descriptions in the literature [
44,
45,
46,
47,
48], compartment syndromes that include the deltoid are more rare, likely because the deltoid fascia is usually connected to the infraspinatus fascia [
47], but the compartments do not communicate directly. In our finding, it is probable that a greater incidence of compartment syndrome is likely that includes the deltoid muscle as we find a direct relationship between the infraspinatus and the deltoid muscle.
The knowledge of the anatomical variations is indispensable in surgical interventions since the anatomical spaces or the reference points for the incisions can vary. Previous studies have shown how anatomical variations can complicate surgeries [
49]. Neurovascular structures, such as the axillary nerve or posterior circumflex artery, are vulnerable to traumatic lesions. The correct understanding of the anatomy in situ is essential for a good diagnosis and treatment of the surgical pathology of the shoulder. Unexpected anatomical variations can delay surgical times. Scully et al. [
50] found that prolonged surgical times may interfere with intervention by either treatment failure or iatrogenic injury.
Future work should focus on economical and non-invasive techniques for detecting anatomical anomalies before surgery, especially in complicated surgeries. In this line, ultrasound with 3D Doppler effectively detects anatomical variations of the shoulder [
51]. Knowledge of these abnormalities is likely to improve surgical outcomes and reduce complications.
5. Conclusions
The existence of such variations of the deltoid muscle (the additional belly of the deltoid muscle) should be kept in mind by surgeons.
Abnormal conditions of the deltoid muscle are also considered in compartment syndrome involving the shoulder. Therefore, consideration of this variant is necessary for the correct diagnosis and treatment of trauma or other shoulder pathology, which can be t is refractory to standard treatments.
Author Contributions
S.M.G.-S., A.G.-C. and F.G.-E. conceived and designed the study; S.M.G.-S., A.G.-C., J.D.-G., G.D.-G. and M.A.P.-G. carried out the dissection; S.M.G.-S., J.D.-G., M.A.P.-G., F.G.-E., G.D.-G. and A.G.-C. wrote the paper and done the final approval of the version to be submitted. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The donation process as well as the procurement and use of corpses, human remains and cadaveric remains for scientific and teaching purposes at the Rey Juan Carlos University, adhered to the appropriate regulation. These regulations were approved by the Governing Council of the Rey Juan Carlos University on 28 April 2009.
Informed Consent Statement
The bodies used in this study were donated legally to the Faculty of Health Sciences at the Universidad Rey Juan Carlos.
Acknowledgments
The authors would like to recognize those who graciously donated themselves to enable this research. Thank you. We thank Beatriz Santamaría and Alfonso García from Universidad Rey Juan Carlos for optimal technical assistance.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lumley, J.S. Surface Anatomy: The Anatomical Basis of Clinical Examination; Elsevier Health Sciences: Amsterdam, The Netherlands, 2008. [Google Scholar]
- Fick, R.A. Handbuch Der Anatomie Und Mechanik Der Gelenke: T. Spezielle Gelenk-Und Muskelmechanik; G. Fischer: Schaffhausen, Switzerland, 1911. [Google Scholar]
- Kapandji, A.I.; Kapandji, I.A. The Physiology of the Joints: The Upper Limb; Churchill Livingstone: London, UK, 2007; Volume I. [Google Scholar]
- Brown, J.; Wickham, J.; McAndrew, D.; Huang, X.-F. Muscles within muscles: Coordination of 19 muscle segments within three shoulder muscles during isometric motor tasks. J. Electromyogr. Kinesiol. 2007, 17, 57–73. [Google Scholar] [CrossRef] [PubMed]
- Gorelick, M.L.; Brown, J.M.M. Mechanomyographic assessment of contractile properties within seven segments of the human deltoid muscle. Eur. J. Appl. Physiol. 2007, 100, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Sakoma, Y.; Sano, H.; Shinozaki, N.; Itoigawa, Y.; Yamamoto, N.; Ozaki, T.; Itoi, E. Anatomical and functional segments of the deltoid muscle. J. Anat. 2011, 218, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Moccia, D.; Nackashi, A.A.; Schilling, R.; Ward, P.J. Fascial bundles of the infraspinatus fascia: Anatomy, function, and clinical considerations. J. Anat. 2016, 228, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, R.R.; Nandedkar, A.N.; Mysorekar, V.R. Position of the axillary nerve in the deltoid muscle. Anat. Rec. 1992, 232, 316–317. [Google Scholar] [CrossRef]
- Groh, G.I.; Simoni, M.; Rolla, P.; Rockwood, C.A. Loss of the deltoid after shoulder operations: An operative disaster. J. Shoulder Elb. Surg. 1994, 3, 243–253. [Google Scholar] [CrossRef]
- Rouviere, H.; Delmas, A. Anatomía Humana Descriptiva, Topográfica y Funcional; Masson: Barcelona, Spain, 2002; pp. 170–177. [Google Scholar]
- Loukas, M.; Grabska, J.; Tubbs, R.S.; Apaydin, N.; Jordan, R. Mapping the axillary nerve within the deltoid muscle. Surg. Radiol. Anat. 2008, 31, 43–47. [Google Scholar] [CrossRef]
- Leechavengvongs, S.; Teerawutthichaikit, T.; Witoonchart, K.; Uerpairojkit, C.; Malungpaishrope, K.; Suppauksorn, S.; Chareonwat, B. Surgical anatomy of the axillary nerve branches to the deltoid muscle. Clin. Anat. 2015, 28, 118–122. [Google Scholar] [CrossRef]
- Eakin, C.L.; Dvirnak, P.; Miller, C.M.; Hawkins, R.J. The Relationship of the Axillary Nerve to Arthroscopically Placed Capsulolabral Sutures. Am. J. Sports Med. 1998, 26, 505–509. [Google Scholar] [CrossRef]
- Perlmutter, G.S. Axillary nerve injury. Clin. Orthop. Relat. Res. 1999, 368, 28–36. [Google Scholar] [CrossRef]
- Cetik, O.; Uslu, M.; Acar, H.I.; Comert, A.; Tekdemir, I.; Cift, H. Is there a safe area for the axillary nerve in the deltoid muscle? A cadaveric study. JBJS 2006, 88, 2395–2399. [Google Scholar] [CrossRef]
- Mansat, P.; Cofield, R.H.; Kersten, T.E.; Rowland, C.M. Complications of rotator cuff repair. Orthop. Clin. 1997, 28, 205–213. [Google Scholar] [CrossRef]
- Albritton, M.J.; Barnes, C.J.; Basamania, C.J.; Karas, S.G. Relationship of the Axillary Nerve to the Proximal Screws of a Flexible Humeral Nail System: An Anatomic Study. J. Orthop. Trauma 2003, 17, 411–414. [Google Scholar] [CrossRef] [PubMed]
- Lewicky, Y.M.; Sheppard, J.E.; Ruth, J.T. The Combined Olecranon Osteotomy, Lateral Paratricipital Sparing, Deltoid Insertion Splitting Approach for Concomitant Distal Intra-articular and Humeral Shaft Fractures. J. Orthop. Trauma 2007, 21, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Rashid, A.; Abdul-Jabar, H.; Lam, F. Nerve injury associated with shoulder surgery. Curr. Orthop. 2008, 22, 284–288. [Google Scholar] [CrossRef]
- Stecco, C.; Gagliano, G.; Lancerotto, L.; Tiengo, C.; Macchi, V.; Porzionato, A.; De Caro, R.; Aldegheri, R. Surgical anatomy of the axillary nerve and its implication in the transdeltoid approaches to the shoulder. J. Shoulder Elb. Surg. 2010, 19, 1166–1174. [Google Scholar] [CrossRef] [PubMed]
- Fridén, J.; Lieber, R. Quantitative evaluation of the posterior deltoid to triceps tendon transfer based on muscle architectural properties. J. Hand Surg. 2001, 26, 147–155. [Google Scholar] [CrossRef]
- Crouch, D.L.; Plate, J.F.; Li, Z.; Saul, K. Biomechanical Contributions of Posterior Deltoid and Teres Minor in the Context of Axillary Nerve Injury: A Computational Study. J. Hand Surg. 2013, 38, 241–249. [Google Scholar] [CrossRef]
- Horan, F. (Ed.) Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 40th ed.; Churchill Livingstone Elsevier: Edinburgh, UK, 2008; ISBN 978-0-443-06684-9. [Google Scholar]
- Kayikçioglu, A.; Celik, H.H.; Yilmaz, E. An anatomic variation of the deltoid muscle (case report). Bull. De L’association Des Anat. 1993, 77, 15–16. [Google Scholar]
- Kamburoğlu, H.O.; Boran, O.F.; Sargon, M.F.; Keçik, A. An unusual variation of deltoid muscle. Int. J. Shoulder Surg. 2008, 2, 62. [Google Scholar] [CrossRef]
- Sawant, S.P.; Shaikh, S.T.; More, R.M. A Variant Deltoid Muscle—A Case Report. Int. J. Curr. Res. Rev. 2012, 4, 78. [Google Scholar]
- Fraser, P.R.; Thomas, J.; Guttmann, G.D.; Rosales, A.A. Rare accessory slip of the deltoid muscle conjoined with teres minor. Eur. J. Anat. 2014, 18, 195–197. [Google Scholar]
- Koch-Borner, S.; Dunn, J.A.; Fridén, J.; Wangdell, J. Rehabilitation After Posterior Deltoid to Triceps Transfer in Tetraplegia. Arch. Phys. Med. Rehabil. 2016, 97, S126–S135. [Google Scholar] [CrossRef] [PubMed]
- Métais, P.; Grimberg, J.; Clavert, P.; Kouvalchouk, J.-F.; Sirveaux, F.; Nourissat, G.; Garret, J.; Mansat, P.; Godenèche, A. Posterior shoulder instability managed by arthroscopic acromial pediculated bone-block. Technique. Orthop. Traumatol. Surg. Res. 2017, 103, S203–S206. [Google Scholar] [CrossRef] [PubMed]
- Löw, S.; Herold, D.; Eingartner, C. Pediculated deltoid muscle flap: An alternative for coverage of chronic radionecrotic lesions in the shoulder region. Der Unf. 2014, 117, 662. [Google Scholar]
- Veen, E.J.D.; Koorevaar, C.T.; Verdonschot, K.H.M.; Sluijter, T.E.; de Groot, T.; van der Hoeven, J.H.; Diercks, R.L.; Stevens, M. Compensatory Movement Patterns Are Based on Abnormal Activity of the Biceps Brachii and Posterior Deltoid Muscles in Patients with Symptomatic Rotator Cuff Tears. Clin. Orthop. Relat. Res. 2021, 479, 378–388. [Google Scholar] [CrossRef]
- Tubbs, R.S.; Tyler-Kabara, E.C.; Aikens, A.C.; Martin, J.P.; Weed, L.L.; Salter, E.G.; Oakes, W.J. Surgical anatomy of the axillary nerve within the quadrangular space. J. Neurosurg. 2005, 102, 912–914. [Google Scholar] [CrossRef]
- Muscolino, J.E. The Muscular System Manual: The Skeletal Muscles of the Human Body; Elsevier Health Sciences: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Palastanga, N.; Field, D.; Soames, R. Anatomy and Human Movement: Structure and Function; Elsevier Health Sciences: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Reinold, M.M.; Macrina, L.C.; Wilk, K.E.; Fleisig, G.S.; Dun, S.; Barrentine, S.W.; Ellerbusch, M.T.; Andrews, J.R. Electromyographic analysis of the supraspinatus and deltoid muscles during 3 common rehabilitation exercises. J. Athl. Train. 2007, 42, 464–469. [Google Scholar]
- Lorne, E.; Gagey, O.; Quillard, J.; Hue, E.; Gagey, N. The Fibrous Frame of the Deltoid Muscle: Its Functional and Surgical Relevance. Clin. Orthop. Relat. Res. 2001, 386, 222–225. [Google Scholar] [CrossRef]
- Leijnse, J.N.A.L.; Han, S.-H.; Kwon, Y.H. Morphology of deltoid origin and end tendons—A generic model. J. Anat. 2008, 213, 733–742. [Google Scholar] [CrossRef]
- Audenaert, E.; Barbaix, E. Separate segments within the deltoid muscle: Anatomical variants or wishful thinking? Int. J. Shoulder Surg. 2008, 2, 69. [Google Scholar] [CrossRef] [PubMed]
- Wickham, J.B.; Brown, J. Muscles within muscles: The neuromotor control of intra-muscular segments. Eur. J. Appl. Physiol. Occup. Physiol. 1998, 78, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Solomon, L.; Ravindranath, N.; Vidic, B.; Dym, M. Anatomical variant of the lateral pectoral nerve innervating the anterior portion of the deltoid muscle: A case report. Anat. Rec. Off. Publ. Am. Assoc. Anat. 1997, 249, 506–509. [Google Scholar] [CrossRef]
- Takakuwa, T.; Takeda, M.; Tada, H.; Katsuki, M.; Nakamura, S.; Matsuno, T. Acute compartment syndrome of the supraspinatus: A case report. J. Shoulder Elb. Surg. 2000, 9, 152–156. [Google Scholar] [CrossRef]
- Stahlfeld, K.R.; Parker, J.E.; McClain, E.J., 3rd. Supraspinatus compartment syndrome. Am. J. Orthop. (Belle Mead NJ) 2004, 33, 615–617. [Google Scholar]
- Kenny, R.M.; Beiser, C.W.; Patel, A. Supraspinatus and infraspinatus compartment syndrome following scapular fracture. Int. J. Shoulder Surg. 2013, 7, 28–31. [Google Scholar] [CrossRef]
- Diminick, M.; Shapiro, G.; Cornell, C. Acute Compartment Syndrome of the Triceps and Deltoid. J. Orthop. Trauma 1999, 13, 225–227. [Google Scholar] [CrossRef]
- Klocker, J.; Chemelli, A.; Bodner, G.; Gschwendtner, A.; Perkmann, R.; Tauscher, T.; Jaschke, W.; Fraedrich, G. Hyperperfusion Syndrome of the Deltoid Muscle after Subclavian Artery Angioplasty and Stenting. J. Endovasc. Ther. 2003, 10, 833–837. [Google Scholar] [CrossRef]
- Knapke, D.M.; Truumees, E. Posterior Arm and Deltoid Compartment Syndrome After Vitamin B12 Injection. Orthopedics 2004, 27, 520–521. [Google Scholar] [CrossRef]
- Rohde, R.S.; Goitz, R.J. Deltoid compartment syndrome: A result of operative positioning. J. Shoulder Elb. Surg. 2006, 15, 383–385. [Google Scholar] [CrossRef]
- Gaffney, D.; Slabaugh, M. Deltoid Compartment Syndrome After Antegrade Humeral Nailing. J. Orthop. Trauma 2009, 23, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Baraliakos, X.; Kanawati, B.; Boudelal, R.; Teske, W.; Kraemer, J.; Theodoridis, T. Microsurgical nerve root decompression in scoliotic lumbar spines—the relationship between important anatomical structures in correlation to imaging and implications for daily practice: Anatomic cadaveric study. J. Neurosurgery: Spine 2010, 13, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Scully, W.F.; Wilson, D.J.; Parada, S.A.; Arrington, E.D. Iatrogenic nerve injuries in shoulder surgery. JAAOS-J. Am. Acad. Orthop. Surg. 2013, 21, 717–726. [Google Scholar] [CrossRef]
- Kim, H.; Dahiya, N.; Teefey, S.A.; Keener, J.D.; Yamaguchi, K. Sonography of the teres minor: A study of cadavers. Am. J. Roentgenol. 2008, 190, 589–594. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, {kind=link}
{kind=link}
{kind=link}


