
Sex-Related Differences of Weight Bearing and Non-Weight Bearing Muscle Properties


Abstract
:1. Introduction
2. Results
Relationships among Muscle Characteristics with Relative and Absolute Strength
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Participants
4.3. Procedures
4.3.1. Hydration and Body Composition Assessment
4.3.2. Musculoskeletal Ultrasonography
4.3.3. Muscular Strength Assessment
4.3.4. Quantifying Muscle Quality
4.4. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lynch, N.A.; Metter, E.J.; Lindle, R.S.; Fozard, J.L.; Tobin, J.D.; Roy, T.A.; Fleg, J.L.; Hurley, B.F. Muscle Quality. I. Age-Associated Differences between Arm and Leg Muscle Groups. J. Appl. Physiol. 1999, 86, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Glenmark, B.; Nilsson, M.; Gao, H.; Gustafsson, J.-Å.; Dahlman-Wright, K.; Westerblad, H. Difference in Skeletal Muscle Function in Males vs. Females: Role of Estrogen Receptor-β. Am. J. Physiol.-Endocrinol. Metab. 2004, 287, E1125–E1131. [Google Scholar] [CrossRef] [PubMed]
- Haizlip, K.M.; Harrison, B.C.; Leinwand, L.A. Sex-Based Differences in Skeletal Muscle Kinetics and Fiber-Type Composition. Physiology 2015, 30, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.E.J.; MacDougall, J.D.; Tarnopolsky, M.A.; Sale, D.G. Gender Differences in Strength and Muscle Fiber Characteristics. Eur. J. Appl. Physiol. 1993, 66, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Staron, R.S.; Hagerman, F.C.; Hikida, R.S.; Murray, T.F.; Hostler, D.P.; Crill, M.T.; Ragg, K.E.; Toma, K. Fiber Type Composition of the Vastus Lateralis Muscle of Young Men and Women. J. Histochem. Cytochem. Off. J. Histochem. Soc. 2000, 48, 623–629. [Google Scholar] [CrossRef]
- Simoneau, J.A.; Bouchard, C. Human Variation in Skeletal Muscle Fiber-Type Proportion and Enzyme Activities. Am. J. Physiol.-Endocrinol. Metab. 1989, 257, E567–E572. [Google Scholar] [CrossRef]
- Bouillon, L.E.; Wilhelm, J.; Eisel, P.; Wiesner, J.; Rachow, M.; Hatteberg, L. Electromyographic Assessment of Muscle Activity between Genders during Unilateral Weight-Bearing Tasks Using Adjusted Distances. Int. J. Sports Phys. Ther. 2012, 7, 595–605. [Google Scholar]
- de Boer, M.D.; Seynnes, O.R.; di Prampero, P.E.; Pišot, R.; Mekjavić, I.B.; Biolo, G.; Narici, M.V. Effect of 5 Weeks Horizontal Bed Rest on Human Muscle Thickness and Architecture of Weight Bearing and Non-Weight Bearing Muscles. Eur. J. Appl. Physiol. 2008, 104, 401–407. [Google Scholar] [CrossRef]
- Ivey, F.M.; Tracy, B.L.; Lemmer, J.T.; NessAiver, M.; Metter, E.J.; Fozard, J.L.; Hurley, B.F. Effects of Strength Training and Detraining on Muscle Quality: Age and Gender Comparisons. J. Gerontol. A. Biol. Sci. Med. Sci. 2000, 55, B152–B157. [Google Scholar] [CrossRef]
- Yoshiko, A.; Yamauchi, K.; Kato, T.; Ishida, K.; Koike, T.; Oshida, Y.; Akima, H. Effects of Post-Fracture Non-Weight-Bearing Immobilization on Muscle Atrophy, Intramuscular and Intermuscular Adipose Tissues in the Thigh and Calf. Skelet. Radiol. 2018, 47, 1541–1549. [Google Scholar] [CrossRef]
- Fukumoto, K.; Fukuda, O.; Tsubai, M.; Muraki, S. Development of a Flexible System for Measuring Muscle Area Using Ultrasonography. IEEE Trans. Biomed. Eng. 2011, 58, 1147–1155. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.; Spitz, R.W.; Bell, Z.W.; Viana, R.B.; Chatakondi, R.N.; Abe, T.; Loenneke, J.P. Exercise Induced Changes in Echo Intensity within the Muscle: A Brief Review. J. Ultrasound 2020, 23, 457–472. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, E.N.; Rech, A.; Minozzo, F.; Radaelli, R.; Botton, C.E.; Pinto, R.S. Relationship between Quadriceps Femoris Echo Intensity, Muscle Power, and Functional Capacity of Older Men. AGE 2014, 36, 9625. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C. Assessing Regional Muscle Mass with Segmental Measurements of Bioelectrical Impedance in Obese Women during Weight Lossa,b. Ann. N. Y. Acad. Sci. 2000, 904, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Zoeller, R.F.; Ryan, E.D.; Gordish-Dressman, H.; Price, T.B.; Seip, R.L.; Angelopoulos, T.J.; Moyna, N.M.; Gordon, P.M.; Thompson, P.D.; Hoffman, E.P. Allometric Scaling of Isometric Biceps Strength in Adult Females and the Effect of Body Mass Index. Eur. J. Appl. Physiol. 2008, 104, 701–710. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Kearns, C.F.; Fukunaga, T. Sex Differences in Whole Body Skeletal Muscle Mass Measured by Magnetic Resonance Imaging and Its Distribution in Young Japanese Adults. Br. J. Sports Med. 2003, 37, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Heymsfield, S.B.; Wang, Z.; Ross, R. Skeletal Muscle Mass and Distribution in 468 Men and Women Aged 18–88 Yr. J. Appl. Physiol. 2000, 89, 81–88. [Google Scholar] [CrossRef]
- Stock, M.S.; Oranchuk, D.J.; Burton, A.M.; Phan, D.C. Age-, Sex-, and Region-Specific Differences in Skeletal Muscle Size and Quality. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2020, 45, 1253–1260. [Google Scholar] [CrossRef]
- Caresio, C.; Molinari, F.; Emanuel, G.; Minetto, M.A. Muscle Echo Intensity: Reliability and Conditioning Factors. Clin. Physiol. Funct. Imaging 2015, 35, 393–403. [Google Scholar] [CrossRef]
- Young, H.-J.; Jenkins, N.T.; Zhao, Q.; Mccully, K.K. Measurement of Intramuscular Fat by Muscle Echo Intensity. Muscle Nerve 2015, 52, 963–971. [Google Scholar] [CrossRef]
- Reimers, K.; Reimers, C.D.; Wagner, S.; Paetzke, I.; Pongratz, D.E. Skeletal Muscle Sonography: A Correlative Study of Echogenicity and Morphology. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 1993, 12, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Palmer, T.B.; Akehi, K.; Thiele, R.M.; Smith, D.B.; Thompson, B.J. Reliability of Panoramic Ultrasound Imaging in Simultaneously Examining Muscle Size and Quality of the Hamstring Muscles in Young, Healthy Males and Females. Ultrasound Med. Biol. 2015, 41, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Egan, B.; Zierath, J.R. Exercise Metabolism and the Molecular Regulation of Skeletal Muscle Adaptation. Cell Metab. 2013, 17, 162–184. [Google Scholar] [CrossRef] [PubMed]
- Horwath, O.; Moberg, M.; Larsen, F.J.; Philp, A.; Apró, W.; Ekblom, B. Influence of Sex and Fiber Type on the Satellite Cell Pool in Human Skeletal Muscle. Scand. J. Med. Sci. Sports 2021, 31, 303–312. [Google Scholar] [CrossRef]
- Witteveen, E.; Sommers, J.; Wieske, L.; Doorduin, J.; van Alfen, N.; Schultz, M.J.; van Schaik, I.N.; Horn, J.; Verhamme, C. Diagnostic Accuracy of Quantitative Neuromuscular Ultrasound for the Diagnosis of Intensive Care Unit-Acquired Weakness: A Cross-Sectional Observational Study. Ann. Intensive Care 2017, 7, 40. [Google Scholar] [CrossRef]
- Bartolomei, S.; Grillone, G.; Di Michele, R.; Cortesi, M. A Comparison between Male and Female Athletes in Relative Strength and Power Performances. J. Funct. Morphol. Kinesiol. 2021, 6, 17. [Google Scholar] [CrossRef]
- Kubo, K.; Kanehisa, H.; Fukunaga, T. Effects of Resistance and Stretching Training Programmes on the Viscoelastic Properties of Human Tendon Structures in Vivo. J. Physiol. 2002, 538, 219–226. [Google Scholar] [CrossRef]
- Trevino, M.A.; Sterczala, A.J.; Miller, J.D.; Wray, M.E.; Dimmick, H.L.; Ciccone, A.B.; Weir, J.P.; Gallagher, P.M.; Fry, A.C.; Herda, T.J. Sex-Related Differences in Muscle Size Explained by Amplitudes of Higher-Threshold Motor Unit Action Potentials and Muscle Fibre Typing. Acta Physiol. Oxf. Engl. 2019, 225, e13151. [Google Scholar] [CrossRef]
- Coratella, G.; Longo, S.; Rampichini, S.; Limonta, E.; Shokohyar, S.; Bisconti, A.V.; Cè, E.; Esposito, F. Quadriceps and Gastrocnemii Anatomical Cross-Sectional Area and Vastus Lateralis Fascicle Length Predict Peak-Power and Time-To-Peak-Power. Res. Q. Exerc. Sport 2020, 91, 158–165. [Google Scholar] [CrossRef]
- Atkinson, R.A.; Srinivas-Shankar, U.; Roberts, S.A.; Connolly, M.J.; Adams, J.E.; Oldham, J.A.; Wu, F.C.W.; Seynnes, O.R.; Stewart, C.E.H.; Maganaris, C.N.; et al. Effects of Testosterone on Skeletal Muscle Architecture in Intermediate-Frail and Frail Elderly Men. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 1215–1219. [Google Scholar] [CrossRef]
- Snyder, P.J.; Peachey, H.; Hannoush, P.; Berlin, J.A.; Loh, L.; Lenrow, D.A.; Holmes, J.H.; Dlewati, A.; Santanna, J.; Rosen, C.J.; et al. Effect of Testosterone Treatment on Body Composition and Muscle Strength in Men over 65 Years of Age. J. Clin. Endocrinol. Metab. 1999, 84, 2647–2653. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.M.; Ferriolli, E.; Stephens, N.A.; Fearon, K.C.H.; Greig, C. Relationship between Sedentary Behaviour, Physical Activity, Muscle Quality and Body Composition in Healthy Older Adults. Age Ageing 2012, 41, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Bishop, P.; Cureton, K.; Collins, M. Sex Difference in Muscular Strength in Equally-Trained Men and Women. Ergonomics 1987, 30, 675–687. [Google Scholar] [CrossRef] [PubMed]
- Merrigan, J.J.; White, J.B.; Hu, Y.E.; Stone, J.D.; Oliver, J.M.; Jones, M.T. Differences in Elbow Extensor Muscle Characteristics between Resistance-Trained Men and Women. Eur. J. Appl. Physiol. 2018, 118, 2359–2366. [Google Scholar] [CrossRef] [PubMed]
- Schantz, P.; Randall-Fox, E.; Hutchison, W.; Tydén, A.; Astrand, P.O. Muscle Fibre Type Distribution, Muscle Cross-Sectional Area and Maximal Voluntary Strength in Humans. Acta Physiol. Scand. 1983, 117, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Murphy, A.J.; Wilson, G.J. Poor Correlations between Isometric Tests and Dynamic Performance: Relationship to Muscle Activation. Eur. J. Appl. Physiol. 1996, 73, 353–357. [Google Scholar] [CrossRef] [PubMed]
- McGuigan, M.R.; Newton, M.J.; Winchester, J.B.; Nelson, A.G. Relationship between Isometric and Dynamic Strength in Recreationally Trained Men. J. Strength Cond. Res. 2010, 24, 2570–2573. [Google Scholar] [CrossRef]
- Cadore, E.L.; Izquierdo, M.; Conceição, M.; Radaelli, R.; Pinto, R.S.; Baroni, B.M.; Vaz, M.A.; Alberton, C.L.; Pinto, S.S.; Cunha, G.; et al. Echo Intensity Is Associated with Skeletal Muscle Power and Cardiovascular Performance in Elderly Men. Exp. Gerontol. 2012, 47, 473–478. [Google Scholar] [CrossRef]
- Fukumoto, Y.; Ikezoe, T.; Yamada, Y.; Tsukagoshi, R.; Nakamura, M.; Mori, N.; Kimura, M.; Ichihashi, N. Skeletal Muscle Quality Assessed from Echo Intensity Is Associated with Muscle Strength of Middle-Aged and Elderly Persons. Eur. J. Appl. Physiol. 2012, 112, 1519–1525. [Google Scholar] [CrossRef]
- Uezumi, A.; Fukada, S.; Yamamoto, N.; Takeda, S.; Tsuchida, K. Mesenchymal Progenitors Distinct from Satellite Cells Contribute to Ectopic Fat Cell Formation in Skeletal Muscle. Nat. Cell Biol. 2010, 12, 143–152. [Google Scholar] [CrossRef]
- Sammour, I.; Somashekar, S.; Huang, J.; Batlahally, S.; Breton, M.; Valasaki, K.; Khan, A.; Wu, S.; Young, K.C. The Effect of Gender on Mesenchymal Stem Cell (MSC) Efficacy in Neonatal Hyperoxia-Induced Lung Injury. PLoS ONE 2016, 11, e0164269. [Google Scholar] [CrossRef] [PubMed]
- Seo, N.J.; Armstrong, T.J.; Ashton-Miller, J.A.; Chaffin, D.B. Wrist Strength Is Dependent on Simultaneous Power Grip Intensity. Ergonomics 2008, 51, 1594–1605. [Google Scholar] [CrossRef] [PubMed]
- Song, J.S.; Abe, T.; Bell, Z.W.; Wong, V.; Spitz, R.W.; Yamada, Y.; Loenneke, J.P. The Relationship between Muscle Size and Strength Does Not Depend on Echo Intensity in Healthy Young Adults. J. Clin. Densitom. 2021, 24, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Kenis-Coskun, O.; Giray, E.; Gencer-Atalay, Z.K.; Yagci, I.; Karadag-Saygi, E. Reliability of Quantitative Ultrasound Measurement of Flexor Digitorum Superficialis and Profundus Muscles in Stroke. J. Comp. Eff. Res. 2020, 9, 1293–1300. [Google Scholar] [CrossRef]
- Beck, T.W. The Importance of a Priori Sample Size Estimation in Strength and Conditioning Research. J. Strength Cond. Res. 2013, 27, 2323–2337. [Google Scholar] [CrossRef]
- Organ, L.W.; Bradham, G.B.; Gore, D.T.; Lozier, S.L. Segmental Bioelectrical Impedance Analysis: Theory and Application of a New Technique. J. Appl. Physiol. 1994, 77, 98–112. [Google Scholar] [CrossRef]
- Chiles Shaffer, N.; Fabbri, E.; Ferrucci, L.; Shardell, M.; Simonsick, E.M.; Studenski, S. Muscle Quality, Strength, and Lower Extremity Physical Performance in the Baltimore Longitudinal Study of Aging. J. Frailty Aging 2017, 6, 183–187. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Males (n = 14) | Females (n = 14) | Effect Size | ||
|---|---|---|---|---|
| Body Composition | Mean ± SD | Mean ± SD | t-Ratio | Cohen’s d |
| TFFM (kg) | 70.61 ± 14.24 * | 46.74 ± 5.90 | −5.8 | 2.19 |
| % BF (%) | 22.57 ± 8.95 | 28.56 ± 8.27 | 1.84 | 0.7 |
| ArmFFM (kg) | 4.46 ± 1.08 * | 2.49 ± 0.42 | −6.34 | 2.33 |
| LegFFM (kg) | 9.53 ± 1.90 * | 6.87 ± 0.96 | −4.66 | 1.76 |
| Muscle Composition Leg | ||||
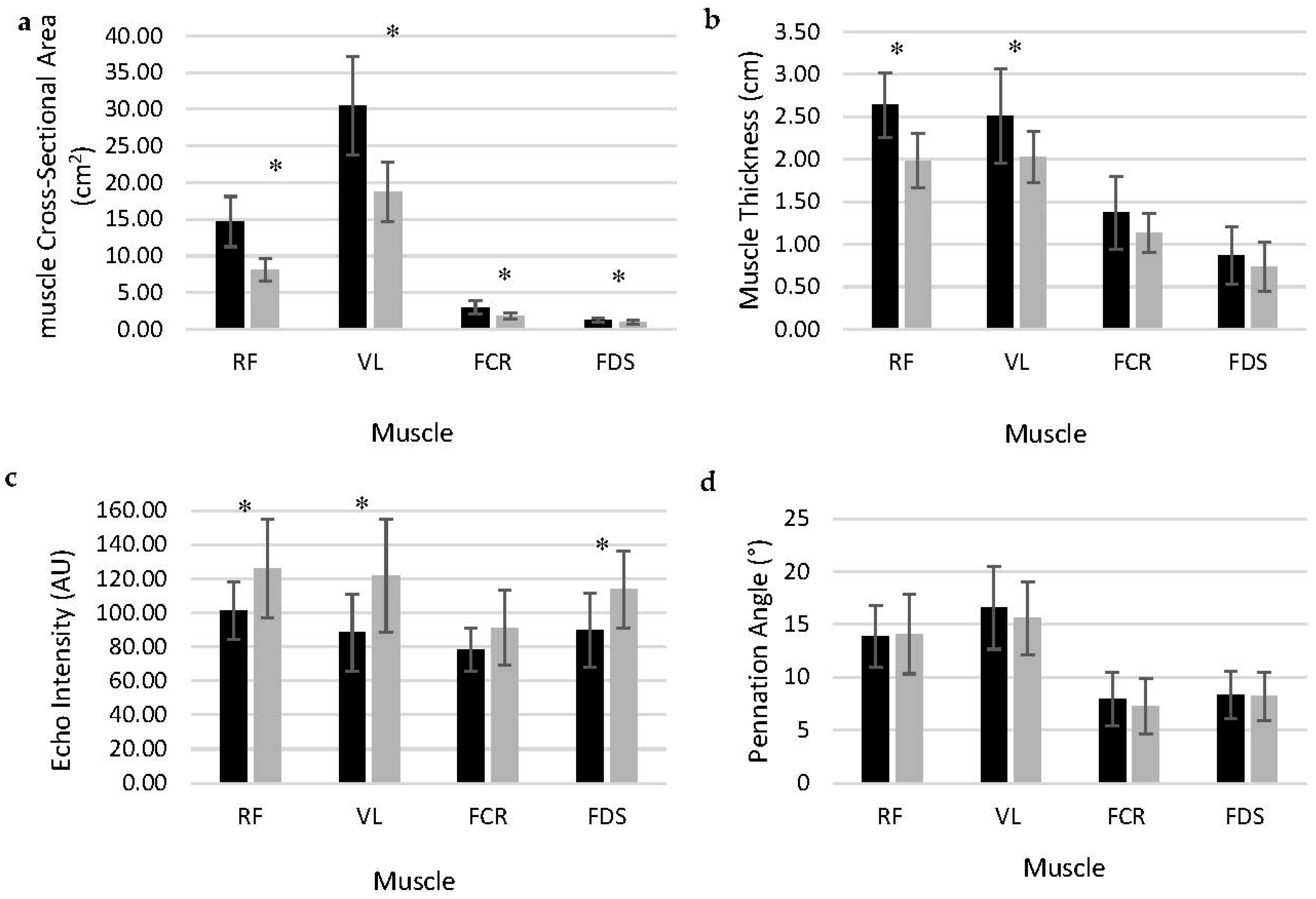
| RF mCSA (cm2) | 14.69 ± 3.43 * | 8.13 ± 1.53 | −6.53 | 2.47 |
| RF EI (AU) | 101.53 ± 16.94 | 126.23 ± 29.00 * | 2.75 | 1.04 |
| RF MT (cm) | 2.64 ± 0.38 * | 1.98 ± 0.32 | −4.97 | 1.88 |
| VL mCSA (cm2) | 30.52 ± 6.71 * | 18.75 ± 4.07 | −5.61 | 2.12 |
| VL EI (AU) | 88.30 ± 22.65 | 122.08 ± 32.14 * | 3.22 | 1.22 |
| VL MT (cm) | 2.51 ± 0.56 * | 2.01 ± 0.28 | −3.02 | 1.14 |
| Muscle Composition Arm | ||||
| FCR mCSA (cm2) | 3.00 ± 0.87 * | 1.80 ± 0.41 | −4.7 | 1.78 |
| FCR EI (AU) | 78.12 ± 12.73 | 88.91 ± 21.14 | 1.64 | 0.62 |
| FCR MT (cm) | 1.37 ± 0.43 | 1.23 ± 0.30 | −1 | 0.38 |
| FDS mCSA (cm2) | 1.24 ± 0.31 * | 0.95 ± 0.26 | −2.71 | 1.03 |
| FDS EI (AU) | 89.63 ± 21.70 | 113.84 ± 22.66 * | 2.89 | 1.09 |
| FDS MT (cm) | 0.87 ± 0.34 | 0.78 ± 0.28 | −0.8 | 0.3 |
| Relative Strength | ||||
| ArmMQ | 13.06 ± 1.90 | 12.94 ± 2.90 | −0.14 | 0.79 |
| LegMQ | 7.13 ± 1.73 | 6.10 ± 1.00 | −1.93 | 0.73 |
| Absolute Strength | ||||
| HG (kg) | 57.29 ± 11.45 * | 31.50 ± 4.93 | −7.73 | 2.93 |
| LE (kg) | 66.89 ± 18.10 * | 41.94 ± 8.89 | −4.63 | 1.75 |
| Pennation Angle | ||||
| RF PA (°) | 13.90 ± 2.90 | 14.10 ± 3.77 | 0.16 | 0.6 |
| VL PA (°) | 16.56 ± 3.90 | 15.62 ± 3.45 | −0.67 | 0.25 |
| FCR PA (°) | 7.95 ± 2.51 | 7.29 ± 2.62 | −0.68 | 0.28 |
| FDS PA (°) | 8.32 ± 2.25 | 8.18 ± 2.31 | −0.17 | 0.06 |
| Males | Females | |||
|---|---|---|---|---|
| Pearson’s r | p-Value | Pearson’s r | p-Value | |
| Leg Extension | ||||
| RF mCSA | 0.521 | 0.056 | 0.44 | 0.116 |
| RF EI | −0.296 | 0.304 | −0.373 | 0.188 |
| RF mT | 0.303 | 0.293 | 0.424 | 0.131 |
| RF PA | −0.087 | 0.766 | 0.141 | 0.632 |
| VL mCSA | 0.455 | 0.111 | 0.592 * | 0.026 |
| VL EI | −0.270 | 0.350 | −0.321 | 0.263 |
| VL mT | 0.402 | 0.154 | 0.202 | 0.488 |
| VL PA | 0.084 | 0.775 | 0.057 | 0.847 |
| Total Leg mCSA | 0.491 | 0.074 | 0.667 * | 0.009 |
| LegFFM | 0.356 | 0.212 | 0.652 * | 0.012 |
| RF EI | −0.656 * | 0.011 | −0.412 | 0.143 |
| VL EI | −0.407 | 0.148 | −0.518 | 0.058 |
| Handgrip | ||||
| FCR mCSA | 0.468 | 0.092 | 0.053 | 0.857 |
| FCR EI | 0.340 | 0.235 | −0.220 | 0.451 |
| FCR mT | −0.071 | 0.810 | −0.238 | 0.412 |
| FCR PA | −0.293 | 0.310 | −0.088 | 0.766 |
| FDS mCSA | 0.133 | 0.650 | 0.391 | 0.167 |
| FDS EI | −0.427 | 0.128 | −0.450 | 0.106 |
| FDS mT | −0.115 | 0.697 | −0.087 | 0.768 |
| FDS PA | −0.133 | 0.651 | −0.431 | 0.124 |
| Total Arm mCSA | 0.742 * | 0.002 | 0.282 | 0.329 |
| ArmFFM | 0.815 * | <0.001 | 0.201 | 0.492 |
| ArmMQ | ||||
| FCR EI | −0.050 | 0.865 | −0.100 | 0.733 |
| FDS EI | −0.413 | 0.142 | −0.024 | 0.936 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nabavizadeh, O.; Herda, A.A. Sex-Related Differences of Weight Bearing and Non-Weight Bearing Muscle Properties. Muscles 2023, 2, 400-412. https://doi.org/10.3390/muscles2040031
Nabavizadeh O, Herda AA. Sex-Related Differences of Weight Bearing and Non-Weight Bearing Muscle Properties. Muscles. 2023; 2(4):400-412. https://doi.org/10.3390/muscles2040031
Chicago/Turabian StyleNabavizadeh, Omid, and Ashley A. Herda. 2023. "Sex-Related Differences of Weight Bearing and Non-Weight Bearing Muscle Properties" Muscles 2, no. 4: 400-412. https://doi.org/10.3390/muscles2040031