1. Introduction
Myofascial pain syndrome (MPS) is a common, costly and often persistent musculoskeletal problem that affects 85% of the general population at some point in their lifetime (Fleckenstein et al., 2010; Simon, 1996) [
1,
2]. Overall rates vary between the male and female population and with different patient populations with MPS reported as the leading cause of chronic and persistent musculoskeletal regional pain. MPS can be multi-regional to include neck, shoulder, chronic back and facial pain (Li et al., 2017) [
3]. In the United States, the estimated economic cost for the management of chronic pain is about USD 560–635 billion per annum for medical care and disability programs, with the potential to increase year on year (Gaskin and Richard, 2012) [
4]. Therefore, it is important that chronic musculoskeletal pain such as MPS in the neck and upper back is treated efficiently and effectively in order to improve patient’s clinical outcomes and experiences.
The clinical manifestation of MPS varies widely because it is not a distinct pathology. It is characterised by localised pain, muscle tenderness, palpable intramuscular taut band, local twitch response, referred pain, muscle spasm and sleep disturbance (Fernández-de-las-Peñas et al., 2012; Sciotti et al., 2001; Alvarez and Rockwell, 2001; Travell and Simmons, 1999) [
5,
6,
7,
8]. Myofascial trigger points can produce symptoms of pain upon palpation and pressure. A nail bed palpation by pressing manually with a thumb or using a digital algometer probe can trigger a local twitch response (LTR), which can reproduce symptoms of pain. This study will use a digital algometer to measure pressure pain threshold, which has been used by previous authors (Luan et al., 2019) [
9].
Most patients with MPS are treated by physiotherapists, physicians, Chiropractors and Osteopaths using trigger point injection, dry needling, acupuncture, ultrasound, stretches, deep frictional massages and kinesio-taping (Galasso et al., 2020; Tough et al., 2009; Müller-Ehrenberg, 2005; Fernández-de-las-Peñas et al., 2012) [
5,
10,
11,
12]. However, the most effective treatment for MPS is not known.
Radial shockwave is one of the most common and non-invasive treatment methods for musculoskeletal tissue pains such as MPS that are normally very difficult to treat (Watson, 2014) [
13]. It comes with minimal negative side effects. Radial shockwaves are low- to medium-energy pulses, and their penetration depths are normally 0–6 cm (“0–2.3”) (Watson, 2014) [
13]. The therapeutic doses of radial shockwaves range from low (up to 0.08 mJ/mm
2) to high (up to 0.63 mJ/mm
2) energy levels (Watson, 2014) [
13]. The number of shocks per session is usually between 1000 and 2500, and the number of treatment sessions varies between three and seven.
Some of the established therapeutic and biological effects of radial shockwave include mechanical stimulation and increased local blood flow, which potentially lead to tissue repair and regeneration. These actions enhance micro-functional and micro-structural changes, and increase cellular activity—release of substance P, prostaglandin E2 and tumour growth factor (TGF β), transient analgesic effect on afferent nerves and breakdown of calcific deposits (Watson, 2014; Wang, 2012) [
13,
14]. No evidence of serious tissue destruction at therapy level doses has been reported.
Some authors [
15,
16,
17,
18] (Kiraly et al., 2018, Lee and Han, 2013; Gur et al., 2013, Cho et al., 2012) have demonstrated the efficacy of shockwave therapy to improve outcomes of pain and function in neck pain patients presenting with MPS despite unclear pathophysiology. In spite of these findings, recent systematic reviews [
19,
20] (Yoo et al., 2020; Jun et al., 2021), found very low-level evidence to support its use for pain relief in neck pain patients with MPS in the short-term, due to the poor methodological qualities and small sample size. Therefore, the authors recommended further large-scale, good-quality sham (placebo)-controlled trials in this area. Furthermore, previous studies [
17,
21,
22] (Manafnezhad et al., 2019; Gur et al., 2013; and Jeon et al., 2012) that have compared the effectiveness of shockwave therapy were not purely sham (placebo)-controlled trials. A truly appropriate sham (placebo) must be biologically inactive and psychologically credible, meaning it must be indistinguishable (by the patient) from real intervention (Vickers, 2002) [
23]. In this study, the sham shockwave produces sound, which makes it psychologically credible and similar to the real shockwave. However, it is physiologically different compared with the real shockwave because it is biologically inactive (no therapeutic dose). Therefore, given the painful nature of the treatment in both groups, the sham may not exclude a placebo effect.
Furthermore, previous studies on the effect of shockwave therapy on MPS did not consider the experiences of patients regarding this intervention. Moreover, based on our knowledge and extensive literature review, no study has compared both the effectiveness of shockwaves on MPS using a sham versus a true shockwave therapy and the experiences of the patients receiving the treatment. This study will, therefore, investigate the effectiveness of radial shockwave therapy in reducing pain and disability, and improving the function of patients with MPS in the neck and upper back. It will also explore the experiences of patients receiving this treatment.
1.1. Aims of the Study
Primary Aims
To determine the effectiveness of radial shockwave therapy compared to a sham (placebo) for the treatment of patients with MPS in neck and upper back.
To establish the experiences of patients with MPS in the neck and upper back receiving radial shockwave treatment.
1.2. Research Questions
Is radial shockwave therapy more effective at improving MPS in the neck and upper back and compared to a sham (placebo)?
What are the experiences of patients with MPS in the neck and upper back receiving radial shockwave therapy?
2. Methods and Materials
2.1. Mixed Method Design
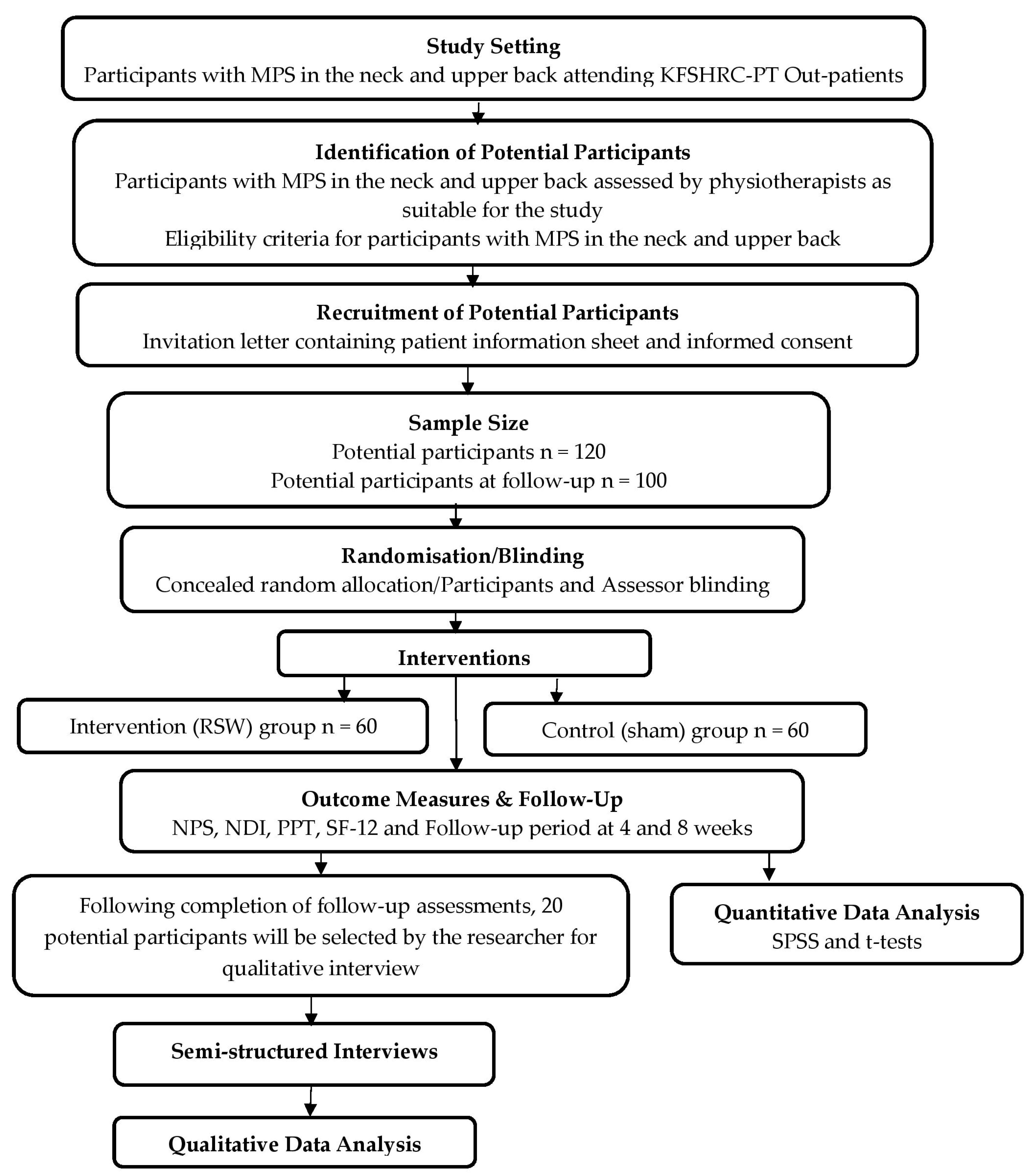
The research design for this study is both quantitative and qualitative. A double-blind RCT with a pragmatic approach will be used as the quantitative study; it will precede the semi-structured interviews that will be used for the qualitative study. This is because the RCT design is capable of detecting clinically important outcomes such as myofascial pain, while the qualitative approach will enable in-depth and rich data to be gathered concerning the patient’s experience Morgan (1993) [
24]. This study adopted the priority sequence approach for mixed methods design suggested by Morgan (1993) [
24] as the research methodology. This means that a principally quantitative approach will be complemented by a qualitative study using semi-structured qualitative interviews. The qualitative method will serve as a follow-up to the quantitative approach. This study will have two phases. Phase 1 will involve an RCT and phase 2 will be a qualitative study using semi-structured interview. The flow chart for the research design is summarised in
Figure 1.
2.2. Phase 1: Methods
Design: Quantitative—Randomised Controlled Trial
This study will make use of a pragmatic, two-arm, parallel, doubled-blind, randomised controlled trial as the quantitative study design. RCTs are regarded as the gold standard when evaluating the effectiveness of interventions such as shockwave therapy because they instil confidence that a difference in outcome can be directly attributed to a difference in the treatments and not due to some other confounding factors such as age (McGovern, 2001) [
25]. However, the experience of receiving such an intervention may play a role (Black, 1996) [
26].
2.3. Study Setting
This study will take place at the outpatient department of the physical rehabilitation, where potential participants will be recruited.
2.4. Identification of Potential Participants
Potential participants will be patients who have been referred to the Physical Rehabilitation service by the family physician and/or other specialists in the hospital with MPS in the neck and/or upper back. At the first appointment, a Physical Therapist (PT) will identify through a face-to-face assessment if they have a diagnosis of MPS in the neck and/or upper back and would benefit from radial shockwave therapy. A diagnosis of MPS (the presence or absence of active myofascial trigger points in the neck and or upper back) will be made by the assessing PT according to the inclusion and exclusion criteria defined by previous authors (Travell and Simons 1999, Luan et al., 2019) [
8,
9]. See
Table 1 below.
2.5. Clinician Involvement in the Study
The principal investigator and five outpatient PTs who are trained and experienced in the use of radial shockwave therapy will be involved in this study. A trained and experienced PT will be involved in obtaining consent from, assessing and treating the patients. The same PT will be involved in the patient’s initial assessment and the baseline measurement. Subsequent appointments and rate of progression will be determined by this Physiotherapist. Information about the eligibility criteria will be provided to all PTs to aid diagnosis, and they will receive training on the study protocol.
2.6. Recruitment of Potential Participants
During the first physical therapy appointment, potential participants will be informed verbally by the admin staff and/or by a letter of invitation to take part in the study. The invitation pack will contain a patient information sheet (PIS) that contains consent form (for both the quantitative study and qualitative interviews). Potential participants will be informed that their participation in the study is voluntary, and that they will be free to withdraw from the study at any time without affecting the course of their treatment. Potential participants who are interested in taking part in the study but have further questions will be encouraged to contact the principal investigator via a study mobile number, which will be provided in the PIS. Potential participants will be asked to read the PIS before participating in the study, they will have an opportunity to ask questions if they wish to participate and will be asked to sign the consent forms. On arrival for their first PT appointment, potential participants who provide written informed consent and fulfil the eligibility criteria after being screened by the assessing and treating PT will be recruited into the study. Participants who do not wish to participate will receive standard PT treatment.
2.7. Randomisation
The randomisation allocation sequence will be based on a computer-generated random sequence using a permuted block size of 4 and concealed random allocation using sealed opaque envelopes. Allocation concealment ensures that participants and clinicians do not know or predict what the next patient and treatment allocation will be (Viera et al., 2007) [
27]. Assignment will be by sequentially numbered, otherwise identical, sealed envelopes with a written code A or B designating intervention (radial shockwave therapy) or control (sham (placebo)), respectively. Following notification of the randomisation result by the admin staff, the treating PT will assign the patient to the treatment allocations using the label A or B on the sealed envelope. The patient will receive either the experimental treatment (radial shockwave therapy) if the envelope is labelled A, or they will receive the control treatment (sham (placebo)) if it is labelled B. This process will minimise systematic bias because it will ensure that there are no order or time effects. The treating PTs have been trained in both treatment methods.
2.8. Interventions
2.8.1. Intervention (Experimental) Group
These patients will receive a total of 6 sessions with a week’s interval of radial shockwaves that will be performed using a (Storz Medical) device with the following manufacturer’s parameters: 0.57 mJ/mm2 (intensity 1.5 bar) applied as low energy, pulses 2000, frequency 15 Hz. The D20 transmitter (Ø 20 mm) headpiece will be used. Total treatment time including standard PT stretches and exercises will be 30 min. The radial shockwave will be delivered by a designated Physiotherapist, who will evaluate the participants before the treatment. Before the treatment, the treating Physiotherapist will ensure aseptic techniques, including the use of clean coupling gel, and they will ensure the participants’ skin is intact. Furthermore, prior to treatment, the myofascial triggers will be specifically confirmed through twitching response induced by a localised probe using a digital algometer.
2.8.2. Control (Sham (Placebo)) Group
These patients will receive an identical treatment regime except that they will receive a no-energy shock of 0.03 mJ/mm
2, an ineffective (a non-therapeutic) level of radial shockwave therapy (Watson, 2014) [
13], and participants will be blinded to their treatment by only hearing the sound from the shockwave machine.
Both groups receiving either a radial shockwave or sham (placebo) will be permitted to continue with their current pain medication regime such as paracetamol or ibuprofen. Other forms of conservative intervention characteristic of the management of MPS in the neck and or upper back such as stretching and strengthening exercises will be allowed for both groups. Therefore, both groups are equally controlled for medications or other treatment modalities. This is reflective of “real life” practice where patients receiving physiotherapy are advised not to receive a single treatment or intervention in isolation (Green et al., 2003) [
28].
Standard aftercare and post-treatment information will be provided verbally, and these will include advice for participants to continue their normal daily activities. Although no serious side effects have been reported with the use of radial shockwave therapy, participants will be informed of potential side effects such as mild pain, redness or swelling (Luan et al., 2019) [
9]. They will be advised to inform their family physician in the event of any adverse reactions such as hematoma. All side effects will be managed by normal clinical procedure by the head of department and the clinical research PT.
2.9. Outcome Measures and Follow-Up
2.9.1. Baseline Assessment
Baseline characteristics will include age, gender, duration of symptoms, current treatment analgesia and current treatment NSAIDS. It will also include the initial NPS, NDI, PPT and SF-12 scores.
2.9.2. Primary Outcomes
The primary outcome measures will be a numeric pain scale (NPS) and neck disability index (NDI), while the secondary outcomes are the pressure-pain threshold (PPT) and the short form health survey (SF-12), which will be at baseline, and 4 and 8 weeks. These measures are routinely used in Physical Therapy practice.
2.9.3. Numeric Pain Scale (NPS)
NPS is a single 11-point numeric scale (with 0 as “no pain” and 10 as the “worst imaginable pain”) to measure pain intensity in adults (Hawker 2011) [
29]. It allows patients to measure their level of pain accordingly using a whole number (0–10 integers) that corresponds to their pain intensity (Rodriguez, 2001) [
30]. The scale is considered reliable (accurate and consistent), responsive (able to detect clinically significant changes) and valid (actually measures what it sets out to) (Hawker, 2011) [
29]. Accordingly, a pain reduction of 2 points, or 30%, on the NPS scores is defined as the minimal clinically important difference (MCID) (Childs et al., 2005; Farrar et al., 2001) [
31,
32]. The NPS is relatively easy to comprehend, and to apply, especially by patients with musculoskeletal disorders such as MPS (Hawker, 2011) [
29].
2.9.4. Neck Disability Index (NDI)
This is the most commonly used self-rated disability score for assessing patients with neck pain according to Vernon and Mior (1991) [
33]. It consists of ten domains: pain intensity, personal care, lifting, reading, headaches, concentration, work, driving, sleeping and recreation. Each question contains six answer choices, scored from 0 (no disability) to 5 (complete disability). All sections are then totalled. Scoring is reported on a 0–50 scale, 0 being the best possible score and 50 being the worst. The score can also be reported as a percentage (0–100%). The minimum detectable change (90% confidence) is 5 points or 10% points [
33] from Vernon and Mior (1991), and the MCID is in the range of 3.5–5.0 points (Pool et al., 2007) [
34].
2.9.5. Pressure Pain Threshold (PPT)
This will be measured using a digital algometer, and pain score measurement will be performed with digital palpation. The algometer circular flat tip with a 1.0 cm
2 surface will be slowly pushed vertically onto the skin over the area of the trigger point/s until the participant interprets the compression on skin as a pain sensation. The exerted pressure will be enlarged at a rate of 1 kg/cm
2. Participants will be requested to inform the treating Physiotherapist by saying “yes” when the pain is perceived. The measurements will be repeated three times with 40 s intervals, and the mean average value will be recorded (Fischer, 1998) [
35]. A mean difference of 0.94 kg/cm
2 in PPT is defined as MCID (Asiri et al., 2020) [
36].
2.9.6. Quality of Life (QoL)
Quality of life status will be evaluated using the short-form SF-12, which is a shorter version of the SF-36 questionnaire. The health survey (SF-12) questionnaire consists of 12 items regarding the quality of life with respect to physical and emotional aspects. Likert scales and yes/no options were used to assess function and wellbeing on this 12-item questionnaire. To score the SF-12, scales are standardised with a scoring algorithm to obtain a score ranging from 0 to 100. Higher scores indicate better health status. SF-12 is one of the most widely used patient outcome reports for musculoskeletal patients with well-documented high validity, reliability and responsiveness rate among many groups varying by age, sex, socio-economic status, geographical region and clinical conditions (Ware et al., 2000, Ware et al., 1996) [
37,
38]. This questionnaire has been translated into a Saudi version, with high reliability and validity scores (Haddad et al., 2021) [
39]. A minimal improvement of 20% in SF-36 scores was defined as MCID by Lauche et al. (2013) [
40].
2.9.7. Follow-Up Assessment
Potential participants will be assessed three times during the study period, at 0 (baseline), 4 and 8 weeks. This will allow inferences to be drawn about immediate and short-term effects. The 8 week timeframe is common in normal clinical practice. Follow-up assessments will be carried out by a member of staff (who is not involved in the patient’s treatment and is blinded to the baseline measurement and group allocation) at 4 and 8 weeks. These timeframes are normal clinical practice and consistent with previous authors (Luan et al., 2019; Eftekharsadat et al., 2020) [
9,
41].
2.10. Blinding
The blinded assessor—a member of staff who can speak both English and Arabic (who is not involved in the patient’s treatment and is blinded to the baseline measurement and group allocation) will collect the outcomes at 4 and 8 weeks. Where necessary, response rate will also be facilitated through a call reminder on up to two occasions each time to ask if they wish to complete the questionnaires. The statistician conducting the primary data analysis will also be blinded to the group allocation.
Potential participants will be blinded to the treatment allocation. They will not know if they are receiving the experimental or sham (placebo) treatment. However, it is not possible for the treating Physiotherapists to be blinded to treatment allocation with this design because they already know what the experimental and sham (placebo) treatment is. However, they do not control which patient they treat because of the concealed random allocation of potential participants.
2.11. Loss to Follow-Up
This study is likely to last for 12 months; therefore, at 4 months, a review of the rate of loss to follow-up will be undertaken to ensure that this does not affect the findings of the study. For example, if the rate of loss to follow-up is much higher in one group compared with the other, the researcher might consider over-enrolling into that group. Patients who are lost to follow-up will be included in the analysis based on intention to treat (ITT).
2.12. Data and Treatment Fidelity
The Physiotherapists who will be providing the treatments are skilled, trained and experienced in the management of MPS using radial shockwaves. To ensure the procedural integrity of the study, the assessment and treatment given to potential participants from the RCT will be evaluated by the principal investigator (CO). Standardised training on the study procedure will also be provided to the treating Physiotherapists to facilitate successful delivery of both treatments. Administrative staff involved in the study will receive training on the study protocol. Some of the treatment sessions from both groups of the study will be observed and documented, and feedback will be provided to the treating Physiotherapists. The radial shockwave machines for this study will have passed their normal regular checks to ensure they are properly calibrated and working well. Participants will be randomly selected and interviews will be conducted 3 months after their initial treatment to obtain their views on the care they received.
2.13. Statistical Considerations
2.13.1. Sample Size Calculations
Sample size calculations will be based on works by [
17,
42] Aktürk et al., (2018) and Gur et al., (2014). We estimated the minimal clinically important difference (MCID) to be a change in NPS of 2 points, at 90% power, with a statistical significance level of 5% and a standard deviation of 4.35 points. Using these figures, a sample of 96 participants is estimated for the study. However, to account for a 20% rate of loss at follow-up, this study will include 120 participants. Therefore, each study group will have 60 participants.
2.13.2. Non-Response and Intention to Treat Analysis
Participants who withdraw from the study will be included in the analysis based on intention to treat (ITT). ITT analysis, therefore, helps to prevent two major issues, noncompliance and missing data, that are associated with RCT (Gupta, 2011) [
43]. The ITT analysis takes into account all randomised patients in the groups to which they were randomly assigned, regardless of their adherence to the entry criteria, treatment they actually received and subsequent withdrawal from treatment or deviation from the study protocol (Kruse et al., 2002; Gupta, 2011) [
43,
44].
2.14. Plan of Analysis
All analyses will be undertaken on an ITT basis. All data will be analysed using the BM SPSS Statistics version 20 (SPSS Inc., Chicago, IL, USA). Descriptive statistics such as mean age, gender and duration of symptoms will be used to describe patients’ baseline characteristics. The results of the outcome measures will give a difference in scores from the baseline to 4 and 8 weeks. Normality will also be checked using the Shapiro–Wilk test since the sample size is 120. The chi-square test will be used to compare the distribution of categorical variables. We will use a paired sample t test for analysing within-group difference, and an independent sample t test for analysing between-group difference. A regression model will be used to evaluate the contribution of participants’ baseline characteristics such as age, gender and symptom duration. The significance level is set at p ≤ 0.05 with a 95% confidence interval to detect a minimal clinically important difference of 2 points between the groups receiving shockwave therapy and sham (placebo) treatment.
2.15. Ethical Considerations
Approval was obtained from the Research Ethics Committee (REC), and this study has been registered on clinicaltrials.gov. Written informed consent, a prerequisite for study participation, will be obtained from all participants. Potential participants will be given the opportunity to determine if they wish to participate in the study or not. The relevance of the research, including the possible risks and benefits, will be carefully explained to them. This is to enable participants to give informed consent based on an understanding that their participation in this research is voluntary.
Potential participants will be informed that they are not obliged to take part in the study and that failure to provide consent or withdrawal of consent without giving a reason will not affect the treatment that they will receive. All participants’ details, as well as their comments, will be kept secure and confidential at all times using a locked cabinet (with controlled access) and on a password-protected computer. Any information they provide to the principal investigator will be anonymised using pseudonyms and unique identifying numbers so that it will not be possible to identify them. Dictaphone recordings of interviews will be destroyed once they have been transcribed, and transcripts will be stored in a locked cabinet (with controlled access) and on a password-protected computer.
No significant adverse reactions are anticipated in the study, but these will be monitored and recorded by the department’s ethics committee lead. Participants will be informed that their physician will be informed of their participation in the study and after obtaining consent from them to do so, the patient’s family physician will be informed of their patient’s participation in the study via a letter. If a participant is feeling distressed or uncomfortable during the trial, they will be advised to consult their family physician and will be excluded from the study, but any data collected up to that point will be included in the analysis.
Potential participants will be informed that there are no direct personal benefits to them taking part in this study. However, the information derived from the study will help clinicians to know which of the two treatment methods is better for treating patients with MPS in the neck and upper back region in the future. Potential participants will be informed that they will be offered radial shockwave or sham (placebo) and each group will receive the usual PT treatments associated with this condition in addition. Both groups will receive the usual care such as education, advice and exercise prescriptions that are usually associated with MPS. However, all exercise will be performed at a speed and intensity that is within participant’s own control.
2.16. Phase 2
Design: Qualitative Semi-Structured Approach
A semi-structured telephone interview approach will be used as the design. This will lead to obtaining data that will enhance the understanding of experiences of potential participants about their symptom relief or aggravation after treatment (Mason, 2017; Coombes et al., 2009) [
45,
46]. This will occur towards the end of phase 1 of the quantitative study. Therefore, data collection will be by means of a semi-structured telephone interview method.
Purposive convenience sampling as suggested by Patton (2002) [
47] will be used to identify potential participants from those who have participated in phase 1 of the randomised controlled study and have agreed to being contacted for interview. This sampling strategy is a positive feature of qualitative study because it is flexible and allows research to develop as the data are collected and analysed simultaneously (Patton, 2002) [
47]. Twenty potential participants, ten each from the radial shockwave and sham (placebo) groups, will be recruited by the principal investigator to participate in the telephone interview. They will be potential participants with different demographics such as gender, ages and socio-economic backgrounds to provide a broad understanding of the topic being studied (Patton, 2002) [
47]. The interview details will include the lived experience of participants receiving radial shockwave or sham (placebo) treatment in addition to the standard PT treatment.
The duration of the interview is expected to be a maximum of 20–30 min, and this will be explained to the participants. Interviews will be Dictaphone-recorded with the consent of the interviewee, and field notes will be taken by the telephone interviewer assessor to contextualise the data (Mason, 2017) [
45]. All data will be anonymised, transcribed verbatim and stored securely in a cabinet (with controlled access) and on a password-protected computer.
The thematic analysis approach reported by Sandelowski and Barroso (2007) [
48] will be used to analyse the qualitative interviews. Data (transcribed interviews) will be initially analysed using computer software package MAXQDA. The analytic process will involve the following three stages: (1) extraction of initial interview findings and coding of findings of each interview, (2) grouping of findings (codes) according to similar themes and (3) abstraction of findings—analysing the grouped findings to identify associated patterns, overlaps and main themes that conceptualise all the findings.

 ,
, 

{kind=link}