1. Introduction
Influenza is the primary cause of influenza-like illness (ILI), presenting signs and symptoms such as headache, fever, sore throat, chills, cough, sneezing, runny nose, and body aches. Cases range from mild symptoms with spontaneous resolution to severe cases requiring hospitalization and potentially leading to death. The circulation of influenza virus strains is seasonal, and annually, the World Health Organization, in collaboration with over 100 countries, collects epidemiological data on the circulation of influenza virus strains in the northern and southern hemisphere [
1]. These data guide the composition of vaccines that have been providing protection against the predominant circulating influenza strains for years. Currently, there are two vaccine formulations against influenza: (1) the trivalent vaccine, containing two types of influenza type A and one of influenza type B, and (2) the quadrivalent vaccine, which adds another strain of influenza type B to this composition [
2]. In the public healthcare system from Brazil, under the National Immunization Program (PNI), the trivalent vaccine is administered to the priority group which includes children aged 6 months to under 5 years old, the elderly, pregnant women, postpartum women, teachers, healthcare professionals, indigenous people, individuals with comorbidities, people with permanent disabilities, security and rescue personnel, armed forces, truck drivers, public transportation workers, port workers, prison system employees, incarcerated populations, and young people aged 12 to 21 years under socioeducational measures. The quadrivalent vaccine is available in the private healthcare sector and is recommended for all individuals above 6 months of age [
3].
In 2019, SARS-CoV-2 emerged as the primary cause of severe acute respiratory illnesses, straining the healthcare system, originating the COVID-19 pandemic. Due to the similarity in the signs and symptoms of influenza and COVID-19 [
4], the need for influenza prevention and the reduction of influenza circulation through vaccination became even more evident [
5]. In the present study, we assessed the adherence to the quadrivalent vaccine in a private company in Belo Horizonte from the year 2019, in the prepandemic scenario, to the year 2021, post-pandemic. Thus, our aim is to examine the kinetics of demand for a vaccine that provides greater protection in a context of widespread circulation of viruses causing ILI. Moreover, based on the analyzed cohort and the wealth of information in the company’s database, we hope to elucidate whether there has been a change in the profile of vaccinated people during the evaluated period.
2. Methods
A quantitative analytical cross-sectional study was conducted. No volunteers were individually identified at any stage of the study; only the registration number assigned at the time of vaccination was used to ensure that the data would not be assessed duplicatively. The sample consisted of 36,478 individuals who, by spontaneous demand, were vaccinated against influenza with the quadrivalent vaccine at the VACSIM vaccination clinic in Belo Horizonte, Minas Gerais, Brazil. All participants from January 2019 to December 2021 were collected from the company’s database. The variables subjected to analysis included the date of vaccination (month, year), the age, and the gender of the volunteers. Categorical variables were presented as absolute and relative frequencies, while numeric variables were expressed as mean +/− standard deviation and median. Associations between variables and vaccination uptake were assessed using the chi-square test. The analyses were conducted using R software version 4.3.2, with a significance level of 5% and a p-value < 0.001 indicating high data reliability.
3. Results
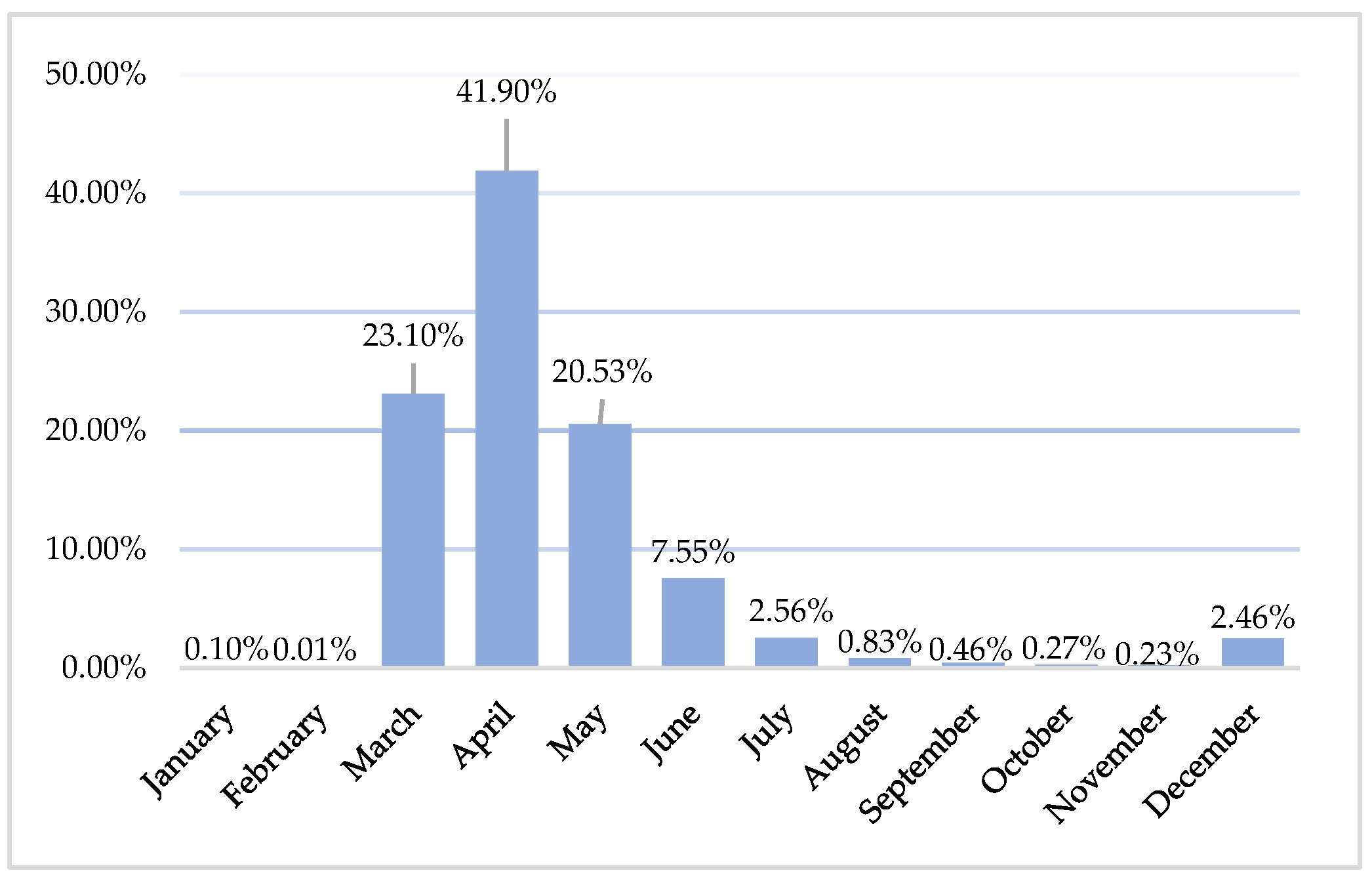
A total of 36,589 records were initially collected from the VACSIM company’s database, pertaining to individuals who voluntarily received the quadrivalent influenza vaccine during the corresponding period from January 2019 to December 2021. We excluded 37 duplicate records and 74 records from participants for whom the date of birth was not adequately documented in the company’s database for the three years under study. Thus, a total of 36,478 records were analyzed, with 10,924 (29.9%) from the year 2019, 12,370 (33.9%) from the year 2020, and 13,184 (36.2%) from 2021. The results reveal a progressively increasing trend in vaccination adherence, with a 20.69% increase between 2019 and 2021. When considering the cumulative number of vaccines administered over the three-year period, there is a prominent concentration of vaccinations in the month of April (41.9%) (
Figure 1). Conversely, the months with the lowest vaccination rates were January (0.01%) and February (0.1%), followed by October (0.27%) and November (0.23%). The combined total of all these months corresponds to 0.61% of the total sample for the three years under study.
3.1. Analysis by Year
When evaluating each year separately, it becomes evident that the highest percentage of adherence consistently occurs in April, with rates of 35% in 2019, 46% in 2020, and 43.8% in 2021 (
Table 1). The timeframe from March to May encompasses the majority of immunizations administered, accounting for 81%, 96.9%, and 79.3% of the total vaccines distributed in the years 2019, 2020, and 2021, respectively.
In the later months, a notable decrease in vaccination rates was observed, with the exception of December 2021, which saw a significant increase to 6.3% of influenza immunizations. This shift in vaccine demand kinetics represents a noteworthy change when comparing the three years (
Table 1).
3.2. Analysis by Age and Sex
Regarding the characteristics of the research participants, the study encompassed an average age of 43.41 years, with a standard deviation of 55.17. Upon consolidating data from the three years, it became evident that the predominant age group fell within the range of 40 and 59 years, constituting 33.4% of the sample. Conversely, the younger population, aged 10 to 19 years, displayed the lowest representation in the overall vaccine cohort, comprising only 9.3% of the participants. Our data also reveal a female predominance in the total sample, with 54% of the participants. When stratifying by age and gender, it becomes evident that the age group below 19 years exhibits a higher percentage of males, whereas from the age of 20 onwards, a higher percentage of females is observed (
Table 2).
When analyzing age groups for each year individually, a shift in the age groups exhibiting lower vaccine adherence became apparent. In 2019 and 2021, the age group of 10 to 19 years consistently demonstrated the lowest demand for the quadrivalent influenza vaccine, with rates of 9.4% and 7.8%, respectively. Meanwhile, in 2020, the lowest adherence was observed among those under 10 years of age (9.6%). Nevertheless, across all three years assessed, including when segmented annually, the age group of 40 to 59 years exhibited the highest demand for the vaccine, with rates of 32.8% in 2019, 35% in 2020, and 34.8% in 2021.
3.3. Variation in COVID-19 Cases with the Influenza Vaccination Period
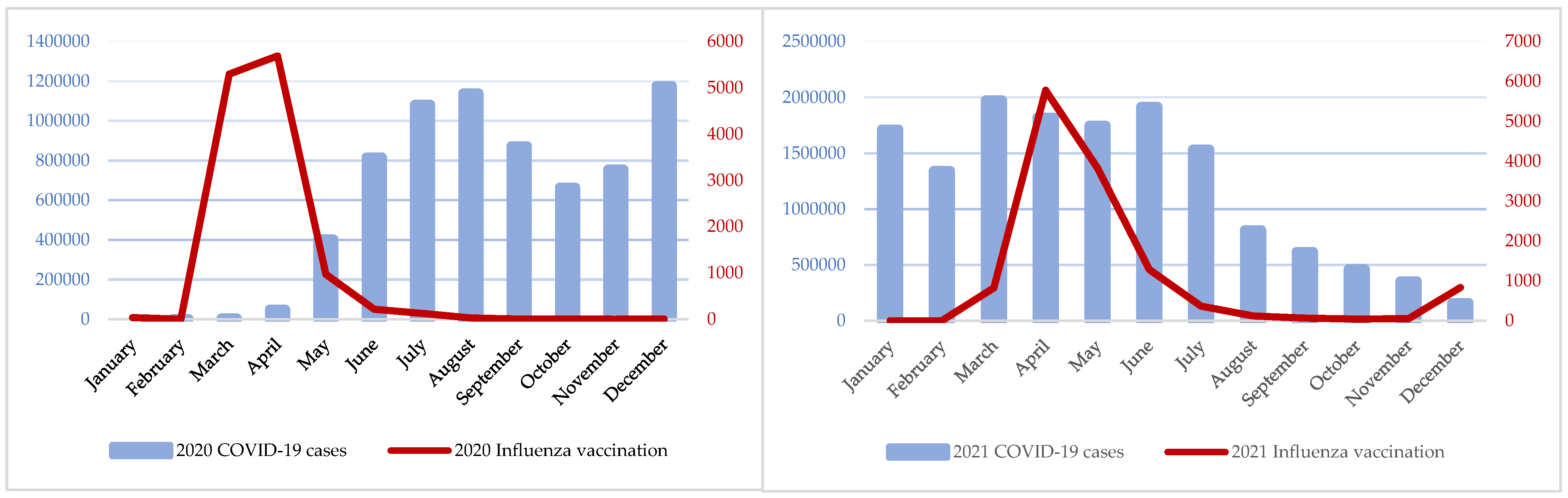
We also assessed the correlation between influenza vaccination within the specified cohort and the monthly notifications of COVID-19 cases in Brazil. the country-initiated weekly epidemiological reporting of the disease in March 2020, coinciding with the first confirmed case in Belo Horizonte on 16 March 2020 [
6]. Concurrently, there was a concomitant increase in influenza vaccination during the same period, with a consistent ascent culminating in the annual peak in April, constituting 46% of the total vaccinations for the year. From May 2020 onwards, vaccination rates began to decline, a trend that persisted until the end of the year when there was a stabilization in the number of new COVID-19 cases within the country. Throughout the year under analysis [
5], there was an approximate monthly average of 622,150 new cases of the disease [
7] (
Figure 2).
In 2021, Brazil experienced a surge in new COVID-19 cases, with a stabilization of the high scenario, especially in the first half of the year. The country recorded an average of approximately 6941 new cases of the disease per 100,000 habitants in the same year [
5]. Concurrently, there was an uptick in the number of influenza vaccinations during the same period compared to the previous year, reaching its peak again in April. However, there was increased vaccination adherence in the subsequent months, particularly in May and June, when compared to the previous year (
Figure 2).
Table 3.
Total vaccination by age in 2019, 2020, and 2021.
Table 3.
Total vaccination by age in 2019, 2020, and 2021.
| AGE | 2019, N = 10,924 1 | 2020, N = 12,334 | 2021, N = 13,182 | TOTAL | p 2 Value |
|---|
| <10 years | 1392 (12.7%) | 1180 (9.6%) | 1538 (11.6%) | 4110 (11.3%) | <0.001 |
| 10 to 19 years | 1029 (9.4%) | 1331 (10.8%) | 1037 (7.8%) | 3397 (9.3%) | |
| 20 to 39 years | 1964 (18.1%) | 2139 (17.3%) | 3627 (27.5%) | 7730 (21.2%) | |
| 40 to 59 years | 3584 (32.8%) | 4311 (35.0%) | 4600 (34.8%) | 12,495 (34.3%) | |
| >60 years | 2955 (27.0%) | 3373 (27.3%) | 2396 (18.3%) | 8724 (23.9%) | |
| Total | 10,924 (30%) | 12,334 (34%) | 13,182 (36%) | N = 36,478 (100%) | |
4. Discussion
The findings of this study provide valuable insights into the dynamics of influenza vaccination in a private company in Belo Horizonte over three years (
Table 3). Several key trends and patterns emerged from the analysis, shedding light on the factors influencing vaccination rates and the impact of external factors, such as the COVID-19 pandemic, on the demand for influenza vaccination.
The decline in influenza vaccination rates in Brazil in 2019, as reported in previous studies [
7], was met with a drastic shift in 2020 due to the emergence of the COVID-19 pandemic. The similarities in transmission modes and clinical manifestations between SARS-CoV-2 and influenza heightened the importance of influenza prevention, especially in the absence of a COVID-19 vaccine [
8]. This urgency likely contributed to the successive increases in influenza vaccination adherence observed in 2019 (29.9%), 2020 (33.9%), and 2021 (36.1%). Our findings align with the existing literature, emphasizing the strategic importance of timing in vaccination campaigns [
9,
10].
A consistent seasonal trend in influenza vaccination was observed, marked by a surge in demand from March to May, corresponding to the preseasonal period for influenza in Brazil. This trend aligns with the national influenza vaccination campaigns and reflects public awareness and preparedness before the peak influenza season. This pattern underscores the need for agile public health responses, capitalizing on heightened awareness and readiness among the populace before the influenza season peaks. A noteworthy deviation occurred in December 2021, marked by an unusual increase in vaccination. This anomaly could be attributed to the emergence of the H3N2 strain, named Darwin, coupled with the relaxation of COVID-19 restrictions and the lack of influenza vaccine coverage for infected individuals [
11,
12]. This exceptional circumstance underscores the intricate interplay between emerging strains, public health policies, and vaccination strategies, highlighting the need for adaptable approaches in the face of evolving infectious disease scenarios.
Our study illuminates significant trends in demographic disparities concerning vaccine adherence. Adults aged 40 to 59 exhibited heightened demand, likely due to their sustained presence in workplaces during the pandemic, potentially increasing their perception of vulnerability and the need for preventive measures. Additionally, the Ministry of Health’s expanded vaccination campaign likely played a role in encouraging this age group to get vaccinated [
13,
14]. Conversely, the lower vaccine coverage observed among the young population (10 to 19 years) indicates a diminished perception of COVID-19 risk and the necessity for prevention. This finding highlights a critical gap that demands focused interventions to enhance awareness and understanding of the risks associated with influenza and COVID-19 [
14]. The demographic disparities in vaccine uptake identified in our study echo the challenges elucidated by Larson et al. (2014) and Opel et al. (2015). Addressing vaccine hesitancy, especially among younger age groups, remains a persistent challenge. Our study reinforces the urgent need for tailored interventions, leveraging sociobehavioral research and communication strategies to bridge the knowledge–action gap [
15,
16].
Analysis by gender revealed a predominant participation of females (54%), indicating a heightened concern among women for preventive health measures. This gender disparity, well-documented in the literature, is attributed to women’s greater access to preventive healthcare services [
17]. Females exhibited superior adherence across age groups, likely contributing to their lower mortality from COVID-19 compared to males. In contrast, males led in vaccination adherence among the younger age group, reflecting the demographic composition of the younger Brazilian population [
18]. Addressing these gender-specific patterns is vital for tailoring public health campaigns effectively.
Examining all the periods under study, a distinct concentration of vaccines was observed in April (41.9%), which coincides with the company’s second month of the influenza vaccination campaign. Notably, in April 2020, the highest number of new COVID-19 cases since the beginning of the pandemic was recorded according to the epidemiological bulletins of the Municipality of Belo Horizonte [
19]. In response, rigorous preventive measures were implemented, including municipal laws and campaigns for social distancing, mask-wearing in public places, closure of businesses, and penalties for those who violated the measures imposed through official decrees [
20]. The interplay between influenza vaccination and the COVID-19 pandemic, highlighted in our findings, resonates with recent studies. Notably, the study by Bartsch et al. (2021) emphasizes the importance of integrated vaccination strategies during pandemics [
21]. Our research extends this understanding by illustrating how heightened awareness of respiratory illnesses during the COVID-19 pandemic influenced influenza vaccine uptake. This underscores the interconnectedness of public health responses and emphasizes the value of leveraging ongoing health crises to promote broader vaccination initiatives [
21]. Our findings have significant policy implications, aligning with the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC) recommendations. Tailored interventions, informed by behavioral insights, should be prioritized, focusing on educational initiatives, community engagement, and innovative communication campaigns. Furthermore, longitudinal studies, akin to the work conducted by Smith et al. (2019), should be encouraged to assess the long-term impact of these interventions on vaccination behavior and public health outcomes [
22].
A potential limitation lies in the specific start date of the influenza vaccination campaign in the private sector, possibly influencing the concentrated immunizations in certain months [
23]. Future studies should incorporate additional years of influenza vaccination data, considering the evolving COVID-19 situation, to assess if vaccination demand remains elevated post-pandemic or reverts to prepandemic levels. Long-term analyses can provide valuable insights into the sustained impact of COVID-19 on influenza vaccination behavior. Our study underscores the intricate interplay between pandemics, public health measures, fear perception, and vaccine adherence. By understanding these complexities, public health campaigns can be tailored to address specific demographic needs, ensuring comprehensive coverage and preparedness against both influenza and emerging infectious diseases.




{kind=link}
{kind=link}

