
Amelioration of Glioblastoma Multiforme via the Combination of Simulated Microgravity and Oncolytic Viral Therapy †



{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results and Discussion
3.1. Simulated Microgravity Effects on Tumor Cells
3.1.1. Simulated Microgravity Effects on Glioblastoma Multiforme
3.1.2. Simulated Microgravity Effects on Thyroid Cancer Cells
3.2. Oncolytic Viral Therapy
3.2.1. Parvovirus and Glioblastoma Multiforme
3.2.2. Reovirus, Measles Virus, and Pancreatic Cancer
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 3D | Three-dimensional |
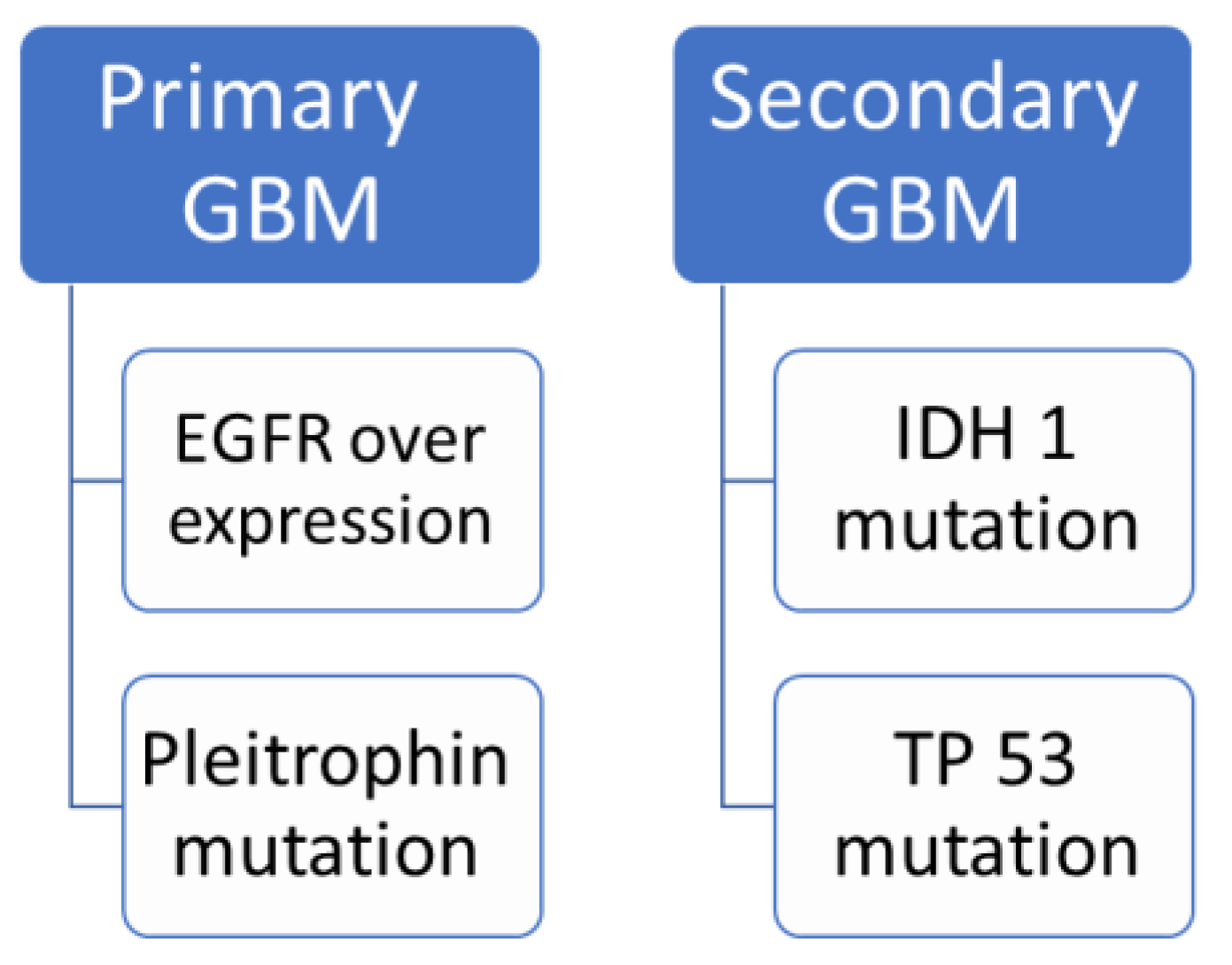
| EGFR | Epidermal growth factor receptor |
| GBM | Glioblastoma multiforme |
| INF | Interferon |
| RIG-1 | Retinoic acid-inducible gene 1 |
| TMZ | temozolimide |
| TNF | Tumor necrosis factor |
| TRAF3 | TNF receptor-associated factor 3 |
| TRAIL | TNF-related apoptosis-inducing ligand |
References
- Ostrom, Q.T.; Price, M.; Neff, C.; Cioffi, G.; Waite, K.A.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2015–2019. Neuro. Oncol. 2022, 24 (Suppl. S5), v1–v95. [Google Scholar] [CrossRef] [PubMed]
- D’Alessio, A.; Proietti, G.; Sica, G.; Scicchitano, B.M. Pathological and Molecular Features of Glioblastoma and Its Peritumoral Tissue. Cancers 2019, 11, 469. [Google Scholar] [CrossRef] [PubMed]
- Ryskalin, L.; Biagioni, F.; Morucci, G.; Busceti, C.L.; Frati, A.; Puglisi-Allegra, S.; Ferrucci, M.; Fornai, F. Spreading of Alpha Synuclein from Glioblastoma Cells towards Astrocytes Correlates with Stem-like Properties. Cancers 2022, 14, 1417. [Google Scholar] [CrossRef] [PubMed]
- Elshourbagy, T.; Brašić, J.R.; Syed, A.B. Guidelines for the Diagnosis and Treatment of Parkinson’s Disease. Biol. Life Sci. Forum 2021, 9, 9. [Google Scholar] [CrossRef]
- Elshourbagy, T.; Syed, A.B.; Amer, M.A.M.; Brasic, J.R. Precision medicine to identify optimal diagnostic and therapeutic interventions for Parkinson’s Disease. Med. Sci. Discov. 2021, 8, 514–519. [Google Scholar] [CrossRef]
- Yong, R.L.; Lonser, R.R. Surgery for Glioblastoma Multiforme: Striking a Balance. World Neurosurg. 2011, 76, 528–530. [Google Scholar] [CrossRef]
- Barani, I.J.; Larson, D.A. Radiation Therapy of Glioblastoma. In Cancer Treatment and Research; Springer International Publishing: Cham, Switzerland, 2015; pp. 49–73. [Google Scholar]
- Fernandes, C.; Costa, A.; Osório, L.; Lago, R.C.; Linhares, P.; Carvalho, B.; Caeiro, C. Glioblastoma; Chapter 11 Current Standards of Care in Glioblastoma Therapy; Creative Commons: Mountain View, CA, USA, 2017; pp. 197–241. [Google Scholar] [CrossRef]
- Carter, T.C.; Medina-Flores, R.; Lawler, B.E. Glioblastoma treatment with temozolomide and bevacizumab and overall survival in a rural tertiary healthcare practice. BioMed Res. Int. 2018, 2018, 1–10. [Google Scholar] [CrossRef]
- Topal, U.; Zamur, C. Microgravity, Stem Cells, and Cancer: A New Hope for Cancer Treatment. Stem Cells Int. 2021, 2021, 1–9. [Google Scholar] [CrossRef]
- Takeda, M.; Magaki, T.; Okazaki, T.; Kawahara, Y.; Manabe, T.; Yuge, L.; Kurisu, K. Effects of simulated microgravity on proliferation and chemosensitivity in malignant glioma cells. Neurosci. Lett. 2009, 463, 54–59. [Google Scholar] [CrossRef]
- Svejgaard, B.; Wehland, M.; Ma, X.; Kopp, S.; Sahana, J.; Warnke, E.; Aleshcheva, G.; Hemmersbach, R.; Hauslage, J.; Grosse, J.; et al. Common Effects on Cancer Cells Exerted by a Random Positioning Machine and a 2D Clinostat. PLoS ONE 2015, 10, e0135157. [Google Scholar] [CrossRef]
- Warnke, E.; Pietsch, J.; Wehland, M.; Bauer, J.; Infanger, M.; Görög, M.; Hemmersbach, R.; Braun, M.; Ma, X.; Sahana, J.; et al. Spheroid formation of human thyroid cancer cells under simulated microgravity: A possible role of CTGF and CAV. Cell Commun. Signal. 2014, 12, 1–11. [Google Scholar] [CrossRef]
- Kopp, S.; Krüger, M.; Bauer, J.; Wehland, M.; Corydon, T.J.; Sahana, J.; Nassef, M.Z.; Melnik, D.; Bauer, T.J.; Schulz, H.; et al. Microgravity affects thyroid cancer cells during the TEXUS-53 mission stronger than hypergravity. Int. J. Mol. Sci. 2018, 19, 4001. [Google Scholar] [CrossRef] [PubMed]
- Grimm, D.; Bauer, J.; Kossmehl, P.; Shakibaei, M.; Schönberger, J.; Pickenhahn, H.; Schulze-Tanzil, G.; Vetter, R.; Eilles, C.; Paul, M.; et al. Simulated microgravity alters differentiation and increases apoptosis in human follicular thyroid carcinoma cells. FASEB J. 2002, 16, 604–606. [Google Scholar] [CrossRef] [PubMed]
- Grimm, D.; Wehland, M.; Pietsch, J.; Aleshcheva, G.; Wise, P.; van Loon, J.; Ulbrich, C.; Magnusson, N.E.; Infanger, M.; Bauer, J. Growing tissues in real and simulated microgravity: New methods for tissue engineering. Tissue Eng. Part B Rev. 2014, 20, 555–556. [Google Scholar] [CrossRef] [PubMed]
- Krüger, M.; Melnik, D.; Kopp, S.; Buken, C.; Sahana, J.; Bauer, J.; Wehland, M.; Hemmersbach, R.; Corydon, T.J.; Infanger, M.; et al. Fighting thyroid cancer with microgravity research. Int. J. Mol. Sci. 2019, 20, 2553. [Google Scholar] [CrossRef]
- Grimm, D.; Kossmehl, P.; Shakibaei, M.; Schulze-Tanzil, G.; Pickenhahn, H.; Bauer, J.; Paul, M.; Cogoli, A. Effects of simulated microgravity on thyroid carcinoma cells. J. Gravit. Physiol. 2002, 9, P253–P256. [Google Scholar] [PubMed]
- Kaufman, H.L.; Kohlhapp, F.J.; Zloza, A. Oncolytic viruses: A new class of immunotherapy drugs. Nat. Rev. Drug Discov. 2015, 14, 642–662. [Google Scholar] [CrossRef]
- Martuza, R.L.; Malick, A.; Markert, J.M.; Ruffner, K.L.; Coen, D.M. Experimental therapy of human glioma by means of a genetically engineered virus mutant. Science 1991, 252, 854–856. [Google Scholar] [CrossRef]
- Clemens, M.J. Targets and mechanisms for the regulation of translation in malignant transformation. Oncogene 2004, 23, 3180–3188. [Google Scholar] [CrossRef]
- McEntee, G.; Kyula, J.N.; Mansfield, D.; Smith, H.; Wilkinson, M.; Gregory, G.; Roulstone, V.; Coffey, M.; Harrington, K.J. Enhanced cytotoxicity of reovirus and radiotherapy in melanoma cells is mediated through increased viral replication and mitochondrial apoptotic signalling. Oncotarget 2016, 7, 48517–48532. [Google Scholar] [CrossRef]
- Geletneky, K.; Hajda, J.; Angelova, A.L.; Leuchs, B.; Capper, D.; Bartsch, A.J.; Neumann, J.-O.; Schöning, T.; Hüsing, J.; Beelte, B.; et al. Oncolytic H-1 parvovirus shows safety and signs of immunogenic activity in a first Phase I/IIa glioblastoma trial. Mol. Ther. 2017, 25, 2620–2634. [Google Scholar] [CrossRef] [PubMed]
- Hirano, S.; Etoh, T.; Okunaga, R.; Shibata, K.; Ohta, M.; Nishizono, A.; Kitano, S. Reovirus inhibits the peritoneal dissemination of pancreatic cancer cells in an immunocompetent animal model. Oncol. Rep. 2009, 21, 1381–1384. [Google Scholar] [CrossRef] [PubMed]
- Galanis, E. Therapeutic potential of oncolytic measles virus: Promises and challenges. Clin. Pharmacol. Ther. 2010, 88, 620–625. [Google Scholar] [CrossRef]
- Baertsch, M.A.; Leber, M.F.; Bossow, S.; Singh, M.; Engeland, C.E.; Albert, J.; Grossardt, C.; Jäger, D.; von Kalle, C.; Ungerechts, G. MicroRNA-mediated multi-tissue detargeting of oncolytic measles virus. Cancer Gene Ther. 2014, 21, 373–380. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elshourbagy, T.; Brašić, J.R. Amelioration of Glioblastoma Multiforme via the Combination of Simulated Microgravity and Oncolytic Viral Therapy. Med. Sci. Forum 2023, 20, 9. https://doi.org/10.3390/IECC2023-14219
Elshourbagy T, Brašić JR. Amelioration of Glioblastoma Multiforme via the Combination of Simulated Microgravity and Oncolytic Viral Therapy. Medical Sciences Forum. 2023; 20(1):9. https://doi.org/10.3390/IECC2023-14219
Chicago/Turabian StyleElshourbagy, Tarek, and James Robert Brašić. 2023. "Amelioration of Glioblastoma Multiforme via the Combination of Simulated Microgravity and Oncolytic Viral Therapy" Medical Sciences Forum 20, no. 1: 9. https://doi.org/10.3390/IECC2023-14219