
Antimicrobial Consumption in England, 2017 to 2021 †
 ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Data and Data Sources
2.2. Data Processing and Statistical Analyses
3. Results
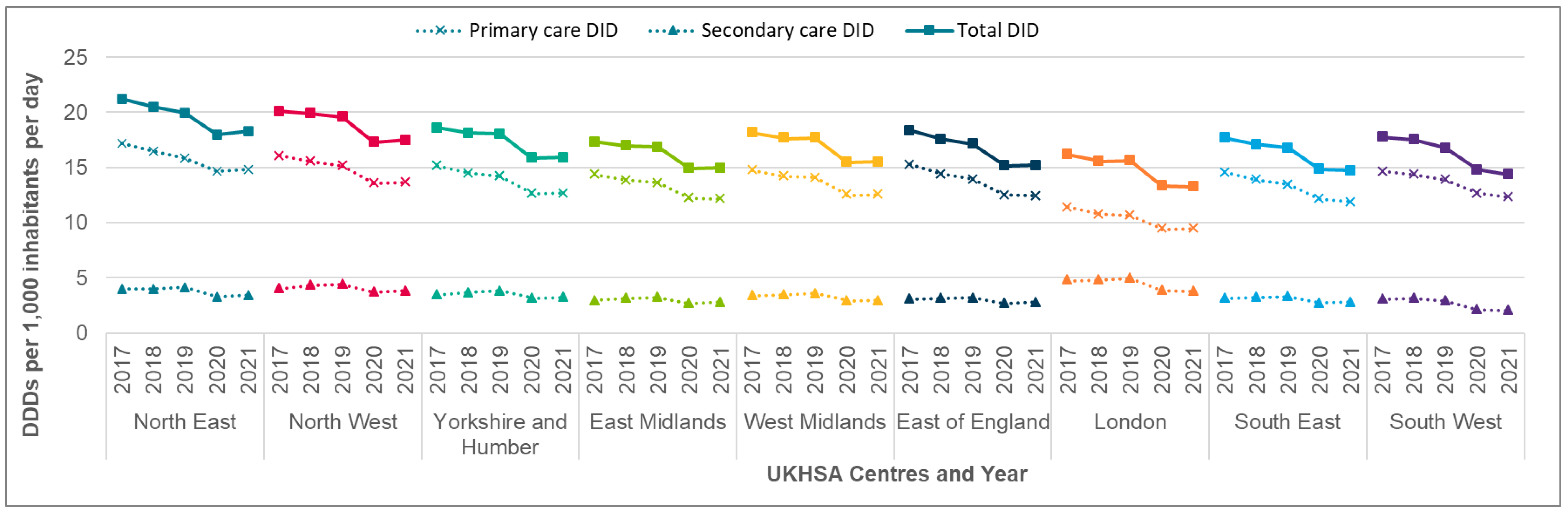
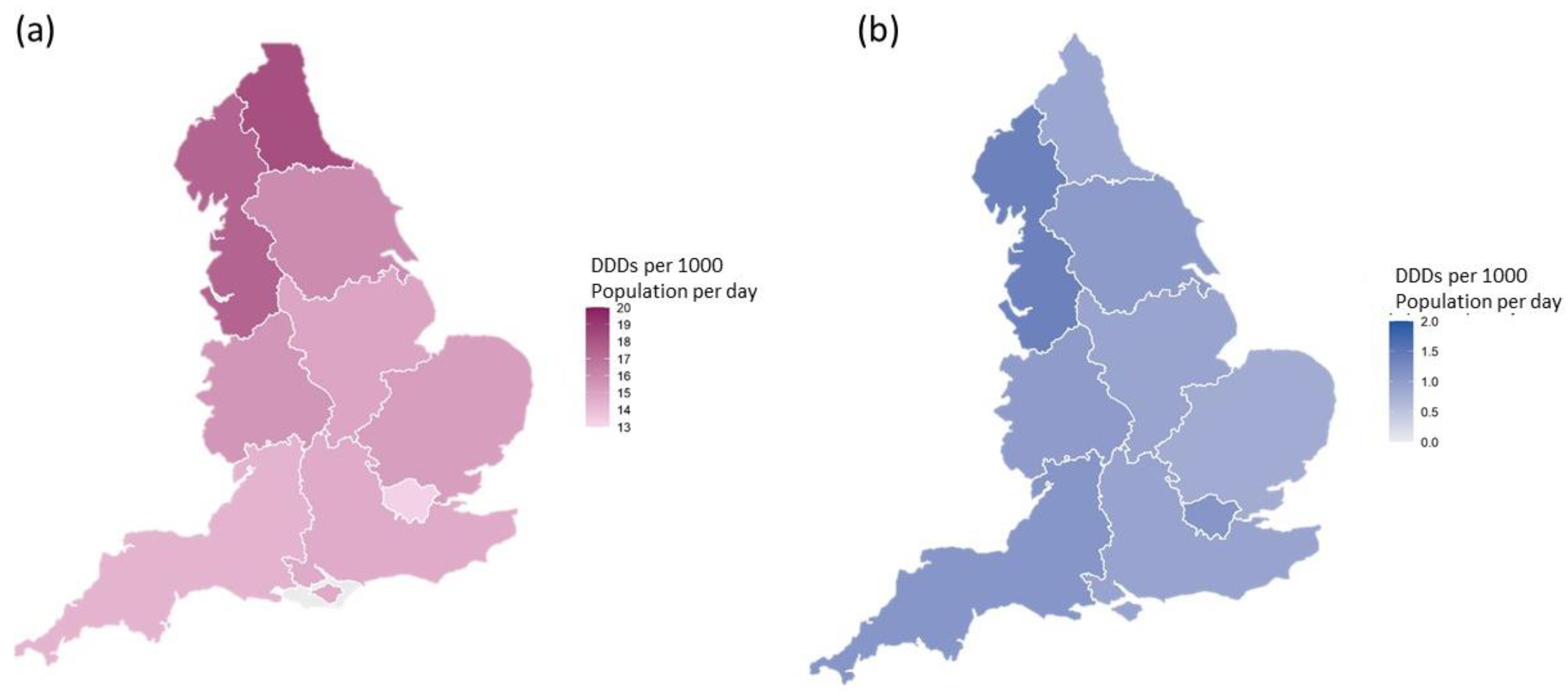
3.1. Total Antibiotic Consumption
3.1.1. Primary Care Antibiotic Consumption
3.1.2. Secondary Care Antibiotic Consumption
3.2. Antifungal Consumption
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mendelson, M.; Sharland, M.; Mpundu, M. Antibiotic resistance: Calling time on the ‘silent pandemic’. JAC Antimicrob Resist 2022, 4, dlac016. [Google Scholar] [CrossRef] [PubMed]
- UK 5-Year Action Plan for Antimicrobial Resistance 2019 to 2024; Department of Health and Social Care: London, UK, 2019.
- Ashiru-Oredope, D.; Susan Hopkins on behalf of the English Surveillance Programme for Antimicrobial Utilization and Resistance Oversight Group; Kessel, A.; Hopkins, S.; Ashiru-Oredope, D.; Brown, B.; Brown, N.; Carter, S.; Charlett, A.; Cichowka, A.; et al. Antimicrobial stewardship: English surveillance programme for antimicrobial utilization and resistance (ESPAUR). J. Antimicrob. Chemother. 2013, 68, 2421–2423. [Google Scholar] [PubMed]
- Bou-Antoun, S.; Falola, A.; Fountain, H.; Squire, H.; Brown, C.S.; Hopkins, S.; Gerver, S.M.; Demirjian, A. The English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report 2021 to 2022, Chapter 3 Antimicrobial Consumption; UK Health Security Agency: London, UK, 2022. [Google Scholar]
- Budd, E.; Cramp, E.; Sharland, M.; Hand, K.; Howard, P.; Wilson, P.; Wilcox, M.; Muller-Pebody, B.; Hopkins, S. Adaptation of the WHO Essential Medicines List for national antibiotic stewardship policy in England: Being AWaRe. JAC 2019, 74, 3384–3389. [Google Scholar] [CrossRef] [PubMed]
- Andrews, A.; Bou-Antoun, S.; Guy, R.; Brown, C.S.; Hopkins, S.; Gerver, S. Respiratory antibacterial prescribing in primary care and the COVID-19 pandemic in England, winter season 2020–21. JAC 2022, 77, 799–802. [Google Scholar] [CrossRef] [PubMed]
- Bou-Antoun, S.; Falola, A.; Fountain, H.; Squire, H.; Budd, E.; Brown, C.S.; Hopkins, S.; Gerver, S.M. The English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) report 2020 to 2021, Chapter 5 Antimicrobial Consumption; UK Health Security Agency: London, UK, 2021. [Google Scholar]
- Shah, S.; Wordley, V.; Thompson, W. How did COVID-19 impact on dental antibiotic prescribing across England? Br. Dent. J. 2020, 229, 601–604, Erratum in: Br. Dent. J. 2022, 232, 303–306. [Google Scholar] [CrossRef] [PubMed]
- The National Institute for Health and Care Excellence (NICE). Pneumonia (Hospital-Acquired): Antimicrobial Prescribing NICEguideline; NG139; UK Health Security Agency: London, UK, 2019. [Google Scholar]
- COVID-19 Rapid Guideline: Antibiotics for Pneumonia in Adults in Hospital; NG173; UK Health Security Agency: London, UK, 2020.
- UKHSA National Statistics: Annual Epidemiological Commentary: Gram-Negative, MRSA, MSSA Bacteraemia and C. Difficile Infections, up to and including Financial Year 2021 to 2022. Available online: https://www.gov.uk/search/research-and-statistics (accessed on 31 December 2022).
- Hatzl, S.; Reisinger, A.C.; Posch, F.; Prattes, J.; Stradner, M.; Pilz, S.; Eller, P.; Schoerghuber, M.; Toller, W.; Gorkiewicz, G.; et al. Antifungal prophylaxis for prevention of COVID-19-associated pulmonary aspergillosis in critically ill patients: An observational study. Crit. Care 2021, 25, 335. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bou-Antoun, S.; Falola, A.; Fountain, H.; Squire, H.; Brown, C.S.; Hopkins, S.; Gerver, S.M.; Demirjian, A. Antimicrobial Consumption in England, 2017 to 2021. Med. Sci. Forum 2022, 15, 1. https://doi.org/10.3390/msf2022015001
Bou-Antoun S, Falola A, Fountain H, Squire H, Brown CS, Hopkins S, Gerver SM, Demirjian A. Antimicrobial Consumption in England, 2017 to 2021. Medical Sciences Forum. 2022; 15(1):1. https://doi.org/10.3390/msf2022015001
Chicago/Turabian StyleBou-Antoun, Sabine, Angela Falola, Holly Fountain, Hanna Squire, Colin S. Brown, Susan Hopkins, Sarah M. Gerver, and Alicia Demirjian. 2022. "Antimicrobial Consumption in England, 2017 to 2021" Medical Sciences Forum 15, no. 1: 1. https://doi.org/10.3390/msf2022015001