
The Pharmacogenetics of Treatment with Quetiapine
 , , and
, , and 
Abstract
:1. Introduction
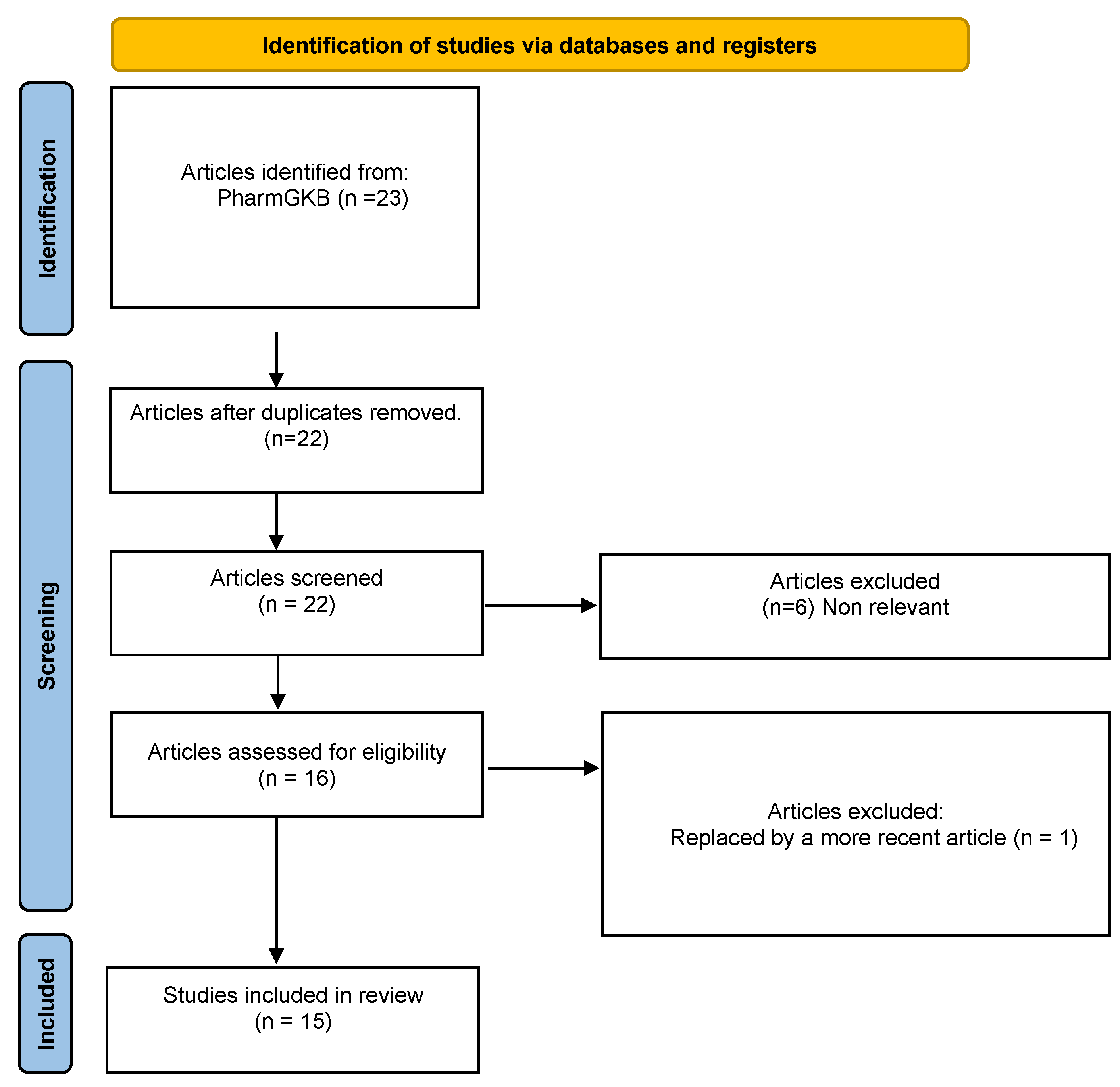
2. Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- FDA. Seroquel. Drug Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/020639s061lbl.pdf (accessed on 20 June 2022).
- Lalonde, C.D.; Van Lieshout, R.J. Treating Generalized Anxiety Disorder with Second Generation Antipsychotics: A Systematic Review and Meta-Analysis. J. Clin. Psychopharmacol. 2011, 31, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Poyurovsky, M.; Weizman, A. Quetiapine for Bipolar Depressive Episode in Obsessive-Compulsive Disorder Patients Maintained on Selective Serotonin Reuptake Inhibitor Treatment. Clin. Neuropharmacol. 2021, 44, 123–125. [Google Scholar] [CrossRef] [PubMed]
- DeVane, C.L.; Nemeroff, C.B. Clinical Pharmacokinetics of Quetiapine: An Atypical Antipsychotic. Clin. Pharmacokinet. 2001, 40, 509–522. [Google Scholar] [CrossRef] [PubMed]
- Zubiaur, P.; Fernández-Campos, P.; Navares-Gómez, M.; Soria-Chacartegui, P.; Villapalos-García, G.; Román, M.; Mejía-Abril, G.; Ochoa, D.; Abad-Santos, F. Variants in COMT, CYP3A5, CYP2B6, and ABCG2 Alter Quetiapine Pharmacokinetics. Pharmaceutics 2021, 13, 1573. [Google Scholar] [CrossRef]
- Hasselstrøm, J.; Linnet, K. IN VITRO STUDIES ON QUETIAPINE METABOLISM USING THE SUBSTRATE DEPLETION APPROACH WITH FOCUS ON DRUG-DRUG INTERACTIONS. Drug Metabol. Drug Interact. 2006, 21, 187–211. [Google Scholar] [CrossRef]
- López-Muñoz, F.; Álamo, C. Active Metabolites as Antidepressant Drugs: The Role of Norquetiapine in the Mechanism of Action of Quetiapine in the Treatment of Mood Disorders. Front. Psychiatry 2013, 4, 102. [Google Scholar] [CrossRef]
- Björkholm, C.; Jardemark, K.; Marcus, M.M.; Malmerfelt, A.; Nyberg, S.; Schilström, B.; Svensson, T.H. Role of concomitant inhibition of the norepinephrine transporter for the antipsychotic effect of quetiapine. Eur. Neuropsychopharmacol. 2013, 23, 709–720. [Google Scholar] [CrossRef]
- Flores-Rojas, L.E.; Hernández, L.A.G.-Z. Efectos secundarios metabólicos de los antipsicóticos de segunda generación. Med. Interna México 2019, 35, 721–731. [Google Scholar]
- The Royal Dutch Society of Pharmacology (KNMP) Dutch Pharmacogenetics Working Group (DPWG). Pharmacogenetics Guidelines. CYP2D6: Aripiprazole 2022. Available online: https://www.g-standaard.nl/risicoanalyse/B0001542.PDF (accessed on 1 July 2022).
- The Royal Dutch Society of Pharmacology (KNMP) Dutch Pharmacogenetics Working Group (DPWG). Pharmacogenetics Guidelines; CYP3A4: Quetiapine; Netherlands, 2022. Available online: https://www.g-standaard.nl/risicoanalyse/B0005991.PDF (accessed on 1 July 2022).
- Quetiapine. Available online: https://www.pharmgkb.org/chemical/PA451201/clinicalAnnotation (accessed on 5 July 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Xu, Q.; Wu, X.; Li, M.; Huang, H.; Minica, C.; Yi, Z.; Wang, G.; Shen, L.; Xing, Q.; Shi, Y.; et al. Association studies of genomic variants with treatment response to risperidone, clozapine, quetiapine and chlorpromazine in the Chinese Han population. Pharm. J. 2016, 16, 357–365. [Google Scholar] [CrossRef]
- Porcelli, S.; Balzarro, B.; Lee, S.-J.; Han, C.; Patkar, A.A.; Pae, C.-U.; Serretti, A. PDE7B, NMBR and EPM2A Variants and Schizophrenia: A Case-Control and Pharmacogenetics Study. Neuropsychobiology 2016, 73, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Crisafulli, C.; Chiesa, A.; Han, C.; Lee, S.-J.; Park, M.H.; Balzarro, B.; Andrisano, C.; Patkar, A.A.; Pae, C.-U.; Serretti, A. Case–control association study for 10 genes in patients with schizophrenia: Influence of 5HTR1A variation rs10042486 on schizophrenia and response to antipsychotics. Eur. Arch. Psychiatry Clin. Neurosci. 2012, 262, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Clark, S.L.; Souza, R.P.; Adkins, D.E.; Åberg, K.; Bukszár, J.; McClay, J.L.; Sullivan, P.F.; van den Oord, E.J.C.G. Genome-wide association study of patient-rated and clinician-rated global impression of severity during antipsychotic treatment. Pharmacogenet. Genom. 2013, 23, 69–77. [Google Scholar] [CrossRef]
- Campbell, D.B.; Ebert, P.J.; Skelly, T.; Stroup, T.S.; Lieberman, J.; Levitt, P.; Sullivan, P.F. Ethnic Stratification of the Association of RGS4 Variants with Antipsychotic Treatment Response in Schizophrenia. Biol. Psychiatry 2008, 63, 32–41. [Google Scholar] [CrossRef]
- Monteleone, P.; Milano, W.; Petrella, C.; Canestrelli, B.; Maj, M. Endocannabinoid Pro129Thr FAAH Functional Polymorphism But Not 1359G/A CNR1 Polymorphism Is Associated With Antipsychotic-Induced Weight Gain. J. Clin. Psychopharmacol. 2010, 30, 441–445. [Google Scholar] [CrossRef]
- López-Rodríguez, R.; Cabaleiro, T.; Ochoa, D.; Román, M.; Borobia, A.M.; Carcas, A.J.; Ayuso, C.; Novalbos, J.; Abad-Santos, F. Pharmacodynamic genetic variants related to antipsychotic adverse reactions in healthy volunteers. Pharmacogenomics 2013, 14, 1203–1214. [Google Scholar] [CrossRef] [PubMed]
- Czerwensky, F.; Leucht, S.; Steimer, W. MC4R rs489693: A clinical risk factor for second generation antipsychotic-related weight gain? Int. J. Neuropsychopharmacol. 2013, 16, 2103–2109. [Google Scholar] [CrossRef]
- Malhotra, A.K. Association Between Common Variants Near the Melanocortin 4 Receptor Gene and Severe Antipsychotic Drug–Induced Weight Gain. Arch. Gen. Psychiatry 2012, 69, 904. [Google Scholar] [CrossRef]
- Delacrétaz, A.; Zdralovic, A.; Vandenberghe, F.; Saigi-Morgui, N.; Glatard, A.; Quteineh, L.; Gholam-Rezaee, M.; Raffoul, W.; Applegate, L.A.; Jafari, P.; et al. Association of variants in SH2B1 and RABEP1 with worsening of low-density lipoprotein and glucose parameters in patients treated with psychotropic drugs. Gene 2017, 628, 8–15. [Google Scholar] [CrossRef]
- Cabaleiro, T.; López-Rodríguez, R.; Román, M.; Ochoa, D.; Novalbos, J.; Borobia, A.; Carcas, A.; Abad-Santos, F. Pharmacogenetics of quetiapine in healthy volunteers: Association with pharmacokinetics, pharmacodynamics, and adverse effects. Int. Clin. Psychopharmacol. 2015, 7, 82–88. [Google Scholar] [CrossRef]
- van der Weide, K.; van der Weide, J. The Influence of the CYP3A4*22 Polymorphism on Serum Concentration of Quetiapine in Psychiatric Patients. J. Clin. Psychopharmacol. 2014, 34, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Saiz-Rodríguez, M.; Almenara, S.; Navares-Gómez, M.; Ochoa, D.; Román, M.; Zubiaur, P.; Koller, D.; Santos, M.; Mejía, G.; Borobia, A.M.; et al. Effect of the Most Relevant CYP3A4 and CYP3A5 Polymorphisms on the Pharmacokinetic Parameters of 10 CYP3A Substrates. Biomedicines 2020, 8, 94. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-A.; Joo, H.-J.; Lee, H.-M.; Park, J.-Y. Influence of ABCB1 and CYP3A5 genetic polymorphisms on the pharmacokinetics of quetiapine in healthy volunteers. Pharmacogenet. Genom. 2014, 24, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Pharmacogenetics in Psychiatry: Misconceptions, Challenges, and Successes. Available online: https://www.pharmacytimes.com/view/pharmacogenetics-in-psychiatry-misconceptions-challenges-and-successes (accessed on 7 June 2022).
- Prioritization of CPIC Guidelines. Available online: https://cpicpgx.org/prioritization-of-cpic-guidelines/ (accessed on 17 May 2022).
- The Royal Dutch Society of Pharmacology (KNMP) Dutch Pharmacogenetics Working Group (DPWG). Pharmacogenetics guidelines. CYP2D6: Quetiapine 2022. Available online: https://www.g-standaard.nl/risicoanalyse/B0002394.PDF (accessed on 1 July 2022).
- Annotation of DPWG Guideline for Quetiapine and CYP3A4, PharmGKB. Available online: https://www.pharmgkb.org/guidelineAnnotation/PA166265421 (accessed on 9 June 2022).
- Annotation of DPWG Guideline for Risperidone and CYP2D6, PharmGKB. Available online: https://www.pharmgkb.org/guidelineAnnotation/PA166104943 (accessed on 9 June 2022).
- Annotation of DPWG Guideline for Aripiprazole and CYP2D6, PharmGKB. Available online: https://www.pharmgkb.org/guidelineAnnotation/PA166104937/annotation (accessed on 9 June 2022).
- Annotation of DPWG Guideline for Haloperidol and CYP2D6, PharmGKB. Available online: https://www.pharmgkb.org/guidelineAnnotation/PA166104988 (accessed on 9 June 2022).
- Annotation of DPWG Guideline for Zuclopenthixol and CYP2D6, PharmGKB. Available online: https://www.pharmgkb.org/guidelineAnnotation/PA166104992 (accessed on 9 June 2022).
- Annotation of DPWG Guideline for Pimozide and CYP2D6, PharmGKB. Available online: https://www.pharmgkb.org/guidelineAnnotation/PA166182819 (accessed on 9 June 2022).
- CPIC® Guideline for Tacrolimus and CYP3A5. Available online: https://cpicpgx.org/guidelines/guideline-for-tacrolimus-and-CYP3A5/ (accessed on 17 May 2022).
- González Jiménez, E.; Aguilar Cordero, M.J.; Padilla López, C.A.; García García, I. Obesidad monogénica humana: Papel del sistema leptina-melanocortina en la regulación de la ingesta de alimentos y el peso corporal en humanos. An. Sist. Sanit. Navar. 2012, 35, 285–293. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Receptor | Norquetiapine Activity | Quetiapine Activity | Effect |
|---|---|---|---|
| Serotonin 5-HT1A receptor | Partial agonism (high affinity *) | Partial agonism | Antidepressant and anxiolytic effects. |
| Serotonin 5-HT2A receptor | Antagonism (high affinity *) $ | Antagonism $ | Treatment of negative and cognitive symptoms, antidepressant activity. |
| Serotonin 5-HT2C receptor | Antagonism (high affinity *) | Antagonism | Possibly related to weight gain. |
| Serotonin 5-HT7 receptor | Antagonism (high affinity *) | Antagonism | Possibly related to antidepressant activity. |
| Dopamine D2 receptor | Antagonism (moderate affinity) | Antagonism (moderate affinity) | Treatment of negative and positive symptoms. |
| Histamine H1 receptor | Antagonism (high affinity *) | Antagonism | Possibly related to weight gain and sedative effects. |
| α1 receptor | Antagonism | Antagonism | Possibly related to orthostatic hypotension. |
| α2 receptor | Antagonism | Antagonism | Antidepressant activity. |
| Norepinephrine transporter (NET) | Antagonism | Antidepressant activity. | |
| Muscarinic receptors | Antagonism (high affinity) | Anticolinergic effects, possibly related to adverse atropinic effects. |
| Gene | Variant | Population | Association | p Value | References |
|---|---|---|---|---|---|
| COMT | rs4818 G>C | 995 Patients with schizophrenia. | C allele was associated with a worse response (PANSS score) compared to G allele carriers. | 0.007 | Xu et al. (2016) [14] |
| rs6269 G>A | A allele was associated with a worse response (PANSS score) compared to G allele. | 0.008 | |||
| rs5993883 G>T | T allele was associated with a worse response (PANSS score) compared to G allele. | 0.007 | |||
| EPM2A | rs1415744 T>C | 573 Patients with schizophrenia. | C allele was associated with an increased response (PANSS score) compared to T allele. | 0.004 | Porcelli et al. (2016) [15] |
| HTR1A | rs10042486 T>C | 221 Patients with schizophrenia and 171 healthy controls. | CT and CC were associated with a worse response (PANSS score) compared to TT allele diplotype. | 1.0 × 10−6 | Crisafulli et al. (2012) [16] |
| PDE4D | rs17742120 A>G | 738 Patients with schizophrenia. | G allele was associated with a decreased response (PANSS score) compared to A allele. | 1.58 × 10−7 | Clark et al. (2013) [17] |
| rs2164660 G>A | A allele was associated with an increased response (PANSS score) compared to G allele. | 1.87 × 10−7 | |||
| rs17382202 C>T | T allele was associated with an increased response (PANSS score) compared to C allele. | 4.21 × 10−8 | |||
| RGS4 | rs951439 C>T | 678 Patients with schizophrenia. | CC diplotype was associated with an increased response (PANSS score) compared to CT and TT allele. | 0.010 | Campbell et al. (2008) [18] |
| Gene | Variant | Population | Association | p Value | References |
|---|---|---|---|---|---|
| FAAH | rs324420 C>A | 83 Patients with psychotic episodes. | A allele was associated with increased weight gain compared to C allele carriers. | 0.002 | Monteleone, P. et al. (2010) [19] |
| GRIN2B | rs1806201 G>A | 211 healthy volunteers treated with a single dose of risperidone olanzapine or quetiapine. | AA diplotype was associated with an increased likelihood of adverse neuronal reactions compared to AG and GG diplotypes. | 0.025 | López-Rodríguez, R et al. (2013) [20] |
| MC4R | rs17782313 T>C | 345 patients with psychiatric episodes. | CC diplotype was associated with an increased likelihood of weight gain compared to CT and TT diplotypes. | 0.005 | Czerwensky, F et al. (2013) [21] |
| rs489693 A>C | 139 patients with psychiatric episodes. | AA diplotype was associated with a decreased likelihood of ADRs compared to AC and CC diplotypes. | <0.01 | Malhotra, A. K (2012) [22] | |
| 345 patients with psychiatric episodes. | 0.017 | Czerwensky, F et al. (2013) [21] | |||
| SH2B1 | rs388819 A>C | 357 patients with psychiatric episodes. | CC diplotype was associated with increased LDL levels compared to AA and AC diplotypes. | 0.005 | Delacrétaz, A et al. (2017) [23] |
| RABEP1 | rs1000940 A>G | 357 patients with psychiatric episodes. | AG and GG diplotypes were associated with lower glucose concentrations compared to AA diplotype. | <0.001 | |
| CYP2C19 | *2, and *4 | 79 healthy volunteers receiving a single dose of each quetiapine formulation. | *1/*2, *2/*2 and *2/*4 diplotypes were associated with higher prolactin plasma concentrations compared to *1/*1 diplotype. | 0.012 | Cabaleiro et al. (2015) [24] |
| CYP2C9 | *2 and *3 | *1/*2, *1/*3 and *2/*3 diplotypes showed somnolence. | 0.015 | ||
| CYP1A1 | *2 | *1/*2 diplotype showed somnolence. | 0.020 | ||
| CYP1A1 | *2 | *1/*2 diplotype showed neurological events. | 0.024 |
| Gene | Variant | Population | Association | p Value | References |
|---|---|---|---|---|---|
| DRD3 | rs6280 C>T | 79 healthy volunteers receiving a single dose of each quetiapine formulation. | TT diplotype was associated with increased clearance compared to CC and CT diplotypes. | 0.030 | Cabaleiro et al. (2015) [24] |
| CYP1A2 | *1,*1C | *1C/*1C diplotype was associated with higher exposure to quetiapine compared to *1/*1 diplotype. | 0.067 | ||
| COMT | rs13306278 C>T | 49 healthy volunteers treated with two doses of quetiapine. | T allele was associated with higher exposure to quetiapine compared to C allele. | 0.008 | Zubiaur et al. (2021) [5] |
| CYP2B6 | PM | PM showed higher t1/2 compared to RM, NM or IM. | 0.005 | ||
| ABCG2 | rs2231142 G>T | T allele was associated with quetiapine accumulation compared to G allele. | 0.027 | ||
| CYP3A5 | *3 | *3/*3 showed higher t1/2 compared to *1/*1 or *1/*3. | 0.018 | ||
| CYP3A4 | *22 | 238 patients treated with quetiapine. | *22/*22 or *22/*1 diplotypes were associated with increased exposure to quetiapine compared to *1/*1 diplotype. | 0.007 | Weide Karen et al. (2014) [25] |
| CYP3A4 | *3,*20,*22 | 19 patients treated with a single dose of quetiapine. | *3,*20,*22 alleles were associated with increased exposure to quetiapine compared to *1 allele. | 0.099 | Saiz Rodriguez et al. (2020) [26] |
| CYP3A5 | *3 | 40 healthy volunteers treated with a single dose of quetiapine. | *3/*3 diplotype was associated with increased exposure to quetiapine compared to *1/*3 or *1/*1 diplotypes. | 0.0017 | Kim, K.-A. et al. (2014) [27] |
| Drug | Phenotype | Implications | Recommendations | Authority |
|---|---|---|---|---|
| Quetiapine (2022) [31] | CYP3A4 PM | Reduced CYP3A4 activity. | Use 30% of the standard dose or choose another alternative that is not metabolized by CYP3A4. | DPWG |
| Risperidone (2020) [32] | CYP2D6 UM | Higher ratio of the active metabolite. | Choose another antipsychotic or titrate the dose according to the maximum dose for the active metabolite. | DPWG |
| CYP2D6 PM | Increased risperidone plasma concentration. | Reduce to 67% of the standard dose. | DPWG | |
| Aripiprazol (2021) [33] | CYP2D6 PM | Increased risk of ADRs. | Administer no more than 10 mg/day or 300 mg/month. | DPWG |
| Haloperidol (2021) [34] | CYP2D6 UM | Increased conversion of haloperidol. | Administer 1.5 times the standard dose or choose an alternative drug. | DPWG |
| CYP2D6 PM | Decreased conversion of haloperidol. | Administer 60% of the standard dose. | DPWG | |
| Zuclopenthixol (2022) [35] | CYP2D6 IM | Decreased conversion of zuclopentixol. | Administer 75% of the standard dose. | DPWG |
| CYP2D6 PM | Decreased conversion of zuclopentixol. | Administer 50% of the standard dose. | DPWG | |
| Pimozide (2021) [36] | CYP2D6 IM | Increased plasma concentration of pimozide. | Administer no more than 80% of the standard maximum dose. | DPWG |
| CYP2D6 PM | Increased plasma concentration of pimozide. | Administer no more than 50% of the standard maximum dose. | DPWG |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega-Ruiz, M.; Soria-Chacartegui, P.; Villapalos-García, G.; Abad-Santos, F.; Zubiaur, P. The Pharmacogenetics of Treatment with Quetiapine. Future Pharmacol. 2022, 2, 276-286. https://doi.org/10.3390/futurepharmacol2030018
Ortega-Ruiz M, Soria-Chacartegui P, Villapalos-García G, Abad-Santos F, Zubiaur P. The Pharmacogenetics of Treatment with Quetiapine. Future Pharmacology. 2022; 2(3):276-286. https://doi.org/10.3390/futurepharmacol2030018
Chicago/Turabian StyleOrtega-Ruiz, María, Paula Soria-Chacartegui, Gonzalo Villapalos-García, Francisco Abad-Santos, and Pablo Zubiaur. 2022. "The Pharmacogenetics of Treatment with Quetiapine" Future Pharmacology 2, no. 3: 276-286. https://doi.org/10.3390/futurepharmacol2030018