
Lightness Peaks during the Menstrual Phase: A Retrospective Challenge to a Visual Arousal Theory of Estrogen

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Scheduling
2.2. Data Collection Sessions
3. Results
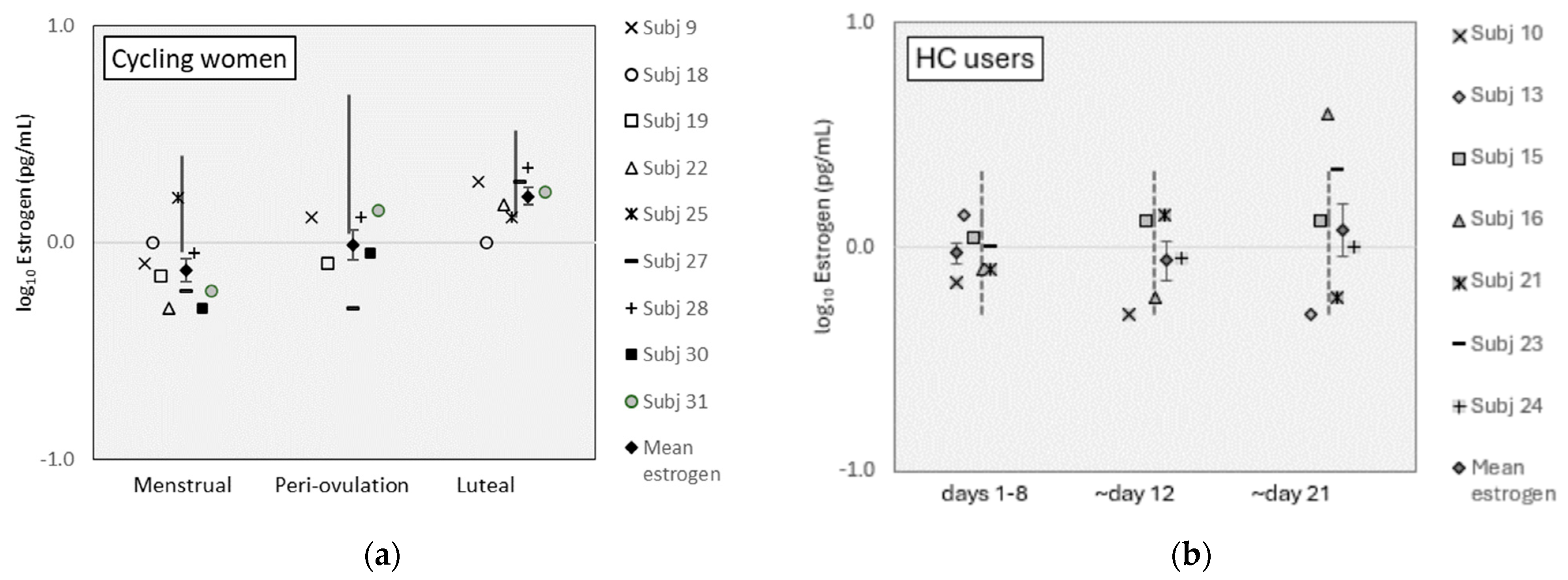
3.1. Salivary Estrogen Measures
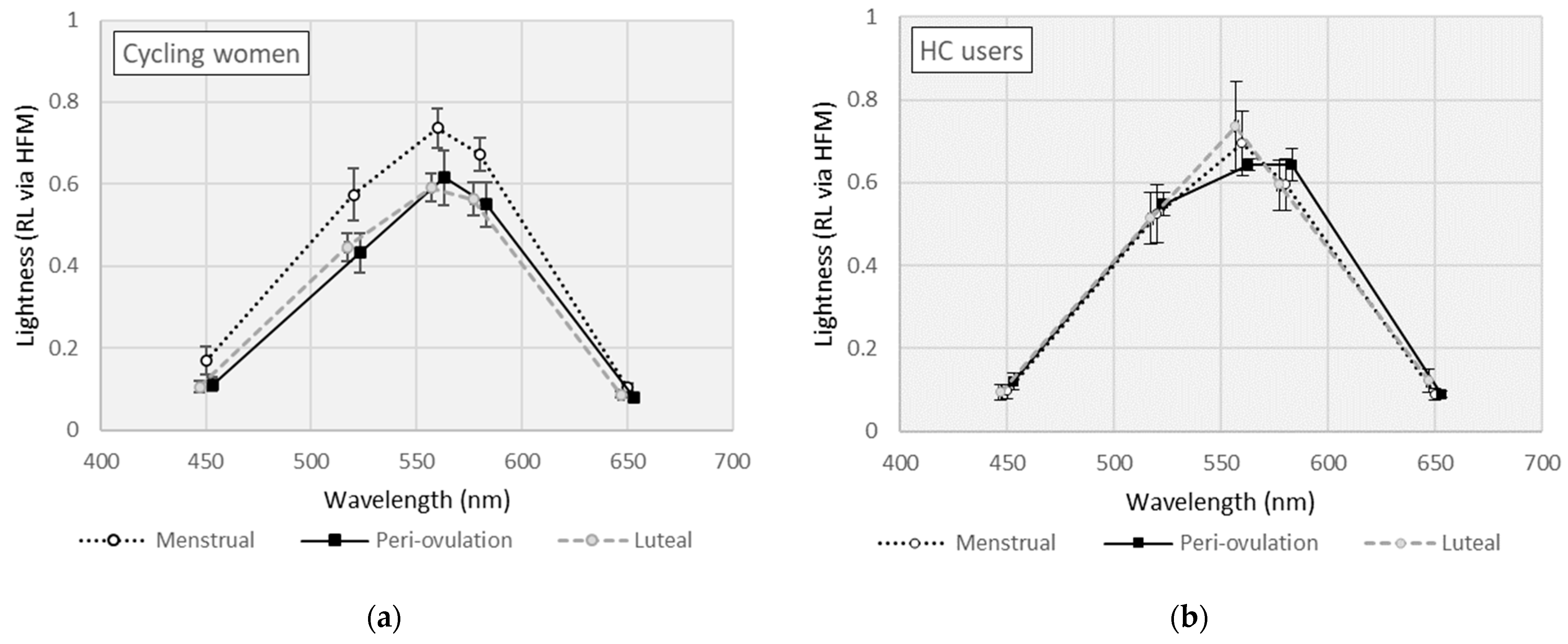
3.2. Effects of Menstrual Cycle Phase (MCP) on Lightness (RL)
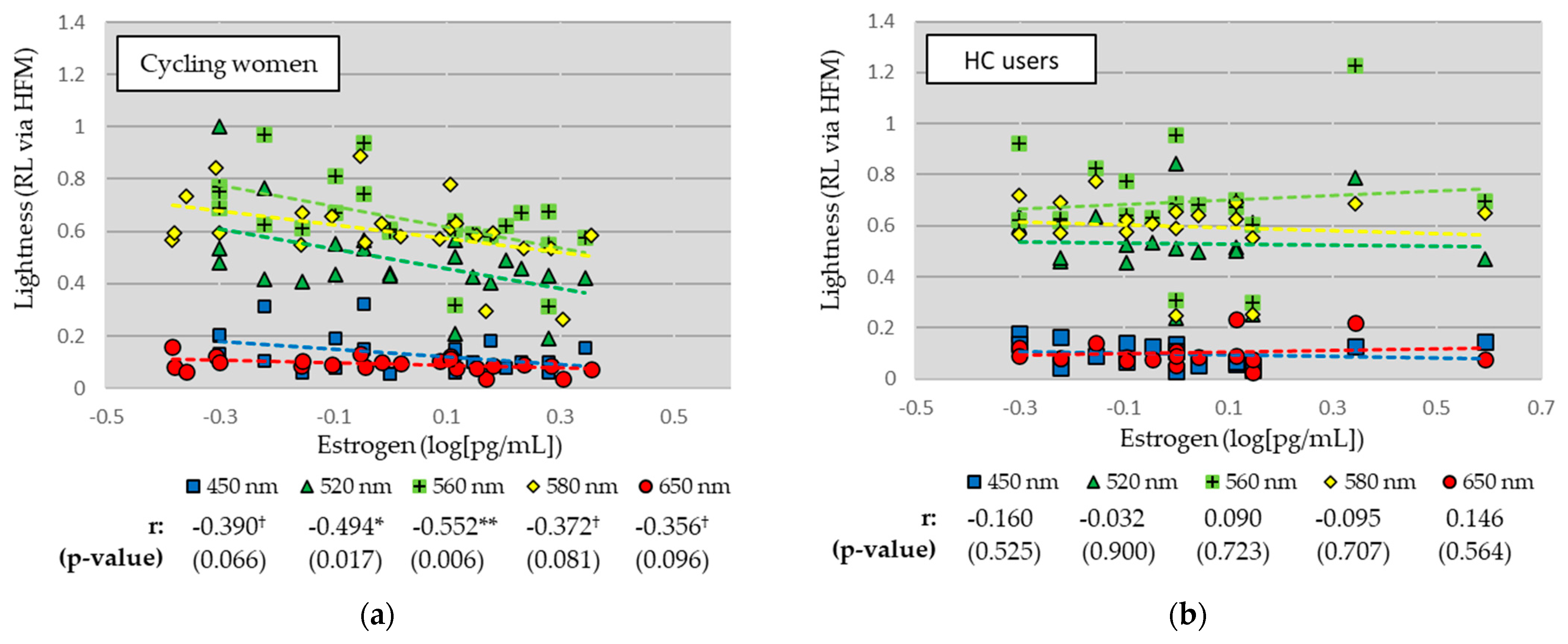
3.3. Relationships between Lightness (RL) and Estrogen (EST) Levels
4. Discussion
4.1. Notable Results
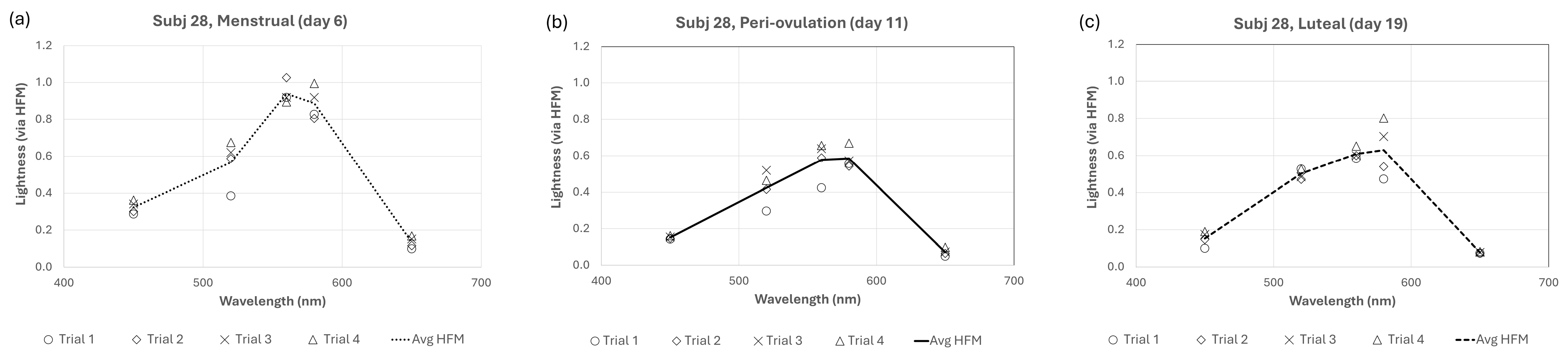
4.2. Reliability and Individual Differences
4.3. Limitations
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, R.; Shen, Y. Estrogen and brain: Synthesis, function and diseases. Front. Biosci. 2005, 10, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Hampson, E. A brief guide to the menstrual cycle and oral contraceptive use for researchers in behavioral endocrinology. Horm. Behav. 2020, 119, 104655. [Google Scholar] [CrossRef] [PubMed]
- Kopell, B.S.; Lunde, D.T.; Clayton, R.B.; Moos, R.H. Variations in some measures of arousal during the menstrual cycle. J. Nerv. Ment. Dis. 1969, 48, 180–187. [Google Scholar] [CrossRef]
- Parlee, M.B. Menstrual rhythms in sensory processes: A review of fluctuations in vision, olfaction, audition, taste, and touch. Psychol. Bull. 1983, 93, 539–548. [Google Scholar] [CrossRef]
- Cahill, L. Why sex matters for neuroscience. Nat. Rev. Neurosci. 2006, 7, 477–484. [Google Scholar] [CrossRef]
- Griffin, L.D. Males are ‘noisy females’ when it comes to reporting the psychological structure of the basic colours. Perception 2002, 32, 387. [Google Scholar]
- Scher, D.; Purcell, D.G.; Caputo, S.J. Visual acuity at two phases of the menstrual cycle. Bull. Psychon. Soc. 1985, 23, 119–121. [Google Scholar] [CrossRef]
- Werblin, F.S. The control of sensitivity in the retina. Sci. Am. 1973, 228, 70. [Google Scholar] [CrossRef]
- Guttridge, N.M. Changes in ocular and visual variables during the menstrual cycle. Ophthalmic Physiol. Opt. 1994, 14, 38–48. [Google Scholar] [CrossRef]
- Handa, R.J.; McGivern, R.F. Steroid hormones, receptors, and perceptual and cognitive sex differences in the visual system. Curr. Eye Res. 2015, 40, 110–127. [Google Scholar] [CrossRef]
- Kobayashi, K.; Kobayashi, H.; Ueda, M.; Honda, Y. Estrogen receptor expression in bovine and rat retinas. Investig. Ophthalmol. Vis. Sci. 1998, 39, 2105–2110. Available online: https://pubmed.ncbi.nlm.nih.gov/9761289/ (accessed on 27 October 2023).
- Ogueta, S.B.; Schwartz, S.D.; Yamashita, C.K.; Farber, D.B. Estrogen receptor in the human eye: Influence of gender and age on gene expression. Investig. Ophthalmol. Vis. Sci. 1999, 40, 1906–1911. Available online: https://pubmed.ncbi.nlm.nih.gov/10440242/ (accessed on 27 October 2023).
- Finkelstein, L.O. On sensory disorders in diseases, and on changes of the fields of vision in menstruation. Opth. Rev. Rec. Ophthal. Sci. 1887, 6, 323–326. [Google Scholar]
- Lorenzetti, F. Contributo allo Studio del Campo Visivo e del Senso Cromatico Della Donna Durante i Periodi Catameniale e Puerperale (Contribution to the study of the visual field and chromatic sense of the woman during the menstrual and post-partum periods). La Clin. Ostet. (Obstet. Clin.) 1926, 48, 345–349. [Google Scholar]
- Akar, Y.; Yucel, I.; Akar, M.E.; Taskin, O. Menstrual cycle-dependent changes in visual field analysis of healthy women. Ophthalmologica 2005, 219, 30–35. [Google Scholar] [CrossRef]
- Yucel, I.; Akar, M.E.; Dora, B.; Akar, Y.; Taskin, O.; Ozer, H.O. Effect of the menstrual cycle on standard achromatic and blue-on-yellow visual field analysis of women with migraine. Can. J. Ophthalmol. 2005, 40, 51–57. [Google Scholar] [CrossRef]
- Eisner, A.; Burke, S.N.; Toomey, M.D. Visual sensitivity across the menstrual cycle. Vis. Neurosci. 2004, 21, 513–531. [Google Scholar] [CrossRef]
- Giuffrè, G.; Di Rosa, L.; Fiorino, F. Changes in colour discrimination during the menstrual cycle. Ophthalmologica 2007, 221, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Iriguchi, M.; Koda, H.; Koyama, T.; Masataka, N. Colour-odour correspondences in women during the menstrual cycle: Comparative analysis between the menstrual and ovulation phases. Color Res. Appl. 2020, 45, 178–182. [Google Scholar] [CrossRef]
- Eisner, A.; Incognito, L.J. The color appearance of stimuli detected via short-wavelength-sensitive cones for breast cancer survivors using tamoxifen. Vis. Res. 2006, 46, 1816–1822. [Google Scholar] [CrossRef]
- Eisner, A.; Austin, D.F.; Samples, J.R. Short wavelength automated perimetry and tamoxifen use. Br. J. Ophthalmol. 2004, 88, 125–130. [Google Scholar] [CrossRef]
- Foutch, B.K. Sex hormones influence the Helmholtz-Kohlrausch Effect. J. Ophthalmic Vis. Res. 2024, 19, 71–81. [Google Scholar] [CrossRef]
- Foutch, B.K.; Bassi, C.J. Is the Helmholtz-Kohlrausch Effect more robust in women? Perception 2020, 49, 636–657. [Google Scholar] [CrossRef] [PubMed]
- Lennie, P.; Pokorny, J.; Smith, V.C. Luminance. J. Opt. Soc. Am. A Opt. Image Sci. Vis. 1993, 10, 1283–1293. [Google Scholar] [CrossRef]
- Cockerill, I.M.; Wormington, J.A.; Nevill, A.M. Menstrual-cycle effects on mood and perceptual-motor performance. J. Psychosom. Res. 1994, 38, 763–771. [Google Scholar] [CrossRef]
- Sommer, B. How does menstruation affect cognitive competence and psychophysiological response? Women Health 1983, 8, 53–90. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.A.; Anfe, T.E.; Matos, A.B.; Vieira, G.F. Influence of gender, anxiety and depression symptoms, and use of oral contraceptive in color perception. J. Esthet. Restor. Dent. 2015, 27 (Suppl. S1), S74–S79. [Google Scholar] [CrossRef] [PubMed]
- Ives, H.E. Studies in the photometry of different colours. I. Spectral luminosity curves obtained by the equality of the brightness photometer and the flicker photometer under similar conditions. Phil. Mag. 1912, 24, 149–188. [Google Scholar] [CrossRef]
- Ikeda, M.; Shimozono, H. Luminous efficiency functions determined by successive brightness matching. J. Am. Opt. Soc. 1978, 68, 1767–1771. [Google Scholar] [CrossRef]
- Draper, C.F.; Duisters, K.; Weger, B.; Chakrabarti, A.; Harms, A.C.; Brennan, L.; Hankemeier, T.; Goulet, L.; Konz, T.; Martin, F.P.; et al. Menstrual cycle rhythmicity: Metabolic patterns in healthy women. Sci. Rep. 2018, 8, 14568, Erratum in Sci. Rep. 2019, 9, 5797. [Google Scholar] [CrossRef]
- National Library of Medicine. Ovulation Home Test. Retrieved from MedlinePlus. 2021. Available online: https://medlineplus.gov/ency/article/007062.htm (accessed on 27 October 2023).
- Lewis, J.G. Steroid analysis in saliva: An overview. Clin. Biochem. Rev. 2006, 27, 139–146. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjects a | Age (Years) | HC Use (on Menstrual Cycle Days) | # of Sessions Completed: During MCPs | |||
|---|---|---|---|---|---|---|
| 1–7 | 8–14 | 21–27 | 22–28 | |||
| Cycling women | 25.8 ± 3.2 | -- | -- | -- | -- | -- |
| Subj 9 | 24 | none | none | none | none | 3: M, Ov, L |
| Subj 18 | 26 | none | none | none | none | 3: M, L(x2) |
| Subj 19 | 22 | none | none | none | none | 3: M, Ov, L |
| Subj 22 | 23 | none | none | none | none | 3: M, L(x2) |
| Subj 25 | 26 | none | none | none | none | 1: M |
| Subj 27 | 25 | none | none | none | none | 3: M, Ov, L |
| Subj 28 | 33 | none | none | none | none | 3: M, Ov, L |
| Subj 30 | 26 | none | none | none | none | 3: M, Ov, L |
| Subj 31 | 22 | none | none | none | none | 3: M, Ov, L |
| HC users | 26.0 ± 6.2 | -- | -- | -- | -- | -- |
| Subj 10 | 24 | EE3/NG1 | EE3/NG2 | EE3/NG3 | none | 3: M, Ov, L |
| Subj 13 | 23 | EE3/NG1 | EE3/NG2 | EE3/NG3 | none | 3: M, Ov, L |
| Subj 15 | 24 | EE3/NG1 | EE3/NG2 | EE3/NG3 | none | 3: M, Ov, L |
| Subj 16 | 24 | EE3/NG1 | EE3/NG2 | EE3/NG3 | none | 3: M, Ov, L |
| Subj 21 | 23 | EE3/NG1 | EE3/NG2 | EE3/NG3 | none | 3: M, Ov, L |
| Subj 23 | 40 | EE4/DRSP | EE4/DRSP | EE4/DRSP | none | 2: M, L |
| Subj 24 | 24 | EE3/NG1 | EE3/NG2 | EE3/NG3 | none | 3: M, Ov, L |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foutch, B. Lightness Peaks during the Menstrual Phase: A Retrospective Challenge to a Visual Arousal Theory of Estrogen. Physiologia 2024, 4, 139-148. https://doi.org/10.3390/physiologia4020008
Foutch B. Lightness Peaks during the Menstrual Phase: A Retrospective Challenge to a Visual Arousal Theory of Estrogen. Physiologia. 2024; 4(2):139-148. https://doi.org/10.3390/physiologia4020008
Chicago/Turabian StyleFoutch, Brian. 2024. "Lightness Peaks during the Menstrual Phase: A Retrospective Challenge to a Visual Arousal Theory of Estrogen" Physiologia 4, no. 2: 139-148. https://doi.org/10.3390/physiologia4020008