
The Effects of Acute Bouts of Aerobic Exercise on Adipokine Concentrations in Individuals with Moderate Stages of Chronic Kidney Disease
 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Participants
2.3. Baseline Demographics
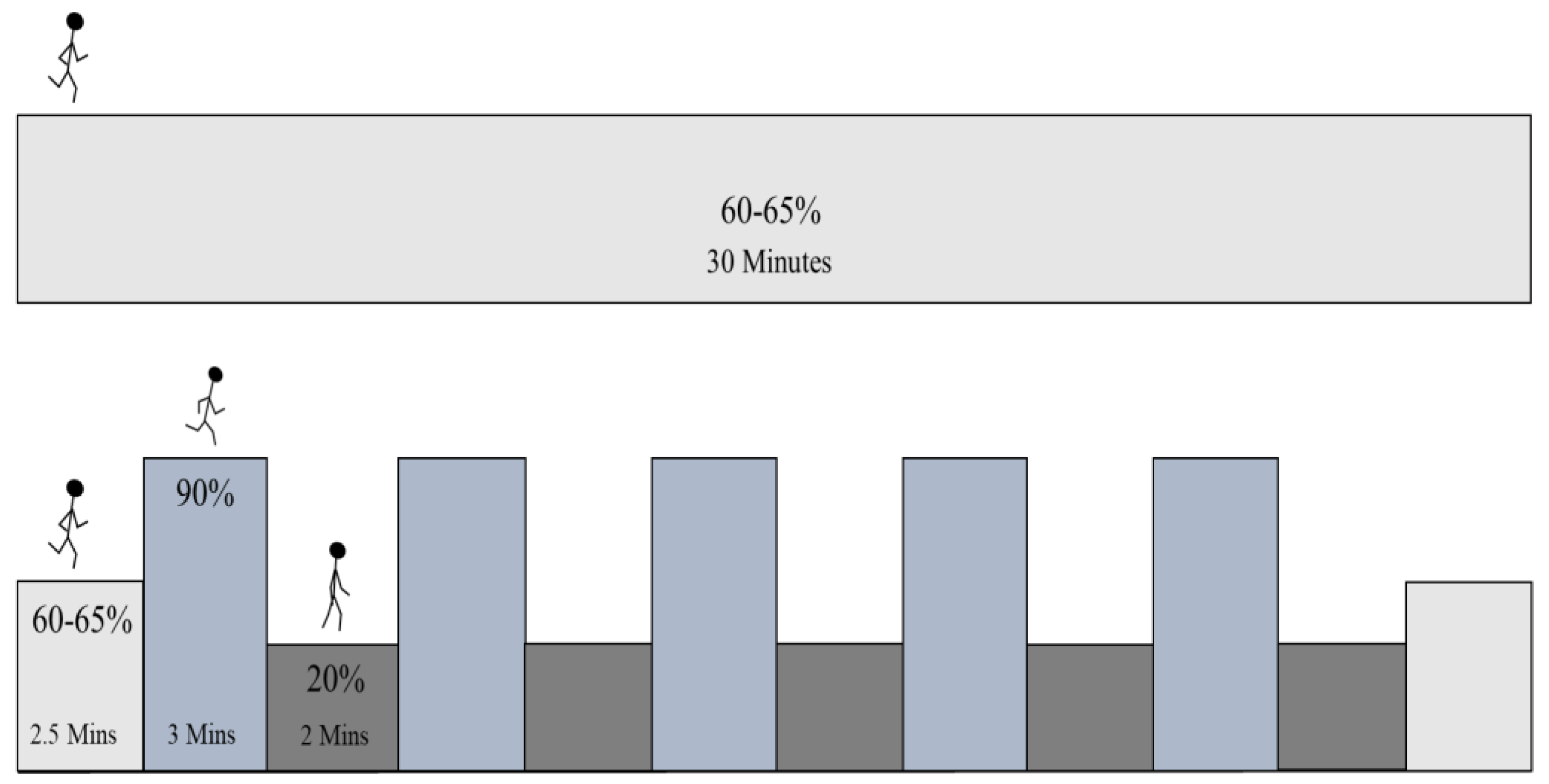
2.4. Exercise Protocol
2.5. Blood Sample Procedures
2.6. Biochemical Analyses
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sharaf El Din, U.A.A.; Salem, M.M.; Abdulazim, D.O. Stop chronic kidney disease progression: Time is approaching. World J. Nephrol. 2016, 5, 258–273. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.; Yang, H.-C.; Fogo, A.B. A perspective on chronic kidney disease progression. Am. J. Physiol. Renal Physiol. 2017, 312, F375–F384. [Google Scholar] [CrossRef] [PubMed]
- Papadakis, Z.; Grandjean, P.W.; Forsse, J.S. Effects of Acute Exercise on Cardiac Autonomic Response and Recovery in Non-Dialysis Chronic Kidney Disease Patients. Res. Q. Exerc. Sport 2022, 94, 812–825. [Google Scholar] [CrossRef] [PubMed]
- Akchurin, O.M.; Kaskel, F. Update on inflammation in chronic kidney disease. Blood Purif. 2015, 39, 84–92. [Google Scholar] [CrossRef]
- Soehnlein, O.; Libby, P. Targeting inflammation in atherosclerosis—From experimental insights to the clinic. Nat. Rev. Drug Discov. 2021, 20, 589–610. [Google Scholar] [CrossRef]
- Forsse, J.S.; Papadakis, Z.; Peterson, M.N.; Taylor, J.K.; Hess, B.W.; Schwedock, N.; Allison, D.C.; Griggs, J.O.; Wilson, R.L.; Grandjean, P.W. The Influence of an Acute Bout of Aerobic Exercise on Vascular Endothelial Function in Moderate Stages of Chronic Kidney Disease. Life 2022, 12, 91. [Google Scholar] [CrossRef]
- Forsse, J.; Papadakis, Z.; Bane, A.; Marroquín, F.M.; Grandjean, P. Brachial Artery FMD and Endothelial Responses to High-Intensity Interval and Steady-State Moderate-Intensity Exercise. Int. J. Exerc. Sci. Conf. Proc. 2016, 2, 10. [Google Scholar] [CrossRef]
- Miricescu, D.; Balan, D.G.; Tulin, A.; Stiru, O.; Vacaroiu, I.A.; Mihai, D.A.; Popa, C.C.; Enyedi, M.; Nedelea, A.S.; Nica, A.E.; et al. Impact of adipose tissue in chronic kidney disease development (Review). Exp. Ther. Med. 2021, 21, 1–8. [Google Scholar] [CrossRef]
- Ouchi, N.; Parker, J.L.; Lugus, J.J.; Walsh, K. Adipokines in inflammation and metabolic disease. Nat. Rev. Immunol. 2011, 11, 85–97. [Google Scholar] [CrossRef]
- Scherer, P.E. Adipose tissue: From lipid storage compartment to endocrine organ. Diabetes 2006, 55, 1537–1545. [Google Scholar] [CrossRef]
- Das, E.; Moon, J.H.; Lee, J.H.; Thakkar, N.; Pausova, Z.; Sung, H.-K. Adipose Tissue and Modulation of Hypertension. Curr. Hypertens. Rep. 2018, 20, 96. [Google Scholar] [CrossRef] [PubMed]
- Freitas Lima, L.C.; de Braga, V.A.; de França Silva, M.d.S.; de Cruz, J.C.; Sousa Santos, S.H.; de Oliveira Monteiro, M.M.; de Balarini, C.M. Adipokines, diabetes and atherosclerosis: An inflammatory association. Front. Physiol. 2015, 6, 304. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, P. The role of adipokines in chronic inflammation. ImmunoTargets Ther. 2016, 5, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Watanabe-Kominato, K.; Takahashi, Y.; Kojima, M.; Watanabe, R. Adipose Tissue-Derived Omentin-1 Function and Regulation. Compr. Physiol. 2017, 7, 765–781. [Google Scholar] [CrossRef]
- Wilms, B.; Ernst, B.; Gerig, R.; Schultes, B. Plasma Omentin-1 Levels are Related to Exercise Performance in Obese Women and Increase Upon Aerobic Endurance Training. Exp. Clin. Endocrinol. Diabetes 2015, 123, 187–192. [Google Scholar] [CrossRef]
- Pereira, S.S.; Alvarez-Leite, J.I. Adipokines: Biological functions and metabolically healthy obese profile. J. Recept. Ligand Channel Res. 2014, 7, 15–25. [Google Scholar] [CrossRef]
- Chapman-Lopez, T.; Wilburn, D.; Fletcher, E.; Adair, K.; Ismaeel, A.; Heileson, J.; Gallucci, A.; Funderburk, L.; Koutakis, P.; Forsse, J.S. The influence of resistance training on adipokines in post-menopausal women: A brief review. Sports Med. Health Sci. 2022, 4, 219–224. [Google Scholar] [CrossRef]
- Golbidi, S.; Laher, I. Exercise induced adipokine changes and the metabolic syndrome. J. Diabetes Res. 2014, 2014, 726861. [Google Scholar] [CrossRef]
- Kashino, I.; Nanri, A.; Kurotani, K.; Akter, S.; Yasuda, K.; Sato, M.; Hayabuchi, H.; Mizoue, T. Association of dietary patterns with serum adipokines among Japanese: A cross-sectional study. Nutr. J. 2015, 14, 58. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Mediterranean dietary pattern, inflammation and endothelial function: A systematic review and meta-analysis of intervention trials. Nutr. Metab. Cardiovasc. Dis. NMCD 2014, 24, 929–939. [Google Scholar] [CrossRef]
- Mika, A.; Macaluso, F.; Barone, R.; Di Felice, V.; Sledzinski, T. Effect of Exercise on Fatty Acid Metabolism and Adipokine Secretion in Adipose Tissue. Front. Physiol. 2019, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Park, K.M.; Park, S.C.; Kang, S. Effects of resistance exercise on adipokine factors and body composition in pre- and postmenopausal women. J. Exerc. Rehabil. 2019, 15, 676–682. [Google Scholar] [CrossRef]
- Parastesh, M.; Alibakhshi, E.; Saremi, A.; Shavandi, N. The effect of aerobic exercise training on leptin and pulmonary function tests during weight loss in men with visceral obesity. J. Shahrekord Univ. Med. Sci. 2020, 22, 96–101. [Google Scholar] [CrossRef]
- Marshall, J.A.; Grunwald, G.K.; Donahoo, W.T.; Scarbro, S.; Shetterly, S.M. Percent body fat and lean mass explain the gender difference in leptin: Analysis and interpretation of leptin in Hispanic and non-Hispanic white adults. Obes. Res. 2000, 8, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Bouassida, A.; Chamari, K.; Zaouali, M.; Feki, Y.; Zbidi, A.; Tabka, Z. Review on leptin and adiponectin responses and adaptations to acute and chronic exercise. Br. J. Sports Med. 2010, 44, 620–630. [Google Scholar] [CrossRef] [PubMed]
- Lehr, S.; Hartwig, S.; Sell, H. Adipokines: A treasure trove for the discovery of biomarkers for metabolic disorders. Proteom. Clin. Appl. 2012, 6, 91–101. [Google Scholar] [CrossRef]
- Forsse, J.S.; Richardson, K.A.; Chapman-Lopez, T.J.; Torres, R.; Heileson, J.L.; Ismaeel, A.; Funderburk, L.; Gallucci, A.R.; Allison, D.C.; Koutakis, P. The Utilization of Body Composition to Predict Cardiorespiratory Fitness and Determine Association with CKD Stage in Individuals with Mid-Spectrum CKD: A Pilot Study. Kidney Dial. 2023, 3, 265–273. [Google Scholar] [CrossRef]
- Forsse, J.S.; Peterson, M.; Papadakis, Z.; Taylor, J.K.; Hess, B.W.; Schwedock, N.; Allison, C.D.; Griggs, J.O.; Wilson, R.L.; Grandjean, P.W. The Effect of Acute Aerobic Exercise on Biomarkers of Renal Health and Filtration in Moderate-CKD. Res. Q. Exerc. Sport 2022. [Google Scholar] [CrossRef]
- Jürimäe, J.; Purge, P.; Jürimäe, T. Adiponectin is altered after maximal exercise in highly trained male rowers. Eur. J. Appl. Physiol. 2005, 93, 502–505. [Google Scholar] [CrossRef]
- Jürimäe, J.; Jürimäe, T. Leptin responses to short term exercise in college level male rowers. Br. J. Sports Med. 2005, 39, 6–9. [Google Scholar] [CrossRef]
- Legakis, I.N.; Mantzouridis, T.; Saramantis, A.; Lakka-Papadodima, E. Rapid decrease of leptin in middle-aged sedentary individuals after 20 minutes of vigorous exercise with early recovery after the termination of the test. J. Endocrinol. Investig. 2004, 27, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Sari, R.; Balci, M.K.; Balci, N.; Karayalcin, U. Acute effect of exercise on plasma leptin level and insulin resistance in obese women with stable caloric intake. Endocr. Res. 2007, 32, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Atashak, S.; Stannard, S.R.; Daraei, A.; Soltani, M.; Saeidi, A.; Moradi, F.; Laher, I.; Hackney, A.C.; Zouhal, H. High-intensity Interval Training Improves Lipocalin-2 and Omentin-1 Levels in Men with Obesity. Int. J. Sports Med. 2022, 43, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.M.; Heidarianpour, A.; Tavassoli, H. Aerobic Exercise Training Effects on Omentin-1, Insulin Resistance, and Lipid Profile Among Male Smokers. Res. Q. Exerc. Sport 2022, 94, 880–885. [Google Scholar] [CrossRef]
- Jamurtas, A.Z.; Theocharis, V.; Koukoulis, G.; Stakias, N.; Fatouros, I.G.; Kouretas, D.; Koutedakis, Y. The effects of acute exercise on serum adiponectin and resistin levels and their relation to insulin sensitivity in overweight males. Eur. J. Appl. Physiol. 2006, 97, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, R.R.; Aboudehen, K.S.; Carruth, A.K.; Durand, R.T.J.; Acevedo, E.O.; Hebert, E.P.; Johnson, L.G.; Castracane, V.D. Adiponectin responses to continuous and progressively intense intermittent exercise. Med. Sci. Sports Exerc. 2003, 35, 1320–1325. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall (n = 14) ** | Males (n = 6) ** | Females (n = 8) ** | p-Value (Male and Female Differences) | Cohen’s d (Male and Female Differences | |
|---|---|---|---|---|---|
| Age (years) | 58.7 ± 9.7 | 56.3 ± 9.3 | 60.5 ± 10.2 | 0.740 | 0.424 |
| Height (cm) | 168.5 ± 9.7 | 178.1 ± 1.7 | 161.3 ± 5.1 | 0.240 | −3.553 |
| Weight (kg) | 83.5 ± 18.2 | 94.5 ± 17.6 | 75.3 ± 14.5 | 0.616 | −1.212 |
| BF (%) | 36.0 ± 9.9 | 26.9 ± 7.8 | 42.8 ± 4.0 | 0.051 | 2.715 |
| VE (L/min) | 50.3 ± 19.4 | 64.2 ± 17.9 | 39.8 ± 13.4 | 0.920 | −1.579 |
| Time Points | SSE ** | HIIE ** | F-Value (1,13) (Condition) | p-Value (Condition) | Partial Eta Squared (Condition) | F-Value (1,13) (Time) | p-Value (Time) | Partial Eta Squared (Time) | |
|---|---|---|---|---|---|---|---|---|---|
| Adiponectin | Baseline | 37.97 ± 30.34 | 45.95 ± 33.96 | 0.065 | 1.085 | 0.353 | 0.077 | ||
| 1 h | 56.83 ± 51.74 | 50.27 ± 44.14 | 0.802 | 0.005 * | |||||
| 24 h | 51.40 ± 42.90 | 46.22 ± 31.09 | |||||||
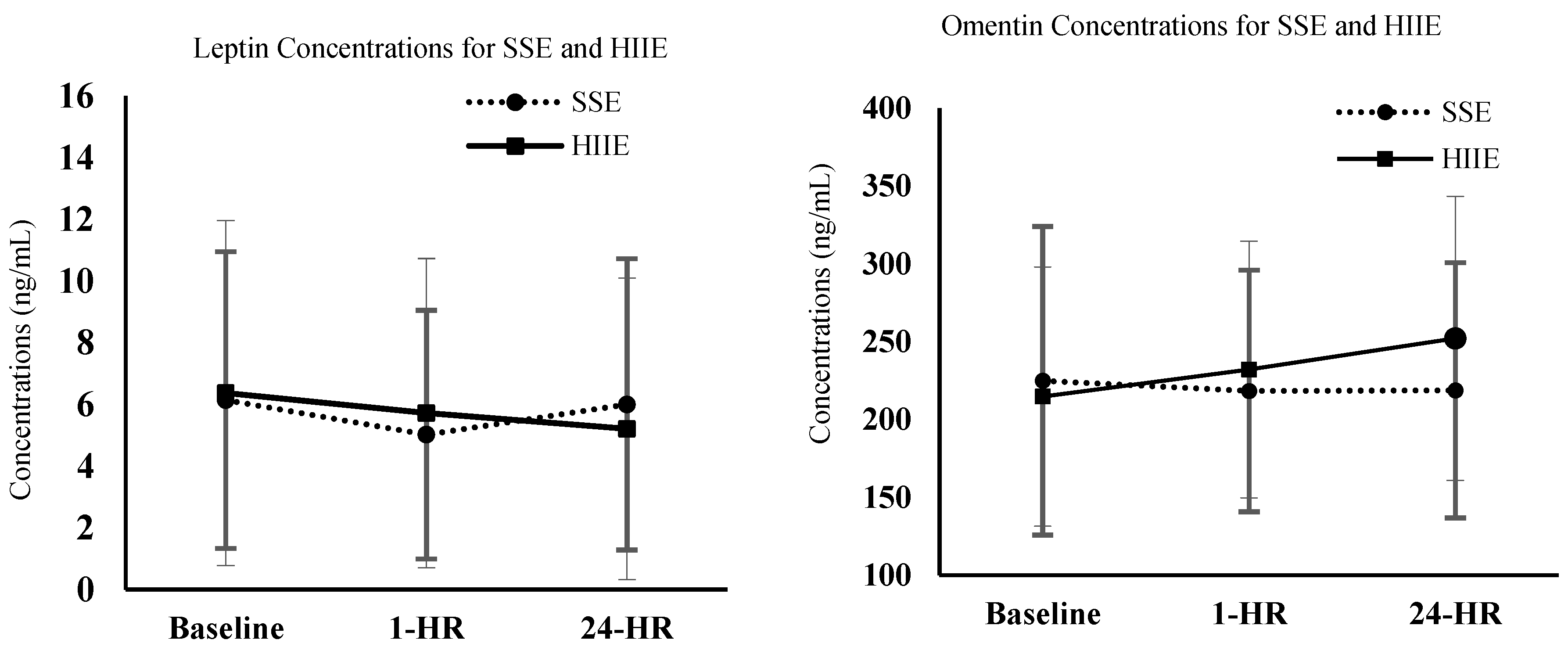
| Leptin | Baseline | 6.14 ± 4.81 | 6.37 ± 5.59 | 0.008 | 0.929 | 2.749 | 0.084 | 0.186 | |
| 1 h | 5.02 ± 4.03 | 5.72 ± 5.01 | 0.001 * | ||||||
| 24 h | 6.00 ± 4.72 | 5.21 ± 4.89 | |||||||
| Omentin | Baseline | 224.81 ± 99.11 | 214.67 ± 83.28 | 0.895 | 0.361 | 1.552 | 0.235 | 0.058 | |
| 1 h | 218.28 ± 77.63 | 232.07 ± 82.43 | 0.064 | ||||||
| 24 h | 218.70 ± 81.99 | 252.04 ± 91.22 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chapman-Lopez, T.J.; Taylor, J.K.; Torres, R.; Wilburn, D.; Funderburk, L.K.; Allison, D.C.; Forsse, J.S. The Effects of Acute Bouts of Aerobic Exercise on Adipokine Concentrations in Individuals with Moderate Stages of Chronic Kidney Disease. Physiologia 2023, 3, 522-530. https://doi.org/10.3390/physiologia3040038
Chapman-Lopez TJ, Taylor JK, Torres R, Wilburn D, Funderburk LK, Allison DC, Forsse JS. The Effects of Acute Bouts of Aerobic Exercise on Adipokine Concentrations in Individuals with Moderate Stages of Chronic Kidney Disease. Physiologia. 2023; 3(4):522-530. https://doi.org/10.3390/physiologia3040038
Chicago/Turabian StyleChapman-Lopez, Tomas J., James Kyle Taylor, Ricardo Torres, Dylan Wilburn, LesLee K. Funderburk, Dale C. Allison, and Jeffrey S. Forsse. 2023. "The Effects of Acute Bouts of Aerobic Exercise on Adipokine Concentrations in Individuals with Moderate Stages of Chronic Kidney Disease" Physiologia 3, no. 4: 522-530. https://doi.org/10.3390/physiologia3040038