
The Diagnostic Challenges of Ovine Pulmonary Adenocarcinoma

 ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Clinical Diagnose
3. Imaging Diagnosis
3.1. Ultrasound
3.2. Radiologic Diagnosis
3.2.1. Radiography (X-ray Imaging)
3.2.2. Computed Tomography
4. Pathological Diagnosis
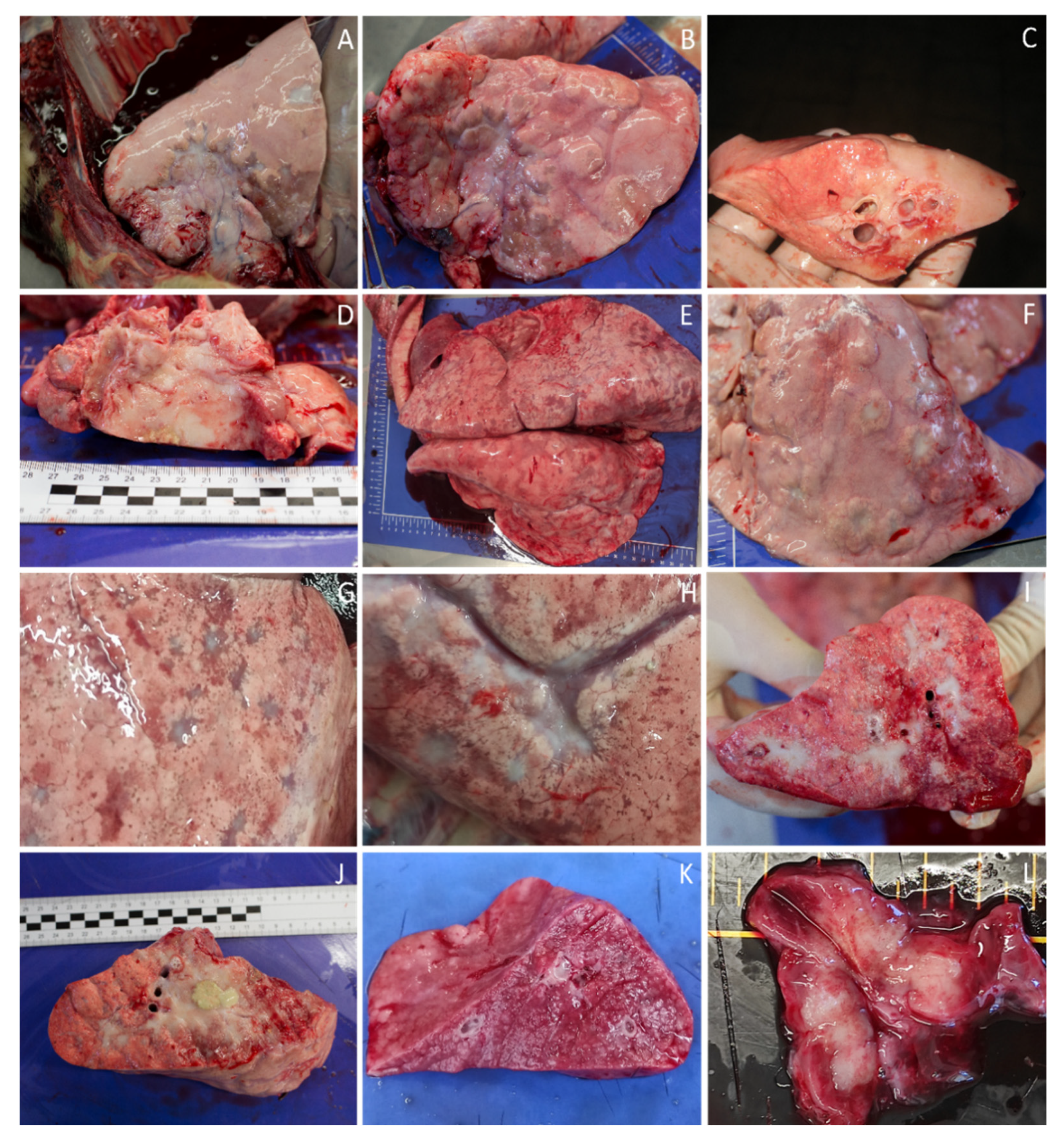
4.1. Macroscopic Diagnosis
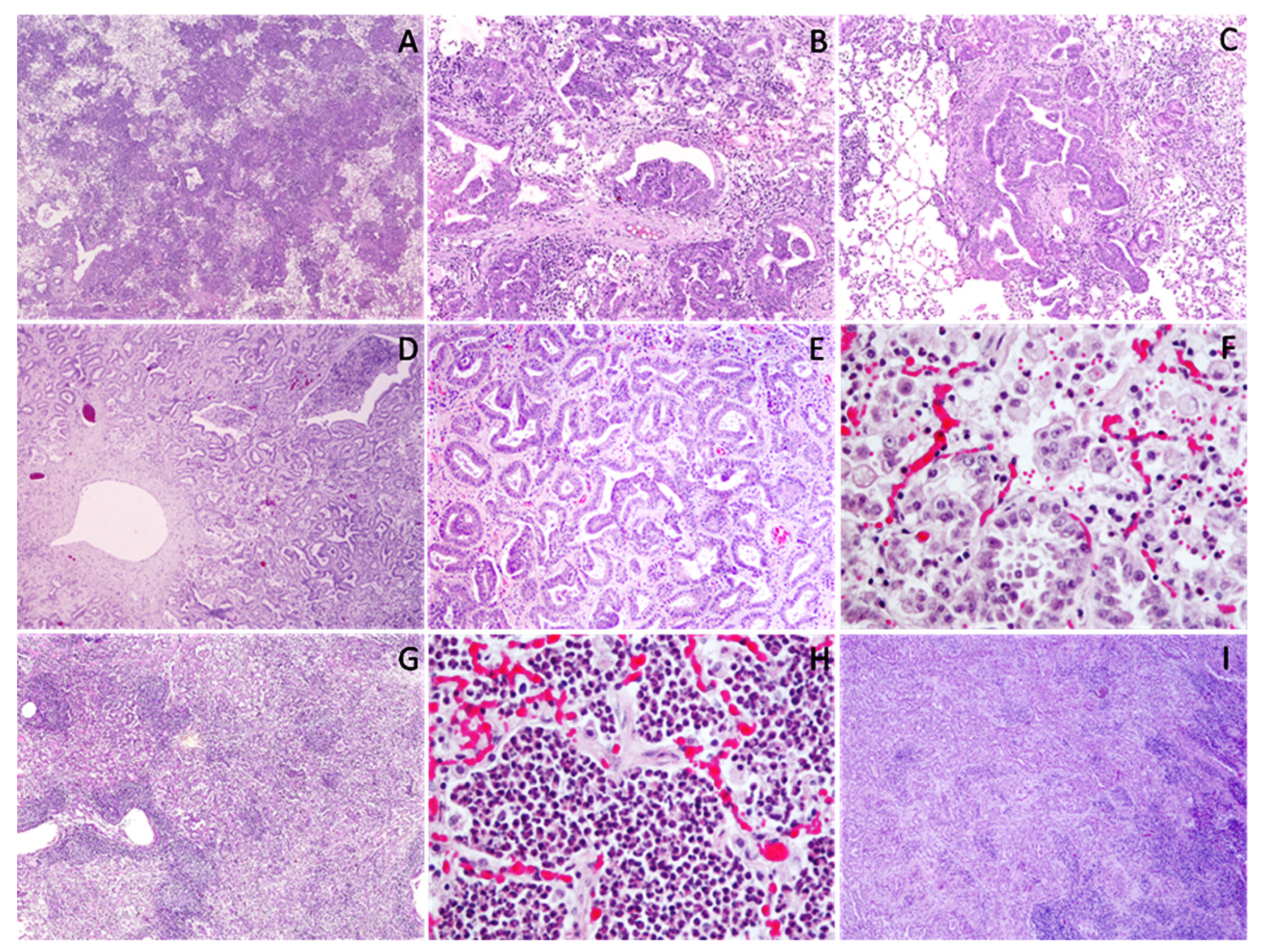
4.2. Microscopic Diagnosis
4.3. Immunohistochemistry Diagnosis
5. Ancillary Tests
5.1. Serological Diagnostic
5.2. Molecular Diagnosis
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Shi, W.; Jia, S.; Guan, X.; Yao, X.; Pan, R.; Huang, X.; Ma, Y.; Wei, J.; Xu, Y. A Survey of Jaagsiekte Sheep Retrovirus (JSRV) Infection in Sheep in the Three Northeastern Provinces of China. Arch. Virol. 2021, 166, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Sanna, M.P.; Sanna, E.; De Las Heras, M.; Leoni, A.; Nieddu, A.M.; Pirino, S.; Sharp, J.M.; Palmarini, M. Association of Jaagsiekte Sheep Retrovirus with Pulmonary Carcinoma in Sardinian Moufflon (Ovis Musimon). J. Comp. Pathol. 2001, 125, 145–152. [Google Scholar] [CrossRef] [PubMed]
- York, D.F.; Querat, G. A History of Ovine Pulmonary Adenocarcinoma (Jaagsiekte) and Experiments Leading to the Deduction of the JSRV Nucleotide Sequence. In Jaagsiekte Sheep Retrovirus and Lung Cancer; Fan, H., Ed.; Current Topics in Microbiology and Immunology; Springer: Berlin/Heidelberg, Germany, 2003; Volume 275, pp. 1–23. ISBN 9783642628979. [Google Scholar]
- Verwoerd, D.W.; Tustin, R.C.; Payne, A.L. Jaagsiekte: An infectious pulmonary adenomatosis of sheep. In Comparative Pathobiology of Viral Diseases; Olsen, R.G., Krakowka, S., Blakeslee, J.R., Eds.; CRC Press: Boca Raton, FL, USA, 2021; pp. 53–76. ISBN 9780367252212. [Google Scholar]
- Lee, A.M.; Wolfe, A.; Cassidy, J.P.; Messam, L.L.M.; Moriarty, J.P.; O’Neill, R.; Fahy, C.; Connaghan, E.; Cousens, C.; Dagleish, M.P.; et al. First Confirmation by PCR of Jaagsiekte Sheep Retrovirus in Ireland and Prevalence of Ovine Pulmonary Adenocarcinoma in Adult Sheep at Slaughter. Ir. Vet. J. 2017, 70, 33. [Google Scholar] [CrossRef]
- Griffiths, D.J.; Martineau, H.M.; Cousens, C. Pathology and Pathogenesis of Ovine Pulmonary Adenocarcinoma. J. Comp. Pathol. 2010, 142, 260–283. [Google Scholar] [CrossRef] [PubMed]
- Hashemnia, M.; Chalechale, A.; Malmir, E. Pulmonary Lesions in Slaughtered Sheepin Western Iran: Gross and Histopathological Findings. Vet. Ital. 2019, 55, 47–56. [Google Scholar] [CrossRef]
- Mekibib, B.; Mikir, T.; Fekadu, A.; Abebe, R. Prevalence of Pneumonia in Sheep and Goats Slaughtered at Elfora Bishoftu Export Abattoir, Ethiopia: A Pathological Investigation. J. Vet. Med. 2019, 2019, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alegria, N. Adenocarcinoma pulmonar dos ovinos em Portugal: Desenvolvimento de métodos para a detecção do agente etiológico. Ph.D. Thesis, Universidade de Trás-os-Montes e Alto Douro, Vila Real, Portugal, 2006. pp. 97–106, 125–134. [Google Scholar]
- De las Heras, M.; Borobia, M.; Ortín, A. Neoplasia-Associated Wasting Diseases with Economic Relevance in the Sheep Industry. Animals 2021, 11, 381. [Google Scholar] [CrossRef] [PubMed]
- Gray, M.E.; Meehan, J.; Sullivan, P.; Marland, J.R.K.; Greenhalgh, S.N.; Gregson, R.; Clutton, R.E.; Ward, C.; Cousens, C.; Griffiths, D.J.; et al. Ovine Pulmonary Adenocarcinoma: A Unique Model to Improve Lung Cancer Research. Front. Oncol. 2019, 9, 335. [Google Scholar] [CrossRef]
- Zhang, K.; Kong, H.; Liu, Y.; Shang, Y.; Wu, B.; Liu, X. Diagnosis and Phylogenetic Analysis of Ovine Pulmonary Adenocarcinoma in China. Virus Genes 2014, 48, 64–73. [Google Scholar] [CrossRef] [Green Version]
- Ortín, A.; De las Heras, M.; Borobia, M.; Ramo, M.A.; Ortega, M.; Ruíz de Arcaute, M. Ovine Pulmonary Adenocarcinoma: A Transmissible Lung Cancer of Sheep, Difficult to Control. Small Rumin. Res. 2019, 176, 37–41. [Google Scholar] [CrossRef]
- York, D.F.; Vigne, R.; Verwoerd, D.W.; Querat, G. Nucleotide Sequence of the Jaagsiekte Retrovirus, an Exogenous and Endogenous Type D and B Retrovirus of Sheep and Goats. J. Virol. 1992, 66, 4930–4939. [Google Scholar] [CrossRef] [Green Version]
- Wilson, D.W. Tumors of the Respiratory Tract. In Tumors in Domestic Animals; Meuten, D.J., Ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2016; pp. 467–498. ISBN 9781119181200. [Google Scholar]
- Palmarini, M.; Cousens, C.; Dalziel, R.G.; Bai, J.; Stedman, K.; DeMartini, J.C.; Sharp, J.M. The Exogenous Form of Jaagsiekte Retrovirus Is Specifically Associated with a Contagious Lung Cancer of Sheep. J. Virol. 1996, 70, 1618–1623. [Google Scholar] [CrossRef] [Green Version]
- Palmarini, M.; Maeda, N.; Murgia, C.; De-Fraja, C.; Hofacre, A.; Fan, H. A Phosphatidylinositol 3-Kinase Docking Site in the Cytoplasmic Tail of the Jaagsiekte Sheep Retrovirus Transmembrane Protein Is Essential for Envelope-Induced Transformation of NIH 3T3 Cells. J. Virol. 2001, 75, 11002–11009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rai, S.K.; DeMartini, J.C.; Miller, A.D. Retrovirus Vectors Bearing Jaagsiekte Sheep Retrovirus Env Transduce Human Cells by Using a New Receptor Localized to Chromosome 3p21.3. J. Virol. 2000, 74, 4698–4704. [Google Scholar] [CrossRef]
- Caporale, M.; Martineau, H.; De las Heras, M.; Murgia, C.; Huang, R.; Centorame, P.; Di Francesco, G.; Di Gialleonardo, L.; Spencer, T.E.; Griffiths, D.J.; et al. Host Species Barriers to Jaagsiekte Sheep Retrovirus Replication and Carcinogenesis. J. Virol. 2013, 87, 10752–10762. [Google Scholar] [CrossRef] [Green Version]
- Yousem, S.A.; Finkelstein, S.D.; Swalsky, P.A.; Bakker, A.; Ohori, N.P. Absence of Jaagsiekte Sheep Retrovirus DNA and RNA in Bronchioloalveolar and Conventional Human Pulmonary Adenocarcinoma by PCR and RT-PCR Analysis. Hum. Pathol. 2001, 32, 1039–1042. [Google Scholar] [CrossRef] [PubMed]
- Sharp, J.M.; DeMartini, J.C. Natural History of JSRV in Sheep. In Jaagsiekte Sheep Retrovirus and Lung Cancer; Fan, H., Ed.; Current Topics in Microbiology and Immunology; Springe: Berlin/Heidelberg, Germany, 2003; Volume 275, pp. 55–79. ISBN 9783642628979. [Google Scholar]
- De Las Heras, M.; González, L.; Sharp, J.M. Pathology of Ovine Pulmonary Adenocarcinoma. In Jaagsiekte Sheep Retrovirus and Lung Cancer; Fan, H., Ed.; Current Topics in Microbiology and Immunology; Springer: Berlin, Heidelberg, 2003; Volume 275, pp. 25–54. ISBN 9783642628979. [Google Scholar]
- Salvatori, D.; González, L.; Dewar, P.; Cousens, C.; de Las Heras, M.; Dalziel, R.G.; Sharp, J.M. Successful Induction of Ovine Pulmonary Adenocarcinoma in Lambs of Different Ages and Detection of Viraemia during the Preclinical Period. J. Gen. Virol. 2004, 85, 3319–3324. [Google Scholar] [CrossRef] [PubMed]
- Palmarini, M.; Fan, H. Retrovirus-Induced Ovine Pulmonary Adenocarcinoma, an Animal Model for Lung Cancer. JNCI J. Natl. Cancer Inst. 2001, 93, 1603–1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verwoerd, D.W. Jaagsiekte (ovine pulmonary adenomatosis virus). In Virus Infections of Ruminants; Dinta, Z., Morein, B., Eds.; Elsevier: Amsterdam, The Netherlands, 1990; pp. 453–462. ISBN 9780444873125. [Google Scholar]
- Palsson, P.A. Maedi/Visna of sheep in Iceland. Introduction of the disease to Iceland, clinical features, control mesures and eradication. In Slow Viruses in Sheep, Goats and Cattle; Sharp, J.M., Hoff-Jørgensen, R., Eds.; Office for Official Publications of the European Communities [distributor]: Luxembourg, 1985; pp. 3–19. ISBN 9789282557150. [Google Scholar]
- Sharp, J.M.; Scott, F.M.M.; Herring, A.J.; Angus, K.W.; Gray, E.W.; Cuthbertson, J.C. Studies of the epidemiology, aetiology and transmission of jaagsiekte in Scotland. In Slow Viruses in Sheep, Goats and Cattle; Sharp, J.M., Hoff-Jørgensen, R., Eds.; Office for Official Publications of the European Communities [distributor]: Luxembourg, 1985; pp. 167–170. ISBN 9789282557150. [Google Scholar]
- Cousens, C.; Thonur, L.; Imlach, S.; Crawford, J.; Sales, J.; Griffiths, D.J. Jaagsiekte Sheep Retrovirus Is Present at High Concentration in Lung Fluid Produced by Ovine Pulmonary Adenocarcinoma-Affected Sheep and Can Survive for Several Weeks at Ambient Temperatures. Res. Vet. Sci. 2009, 87, 154–156. [Google Scholar] [CrossRef] [PubMed]
- Grego, E.; De Meneghi, D.; Álvarez, V.; Benito, A.A.; Minguijón, E.; Ortín, A.; Mattoni, M.; Moreno, B.; de Villarreal, M.P.; Alberti, A.; et al. Colostrum and Milk Can Transmit Jaagsiekte Retrovirus to Lambs. Vet. Microbiol. 2008, 130, 247–257. [Google Scholar] [CrossRef] [Green Version]
- Borobia, M.; De Las Heras, M.; Ramos, J.J.; Ferrer, L.M.; Lacasta, D.; De Martino, A.; Fernández, A.; Loste, A.; Marteles, D.; Ortín, A. Jaagsiekte Sheep Retrovirus Can Reach Peyer’s Patches and Mesenteric Lymph Nodes of Lambs Nursed by Infected Mothers. Vet. Pathol. 2016, 53, 1172–1179. [Google Scholar] [CrossRef]
- Borobia, M.; De las Heras, M.; Godino, J.; Ferrer, L.M.; Lacasta, D.; Loste, A.; Ramos, J.J.; Ortín, A. Jaagsiekte Sheep Retrovirus Found in Milk Macrophages but Not in Milk Lymphocytes or Mammary Gland Epithelia of Naturally Infected Sheep. J. VET Diagn. Investig. 2021. [Google Scholar] [CrossRef] [PubMed]
- Caporale, M.; Centorame, P.; Giovannini, A.; Sacchini, F.; Di Ventura, M.; de las Heras, M.; Palmarini, M. Infection of Lung Epithelial Cells and Induction of Pulmonary Adenocarcinoma Is Not the Most Common Outcome of Naturally Occurring JSRV Infection during the Commercial Lifespan of Sheep. Virology 2005, 338, 144–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonawane, G.G.; Tripathi, B.N.; Kumar, R.; Kumar, J. Diagnosis and Prevalence of Ovine Pulmonary Adenocarcinoma in Lung Tissues of Naturally Infected Farm Sheep. Vet. World 2016, 9, 365–370. [Google Scholar] [CrossRef] [Green Version]
- Sharp, J.M.; De Las Heras, M. Contagious Respiratory Tumors. In Diseases of Sheep; Blackwell Science: Oxford, UK, 2000; pp. 181–186. [Google Scholar]
- Rosadio, R.H.; Lairmore, M.D.; Russell, H.I.; DeMartini, J.C. Retrovirus-Associated Ovine Pulmonary Carcinoma (Sheep Pulmonary Adenomatosis) and Lymphoid Interstitial Pneumonia. I. Lesion Development and Age Susceptibility. Vet. Pathol. 1988, 25, 475–483. [Google Scholar] [CrossRef] [Green Version]
- Summers, C.; Neill, W.; Dewar, P.; Gonzalez, L.; van der Molen, R.; Norval, M.; Sharp, J.M. Systemic Immune Responses Following Infection with Jaagsiekte Sheep Retrovirus and in the Terminal Stages of Ovine Pulmonary Adenocarcinoma. J. Gen. Virol. 2002, 83, 1753–1757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weikel, J. Double infection with maedi virus and adenomatosis virus in Merino sheep. Tierarztl. Prax. 1991, 19, 596–598. [Google Scholar] [PubMed]
- Gonzalez, L.; Juste, R.A.; Cuervo, L.A.; Idigoras, I.; Saez de Ocariz, C. Pathological and Epidemiological Aspects of the Coexistence of Maedi-Visna and Sheep Pulmonary Adenomatosis. Res. Vet. Sci. 1993, 54, 140–146. [Google Scholar] [CrossRef]
- Pritchard, G.C.; Done, S.H. Concurrent Maedi-Visna Virus Infection and Pulmonary Adenomatosis in a Commercial Breeding Flock in East Anglia. Vet. Rec. 1990, 127, 197–200. [Google Scholar]
- Ortín, A.; Pérez de Villarreal, M.; Minguijón, E.; Cousens, C.; Sharp, J.M.; De las Heras, M. Coexistence of Enzootic Nasal Adenocarcinoma and Jaagsiekte Retrovirus Infection in Sheep. J. Comp. Pathol. 2004, 131, 253–258. [Google Scholar] [CrossRef]
- Jahns, H.; Cousens, C. Nasal Adenocarcinoma Associated with Jaagsiekte Sheep Retrovirus Infection in a Sheep. J. VET Diagn. Invest. 2020, 32, 152–155. [Google Scholar] [CrossRef] [PubMed]
- Scott, P. Practical Use of Ultrasound Scan in Small Ruminant Medicine and Surgery. Vet. Clin. N. Am. Food Anim. Pract. 2016, 32, 181–205. [Google Scholar] [CrossRef] [PubMed]
- Cousens, C.; Graham, M.; Sales, J.; Dagleish, M.P. Evaluation of the Efficacy of Clinical Diagnosis of Ovine Pulmonary Adenocarcinoma. Vet. Rec. 2008, 162, 88–89. [Google Scholar] [CrossRef] [PubMed]
- Cousens, C.; Scott, P.R. Assessment of Transthoracic Ultrasound Diagnosis of Ovine Pulmonary Adenocarcinoma in Adult Sheep. Vet. Rec. 2015, 177, 366. [Google Scholar] [CrossRef]
- Scott, P.R.; Sargison, N.D. Ultrasonography as an Adjunct to Clinical Examination in Sheep. Small Rumin. Res. 2010, 92, 108–119. [Google Scholar] [CrossRef]
- Scott, P.R.; Gessert, M.E. Ultrasonographic Examination of the Ovine Thorax. Vet. J. 1998, 155, 305–310. [Google Scholar] [CrossRef]
- Scott, P.R. Use of Ultrasonographic Examination in Sheep Health Management—A General Appraisal. Small Rumin. Res. 2017, 152, 2–9. [Google Scholar] [CrossRef]
- Scott, P.R. Thoracic Ultrasonography as an Adjunct to Clinical Examination in Sheep. Small Rumin. Res. 2017, 152, 107–118. [Google Scholar] [CrossRef]
- Castells, E.; Lacasta, D.; Climent, M.; Pérez, M.; Sanromán, F.; Jiménez, C.; Ferrer, L.M. Diagnostic Imaging Techniques of the Respiratory Tract of Sheep. Small Rumin. Res. 2019, 180, 112–126. [Google Scholar] [CrossRef]
- Crilly, J.P.; Politis, A.P.; Hamer, K. Use of Ultrasonographic Examination in Sheep Veterinary Practice. Small Rumin. Res. 2017, 152, 166–173. [Google Scholar] [CrossRef] [Green Version]
- Ferrer, L.M.; Ramos, J.J.; Castells, E.; Ruíz, H.; Climent, M.; Lacasta, D. Use of Computed Tomography and Thermography for the Diagnosis of Respiratory Disorders in Adult Sheep. In Sheep Farming—An Approach to Feed, Growth and Health; Monteiro, A., Ed.; IntechOpen: London, UK, 2021; ISBN 978-1-78985-975-1. [Google Scholar]
- Scott, P.R. Sheep Medicine, 2nd ed.; CRC Press—Taylor & Francis Group: Boca Raton, FL, USA, 2015; pp. 149–186. ISBN 9780367575786. [Google Scholar]
- Rodríguez-Largo, A.; Castells, E.; de Miguel, R.; Gómez, Á.; Ruiz, H.; Pérez, M.; Reina, R.; Ferrer, L.M.; Luján, L. Detection of Aluminium Hydroxide-Induced Granulomas in Sheep by Computed Tomography: A Feasible Approach for Small Ruminant Lentiviruses Diagnosis and Research. Vet. Med. Sci. 2021. [Google Scholar] [CrossRef] [PubMed]
- García-Goti, M.; González, L.; Cousens, C.; Cortabarría, N.; Extramiana, A.; Minguijón, E.; Ortín, A.; De las Heras, M.; Sharp, J. Sheep Pulmonary Adenomatosis: Characterization of Two Pathological Forms Associated with Jaagsiekte Retrovirus. J. Comp. Pathol. 2000, 122, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Khodakaram-Tafti, A.; Razavi, Z. Morphopathological Study of Naturally Occurring Ovine Pulmonary Adenocarcinoma in Sheep in Fars Province, Iran. IJVR 2010, 11, 134–138. [Google Scholar] [CrossRef]
- Kumar, M.A.; Kumar, R.; Varshney, K.C.; Palanivelu, M.; Sridhar, B.G.; Sivakumar, M. Incidence of Ovine Pulmonary Adenocarcinoma in Southern Parts of India: A Slaughter House Based Study. Indian J. Vet. Pathol. 2014, 38, 149. [Google Scholar] [CrossRef]
- Woldemeskel, M.; Tibbo, M. Pulmonary Adenomatosis and Maedi-Visna in Ethiopian Central Highland Sheep: A Microscopic Study. Trop. Anim. Health Prod. 2010, 42, 995–999. [Google Scholar] [CrossRef] [PubMed]
- Armezzani, A.; Varela, M.; Spencer, T.; Palmarini, M.; Arnaud, F. “Ménage à Trois”: The Evolutionary Interplay between JSRV, EnJSRVs and Domestic Sheep. Viruses 2014, 6, 4926–4945. [Google Scholar] [CrossRef]
- Amara, A.; Jemli, M.H.; Boutouria, M.; Chetoui, C. First case of adenomatosis in a ewe in Tunisia. Rev. Elev. Med. Vet. Pays Trop. 1994, 47, 33–34. [Google Scholar] [CrossRef]
- Azizi, S.; Tajbakhsh, E.; Fathi, F. Ovine Pulmonary Adenocarcinoma in Slaughtered Sheep: A Pathological and Polymerase Chain Reaction Study. J. S. Afr. Vet. Assoc. 2014, 85, 5. [Google Scholar] [CrossRef]
- Palmarini, M.; Fan, H.; Sharp, J.M. Sheep Pulmonary Adenomatosis: A Unique Model of Retrovirus Associated Lung Cancer. Trends Microbiol. 1997, 5, 478–483. [Google Scholar] [CrossRef]
- Cutlip, R.C.; Young, S. Sheep Pulmonary Adenomatosis (Jaagsiekte) in the United States. Am. J. Vet. Res. 1982, 43, 2108–2113. [Google Scholar]
- Bouljihad, M.; Drommer, W.; Leipold, H.W. Pathologic and Ultrastructural Findings in Sheep in Morocco with Naturally Occuring Jaagsiekte (Sheep Pulmonary Adenomatosis). Small Rumin. Res. 1996, 19, 275–280. [Google Scholar] [CrossRef]
- Toma, C.; Bâlteanu, V.A.; Tripon, S.; Trifa, A.; Rema, A.; Amorim, I.; Pop, R.M.; Popa, R.; Catoi, C.; Taulescu, M. Exogenous Jaagsiekte Sheep Retrovirus Type 2 (ExJSRV2) Related to Ovine Pulmonary Adenocarcinoma (OPA) in Romania: Prevalence, Anatomical Forms, Pathological Description, Immunophenotyping and Virus Identification. BMC Vet. Res. 2020, 16, 296. [Google Scholar] [CrossRef] [PubMed]
- Uzal, F.A.; Delhon, G.; Murcia, P.R.; De las Heras, M.; Luján, L.; Fernández Miyakawa, M.E.; Morris, W.E.; Gonzalez, M.J. Ovine Pulmonary Adenomatosis in Patagonia, Argentina. Vet. Res. Commun. 2004, 28, 159–170. [Google Scholar] [CrossRef]
- De las Heras, M.; de Martino, A.; Borobia, M.; Ortín, A.; Álvarez, R.; Borderías, L.; Giménez-Más, J.A. Solitary Tumours Associated with Jaagsiekte Retrovirus in Sheep Are Heterogeneous and Contain Cells Expressing Markers Identifying Progenitor Cells in Lung Repair. J. Comp. Pathol. 2014, 150, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Wootton, S.K.; Metzger, M.J.; Hudkins, K.L.; Alpers, C.E.; York, D.; DeMartini, J.C.; Miller, A.D. Lung Cancer Induced in Mice by the Envelope Protein of Jaagsiekte Sheep Retrovirus (JSRV) Closely Resembles Lung Cancer in Sheep Infected with JSRV. Retrovirology 2006, 3, 94. [Google Scholar] [CrossRef] [Green Version]
- Murgia, C.; Caporale, M.; Ceesay, O.; Di Francesco, G.; Ferri, N.; Varasano, V.; de las Heras, M.; Palmarini, M. Lung Adenocarcinoma Originates from Retrovirus Infection of Proliferating Type 2 Pneumocytes during Pulmonary Post-Natal Development or Tissue Repair. PLoS Pathog. 2011, 7, e1002014. [Google Scholar] [CrossRef] [Green Version]
- Sharp, J.M.; Herring, A.J. Sheep Pulmonary Adenomatosis: Demonstration of a Protein Which Crossreacts with the Major Core Proteins of Mason-Pfizer Monkey Virus and Mouse Mammary Tumour Virus. J. Gen. Virol. 1983, 64, 2323–2327. [Google Scholar] [CrossRef]
- Palmarini, M.; Dewar, P.; De las Heras, M.; Inglis, N.F.; Dalziel, R.G.; Sharp, J.M. Epithelial Tumour Cells in the Lungs of Sheep with Pulmonary Adenomatosis Are Major Sites of Replication for Jaagsiekte Retrovirus. J. Gen. Virol. 1995, 76, 2731–2737. [Google Scholar] [CrossRef]
- Bai, J.; Zhu, R.Y.; Stedman, K.; Cousens, C.; Carlson, J.; Sharp, J.M.; DeMartini, J.C. Unique Long Terminal Repeat U3 Sequences Distinguish Exogenous Jaagsiekte Sheep Retroviruses Associated with Ovine Pulmonary Carcinoma from Endogenous Loci in the Sheep Genome. J. Virol. 1996, 70, 3159–3168. [Google Scholar] [CrossRef] [Green Version]
- Voigt, K.; Brügmann, M.; Huber, K.; Dewar, P.; Cousens, C.; Hall, M.; Sharp, J.M.; Ganter, M. PCR Examination of Bronchoalveolar Lavage Samples Is a Useful Tool in Pre-Clinical Diagnosis of Ovine Pulmonary Adenocarcinoma (Jaagsiekte). Res. Vet. Sci. 2007, 83, 419–427. [Google Scholar] [CrossRef]
- De las Heras, M.; Ortín, A.; Salvatori, D.; Pérez de Villareal, M.; Cousens, C.; Miguel Ferrer, L.; Miguel Cebrián, L.; García de Jalón, J.A.; Gonzalez, L.; Michael Sharp, J. A PCR Technique for the Detection of Jaagsiekte Sheep Retrovirus in the Blood Suitable for the Screening of Ovine Pulmonary Adenocarcinoma in Field Conditions. Res. Vet. Sci. 2005, 79, 259–264. [Google Scholar] [CrossRef]
- Palmarini, M.; Mura, M.; Spencer, T.E. Endogenous Betaretroviruses of Sheep: Teaching New Lessons in Retroviral Interference and Adaptation. J. Gen. Virol. 2004, 85, 1–13. [Google Scholar] [CrossRef]
- Spencer, T.E.; Mura, M.; Gray, C.A.; Griebel, P.J.; Palmarini, M. Receptor Usage and Fetal Expression of Ovine Endogenous Betaretroviruses: Implications for Coevolution of Endogenous and Exogenous Retroviruses. J. Virol. 2003, 77, 749–753. [Google Scholar] [CrossRef] [Green Version]
- McGee-Estrada, K.; Palmarini, M.; Fan, H. HNF-3β Is a Critical Factor for the Expression of the Jaagsiekte Sheep Retrovirus Long Terminal Repeat in Type II Pneumocytes but Not in Clara Cells. Virology 2002, 292, 87–97. [Google Scholar] [CrossRef] [Green Version]
- González, L.; García-Goti, M.; Cousens, C.; Dewar, P.; Cortabarría, N.; Extramiana, A.B.; Ortín, A.; De las Heras, M.; Sharp, J.M. Jaagsiekte Sheep Retrovirus Can Be Detected in the Peripheral Blood during the Pre-Clinical Period of Sheep Pulmonary Adenomatosis. J. Gen. Virol. 2001, 82, 1355–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmarini, M.; Holland, M.J.; Cousens, C.; Dalziel, R.G.; Sharp, J.M. Jaagsiekte Retrovirus Establishes a Disseminated Infection of the Lymphoid Tissues of Sheep Affected by Pulmonary Adenomatosis. J. Gen. Virol. 1996, 77, 2991–2998. [Google Scholar] [CrossRef] [PubMed]
- Borobia, M.; Ortín, A.; Ferrer, L.M.; Ramos, J.J.; Lacasta, D.; De Las Heras, M. Cells Infected with Jaagsiekte Sheep Retrovirus Are Detected in the Bone Marrow of Asymptomatic Sheep. Can. J. Vet. Res. 2014, 78, 237–240. [Google Scholar] [PubMed]
- Lewis, F.I.; Brülisauer, F.; Cousens, C.; McKendrick, I.J.; Gunn, G.J. Diagnostic Accuracy of PCR for Jaagsiekte Sheep Retrovirus Using Field Data from 125 Scottish Sheep Flocks. Vet. J. 2011, 187, 104–108. [Google Scholar] [CrossRef] [PubMed]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quintas, H.; Pires, I.; Garcês, A.; Prada, J.; Silva, F.; Alegria, N. The Diagnostic Challenges of Ovine Pulmonary Adenocarcinoma. Ruminants 2021, 1, 58-71. https://doi.org/10.3390/ruminants1010005
Quintas H, Pires I, Garcês A, Prada J, Silva F, Alegria N. The Diagnostic Challenges of Ovine Pulmonary Adenocarcinoma. Ruminants. 2021; 1(1):58-71. https://doi.org/10.3390/ruminants1010005
Chicago/Turabian StyleQuintas, Hélder, Isabel Pires, Andreia Garcês, Justina Prada, Filipe Silva, and Nuno Alegria. 2021. "The Diagnostic Challenges of Ovine Pulmonary Adenocarcinoma" Ruminants 1, no. 1: 58-71. https://doi.org/10.3390/ruminants1010005