
Variations in Urinary Renin-Angiotensin-Aldosterone Component Concentrations in Paediatric IgA Vasculitis Nephritis
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection and Definitions
2.2. Data Collection
2.3. Sample Processing
2.4. ELISA Assay
2.4.1. Renin
2.4.2. Angiotensinogen
2.4.3. Aldosterone
2.5. Urinary Creatinine Quantification
2.6. Ethical Approval
2.7. Statistical Analysis
3. Results
3.1. Paediatric Cohort
3.2. Urinary and Plasma Renin Concentration
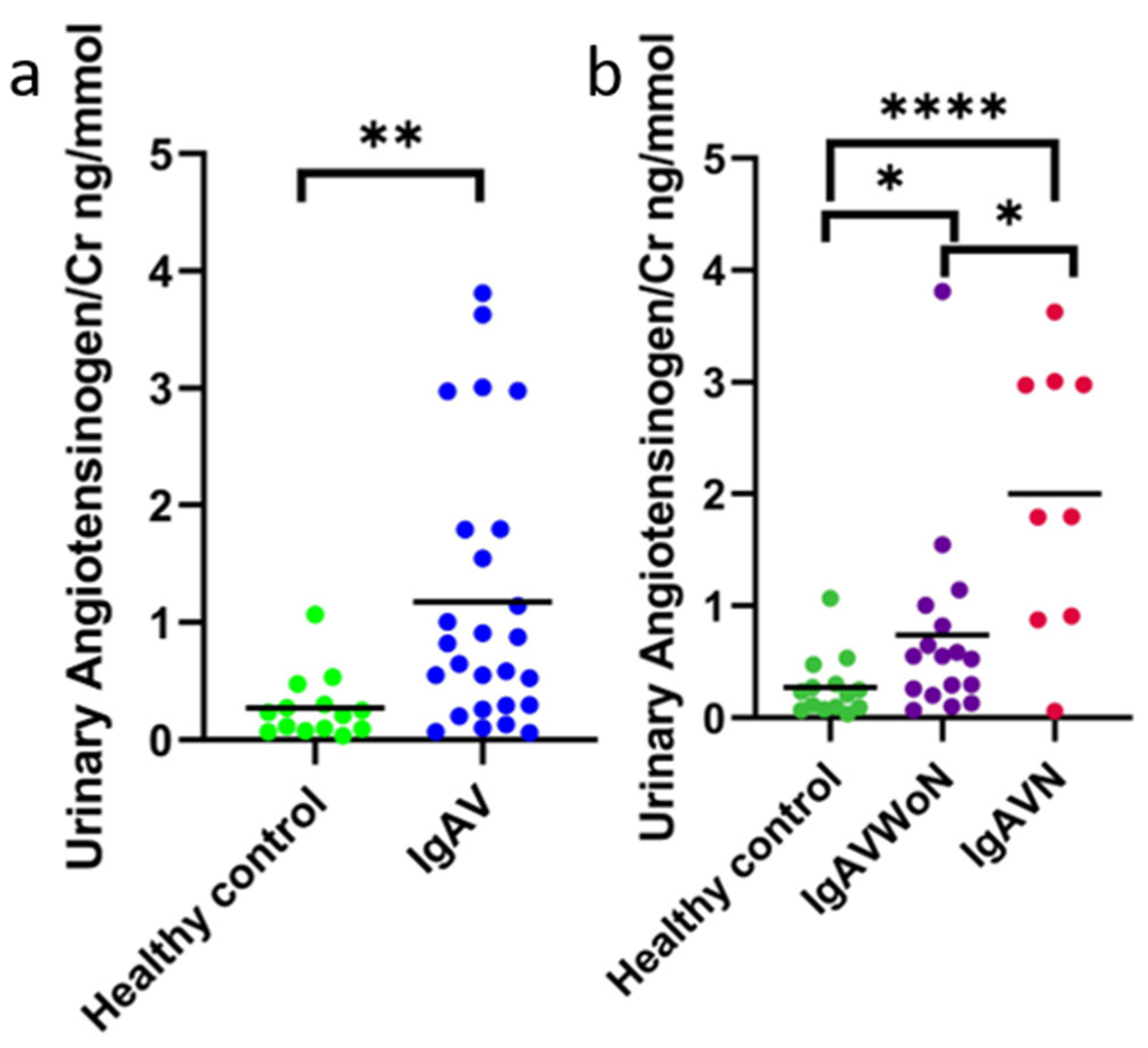
3.3. Urinary Angiotensinogen Concentration
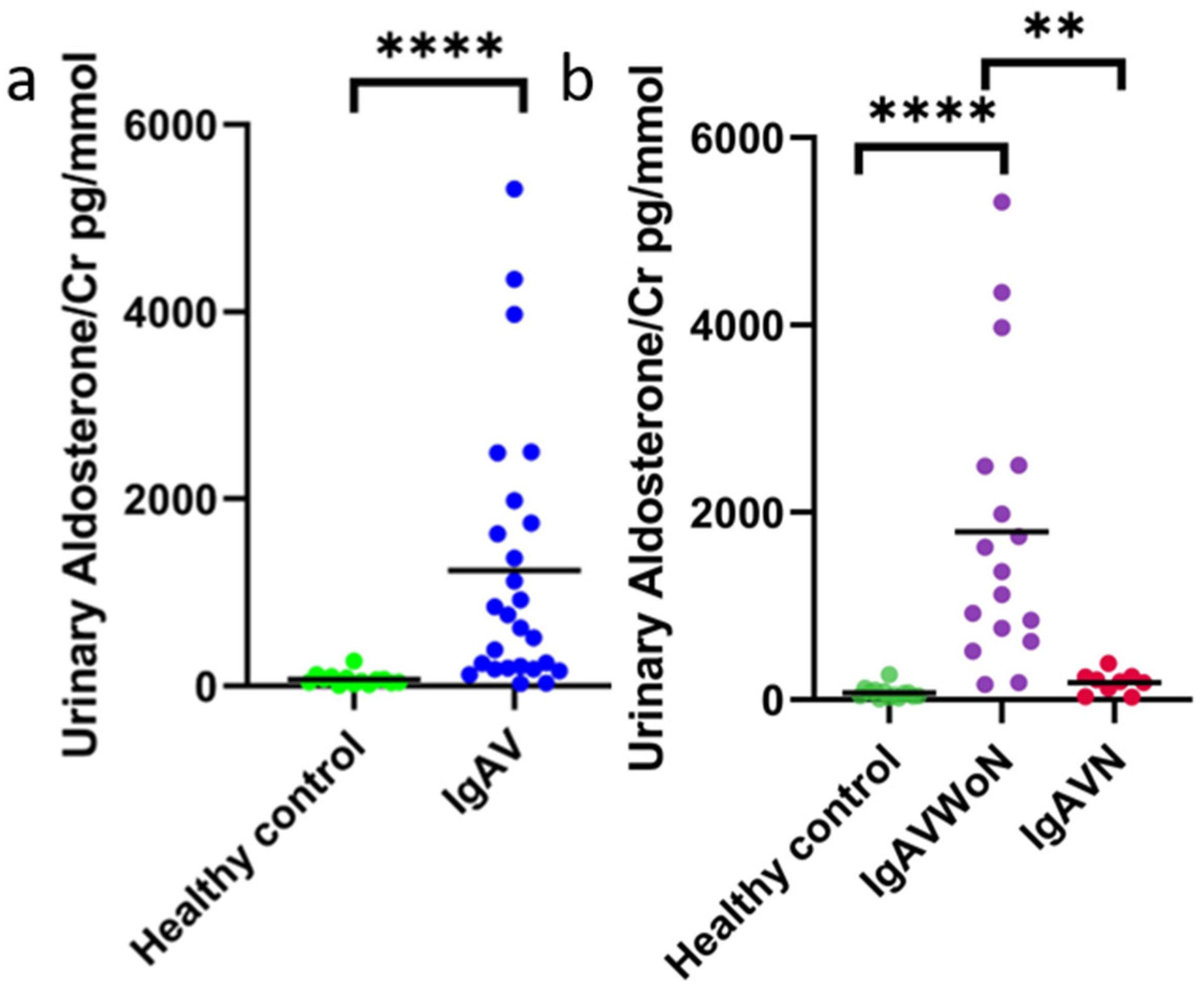
3.4. Urinary Aldosterone Concentration
3.5. Correlation to Proteinuria
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACE | angiotensin converting enzyme |
| ACEi | angiotensin converting enzyme inhibitors |
| AGT | Angiotensinogen |
| CKD | Chronic Kidney Disease |
| Cr | Creatinine |
| ELISA | Enzyme-linked immunosorbent assays |
| HC | Healthy Control |
| IgA | Immunoglobulin A |
| IgAV | Immunoglobulin A Vasculitis |
| IgAVN | Immunoglobulin A Vasculitis-Nephritis |
| IgAVwoN | Immunoglobulin A Vasculitis without Nephritis |
| IgAN | Immunoglobulin A Nephropathy |
| RAAS | Renin-angiotensinogen-aldosterone system |
| UACR | Urine albumin creatinine ratio |
References
- Jennette, J.C. Overview of the 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Clin. Exp. Nephrol. 2013, 17, 603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oni, L.; Sampath, S. Childhood IgA Vasculitis (Henoch Schonlein Purpura)—Advances and Knowledge Gaps. Front. Pediatr. 2019, 7, 257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demir, S.; Kaplan, O.; Celebier, M.; Sag, E.; Bilginer, Y.; Lay, I.; Ozen, S. Predictive Biomarkers of IgA Vasculitis with Nephritis by Metabolomic Analysis. Semin. Arthritis Rheum. 2020, 50, 1238–1244. [Google Scholar] [CrossRef] [PubMed]
- Ozen, S.; Pistorio, A.; Iusan, S.M.; Bakkaloglu, A.; Herlin, T.; Brik, R.; Buoncompagni, A.; Lazar, C.; Bilge, I.; Uziel, Y.; et al. EULAR/PRINTO/PRES Criteria for Henoch–Schönlein Purpura, Childhood Polyarteritis Nodosa, Childhood Wegener Granulomatosis and Childhood Takayasu Arteritis: Ankara 2008. Part II: Final Classification Criteria. Ann. Rheum. Dis. 2010, 69, 798–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pillebout, E. IgA Vasculitis and IgA Nephropathy: Same Disease? J. Clin. Med. 2021, 10, 2310. [Google Scholar] [CrossRef]
- Remuzzi, G.; Perico, N.; Macia, M.; Ruggenenti, P. The Role of Renin-Angiotensin-Aldosterone System in the Progression of Chronic Kidney Disease. Kidney Int. 2005, 68, S57–S65. [Google Scholar] [CrossRef] [Green Version]
- Thethi, T.; Kamiyama, M.; Kobori, H. The Link between the Renin-Angiotensin-Aldosterone System and Renal Injury in Obesity and the Metabolic Syndrome. Curr. Hypertens. Rep. 2012, 14, 160–169. [Google Scholar] [CrossRef] [Green Version]
- Praga, M.; Gutiérrez, E.; González, E.; Morales, E.; Hernandez, E. Treatment of IgA Nephropathy with Ace Inhibitors: A Randomized and Controlled Trial. J. Am. Soc. Nephrol. 2003, 14, 1578–1583. [Google Scholar] [CrossRef] [Green Version]
- Van den Belt, S.M.; Heerspink, H.J.L.; Gracchi, V.; de Zeeuw, D.; Wühl, E.; Schaefer, F.; Anarat, A.; Bakkaloglu, A.; Ozaltin, F.; Peco-Antic, A.; et al. Early Proteinuria Lowering by Angiotensin-Converting Enzyme Inhibition Predicts Renal Survival in Children with CKD. J. Am. Soc. Nephrol. 2018, 29, 2225–2233. [Google Scholar] [CrossRef] [Green Version]
- Marro, J.; Chetwynd, A.J.; Wright, R.D.; Dliso, S.; Oni, L. Urinary Protein Array Analysis to Identify Key Inflammatory Markers in Children with IgA Vasculitis Nephritis. Children 2022, 9, 622. [Google Scholar] [CrossRef]
- Briet, M.; Schiffrin, E.L. Vascular Actions of Aldosterone. J. Vasc. Res. 2013, 50, 89–99. [Google Scholar] [CrossRef]
- Franiek, A.; Sharma, A.; Cockovski, V.; Wishart, D.S.; Zappitelli, M.; Blydt-Hansen, T.D. Urinary Metabolomics to Develop Predictors for Pediatric Acute Kidney Injury. Pediatr. Nephrol. 2022, 37, 2079–2090. [Google Scholar] [CrossRef]
- Williams, C.E.C.; Toner, A.; Wright, R.D.; Oni, L. A Systematic Review of Urine Biomarkers in Children with IgA Vasculitis Nephritis. Pediatr. Nephrol. 2021, 36, 3033–3044. [Google Scholar] [CrossRef]
- Counahan, R.; Winterborn, M.H.; White, R.H.; Heaton, J.M.; Meadow, S.R.; Bluett, N.H.; Swetschin, H.; Cameron, J.S.; Chantler, C. Prognosis of Henoch-Schönlein Nephritis in Children. Br. Med. J. 1977, 2, 11–14. [Google Scholar] [CrossRef] [Green Version]
- Lurbe, E.; Agabiti-Rosei, E.; Cruickshank, J.K.; Dominiczak, A.; Erdine, S.; Hirth, A.; Invitti, C.; Litwin, M.; Mancia, G.; Pall, D.; et al. 2016 European Society OfHypertension Guidelines for Themanagement of High Blood Pressure in Children and Adolescents. J. Hypertens. 2016, 34, 1887–1920. [Google Scholar] [CrossRef] [Green Version]
- Asano, K.; Iwasaki, H.; Fujimura, K.; Ikeda, M.; Sugimoto, Y.; Matsubara, A.; Yano, K.; Irisawa, H.; Kono, F.; Kanbe, M.; et al. Automated Microanalysis of Creatinine by Coupled Enzyme Reactions. Hiroshima J. Med. Sci. 1992, 41, 1–5. [Google Scholar]
- Mukaka, M.M. A Guide to Appropriate Use of Correlation Coefficient in Medical Research. Malawi Med. J. 2012, 24, 69. [Google Scholar]
- Burns, K.D.; Hiremath, S. Urinary Angiotensinogen as a Biomarker of Chronic Kidney Disease: Ready for Prime Time? Nephrol. Dial. Transplant. 2012, 27, 3010–3013. [Google Scholar] [CrossRef]
- Struthers, A. Review of Aldosterone- and Angiotensin II-Induced Target Organ Damage and Prevention. Cardiovasc. Res. 2004, 61, 663–670. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.-G.; Song, S.-B.; Lee, S.-H.; Moon, J.-Y.; Jeong, K.-H.; Lee, T.-W.; Ihm, C.-G. Urinary Angiotensinogen as a Predictive Marker in Patients with Immunoglobulin A Nephropathy. Clin. Exp. Nephrol. 2011, 15, 720–726. [Google Scholar] [CrossRef]
- Kobori, H.; Navar, L.G. Urinary Angiotensinogen as a Novel Biomarker of Intrarenal Renin-Angiotensin System in Chronic Kidney Disease. Int. Rev. Thromb 2011, 6, 108. [Google Scholar]
- Sparks, M.A.; Crowley, S.D.; Gurley, S.B.; Mirotsou, M.; Coffman, T.M. Classical Renin-Angiotensin System in Kidney Physiology. Compr. Physiol. 2014, 4, 1201–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mills, K.T.; Kobori, H.; Hamm, L.L.; Alper, A.B.; Khan, I.E.; Rahman, M.; Navar, L.G.; Liu, Y.; Browne, G.M.; Batuman, V.; et al. Increased Urinary Excretion of Angiotensinogen Is Associated with Risk of Chronic Kidney Disease. Nephrol. Dial. Transplant. 2012, 27, 3176–3181. [Google Scholar] [CrossRef] [PubMed]
- Takamatsu, M.; Urushihara, M.; Kondo, S.; Shimizu, M.; Morioka, T.; Oite, T.; Kobori, H.; Kagami, S. Glomerular Angiotensinogen Protein Is Enhanced in Pediatric IgA Nephropathy. Pediatr. Nephrol. 2008, 23, 1257–1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, Y.N.; Liu, W.; Li, Y.G.; Jia, G.C.; Zhang, Z.; Guan, Y.J.; Zhou, X.F.; Liu, Y.F. Urinary Angiotensinogen Levels in Relation to Renal Involvement of Henoch-Schonlein Purpura in Children. Nephrology 2012, 17, 53–57. [Google Scholar] [CrossRef]
- He, X.; Yin, W.; Ding, Y.; Cui, S.J.; Luan, J.; Zhao, P.; Yue, X.; Yu, C.; Laing, X.; Zhao, Y.L. Higher Serum Angiotensinogen Is an Indicator of IgA Vasculitis with Nephritis Revealed by Comparative Proteomes Analysis. PLoS ONE 2015, 10, e0130536. [Google Scholar] [CrossRef] [Green Version]
- Rudnicki, M.; Mayer, G. Significance of Genetic Polymorphisms of the Renin–Angiotensin–Aldosterone System in Cardiovascular and Renal Disease. Pharmacogenomics 2009, 10, 463–476. [Google Scholar] [CrossRef]
- Chen, S.; Zhang, L.; Wang, H.W.; Wang, X.Y.; Li, X.Q.; Zhang, L.L. The M235T Polymorphism in the Angiotensinogen Gene and Heart Failure: A Meta-Analysis. JRAAS—J. Renin-Angiotensin-Aldosterone Syst. 2014, 15, 190–195. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.D.; Lin, F.J.; Li, X.J.; Wang, L.R.; Jiang, G.R. Genetic Polymorphisms of the Renin-Angiotensin-Aldosterone System in Chinese Patients with End-Stage Renal Disease Secondary to IgA Nephropathy. Chin. Med. J. 2010, 123, 3238–3242. [Google Scholar] [CrossRef]
- Urushihara, M.; Nagai, T.; Kinoshita, Y.; Nishiyama, S.; Suga, K.; Ozaki, N.; Jamba, A.; Kondo, S.; Kobori, H.; Kagami, S. Changes in Urinary Angiotensinogen Posttreatment in Pediatric IgA Nephropathy Patients. Pediatr. Nephrol. 2015, 30, 975–982. [Google Scholar] [CrossRef] [Green Version]
- Brown, N.J. Contribution of Aldosterone to Cardiovascular and Renal Inflammation and Fibrosis. Nat. Rev. Nephrol. 2013, 9, 459–469. [Google Scholar] [CrossRef]
- Brown, N.J. Aldosterone and Vascular Inflammation. Hypertension 2008, 51, 161–167. [Google Scholar] [CrossRef] [Green Version]
- Leung, J.C.K.; Chan, L.Y.Y.; Tang, S.C.W.; Lam, M.F.; Chow, C.W.; Lim, A.I.; Lai, K.N. Oxidative Damages in Tubular Epithelial Cells in IgA Nephropathy: Role of Crosstalk between Angiotensin II and Aldosterone. J. Transl. Med. 2011, 9, 169. [Google Scholar] [CrossRef]
- Camilla, R.; Suzuki, H.; Daprà, V.; Loiacono, E.; Peruzzi, L.; Amore, A.; Ghiggeri, G.M.; Mazzucco, G.; Scolari, F.; Gharavi, A.G.; et al. Oxidative Stress and Galactose-Deficient IgA1 as Markers of Progression in IgA Nephropathy. Clin. J. Am. Soc. Nephrol. 2011, 6, 1903–1911. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall | IgAVN | IgAVwoN | HC | p-Value | |
|---|---|---|---|---|---|
| n (%) | 40 (100%) | 9 (23%) | 17 (43%) | 14 (35%) | - |
| Male a | 23 (28%) | 6 (67%) | 10 (59%) | 7 (50%) | 0.725 |
| Age, years b | 8.3 ± 3.3 | 8.3 ± 3.5 | 6.7 ± 3.0 | 10.3 ± 2.7 + | 0.006 |
| Ethnicity British African Chinese Any other Asian background Not stated | 32 (80%) 3 (8%) 2 (5%) 1 (3%) 2 (5%) | 7 (79%) 0 (0%) 0 (0%) 0 (0%) 2 (22%) | 15 (88%) 0 (0%) 2 (12%) 0 (0%) 0 (0%) | 10 (71%) 3 (21%) 0 (0%) 1 (7%) 0 (0%) | |
| Sampling | |||||
| Sample type | |||||
| Urine and blood a | 19 (100%) | 5 (26%) | 5 (26%) | 9 (47%) | |
| Urine only a | 26 (100%) | 3 (12%) | 18 (69%) | 5 (19%) | |
| Blood only a | 5 (100%) | 5 (100%) | - | - | |
| Weeks from diagnosis to sampling b | 18.4 ± 60.0 | 49.7 ± 97.8 | 1.8 ± 0.9 | - | <0.001 |
| Renal involvement | |||||
| Hypertension a,1 | 4 (23.5%) | 3 (33.3%) | 1 (12.5%) | - | 0.312 |
| Serum creatinine mg/dL b,2 | 51.5 ± 18.5 | 53.3 ± 17.2 | 48.6 ± 22.1 | - | 0.769 |
| Serum albumin g/L b,3 | 39.3 ± 4.3 | 37.1 ± 3.1 | 43.0 ± 3.7 | - | 0.029 |
| UACR mmol/mg b | 90.7 ± 147.6 | 257.8 ± 141.2 | 2.2 ± 5.5 | - | <0.001 |
| Urinary creatinine mmol/L b | 8.7 ± 7.6 | 6.2 ± 4.7 | 7.7 ± 7.7 | 11.5 ± 8.4 | 0.146 |
| Biopsy proven nephritis a | 4 (44%) | ||||
| ISKDC Grade IIIa a IIIb a IV a | - - - | 1 (25%) 2 (50%) 1 (25%) | - - - | - - - | - - - |
| Medications | |||||
| Corticosteroids a | 2 | ||||
| Follow-up | |||||
| Months b | 11.4 ± 17.1 | 23.2 ± 25.0 | 5.1 ± 5.2 | - | 0.005 |
| UACR at last review b | 10.9 ± 20.5 | 31.6 ± 24.0 | 0.0 ± 0.0 | - | <0.001 |
| Outcome a | Full remission, 4 (44%) Partial remission, 5 (56%) Worsened, 0 (0%) |
| Pearson r | p-Value | |
|---|---|---|
| Urinary AGT/Cr | 0.502 | 0.009 |
| Urinary aldosterone/Cr | −0.444 | 0.023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chetwynd, A.J.; Marro, J.; Northey, S.J.; Hughes, D.J.; Oni, L. Variations in Urinary Renin-Angiotensin-Aldosterone Component Concentrations in Paediatric IgA Vasculitis Nephritis. Int. J. Transl. Med. 2022, 2, 597-606. https://doi.org/10.3390/ijtm2040045
Chetwynd AJ, Marro J, Northey SJ, Hughes DJ, Oni L. Variations in Urinary Renin-Angiotensin-Aldosterone Component Concentrations in Paediatric IgA Vasculitis Nephritis. International Journal of Translational Medicine. 2022; 2(4):597-606. https://doi.org/10.3390/ijtm2040045
Chicago/Turabian StyleChetwynd, Andrew J., Julien Marro, Sarah J. Northey, Daniel J. Hughes, and Louise Oni. 2022. "Variations in Urinary Renin-Angiotensin-Aldosterone Component Concentrations in Paediatric IgA Vasculitis Nephritis" International Journal of Translational Medicine 2, no. 4: 597-606. https://doi.org/10.3390/ijtm2040045