
The Promising Role of Mushrooms as a Therapeutic Adjuvant of Conventional Cancer Therapies


Abstract
:1. Introduction
2. Results
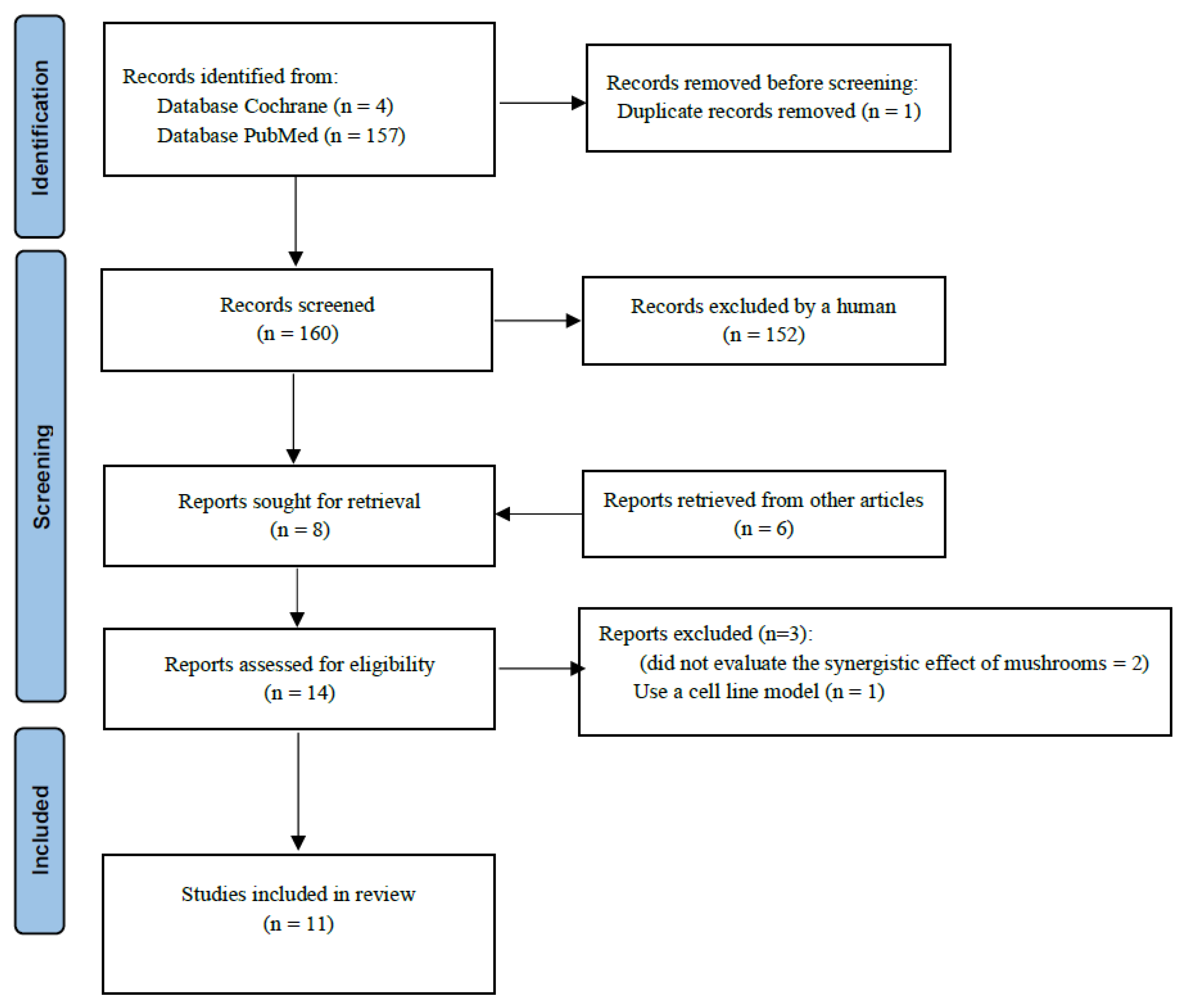
2.1. Characteristics of the Included Studies
2.2. Quality of Included Studies
2.3. Adverse Effects Associated with Mushroom Compounds Use as an Adjuvant on Conventional Cancer Therapies
2.4. Hematological Parameters Associated with Mushroom Compounds/Extracts Use as an Adjuvant in Conventional Cancer Therapies
2.5. Immunological Parameters Associated with Mushroom Compounds/Extracts Use as an Adjuvant in Conventional Cancer Therapies
2.6. Quality of Life Associated with Mushroom Compounds/Extracts Use as an Adjuvant in Conventional Cancer Therapies
3. Discussion
4. Materials and Methods
4.1. Outcome Measures
4.2. Data Extraction
4.3. Quality Assessment
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2020; Volume 68. [Google Scholar]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ayeka, P.A. Potential of Mushroom Compounds as Immunomodulators in Cancer Immunotherapy: A Review. Evid.-Based Complementary Altern. Med. 2018, 2018, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jeitler, M.; Michalsen, A.; Frings, D.; Hübner, M.; Fischer, M.; Koppold-Liebscher, D.A.; Murthy, V.; Kessler, C.S. Significance of Medicinal Mushrooms in Integrative Oncology: A Narrative Review. Front. Pharmacol. 2020, 11, 580656. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Zhang, Q.; Zhao, L.; Huang, X.; Wang, J.; Kang, X. Spore Powder of Ganoderma Lucidum Improves Cancer-Related Fatigue in Breast Cancer Patients Undergoing Endocrine Therapy: A Pilot Clinical Trial. Evid.-Based Complement. Altern. Med. 2012, 2012, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Grant, S.J.; Hunter, J.; Seely, D.; Balneaves, L.G.; Rossi, E.; Bao, T. Integrative Oncology: International Perspectives. Integr. Cancer Ther. 2019, 18, 1534735418823266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozarski, M.; Klaus, A.; Jakovljevic, D.; Todorovic, N.; Vunduk, J.; Petrović, P.; Niksic, M.; Vrvic, M.M.; van Griensven, L. Antioxidants of Edible Mushrooms. Molecules 2015, 20, 19489–19525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elsayed, E.A.; el Enshasy, H.; Wadaan, M.A.M.; Aziz, R. Mushrooms: A Potential Natural Source of Anti-Inflammatory Compounds for Medical Applications. Mediat. Inflamm. 2014, 2014, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.K.; Dutta, S.D.; Ganguly, K.; Cho, S.J.; Lim, K.T. Mushroom-Derived Bioactive Molecules as Immunotherapeutic Agents: A Review. Molecules 2021, 26, 1359. [Google Scholar] [CrossRef] [PubMed]
- Blagodatski, A.; Yatsunskaya, M.; Mikhailova, V.; Tiasto, V.; Kagansky, A.; Katanaev, V.L. Medicinal Mushrooms as an Attractive New Source of Natural Compounds for Future Cancer Therapy. Oncotarget 2018, 9, 29259–29274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, T.P.; Chanda, W.; Padhiar, A.A.; Batool, S.; LiQun, S.; Zhong, M.T.; Huang, M. A Preclinical Evaluation of the Antitumor Activities of Edible and Medicinal Mushrooms: A Molecular Insight. Integr. Cancer Ther. 2018, 17, 200–209. [Google Scholar] [CrossRef] [Green Version]
- Figueiredo, L.; Régis, W.C.B. Medicinal Mushrooms in Adjuvant Cancer Therapies: An Approach to Anticancer Effects and Presumed Mechanisms of Action. Nutrire 2017, 42, 28. [Google Scholar] [CrossRef] [Green Version]
- Zmitrovich, I.v.; Belova, N.v.; Balandaykin, M.E.; Bondartseva, M.A.; Wasser, S.P. Cancer without Pharmacological Illusions and a Niche for Mycotherapy (Review). Int. J. Med. Mushrooms 2019, 21, 105–119. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, B.; Liang, Q.; Fenix, K.; Tamang, B.; Hauben, E.; Ma, L.; Zhang, W. Combining the Anticancer and Immunomodulatory Effects of Astragalus and Shiitake as an Integrated Therapeutic Approach. Nutrients 2021, 13, 2564. [Google Scholar] [CrossRef] [PubMed]
- Chay, W.Y.; Tham, C.K.; Toh, H.C.; Lim, H.Y.; Tan, C.K.; Lim, C.; Wang, W.W.; Choo, S.P. Coriolus Versicolor (Yunzhi) Use as Therapy in Advanced Hepatocellular Carcinoma Patients with Poor Liver Function or Who Are Unfit for Standard Therapy. J. Altern. Complement. Med. 2017, 23, 648–652. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.Y.; Hung, Y.C.; Chen, Y.H.; Chen, Y.H.; Huang, Y.C.; Kao, C.W.; Su, Y.L.; Chiu, H.H.E.; Rau, K.M. A Preliminary Randomised Controlled Study of Short-Term Antrodia Cinnamomea Treatment Combined with Chemotherapy for Patients with Advanced Cancer. BMC Complement. Altern. Med. 2016, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Tangen, J.M.; Tierens, A.; Caers, J.; Binsfeld, M.; Olstad, O.K.; Trøseid, A.M.S.; Wang, J.; Tjønnfjord, G.E.; Hetland, G. Immunomodulatory Effects of the Agaricus Blazei Murrill-Based Mushroom Extract Andosan in Patients with Multiple Myeloma Undergoing High Dose Chemotherapy and Autologous Stem Cell Transplantation: A Randomized, Double Blinded Clinical Study. BioMed Res. Int. 2015, 2015, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Nagashima, Y.; Maeda, N.; Yamamoto, S.; Yoshino, S.; Oka, M. Evaluation of Host Quality of Life and Immune Function in Breast Cancer Patients Treated with Combination of Adjuvant Chemotherapy and Oral Administration of Lentinula Edodes Mycelia Extract. OncoTargets Ther. 2013, 6, 853–859. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, N.; Takimoto, Y.; Suzuki, R.; Arai, T.; Uebaba, K.; Nakai, M.; Strong, J.M.; Tokuda, H. Efficacy of Oral Administration of Lentinula Eododes Mycelia Extract for Breast Cancer Patients Undergoing Postoperative Hormone Therapy. Asian Pac. J. Cancer Prev. 2013, 14, 3469–3472. [Google Scholar] [CrossRef] [Green Version]
- Valadares, F.; Novaes, M.R.C.G.; Villafranca, R.C.; Menezes, M.D.C.; Reis, M.C.; Goncalves, D.R. Effect of Dietary Supplementation with Agaricus Sylvaticus Fungus on the Hematology and Immunology Systems of Breast Cancer Patients Undergoing Chemotherapy. Turk. Bull. Hyg. Exp. Biol. 2011, 68, 59–72. [Google Scholar] [CrossRef]
- Okuno, K.; Uno, K. Efficacy of Orally Administered Lentinula Edodes Mycelia Extract for Advanced Gastrointestinal Cancer Patients Undergoing Cancer Chemotherapy: A Pilot Study. Asian Pac. J. Cancer Prev. 2011, 12, 1671–1674. [Google Scholar]
- Valadares, F.; Novaes, M.R.C.G.; Cañete, R. Effect of Agaricus Sylvaticus Supplementation on Nutritional Status and Adverse Events of Chemotherapy of Breast Cancer: A Randomized, Placebo-Controlled, Double-Blind Clinical Trial. Indian J. Pharmacol. 2013, 45, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, Y.; Miyahara, E.; Hihara, J. Efficacy and Safety of Orally Administered Lentinula Edodes Mycelia Extract for Patients Undergoing Cancer Chemotherapy: A Pilot Study. Am. J. Chin. Med. 2011, 39, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Ahn, W.S.; Kim, D.J.; Chae, G.T.; Lee, J.M.; Bae, S.M.; Sin, J.I.; Kim, Y.W.; Namkoong, S.E.; Lee, I.P. Natural Killer Cell Activity and Quality of Life Were Improved by Consumption of a Mushroom Extract, Agaricus Blazei Murill Kyowa, in Gynecological Cancer Patients Undergoing Chemotherapy. Int. J. Gynecol. Cancer 2004, 14, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Baldo, P.; Fornasier, G.; Ciolfi, L.; Sartor, I.; Francescon, S. Pharmacovigilance in Oncology. Int. J. Clin. Pharm. 2018, 40, 832–841. [Google Scholar] [CrossRef] [Green Version]
- Weng, Y.P.; Hong, R.M.; Chen, V.C.H.; Tsai, C.J.; Yeh, D.C.; Fang, Y.H. Sleep Quality and Related Factors in Patients with Breast Cancer: A Cross-Sectional Study in Taiwan. Cancer Manag. Res. 2021, 13, 4725–4733. [Google Scholar] [CrossRef]
- Otte, J.L.; Carpenter, J.S.; Manchanda, S.; Rand, K.L.; Skaar, T.C.; Weaver, M.; Chernyak, Y.; Zhong, X.; Igega, C.; Landis, C. Systematic Review of Sleep Disorders in Cancer Patients: Can the Prevalence of Sleep Disorders Be Ascertained? Cancer Med. 2015, 4, 183–200. [Google Scholar] [CrossRef] [Green Version]
- Ravasco, P. Nutrition in Cancer Patients. J. Clin. Med. 2019, 8, 1211. [Google Scholar] [CrossRef] [Green Version]
- El Enshasy, H.A.; Hatti-Kaul, R. Mushroom immunomodulators: Unique molecules with unlimited applications. Trends Biotechnol. 2013, 31, 668–677. [Google Scholar] [CrossRef]
- Guggenheim, A.G.; Wright, K.M.; Zwickey, H.L. Immune modulation from five major mushrooms: Application to integrative oncology. Integr. Med. 2014, 13, 32–44. [Google Scholar]
- Jin, X.; Ruiz Beguerie, J.; Sze, D.M.Y.; Chan, G.C.F. Ganoderma Lucidum (Reishi Mushroom) for Cancer Treatment. Cochrane Database Syst. Rev. 2016, 2016, CD007731. [Google Scholar] [CrossRef]
- Chen, L.; Kong, X.; Yan, C.; Fang, Y.; Wang, J. The Research Progress on the Prognostic Value of the Common Hematological Parameters in Peripheral Venous Blood in Breast Cancer. OncoTargets Ther. 2020, 13, 1397–1412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neergheen, V.S.; Hip Kam, A.; Pem, Y.; Ramsaha, S.; Bahorun, T. Regulation of Cancer Cell Signaling Pathways as Key Events for Therapeutic Relevance of Edible and Medicinal Mushrooms. Semin. Cancer Biol. 2020, in press. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author (Year) | Country | Species Name | Type of Study | Sample Size | Cancer Type | Conventional Therapy (CT) | Treatment (T) | Duration of Treatment | Outcomes Measures | Significant Findings |
|---|---|---|---|---|---|---|---|---|---|---|
| Chay et al. (2017) [15] | Singapore | Coriolus versicolor | Clinical trial | CT: 6 T: 9 | Advanced hepatocellular carcinoma | Placebo | Standard continuous daily dose of 2.4 g | CT: 1.5 cycles (5.9 weeks) T: 3 cycles (12.1 weeks) | Primary outcomes: median time to progression. Secondary outcomes: response rates, toxicity, quality of life, progression-free survival, and overall survival. | Better social and emotional functioning scores. Better appetite. Less pain symptoms. |
| Tsai et al. (2016) [16] | Taiwan | Antrodia cinnamomea (AC) | Randomized clinical trial | CT: 20 T: 17 | Advanced or recurrent, untreated, stage III–IV adenocarcinomas | Chemotherapy + placebo | Chemotherapy + A. cinnamomea (orally, 20 mL twice daily) | 30 days | Primary outcomes: 6-month overall survival. Secondary outcomes: disease control rate, quality of life, adverse event, and biochemical features. | Improvements in quality of sleep. |
| Tangen et al. (2015) [17] | Norway | 82.4% of Agaricus blazei Murill, 14.7% of Hericium erinaceus, and 2.9% of Grifola frondosa (AndoSan) | Randomized clinical trial | CT: 21 T: 19 | Multiple myeloma | Chemotherapy with autologous stem cell support + placebo | Chemotherapy with autologous stem cell support + AndoSan (60 mL daily orally) | 7 weeks | Primary outcomes: serum levels of cytokines, chemokines, and growth factors; expression levels of genes involved in immune activation by whole genome assay; stem cell harvest product of several mononuclear cell subsets associated with the immune system. Primary outcomes: overall survival, quality of life. | Increase in serum levels of IL-1, IL-5 and IL-7. Increased expression of immunoglobulin genes, killer immunoglobulin receptor genes and HLA genes. |
| Nagashima et al. (2013) [18] | Japan | Lentinula edodes (LEM) | Open-label trial with a single group | 10 | Breast cancer | Chemotherapy alone (3 weeks) | LEM (1800 mg/day) + chemotherapy (3 weeks) | 6 weeks (3 weeks each) | Primary outcomes: quality of life and immune function. | Not achieved. |
| Suzuki et al. (2013) [19] | Japan | Lentinula edodes (LEM) | Single-arm, open-label study | 20 | Breast cancer | Hormone therapy (4 weeks) | Hormone therapy + LEM (oral ingestion at 1800 mg daily) (8 weeks) | 12 weeks | Primary outcomes: quality of life and peripheral blood cytokine production levels. | Not achieved. |
| Valadares et al. (2013) [20] | Brazil | Agaricus sylvaticus | Randomized clinical trial | CT: 23 T: 23 | Breast cancer | Chemotherapy + placebo | Chemotherapy + A. sylvaticus (2.1 g, in two daily administrations) | 3–6 months (21 days cycles) | Primary outcomes: adverse events. | Improved nutritional status and reduced abnormal bowel functions, nausea, vomiting, and anorexia. |
| Zhao et al. (2012) [5] | China | Ganoderma lucidum | Randomized controlled trial | CT: 23 T: 25 | Breast cancer | Placebo | Spore powder of G. lucidum (1000 mg 3 times a day) | 4 weeks | Primary outcomes: functional assessment of cancer therapy-fatigue (FACT-F), hospital anxiety and depression scale (HADS), EORTC quality-of life questionnaires (QLQ-C30). Secondary outcomes: TNF-α, IL-6, and liver-kidney function. | Beneficial effects on cancer-related fatigue and quality of life in breast cancer patients undergoing endocrine therapy. |
| Okuno and Uno (2011) [21] | Japan | Lentinula edodes (LEM) | Single-group open study | 8 | Gastric and colorectal cancer | Chemotherapy alone (4 weeks) | Chemotherapy + LEM (1800 mg/day) (4 weeks) | 8 weeks (4 weeks each) | Primary outcomes: adverse events and IFN-γ production by CD4+ T, CD8+ T and CD56+ NK/NKT cells. | Decrease in the incidence of adverse effects. |
| Valadares et al. (2011) [22] | Brazil | Agaricus sylvaticus | Randomized controlled trial | CT: 23 T: 23 | Breast cancer | Chemotherapy + placebo | Chemotherapy + A. sylvaticus (2.1 g/day) | 6 months | Primary outcomes: hematological and immunological parameters. | Increase of hematocrit, red blood count, MCHC, leukocytes, monocytes, and total lymphocyte count. |
| Yamaguchi et al. (2011) [23] | Japan | Lentinula edodes (LEM) | Single-group open study | 7 | Breast (3 patients), gastrointestinal (2 patients) or to prevent recurrence of gastrointestinal cancer (2 patients) | Chemotherapy | Chemotherapy + LEM (1800 mg/day for four weeks) | 8 weeks | Primary outcomes: safety, quality of life and immune response. | Increase in LAK cell activity and NK cell activity and a decrease in IAP levels. |
| Ahn et al. (2004) [24] | South Korea | Agaricus blazei Murill Kyowa (ABMK) | Randomized clinical trial | CT: 61 T: 39 | Gynecological cancer (cervical, ovarian and endometrial) | Chemotherapy + placebo | Chemotherapy + ABMK (daily oral consumption) | 3 weeks for at least three cycles | Primary outcomes: activities of NK and LAK cells and the counts of white blood cells, lymphocytes, monocytes, CD3þ, CD4þ, CD8þ, CD48þ, and CD56þ cells. | ABMK treatment might be beneficial for gynecological cancer patients undergoing chemotherapy. |
| Quality Assessment of Controlled Intervention Studies | ||||
|---|---|---|---|---|
| No | Question | Number of Studies (n = 7) | ||
| Yes | No | Other (CD, NA, NR) | ||
| 1 | Was the study described as randomized, a randomized trial, a randomized clinical trial, or an RCT? | 7 | 0 | 0 |
| 2 | Was the method of randomization adequate (i.e., use of randomly generated assignment)? | 2 | 0 | 5 |
| 3 | Was the treatment allocation concealed (so that assignments could not be predicted)? | 2 | 0 | 5 |
| 4 | Were study participants and providers blinded to treatment group assignment? | 4 | 0 | 3 |
| 5 | Were the people assessing the outcomes blinded to the participants’ group assignments? | 4 | 0 | 3 |
| 6 | Were the groups similar at baseline on important characteristics that could affect outcomes (e.g., demographics, risk factors, co-morbid conditions)? | 1 | 3 | 3 |
| 7 | Was the overall drop-out rate from the study at endpoint 20% or lower of the number allocated to treatment? | 6 | 1 | 0 |
| 8 | Was the differential drop-out rate (between treatment groups) at endpoint 15 percentage points or lower? | 6 | 1 | 0 |
| 9 | Was there high adherence to the intervention protocols for each treatment group? | 7 | 0 | 0 |
| 10 | Were other interventions avoided or similar in the groups (e.g., similar background treatments)? | 6 | 1 | 0 |
| 11 | Were outcomes assessed using valid and reliable measures, implemented consistently across all study participants? | 7 | 0 | 0 |
| 12 | Did the authors report that the sample size was sufficiently large to be able to detect a difference in the main outcome between groups with at least 80% power? | 1 | 6 | 0 |
| 13 | Were outcomes reported or subgroups analyzed prespecified (i.e., identified before analyses were conducted)? | 2 | 0 | 5 |
| 14 | Were all randomized participants analyzed in the group to which they were originally assigned, i.e., did they use an intention-to-treat analysis? | 1 | 0 | 6 |
| Quality Assessment Tool for Before-After (Pre-Post) Studies with No Control Group | ||||
|---|---|---|---|---|
| No | Question | Number of Studies (n = 4) | ||
| Yes | No | Other (CD, NA, NR) | ||
| 1 | Was the study question or objective clearly stated? | 3 | 1 | 0 |
| 2 | Were eligibility/selection criteria for the study population prespecified and clearly described? | 4 | 0 | 0 |
| 3 | Were the participants in the study representative of those who would be eligible for the test/service/intervention in the general or clinical population of interest? | 0 | 4 | 0 |
| 4 | Were all eligible participants that met the prespecified entry criteria enrolled? | 4 | 0 | 0 |
| 5 | Was the sample size sufficiently large to provide confidence in the findings? | 0 | 4 | 0 |
| 6 | Was the test/service/intervention clearly described and delivered consistently across the study population? | 4 | 0 | 0 |
| 7 | Were the outcome measures prespecified, clearly defined, valid, reliable, and assessed consistently across all study participants? | 4 | 0 | 0 |
| 8 | Were the people assessing the outcomes blinded to the participants’ exposures/interventions? | 0 | 0 | 4 |
| 9 | Was the loss to follow-up after baseline 20% or less? Were those lost to follow-up accounted for in the analysis? | 4 | 0 | 0 |
| 10 | Did the statistical methods examine changes in outcome measures from before to after the intervention? Were statistical tests done that provided p values for the pre-to-post changes? | 4 | 0 | 0 |
| 11 | Were outcome measures of interest taken multiple times before the intervention and multiple times after the intervention (i.e., did they use an interrupted time-series design)? | 0 | 0 | 4 |
| 12 | If the intervention was conducted at a group level (e.g., a whole hospital, a community, etc.) did the statistical analysis consider the use of individual-level data to determine effects at the group level? | 0 | 0 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plácido, A.I.; Roque, F.; Morgado, M. The Promising Role of Mushrooms as a Therapeutic Adjuvant of Conventional Cancer Therapies. Biologics 2022, 2, 58-68. https://doi.org/10.3390/biologics2010005
Plácido AI, Roque F, Morgado M. The Promising Role of Mushrooms as a Therapeutic Adjuvant of Conventional Cancer Therapies. Biologics. 2022; 2(1):58-68. https://doi.org/10.3390/biologics2010005
Chicago/Turabian StylePlácido, Ana Isabel, Fátima Roque, and Manuel Morgado. 2022. "The Promising Role of Mushrooms as a Therapeutic Adjuvant of Conventional Cancer Therapies" Biologics 2, no. 1: 58-68. https://doi.org/10.3390/biologics2010005