
SARS-CoV-2 and Smoker’s Paradox: Mediation by Ciliary Beat Frequency and Mucociliary Clearance?


School of Public Health Sciences, University of Waterloo, Waterloo, ON N2L 3G1, Canada
BioMed 2022, 2(1), 88-93; https://doi.org/10.3390/biomed2010009
Submission received: 29 January 2022
/
Revised: 14 February 2022
/
Accepted: 16 February 2022
/
Published: 18 February 2022
Abstract
:A COVID-19 smoker’s paradox was identified during the early days of the COVID-19 pandemic—many studies reported that smokers appeared to be protected against SARS-CoV-2 infections. Conversely, other studies added to the smoker’s paradox controversy with findings of increased risk for COVID-19 in heavy smokers. Ciliary beat frequency (CBF) within the ciliated epithelium of the nasal tract can be stimulated to a higher frequency and provide increased protection against transient exposure to airway irritants. Smokers as well as non-smokers exposed to secondhand tobacco smoke were found to have higher CBFs. However, with extended exposure to irritants, persistent upregulated CBF can damage and remodel the epithelial layer with fewer protective cilia. Additionally, mucociliary clearance (MCC), the innate defense mechanism of the respiratory system, traps particles and pathogens within the mucous layer of the epithelium and propels them out of the airways through ciliary activity. However, this mechanism becomes defective as disease progresses, increasing susceptibility to viral respiratory infections. This paper proposes that a smoker’s paradox associated with SARS-CoV-2 infection in COVID-19 patients may be mediated by upregulated ciliary beating frequency and mucociliary clearance with transient exposure to tobacco smoke, and downregulated CBF and MCC with extended exposure to tobacco smoke.
{kind=link}
{kind=link}
{kind=link}
1. Introduction
Tobacco use is associated with increased risk of infectious diseases of the respiratory tract in a dose-dependent manner [1]. Over 250 of the more than 7000 chemicals in tobacco smoke are toxic or carcinogenic, and these substances irritate the human respiratory airway passages. Tobacco smoke also alters the structure and function of immunological mechanisms that defend against infection and disease. Although short-term exposure to tobacco smoke stimulates innate immune cell function in macrophages, neutrophils, and inflammatory mediators, long-term exposure damages and inhibits production of these cells. Furthermore, the functions of adaptive immune cells such as B-cells and T-cells are also impaired by smoking, and antibody production is reduced.
Risks of viral infections of the upper respiratory tract are generally increased by smoking [1]. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes COVID-19, binds to angiotensin-converting enzyme 2 (ACE2) [2], and ACE2 expression is upregulated in the airway epithelium of smokers [3]. Yet, a COVID-19 smoker’s paradox was identified during the early days of the COVID-19 pandemic—many studies reported that smokers appeared to be protected against SARS-CoV-2 infection, and researchers suggested plausible therapeutic effects of nicotine and nitric oxide from smoking [4]. For example, pro-inflammatory cytokines involved in the cytokine-storm syndrome in severe COVID-19, such as tumor necrosis factor, interleukin 1, and interleukin 6, are inhibited by nicotine. Additionally, nitric oxide helps maintain airway dilation and filtration.
Studies in various countries have shown low rates of smokers hospitalized with COVID-19, including in China [5,6], Israel [7], United Kingdom [8], and Italy [9,10]. However, reported findings in many of these studies were criticized for having “methodological flaws” and drawing “hasty conclusions” [11]. Research design issues include selection bias from participants’ inaccuracies in self-reporting smoking, and the need to confirm tobacco smoke exposure using reliable biomarkers. Researchers should also quantify levels of tobacco smoking—e.g., light smoking (1–5 cigarettes per day) and heavy smoking (>20 cigarettes per day) [12].
Adding to the smoker’s paradox controversy, other studies reported increased risk for COVID-19 in heavy smokers [13,14,15,16]. Nevertheless, controversies persist and the issue remains unsettled. For example, a cross-sectional national study of 6857 participants in Italy, published in April 2021, continued to confirm a dose-dependent association between smoking and negative results from nasopharyngeal tests for SARS-CoV-2 [17]. The researchers arrived at their findings after “taking into account a wide number of potential confounding factors” which were overlooked in earlier studies. Clearly, controversial findings of smoking and COVID-19 indicate a need for further investigations of the underlying causative mechanisms that may explain the paradoxical findings.
The present paper presents the author’s unique perspective and insights into the COVID-19 smoking paradox. Using a grounded theory method to review the research literature [18], the author synthesized research findings into a novel theory that explains potential causative biomedical mechanisms relating a smoker’s paradox to SARS-CoV-2 infection. The author’s proposed theory may be useful for generating testable hypotheses in future biomedical research on this subject. The following sections of the paper describe relevant pathophysiological and immunological mechanisms of the nasal immune system.
2. Ciliated Epithelium
The human respiratory tract is lined throughout with a protective ciliated epithelium, interspersed with goblet cells that secrete a layer of mucus, as shown in Figure 1. Submucosal glands also secrete a protective airway surface liquid (ASL) across the epithelium [19]. Respiratory cilia are motion-producing hair-like structures that project from the apical membranes of epithelial cells in groups of 200–300 cilia per cell [20]. The cilium structure consists of nine microtubule doublets surrounding two central single microtubules [21]. Ciliary beating occurs in synchronized metachronal waves, regulated by calcium. The energy for the cilium stroke is hydrolyzed from ATP by dynein, a protein lying between the microtubule doublets which acts as a motor, putting force on the microtubules and causing the cilium to bend [22].
Zhou et al. found that ciliary beat frequency (CBF) within the ciliated epithelium of the nasal tract is approximately 7–8 Hz at room temperature—importantly, the CBF can be stimulated to a higher frequency and provide increased protection against transient exposure to irritants [23]. For example, compared to nonsmokers, smokers as well as non-smokers exposed to secondhand tobacco smoke were found to have higher CBFs. The CBF in heavy smokers averaged over 8.5 Hz. However, with extended exposure to irritants, persistent upregulated CBF can predispose one to “the emergence of adverse health effects and chronic respiratory disease”, including neoplasms.
Relatedly, temporary ciliostasis of airway epithelial cells, in which cilia become motionless, was induced in vitro when treated with 2% sodium chloride [24]. Ciliostasis allowed a two- to three-fold increase in infection of the treated cells with influenza A virus, compared to cells with functioning cilia—thereby demonstrating the importance of cilia activity in inhibiting viral infection. Moreover, the paralyzing effect of sodium chloride on the ciliated epithelium of the respiratory tract could be a causative factor in the nutritional immunology of COVID-19 and SARS-CoV-2 infection [25].
In addition to impaired function from exposure to irritants, ciliated cells are vulnerable to injury and death from exposure to inflammatory mechanisms and infectious agents and their products, which can remodel the epithelial layer with fewer protective cilia and greater mucous secretion [23]. For example, smoking can cause airway epithelial barrier dysfunction [26], and smokers were found to have greater nasal epithelium thickness and hyperplasia of mucous-secreting goblet cells [27]. The present paper proposes that the distinction between innate protective responses and chronic pathophysiological changes within the ciliated epithelium may mediate paradoxical findings of SARS-CoV-2 infection associated with transient and extended exposures to tobacco smoke.
3. Mucociliary Clearance and SARS-CoV-2 Infection
Mucociliary clearance (MCC) is the innate defense mechanism of the respiratory system [28]. Particles and pathogens trapped within the mucous layer of the epithelium are propelled out of the airways by beating cilia. However, this mechanism becomes defective as disease progresses, with increasing susceptibility to respiratory infections involving viruses such as coronavirus, influenza, and rhinovirus [20]. For example, MCC was delayed in patients infected with SARS-CoV-2 compared to healthy people [29]. The researchers found that clearance time measured using a saccharine test was approximately 15.5 min in infected people, compared to 9.5 min in healthy people. Other studies have found that levels of ACE2 that binds with SARS-CoV-2 were more highly expressed in the nasal epithelial cells, compared to reduced levels of ACE2 expressed in the more distal bronchial epithelial cells of the lower respiratory tract [30].
The connection between MCC and SARS-CoV-2 infection implies that smokers with upregulated CBFs, based on the findings of Zhou et al. [23], are more likely to have increased MCC. This, in turn, would explain smokers’ increased odds of negative results from nasopharyngeal tests. An exception would occur in those smokers with more severe and chronic underlying respiratory diseases where the ciliated epithelium is dysfunctional and no longer protective against the accumulation of pathogens in the nasopharyngeal tract. This would explain increased risk of COVID-19 in heavy smokers.
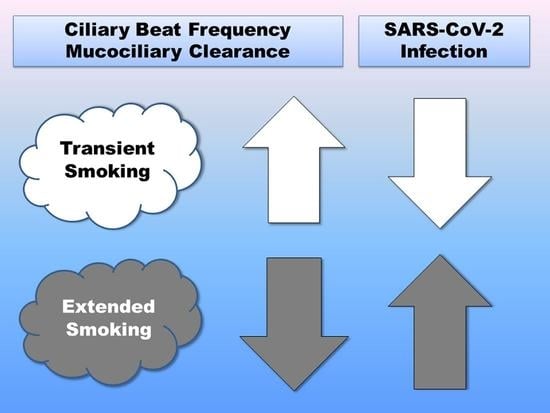
Figure 2 shows how ciliary beat frequency and mucociliary clearance is proposed to mediate the association of tobacco smoke exposure with SARS-CoV-2 nasopharyngeal infection. Depending on whether tobacco smoke exposure is transient or extended, the association between smoking and SARS-CoV-2 nasopharyngeal infection is proposed to either decrease or increase infection, consistent with the smoker’s paradox in COVID-19. Specifically, transient exposure to tobacco smoke upregulates CBF and MCC responses, and reduces SARS-CoV-2 nasopharyngeal infection. By contrast, extended exposure to tobacco smoke damages the ciliated epithelium and downregulates CBF and MCC responses, which increases SARS-CoV-2 nasopharyngeal infection.
Importantly, nasopharyngeal infections may not always correlate with COVID-19 symptoms, as seen, for example, in asymptomatic SARS-CoV-2 infections [31], and also in post-acute COVID-19 syndrome, in which disease symptoms persist after the nasopharyngeal viral infection has subsided [32]. Therefore, although the smoker’s paradox may appear to provide protection based on negative test results of SARS-CoV-2 infection, systemic adverse effects of smoking likely continue to detract from the smokers’ overall health status, even with transient or secondhand exposure to tobacco smoke [33]. This could increase the smoker’s susceptibility to symptoms and health risks associated with COVID-19, including comorbidities such as heart disease and stroke [34]. It should be repeatedly emphasized that smoking increases risks for COVID-19 and other diseases, regardless of a negative SARS-CoV-2 test.
4. Conclusions
This paper used a grounded theory method to synthesize evidence supporting a biomedical theory that explains controversial findings of a smoker’s paradox in COVID-19. Transient exposure to tobacco smoke associated with reduced SARS-CoV-2 infection in COVID-19 patients may be mediated by upregulated ciliary beating frequency and greater mucociliary clearance, which increases innate immune protection. On the other hand, downregulated CBF and MCC due to damage to the ciliated epithelium from extended exposure to tobacco smoke reduces innate immune protection and increases SARS-CoV-2 infection. More studies are needed to investigate smokers’ susceptibility to COVID-19 and SARS-CoV-2 infection.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
References
- Jiang, C.; Chen, Q.; Xie, M. Smoking increases the risk of infectious diseases: A narrative review. Tob. Induc. Dis. 2020, 18, 60. [Google Scholar] [CrossRef]
- Xu, X.; Chen, P.; Wang, J.; Feng, J.; Zhou, H.; Li, X.; Zhong, W.; Hao, P. Evolution of the novel coronavirus from the ongoing Wuhan outbreak and modeling of its spike protein for risk of human transmission. Sci. China Life Sci. 2020, 63, 457–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Rostami, M.R.; Leopold, P.L.; Mezey, J.G.; O’Beirne, S.L.; Strulovici-Barel, Y.; Crystal, R.G. Expression of the SARS-CoV-2 ACE2 Receptor in the Human Airway Epithelium. Am. J. Respir. Crit. Care Med. 2020, 202, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Usman, M.S.; Siddiqi, T.J.; Khan, M.S.; Patel, U.K.; Shahid, I.; Ahmed, J.; Kalra, A.; Michos, E.D. Is there a smoker’s paradox in COVID-19? BMJ Evid.-Based Med. 2021, 26, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Vardavas, C.I.; Nikitara, K. COVID-19 and smoking: A systematic review of the evidence. Tob. Induc. Dis. 2020, 18, 20. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Henry, B.M. Active smoking is not associated with severity of coronavirus disease 2019 (COVID-19). Eur. J. Intern. Med. 2020, 75, 107–108. [Google Scholar] [CrossRef]
- Yanover, C.; Mizrahi, B.; Kalkstein, N.; Marcus, K.; Akiva, P.; Barer, Y.; Shalev, V.; Chodick, G. What Factors Increase the Risk of Complications in SARS-CoV-2-Infected Patients? A Cohort Study in a Nationwide Israeli Health Organization. JMIR Public Health Surveill. 2020, 6, e20872. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Young, D.; Coupland, C.; Channon, K.M.; Tan, P.S.; Harrison, D.A.; Rowan, K.; Aveyard, P.; Pavord, I.D.; Watkinson, P.J. Risk of severe COVID-19 disease with ACE inhibitors and angiotensin receptor blockers: Cohort study including 8.3 million people. Heart 2020, 106, 1503–1511. [Google Scholar] [CrossRef]
- Meini, S.; Fortini, A.; Andreini, R.; Sechi, L.A.; Tascini, C. The Paradox of the Low Prevalence of Current Smokers Among COVID-19 Patients Hospitalized in Nonintensive Care Wards: Results From an Italian Multicenter Case–Control Study. Nicotine Tob. Res. 2020, 23, 1436–1440. [Google Scholar] [CrossRef]
- Rossato, M.; Russo, L.; Mazzocut, S.; Di Vincenzo, A.; Fioretto, P.; Vettor, R. Current smoking is not associated with COVID-19. Eur. Respir. J. 2020, 55, 2001290. [Google Scholar] [CrossRef]
- Van Westen-Lagerweij, N.A.; Meijer, E.; Meeuwsen, E.G.; Chavannes, N.H.; Willemsen, M.C.; Croes, E.A. Are smokers protected against SARS-CoV-2 infection (COVID-19)? The origins of the myth. NPJ Prim. Care Respir. Med. 2021, 31, 10. [Google Scholar] [CrossRef] [PubMed]
- Le Bras, A. Light smoking and CVD risk. Nat. Rev. Cardiol. 2018, 15, 136. [Google Scholar] [CrossRef] [PubMed]
- Clift, A.K.; von Ende, A.; Tan, P.S.; Sallis, H.M.; Lindson, N.; Coupland, C.A.C.; Munafò, M.R.; Aveyard, P.; Hippisley-Cox, J.; Hopewell, J.C. Smoking and COVID-19 outcomes: An observational and Mendelian randomisation study using the UK Biobank cohort. Thorax 2022, 77, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Ruiz, C.A.; López-Padilla, D.; Alonso-Arroyo, A.; Aleixandre-Benavent, R.; Solano-Reina, S.; de Granda-Orive, J.I. COVID-19 and Smoking: A Systematic Review and Meta-Analysis of the Evidence. Arch. Bronconeumol. 2021, 57, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Hopkinson, N.S.; Rossi, N.; El-Sayed_Moustafa, J.; Laverty, A.A.; Quint, J.K.; Freidin, M.; Visconti, A.; Murray, B.; Modat, M.; Ourselin, S.; et al. Current smoking and COVID-19 risk: Results from a population symptom app in over 2.4 million people. Thorax 2021, 76, 714–722. [Google Scholar] [CrossRef] [PubMed]
- Ponsford, M.J.; Gkatzionis, A.; Walker, V.M.; Grant, A.J.; Wootton, R.E.; Moore, L.S.P.; Fatumo, S.; Mason, A.M.; Zuber, V.; Willer, C.; et al. Cardiometabolic Traits, Sepsis, and Severe COVID-19: A Mendelian Randomization Investigation. Circulation 2020, 142, 1791–1793. [Google Scholar] [CrossRef] [PubMed]
- Prinelli, F.; Bianchi, F.; Drago, G.; Ruggieri, S.; Sojic, A.; Jesuthasan, N.; Molinaro, S.; Bastiani, L.; Maggi, S.; Noale, M.; et al. Association Between Smoking and SARS-CoV-2 Infection: Cross-sectional Study of the EPICOVID19 Internet-Based Survey. JMIR Public Health Surveill. 2021, 7, e27091. [Google Scholar] [CrossRef]
- Wolfswinkel, J.F.; Furtmueller, E.; Wilderom, C.P.M. Using grounded theory as a method for rigorously reviewing literature. Eur. J. Inf. Syst. 2013, 22, 45–55. [Google Scholar] [CrossRef]
- Widdicombe, J.H.; Wine, J.J. Airway Gland Structure and Function. Physiol. Rev. 2015, 95, 1241–1319. [Google Scholar] [CrossRef] [Green Version]
- Kuek, L.E.; Lee, R.J. First contact: The role of respiratory cilia in host-pathogen interactions in the airways. Am. J. Physiol. Lung Cell. Mol. Physiol. 2020, 319, L603–L619. [Google Scholar] [CrossRef]
- Cicuta, P. The use of biophysical approaches to understand ciliary beating. Biochem. Soc. Trans. 2020, 48, 221–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueno, H.; Yasunaga, T.; Shingyoji, C.; Hirose, K. Dynein pulls microtubules without rotating its stalk. Proc. Natl. Acad. Sci. USA 2008, 105, 19702–19707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, H.; Wang, X.; Brighton, L.; Hazucha, M.; Jaspers, I.; Carson, J.L. Increased nasal epithelial ciliary beat frequency associated with lifestyle tobacco smoke exposure. Inhal. Toxicol. 2009, 21, 875–881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, Y.; Tong, J.; Meng, F.; Hoeltig, D.; Liu, G.; Yin, X.; Herrler, G. Ciliostasis of airway epithelial cells facilitates influenza A virus infection. Vet. Res. 2018, 49, 65. [Google Scholar] [CrossRef] [Green Version]
- Brown, R.B. Sodium Toxicity in the Nutritional Epidemiology and Nutritional Immunology of COVID-19. Medicina 2021, 57, 739. [Google Scholar] [CrossRef] [PubMed]
- Aghapour, M.; Raee, P.; Moghaddam, S.J.; Hiemstra, P.S.; Heijink, I.H. Airway Epithelial Barrier Dysfunction in Chronic Obstructive Pulmonary Disease: Role of Cigarette Smoke Exposure. Am. J. Respir. Cell. Mol. Biol. 2018, 58, 157–169. [Google Scholar] [CrossRef]
- Hadar, T.; Yaniv, E.; Shvili, Y.; Koren, R.; Shvero, J. Histopathological changes of the nasal mucosa induced by smoking. Inhal. Toxicol. 2009, 21, 1119–1122. [Google Scholar] [CrossRef] [PubMed]
- Bustamante-Marin, X.M.; Ostrowski, L.E. Cilia and Mucociliary Clearance. Cold Spring Harb. Perspect. Biol. 2017, 9, a028241. [Google Scholar] [CrossRef]
- Koparal, M.; Kurt, E.; Altuntas, E.E.; Dogan, F. Assessment of mucociliary clearance as an indicator of nasal function in patients with COVID-19: A cross-sectional study. Eur. Arch. Otorhinolaryngol. 2021, 278, 1863–1868. [Google Scholar] [CrossRef]
- Hou, Y.J.; Okuda, K.; Edwards, C.E.; Martinez, D.R.; Asakura, T.; Dinnon, K.H., 3rd; Kato, T.; Lee, R.E.; Yount, B.L.; Mascenik, T.M.; et al. SARS-CoV-2 Reverse Genetics Reveals a Variable Infection Gradient in the Respiratory Tract. Cell 2020, 182, 429–446.e14. [Google Scholar] [CrossRef]
- Oran, D.P.; Topol, E.J. Prevalence of asymptomatic SARS-CoV-2 infection: A narrative review. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- CDC. Health Effects of Secondhand Smoke. Centers for Disease Control and Prevention—Smoking & Tobacco Use. Available online: https://www.cdc.gov/tobacco/data_statistics/fact_sheets/secondhand_smoke/health_effects/index.htm (accessed on 29 January 2022).
- Nishiga, M.; Wang, D.W.; Han, Y.; Lewis, D.B.; Wu, J.C. COVID-19 and cardiovascular disease: From basic mechanisms to clinical perspectives. Nat. Rev. Cardiol. 2020, 17, 543–558. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Ciliated epithelium of the respiratory tract.

Figure 2.
Ciliary beat frequency and mucociliary clearance may mediate the association of tobacco smoke exposure with SARS-CoV-2 nasopharyngeal infection. Transient exposure to tobacco smoke upregulates CBF and MCC responses, and reduces SARS-CoV-2 nasopharyngeal infection. Extended exposure to tobacco smoke downregulates CBF and MCC responses, and increases SARS-CoV-2 nasopharyngeal infection.
Figure 2.
Ciliary beat frequency and mucociliary clearance may mediate the association of tobacco smoke exposure with SARS-CoV-2 nasopharyngeal infection. Transient exposure to tobacco smoke upregulates CBF and MCC responses, and reduces SARS-CoV-2 nasopharyngeal infection. Extended exposure to tobacco smoke downregulates CBF and MCC responses, and increases SARS-CoV-2 nasopharyngeal infection.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Brown, R.B. SARS-CoV-2 and Smoker’s Paradox: Mediation by Ciliary Beat Frequency and Mucociliary Clearance? BioMed 2022, 2, 88-93. https://doi.org/10.3390/biomed2010009
AMA Style
Brown RB. SARS-CoV-2 and Smoker’s Paradox: Mediation by Ciliary Beat Frequency and Mucociliary Clearance? BioMed. 2022; 2(1):88-93. https://doi.org/10.3390/biomed2010009
Chicago/Turabian StyleBrown, Ronald B. 2022. "SARS-CoV-2 and Smoker’s Paradox: Mediation by Ciliary Beat Frequency and Mucociliary Clearance?" BioMed 2, no. 1: 88-93. https://doi.org/10.3390/biomed2010009