
Kidney Issues Associated with COVID-19 Disease
 , ,
, ,
Definition
:1. Introduction
2. Acute Kidney Injury (AKI) Associated with COVID-19
3. Clinical Presentation of COVID-19-Associated AKI
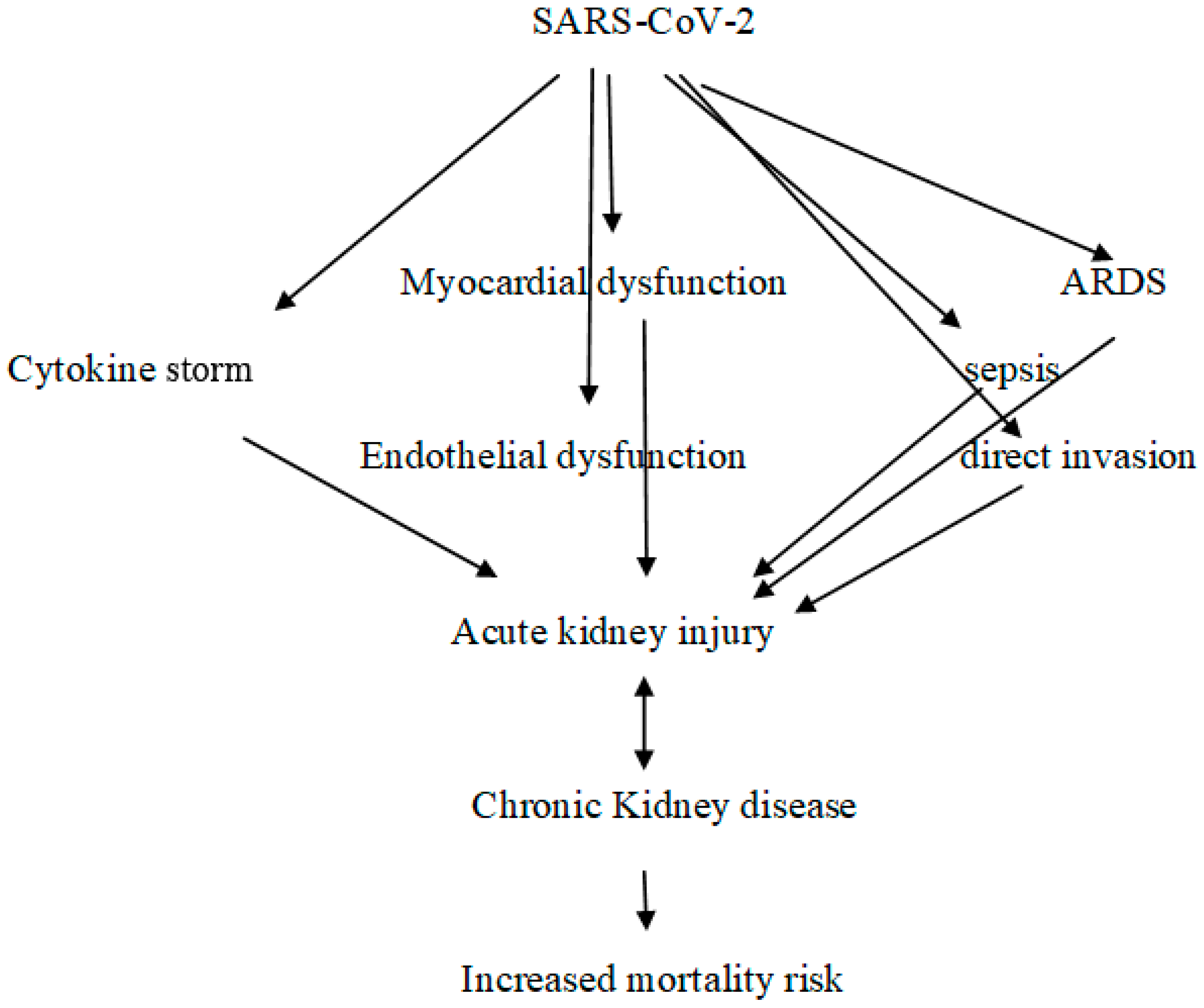
4. Pathophysiology of AKI in COVID-19 Patients
5. COVAN
6. Coagulation Disorders and Endothelial Dysfunction
7. Involvement of the Immune System
8. Other Factors Contributing to the Development of AKI
9. AKI and Progression to CKD
10. COVID-19 and Cardiorenal Syndrome
11. COVID-19 in Dialysis Patients
12. COVID-19 and Kidney Transplantation
13. Therapeutic Strategies for COVID-19 in CKD Patients
14. Vaccines
15. Post-COVID-19 Syndrome
16. Conclusions
- The relationship between COVID-19 and CKD is bidirectional.
- COVID-19 causes AKI and may exacerbate persistent CKD, and CKD is a risk factor for COVID-19.
- In this context, there are several common risk factors, including advanced age, diabetes, hypertension, and cardiovascular disease.
- Therefore, it is not surprising that the coexistence of COVID-19 and CKD is associated with higher morbidity and mortality.
- Further large-scale prospective cohort studies are needed to elucidate this association.
Author Contributions
Funding
Conflicts of Interest
References
- Jackson, C.B.; Farzan, M.; Chen, B.; Hyeryun, C. Mechanisms of SARS-CoV-2 entry into cells. Nat. Rev. Mol. Cell Biol. 2022, 23, 3–20. [Google Scholar] [CrossRef]
- Zandi, M.; Shafaati, M.; Kalantar-Neyestanaki, D.; Pourghadamyari, H.; Fani, M.; Soltani, S.; Kaleji, H.; Abbasi, S. The role of SARS-CoV-2 accessory proteins in immune evasion. Biomed Pharmacother 2022, 156, 113889. [Google Scholar] [CrossRef]
- Zandi, M. ORF9c and ORF10 as accessory proteins of SARS-CoV-2 in immune evasion. Nat. Rev. Immunol. 2022, 22, 331. [Google Scholar] [CrossRef]
- Dettlaff-Pokora, A.; Swierczynski, J. Dysregulation of the Renin-Angiotensin- Aldosterone System (RAA) in Patients Infected with SARS-CoV-2-Possible Clinical Consequences. Int. J. Mol. Sci. 2021, 22, 4503. [Google Scholar] [CrossRef]
- Hu, B.; Huang, S.; Yin, L. The cytokinestorm and COVID-19. J. Med. Virol. 2021, 93, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Kaklamanos, A.; Belogiannis, K.; Skendros, P.; Gorgoulis, V.G.; Vlachoyiannopoulos, P.G.; Tzioufas, A.G. COVID-19 Immuno-biology: Lessons Learned, New Questions Arise. Front. Immunol. 2021, 12, 719023. [Google Scholar] [CrossRef] [PubMed]
- Hassler, L.; Batlle, D. Potential SARS-CoV-2 kidney infection and paths to injury. Nat. Rev. Nephrol. 2022, 18, 275–276. [Google Scholar] [CrossRef] [PubMed]
- Pei, G.; Zhang, Z.; Peng, J.; Liu, L.; Zhang, C.; Yu, C.; Ma, Z.; Huang, Y.; Liu, W.; Yao, Y.; et al. Renal Involvement and Early Prognosis in Patients with COVID-19 Pneumonia. J. Am. Soc. Nephrol. 2020, 31, 1157–1165. [Google Scholar] [CrossRef]
- Kudose, S.; Batal, I.; Santoriello, D.; Xu, K.; Barasch, J.; Peleg, Y.; Canetta, P.; Ratner, L.E.; Marasa, M.; Gharavi, A.G.; et al. Kidney Biopsy Findings in Patients with COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1959–1968. [Google Scholar] [CrossRef]
- Velez, J.C.Q.; Caza, T.; Larsen, C.P. COVAN is the new HIVAN: The re-emergence of collapsing glomerulopathy with COVID-19. Nat. Rev. Nephrol. 2020, 16, 565–567. [Google Scholar] [CrossRef]
- Wu, H.; Larsen, C.P.; Hernandez-Arroyo, C.F.; Mohamed, M.M.B.; Caza, T.; Sharshir, M.; Chughtai, A.; Xie, L.; Gimenez, J.M.; Sandow, T.A.; et al. AKI and Col-lapsing Glomerulopathy Associated with COVID-19 and APOL1 High-Risk Genotype. J. Am. Soc. Nephrol. 2020, 3, 1688–1695. [Google Scholar] [CrossRef]
- Ng, J.H.; Hirsch, J.S.; Hazzan, A.; Wanchoo, R.; Shah, H.H.; Malieckal, D.A.; Ross, D.W.; Sharma, P.; Sakhiya, V.; Fishbane, S.; et al. Northwell Nephrology COVID-19 Research Consortium. Outcomes Among Patients Hospitalized With COVID-19 and Acute KidneyInjury. Am. J. Kidney Dis. 2021, 77, 204–215. [Google Scholar] [CrossRef]
- Chung, E.Y.; Palmer, S.C.; Natale, P.; Krishnan, A.; Cooper, T.E.; Saglimbene, V.M.; Ruospo, M.; Au, E.; Jayanti, S.; Liang, A.; et al. Incidence and Outcomes of COVID-19 in People with CKD: A Systematic Review and Meta-analysis. Am. J. Kidney Dis. 2021, 78, 804–815. [Google Scholar] [CrossRef]
- Ozturk, S.; Turgutalp, K.; Arici, M.; Odabas, A.R.; Altiparmak, M.R.; Aydin, Z.; Cebeci, E.; Basturk, T.; Soypacaci, Z.; Sahin, G.; et al. Mortality analysis of COVID-19 infection in chronic kidney disease, haemodialysis and renal transplant patients compared with patients without kidney disease: A nationwide analysis from Turkey. Nephrol. Dial. Transplant. 2020, 35, 2083–2095. [Google Scholar] [CrossRef] [PubMed]
- Jager, K.J.; Kramer, A.; Chesnaye, N.C.; Couchoud, C.; Sánchez-Álvarez, J.E.; Garneata, L.; Collart, F.; Hemmelder, M.H.; Ambühl, P.; Kerschbaum, J.; et al. Results from the ERA-EDTA Registry indicate a high mortality due to COVID-19 in dialysis patients and kidney transplant recipients across Europe. Kidney Int. 2020, 98, 1540–1548. [Google Scholar] [CrossRef] [PubMed]
- Valeri, A.M.; Robbins-Juarez, S.Y.; Stevens, J.S.; Ahn, W.; Rao, M.K.; Radhakrishnan, J.; Gharavi, A.G.; Mohan, S.; Husain, S.A. Presentation and Outcomes of Patients with ESKD and COVID-19. J. Am. Soc. Nephrol. 2020, 31, 1409–1415. [Google Scholar] [CrossRef]
- El Karoui, K.; De Vriese, A.S. COVID-19 in dialysis: Clinical impact, immune response, prevention, and treatment. Kidney Int. 2022, 101, 883–894. [Google Scholar] [CrossRef] [PubMed]
- Jawdeh, B.G. COVID-19 in Kidney Transplantation: Outcomes, Immunosuppression Management, and Operational Challenges. Adv. Chronic Kidney Dis. 2020, 27, 383–389. [Google Scholar] [CrossRef]
- Tylicki, L.; Biedunkiewicz, B.; Puchalska-Reglińska, E.; Gellert, R.; Burnier, M.; Wolf, J.; Dȩbska-Ślizień, A. COVID-19 vac-cination reduces mortality in patients on maintenance hemodialysis. Front. Med. (Lausanne) 2022, 9, 937167. [Google Scholar] [CrossRef]
- Klomjit, N.; Alexander, M.P.; Fervenza, F.C.; Zoghby, Z.; Garg, A.; Hogan, M.C.; Nasr, S.H.; Abu Minshar, M.; Zand, L. COVID-19 Vaccination and Glomerulonephritis. Kidney Int. Rep. 2021, 6, 2969–2978. [Google Scholar] [CrossRef]
- Kale, A.; Shelke, V.; Dagar, N.; Anders, H.J.; Gaikwad, A.B. How to use COVID-19 antiviral drugs in patients with chronic kidney disease. Front. Pharmacol. 2023, 14, 1053814. [Google Scholar] [CrossRef]
- Copur, S.; Berkkan, M.; Basile, C.; Tuttle, K.; Kanbay, M. Post-acute COVID-19 syndrome and kidney diseases: What do we know? J. Nephrol. 2022, 35, 795–805. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Zhong, N.S. Clinical Characteristics of COVID-19 in China. Reply. N. Engl. J. Med. 2020, 382, 1861–1862. [Google Scholar] [PubMed]
- Batlle, D.; Soler, M.; Sparks, M.A.; Hiremath, S.; South, A.M.; Welling, P.A.; Swaminathan, S. COVID-19 and ACE2 in Cardi-ovascular, Lung, and Kidney Working Group. Acute Kidney Injury in COVID-19: Emerging Evidence of a Distinct Patho-physiology. J. Am. Soc. Nephrol. 2020, 31, 1380–1383. [Google Scholar] [CrossRef]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, J.S.; Ng, J.H.; Ross, D.W.; Sharma, P.; Shah, H.H.; Barnett, R.L.; Hazzan, A.D.; Fishbane, S.; Jhaveri, K.D. Northwell COVID-19 Research Consortium; Northwell Nephrology COVID-19 Research Consortium. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020, 98, 209–218. [Google Scholar] [CrossRef]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Claassen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: A prospective cohort study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Gupta, S.; Coca, S.G.; Chan, L.; Melamed, M.L.; Brenner, S.K.; Hayek, S.S.; Sutherland, A.; Puri, S.; Srivastava, A.; Leonberg-Yoo, A.; et al. AKI Treated with Renal Replacement Therapy in Critically Ill Patients with COVID-19. J. Am. Soc. Nephrol. 2020, 32, 161–176. [Google Scholar] [CrossRef]
- Peng, S.; Wang, H.Y.; Sun, X.; Li, P.; Ye, Z.; Li, Q.; Wang, J.; Shi, X.; Liu, L.; Yao, Y.; et al. Early versus late acute kidney injury among patients with COVID-19-a multicenter study from Wuhan, China. Nephrol. Dial. Transplant. 2020, 35, 2095–2102. [Google Scholar] [CrossRef]
- Fu, E.L.; Janse, R.J.; de Jong, Y.; van der Endt, V.H.; Milders, J.; van der Willik, E.M.; de Rooij, E.N.; Dekkers, O.M.; Rotmans, J.I.; van Diepen, M. Acute kidney injury and kidney replacement therapy in COVID-19: A systematic review and metaanalysis. Clin. Kidney J. 2020, 13, 550–563. [Google Scholar] [CrossRef]
- Chan, L.; Chaudhary, K.; Saha, A.; Chauhan, K.; Vaid, A.; Zhao, S.; Paranjpe, I.; Somani, S.; Richter, F.; Miotto, R.; et al. AKI in Hospitalized Patients with COVID-19. J. Am. Soc. Nephrol. 2021, 32, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Shemies, R.S.; Nagy, E.; Younis, D.; Sheashaa, H. Renal replacement therapy for critically ill patients with COVID-19-associated acute kidney injury: A review of current knowledge. Ther. Apher. Dial. 2021, 26, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Pecly, I.M.D.; Azevedo, R.B.; Muxfeldt, E.S.; Botelho, B.G.; Albuquerque, G.G.; Diniz, P.H.P.; Silva, R.; Rodrigues, C.I.S. COVID-19 and chronic kidney disease: A comprehensive review. Braz. J. Nephrol. 2021, 43, 383–399. [Google Scholar]
- Bowe, B.; Cai, M.; Xie, Y.; Gibson, A.K.; Maddukuri, G.; Al-Aly, Z. Acute Kidney Injury in a National Cohort of Hospitalized US Veterans th COVID-19. Clin. J. Am. Soc. Nephrol. 2020, 16, 14–25. [Google Scholar] [CrossRef]
- Charytan, D.M.; Parnia, S.; Khatri, M.; Petrilli, C.M.; Jones, S.; Benstein, J.; Horwitz, L.I. Decreasing Incidence of Acute Kid-ney Injury in Patients with COVID-19 Critical Illness in New York City. Kidney Int. Rep. 2021, 6, 916–927. [Google Scholar] [CrossRef]
- Chaudhri, I.; Moffitt, R.; Taub, E.; Annadi, R.R.; Hoai, M.; Bolotova, O.; Yoo, J.; Dhaliwal, S.; Sahib, H.; Daccueil, F.; et al. Association of Proteinuria and Hematuria with Acute Kidney Injury and Mortality in Hospitalized Patients with COVID-19. Kidney Blood Press. 2020, 45, 1018–1032. [Google Scholar] [CrossRef]
- Hidayat, A.A.; Gunawan, V.A.; Iragama, F.R.; Alfiansyah, R.; Hertanto, D.M.; Tjempakasari, A.; Thaha, M. Risk Factors and Clinical Characteristics of Acute Kidney Injury in Patients with COVID-19: A Systematic Review and Meta-Analysis. Pathophysiology 2023, 30, 233–247. [Google Scholar] [CrossRef]
- Kormann, R.; Jacquot, A.; Alla, A.; Corbel, A.; Koszutski, M.; Voirin, P.; Parrilla, M.G.; Bevilacqua, S.; Schvoerer, E.; Gueant, J.-L.; et al. Coronavirus disease 2019: Acute Fanconi syndrome precedes acute kidney injury. Clin. Kidney J. 2020, 13, 362–370. [Google Scholar] [CrossRef]
- Werion, A.; Belkhir, L.; Perrot, M.; Schmit, G.; Aydin, S.; Chen, Z. Cliniquesuniversitaires Saint-Luc (CUSL) COVID-19 Research Group. SARS-CoV-2 causes a specific dysfunction of the kid-ney proximal tubule. Kidney Int. 2020, 98, 1296–1307. [Google Scholar] [CrossRef]
- Ferlicot, S.; Jamme, M.; Gaillard, F.; Oniszczuk, J.; Couturier, A.; May, O.; Grünenwald, A.; Sannier, A.; Moktefi, A.; Le Mon-nier, O.; et al. AP-HP/Universities/Inserm COVID-19 research collaboration. The spectrum of kidney bi-opsies in hospitalized patients with COVID-19, acute kidney injury, and/or proteinuria. Nephrol. Dial. Transplant. 2021, 12, gfab042. [Google Scholar]
- Legrand, M.; Bell, S.; Forni, L.; Joannidis, M.; Koyner, J.L.; Liu, K.; Cantaluppi, V. Pathophysiology of COVID-19-associated acute kidney injury. Nat. Rev. Nephrol. 2021, 17, 751–764. [Google Scholar] [CrossRef]
- Santoriello, D.; Khairallah, P.; Bomback, A.S.; Xu, K.; Kudose, S.; Bata, I.; Barasch, J.; Radhakrishnan, J.; D’Agati, V.; Markowitz. Postmortem Kidney Pathology Findings in Patients with COVID-19G. J. Am. Soc. Nephrol. 2020, 31, 2158–2167. [Google Scholar] [CrossRef]
- Miller, S.E.; Brealey, J.K. Visualization of putative coronavirus in kidney. Kidney Int. 2020, 98, 231–232. [Google Scholar] [CrossRef]
- Hanley, B.; Naresh, K.N.; Roufosse, C.; Nicholson, A.G.; Weir, J.; Cooke, G.S.; Thursz, M.; Manousou, P.; Corbett, R.; Goldin, R.; et al. Histopathological findings and viral tropism in UK patients with severe fatal COVID-19: A post-mortem study. Lancet Microbe 2020, 1, e245–e253. [Google Scholar] [CrossRef] [PubMed]
- Akilesh, S.; Nast, C.C.; Yamashita, M.; Henriksen, K.; Charu, V.; Troxell, M.L.; Kambham, N.; Bracamonte, E.; Houghton, D.; Ahmed, N.I.; et al. Multicenter Clinicopathologic Correlation of Kidney Biopsies Performed in COVID-19 Patients Presenting With Acute Kidney Injury or Proteinuria. Am. J. Kidney Dis. 2021, 77, 82–93.e1. [Google Scholar] [CrossRef]
- Braun, F.; Lütgehetmann, M.; Pfefferle, S.; Wong, M.N.; Carsten, A.; Lindenmeyer, M.T.; Nörz, D.; Heinrich, F.; Meißner, K.; Wichmann, D.; et al. SARS-CoV-2 renal tropism associates with acute kidney injury. Lancet 2020, 396, 597–598. [Google Scholar] [CrossRef]
- Sun, J.; Zhu, A.; Li, H.; Zheng, K.; Zhuang, Z.; Chen, Z.; Shi, Y.; Zhang, Z.; Chen, S.B.; Liu, X.; et al. Isolation of infectious SARS-CoV-2 from urine of a COVID-19 patient. Emerg. Microbes Infect. 2020, 9, 991–993. [Google Scholar] [CrossRef]
- Puelles, V.G.; Lütgehetmann, M.; Lindenmeyer, M.T.; Sperhake, J.P.; Wong, M.N.; Allweiss, L.; Chilla, S.; Heinemann, A.; Wanner, N.; Liu, S.; et al. Multiorgan and Renal Tropism of SARS-CoV-2. N. Engl. J. Med. 2020, 6, 590–592. [Google Scholar] [CrossRef]
- Schwimmer, J.A.; Markowitz, G.S.; Valeri, A.; Appel, G.B. Collapsing glomerulopathy. Semin. Nephrol. 2003, 23, 209–218. [Google Scholar] [CrossRef]
- Giannini, G.; Velez, J.C.; May, R.M.; Sharma, S.G.; Mohamed, M.M.; Cassol, C.A.; Larsen, C.P.; Caza, T.N. Renal Prognosis of COVID-19 Associated Nephropathy. Kidney Int. Rep. 2022, 7, 2722–2725. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogene-sis in COVID-19. N. Engl. J. Med. 2020, 9, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Vassiliou, A.G.; Keskinidou, C.; Jahaj, E.; Gallos, P.; Dimopoulou, I.; Kotanidou, A.; Orfanos, S.E. ICU Admission Levels of Endothelial Biomarkers as Predictors of Mortality in Critically Ill COVID-19 Patients. Cells 2021, 10, 186. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Connors, J.M.; Levy, J.H. The coagulopathy, endotheliopathy, and vasculitis of COVID-19. Inflamm. Res. 2020, 69, 1181–1189. [Google Scholar] [CrossRef] [PubMed]
- Macor, P.; Durigutto, P.; Mangogna, A.; Bussani, R.; De Maso, L.; D’errico, S.; Zanon, M.; Pozzi, N.; Meroni, P.L.; Tedesco, F. Multiple-Organ Complement Deposition on Vascular Endothelium in COVID-19 Patients. Biomedicines 2021, 9, 1003. [Google Scholar] [CrossRef] [PubMed]
- Ince, C. The central role of renal microcirculatory dysfunction in the pathogenesis of acute kidney injury. Nephron Clin. Pract. 2014, 127, 124–128. [Google Scholar] [CrossRef]
- Taha, M.; Sano, D.; Hanoudi, S.; Esber Elahi, M.; Gabali, A.; Chopra, T.; Draghici, S.; Samavat, I.L. Platelets and renal failure in the SARS-CoV-2 syndrome. Platelets 2021, 32, 130–137. [Google Scholar] [CrossRef]
- Zuo, Y.; Estes, S.K.; Ali, R.A.; Gandhi, A.A.; Yalavarthi, S.; Shi, H.; Sule, G.; Gockman, K.; Madison, J.A.; Zuo, M.; et al. Prothrombotic autoan-tibodies in serum from patients hospitalized with COVID-19. Sci. Med. Transl. 2020, 12, eabd3876. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.E.; Lameira, F.S.; Rinke, E.B.; Vander Heide, R.S. Cardiac Endotheliitis and Multisystem Inflammatory Syndrome Af-ter COVID-19. Ann. Intern. Med. 2020, 173, 1025–1027. [Google Scholar] [CrossRef]
- Plášek, J.; Gumulec, J.; Máca, J.; Škarda, J.; Procházka, V.; Grézl, T.; Václavík, J. COVID-19 associated coagulopathy: Mecha-nisms and host-directed treatment. Am. J. Med. Sci. 2022, 363, 465–475. [Google Scholar] [CrossRef]
- Ville, S.; Le Bot, S.; Chapelet-Debout, A.; Blancho, G.; Fremeaux-Bacchi, V.; Deltombe, C.; Fakhouri, F. Atypical HUS relapse triggered by COVID-19. Kidney Int. 2020, 99, 267–268. [Google Scholar] [CrossRef]
- Yu, J.; Yuan, X.; Chen, H.; Chaturvedi, S.; Braunstein, E.M.; Brodsky, R.A. Direct activation of the alternative complement pathway by SARS-CoV-2 spike proteins is blocked by factor D inhibition. Blood 2020, 136, 2080–2089. [Google Scholar] [CrossRef] [PubMed]
- Perico, L.; Benigni, A.; Casiraghi, F.; Ng, L.F.P.; Renia, L.; Remuzzi, G. Immunity, endothelial injury and comple-ment-induced coagulopathy in COVID-19. Nat. Rev. Nephrol. 2021, 17, 46–64. [Google Scholar] [CrossRef] [PubMed]
- Fang, W.; Jiang, J.; Su, L.; Shu, T.; Liu, H.; Lai, S.; Ghiladi, R.A.; Wang, J. The role of NO in COVID-19 and potential therapeutic strategies. Free Radic. BiolMed. 2021, 163, 153–162. [Google Scholar] [CrossRef] [PubMed]
- El Shamy, O.; Munoz-Casablanca, N.; Coca, S.; Sharma, S.; Lookstein, R.; Uribarri, J. Bilateral Renal Artery Thrombosis in a Patient With COVID-19. Kidney Med. 2020, 3, 116–119. [Google Scholar] [CrossRef]
- Moderbacher, C.R.; Ramirez, S.I.; Dan, J.M.; Grifoni, A.; Hastie, K.M.; Weiskopf, D.; Belanger, S.; Abbott, R.K.; Kim, C.; Choi, J.; et al. Antigen-Specific Adaptive Immunity to SARS-CoV-2 in Acute COVID-19 and Associations with Age and Disease Severity. Cell 2020, 183, 996–1012.e19. [Google Scholar] [CrossRef]
- Pawelec, G. Age and immunity: What is “immunosenescence”? Exp. Gerontol. 2018, 105, 4–9. [Google Scholar] [CrossRef]
- Fuentes, E.; Fuentes, M.; Alarcón, M.; Palomo, I. Immune System Dysfunction in the Elderly. An. Da Acad. Bras. De Ciências 2017, 89, 285–299. [Google Scholar] [CrossRef] [PubMed]
- Cantaluppi, V.; Quercia, A.D.; Dellepiane, S.; Ferrario, S.; Camussi, G.; Biancone, L. Interaction between systemic inflamma-tion and renal tubular epithelial cells. Nephrol. Dial. Transplant. 2014, 29, 2004–2011. [Google Scholar] [CrossRef] [PubMed]
- Cutuli, S.L.; Artigas, A.; Fumagalli, R.; Monti, G.; Ranieri, V.M.; Ronco, C.; Antonelli, M. The EUPHAS 2 Collaborative Group Polymyxin-B hemoperfusion in septic patients: Analysis of a multicenter registry. Ann. Intensiv. Care 2016, 6, 1–9. [Google Scholar] [CrossRef]
- Zarbock, A.; Gomez, H.; Kellum, J.A. Sepsis-induced acute kidney injury revisited: Pathophysiology, prevention and future therapies. CurrOpinCritCare 2014, 20, 588–595. [Google Scholar] [CrossRef]
- Buszko, M.; Nita-Lazar, A.; Park, J.-H.; Schwartzberg, P.L.; Verthelyi, D.; Young, H.A.; Rosenberg, A.S. Lessons learned: New insights on the role of cytokines in COVID-19. Nat. Immunol. 2021, 22, 404–411. [Google Scholar] [CrossRef]
- Koning, R.; Bastard, P.; Casanova, J.-L.; Brouwer, M.C.; van de Beek, D.; van Agtmael, M.; Algera, A.G.; Appelman, B.; van Baarle, F.; Bax, D.; et al. Autoantibodies against type I interferons are associated with multi-organ failure in COVID-19 patients. Intensiv. Care Med. 2021, 47, 704–706. [Google Scholar] [CrossRef]
- Migliorini, A.; Angelotti, M.L.; Mulay, S.R.; Kulkarni, O.O.; Demleitner, J.; Dietrich, A.; Sagrinati, C.; Ballerini, L.; Peired, A.; Shankland, S.J.; et al. The antiviral cytokines IFN-α and IFN-β modulate parietal epithelial cells and promote podocyte loss: Implications for IFN toxicity, viral glomerulonephritis, and glomerular regeneration. Am. J. Pathol. 2013, 183, 431–440. [Google Scholar] [CrossRef]
- Beckerman, P.; Bi-Karchin, J.; Park, A.S.; Qiu, C.; Dummer, P.D.; Soomro, I.; Boustany-Kari, C.M.; Pullen, S.S.; Miner, J.H.; Hu, C.A. Transgenic expression of human APOL1 risk variants in podocytes induces kidney disease in mice. Nat. Med. 2017, 23, 429–438. [Google Scholar] [CrossRef]
- Pfister, F.; Vonbrunn, E.; Ries, T.; Jäck, H.-M.; Überla, K.; Lochnit, G.; Sheriff, A.; Herrmann, M.; Büttner-Herold, M.; Amann, K.; et al. Complement Activation in Kidneys of Patients With COVID-19. Front. Immunol. 2020, 11, 594849. [Google Scholar] [CrossRef]
- Vinayagam, S.; Sattu, K. SARS-CoV-2 and coagulation disorders in different organs. Life Sci. 2020, 260, 118431. [Google Scholar] [CrossRef]
- Castellano, G.; Franzin, R.; Sallustio, F.; Stasi, A.; Banelli, B.; Romani, M.; De Palma, G.; Lucarelli, G.; Divella, C.; Battaglia, M.; et al. Complement component C5a induces aberrant epigenetic modifications in renal tubular epithelial cells accelerating se-nescence by Wnt4/βcatenin signaling after ischemia/reperfusion injury. Aging 2019, 11, 4382–4406. [Google Scholar] [CrossRef]
- Laing, A.G.; Lorenc, A.; Del Molino Del Barrio, I.; Das, A.; Fish, M.; Monin, L.; Muñoz-Ruiz, M.; McKenzie, D.R.; Hayday, T.S.; Francos-Quijorna, I.; et al. A dynamic COVID-19 immune signature includes associations with poor prognosis. Nat. Med. 2020, 26, 1623–1635. [Google Scholar] [CrossRef]
- Olagnier, D.; Farahani, E.; Thyrsted, J.; Blay-Cadanet, J.; Herengt, A.; Idorn, M.; Hait, A.; Hernaez, B.; Knudsen, A.; Iversen, M.B.; et al. SARS-CoV2-mediated suppression of NRF2-signaling reveals potent antiviral and anti-inflammatory activity of 4-octyl-itaconate and dimethyl fumarate. Nat Commun. 2020, 2, 4938. [Google Scholar] [CrossRef]
- Noel, S.; Martina, M.N.; Bandapalle, S.; Racusen, L.C.; Potteti, H.R.; Hamad, A.R.; Reddy, S.P.; Rabb, H.T. Lymphocyte–Specific Activation of Nrf2 Protects from AKI. J. Am. Soc. Nephrol. 2015, 26, 2989–3000. [Google Scholar] [CrossRef]
- Liu, M.; Grigoryev, D.N.; Crow, M.T.; Haas, M.; Yamamoto, M.; Reddy, S.P.; Rabb, H. Transcription factor Nrf2 is protective during ischemic and nephrotoxic acute kidney injury in mice. Kidney Int. 2009, 76, 277–285. [Google Scholar] [CrossRef]
- Camargo, R.L.; Bombassaro, B.; Monfort-Pires, M.; Mansour, E.; Palma, A.C.; Ribeiro, L.C.; Ulaf, R.G.; Bernardes, A.F.; Nunes, T.A.; Agrela, M.V.; et al. Plasma Angiotensin II Is Increased in Critical Coronavirus Disease 2019. Front. Cardiovasc. Med. 2022, 9, 847809. [Google Scholar] [CrossRef]
- Beyerstedt, S.; Casaro, E.B.; Rangel, É.B. COVID-19: Angiotensin-converting enzyme 2 (ACE2) expression and tissue suscep-tibility to SARS-CoV-2 infection. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 905–919. [Google Scholar] [CrossRef]
- McMillan, P.; Dexhiemer, T.; Neubig, R.R.; Uhal, B.D. COVID-19—A Theory of Autoimmunity Against ACE-2 Explained. Front. Immunol. 2021, 12, 582166. [Google Scholar] [CrossRef]
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 3, 2255–2273. [Google Scholar] [CrossRef]
- Xia, P.; Wen, Y.; Duan, Y.; Su, H.; Cao, W.; Xiao, M.; Ma, J.; Zhou, Y.; Chen, G.; Jiang, W.; et al. Clinico-pathological Features and Outcomes of Acute Kidney Injury in Critically Ill COVID-19 with Prolonged Disease Course: A Retrospective Cohort. J. Am. Soc. Nephrol. 2020, 31, 2205–2221. [Google Scholar]
- Coomes, E.A.; Haghbayan, H. Interleukin-6 in COVID-19: A systematic review and meta-analysis. Rev. Med. Virol. 2020, 30, e2141. [Google Scholar] [CrossRef]
- Leisman, D.E.; Ronner, L.; Pinotti, R.; Taylor, M.D.; Sinha, P.; Calfee, C.S.; Hirayama, A.V.; Mastroiani, F.; Turtle, C.J.; Harhay, M.O. Cytokine elevation in severe and critical COVID-19: A rapid systematic review, meta-analysis, and comparison with other inflammatory syndromes. Lancet Respir. Med. 2020, 8, 1233–1244. [Google Scholar] [CrossRef]
- Kox, M.; Waalders, N.J.B.; Kooistra, E.J.; Gerretsen, J.; Pickkers, P. Cytokine Levels in Critically Ill Patients With COVID-19 and Other Conditions. JAMA 2020, 324, 1565–1567. [Google Scholar] [CrossRef]
- Legrand, M.; Mik, E.G.; Johannes, T.; Payen, D.; Ince, C. Renal Hypoxia and Dysoxia After Reperfusion of the Ischemic Kidney. Mol. Med. 2008, 14, 502–516. [Google Scholar]
- Hall, A.; Busse, L.W.; Ostermann, M. Angiotensin in Critical Care. Crit. Care 2018, 22, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Barthélémy, R.; Beaucoté, V.; Bordier, R.; Collet, M.; Le Gall, A.; Hong, A.; de Roquetaillade, C.; Gayat, E.; Mebazaa, A.; Chousterman, B.G. Haemodynamic impact of positive end-expiratory pressure in SARS-CoV-2 acute respiratory distress syndrome: Oxygenation versus oxygen delivery. Br. J. Anaesth. 2021, 126, e70–e72. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, R.; Sinclair, H.C.; Patel, K.; Low, B.; Pericao, A.; Manisty, C.; Guttmann, O.; Zemrak, F.; Miller, O.; Longhi, P.; et al. Delayed-onset myocarditis following COVID-19. Lancet Respir. Med. 2021, 9, e32–e34. [Google Scholar] [CrossRef]
- Kotecha, T.; Knight, D.S.; Razvi, Y.; Kumar, K.; Vimalesvaran, K.; Thornton, G.; Patel, R.; Chacko, L.; Brown, J.T.; Coyle, C.; et al. Faculty Opinions recommendation of Patterns of myocardial injury in recovered troponin-positive COVID-19 patients assessed by cardiovascular magnetic resonance. Eur. Heart J. 2021, 42, 1866–1878. [Google Scholar] [CrossRef] [PubMed]
- Legrand, M.; Dupuis, C.; Simon, C.; Gayat, E.; Mateo, J.; Lukaszewicz, A.C.; Payen, D. Association between systemic hemo-dynamics and septic acute kidney injury in critically ill patients: A retrospective observational study. Crit Care 2013, 29, R278. [Google Scholar] [CrossRef]
- Cruces, P.; Lillo, P.; Salas, C.; Salomon, T.; Lillo, F.; González, C.; Pacheco, A.; Hurtado, D.E. RenalDecapsulation Prevents Intrinsic Renal Compartment Syndrome in Ischemia-Reperfusion-Induced Acute Kidney Injury: A Physiologic Approach. CritCareMed 2018, 46, 216–222. [Google Scholar]
- Sang, L.; Chen, S.; Zheng, X.; Guan, W.; Zhang, Z.; Liang, W.; Zhong, M.; Jiang, L.; Pan, C.; Zhang, W.; et al. The incidence, risk factors and prognosis of acute kidney injury in severe and critically ill patients with COVID-19 in mainland China: A retrospective study. BMC Pulm. Med. 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Gillenwater, S.; Rahaghi, F.; Hadeh, A. Remdesivir for the Treatment of COVID-19—Final Report. N. Engl. J. Med. 2020, 5, 1813–1826. [Google Scholar]
- Binois, Y.; Hachad, H.; Salem, J.-E.; Charpentier, J.; Lebrun-Vignes, B.; Pène, F.; Cariou, A.; Chiche, J.-D.; Mira, J.-P.; Nguyen, L.S. Acute Kidney Injury Associated With Lopinavir/Ritonavir Combined Therapy in Patients With COVID-19. Kidney Int. Rep. 2020, 5, 1787–1790. [Google Scholar] [CrossRef]
- Geng, Y.; Ma, Q.; Du, Y.-S.; Peng, N.; Yang, T.; Zhang, S.-Y.; Wu, F.-F.; Lin, H.-L.; Su, L. Rhabdomyolysis is Associated with In-Hospital Mortality in Patients With COVID-19. Shock 2021, 56, 360–367. [Google Scholar] [CrossRef]
- Shaefi, S.; Brenner, S.K.; Gupta, S.; O’Gara, B.P.; Krajewski, M.L.; Charytan, D.M.; Chaudhry, S. Extracorporeal mem-brane oxygenation in patients with severe respiratory failure from COVID-19. Intensive Care Med. 2021, 47, 208–221. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Hajage, D.; Lebreton, G.; Monsel, A.; Voiriot, G.; Levy, D.; Baron, E. Extracorporeal membrane oxygena-tion for severe acute respiratory distress syndrome associated with COVID-19: A retrospective cohort study. Lancet Respir. Med. 2020, 8, 1121–1131. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.; Wu, G.; Zhang, J.; Yang, L. Risk Factors for Acute Kidney Injury in Adult Patients With COVID-19: A Systematic Re-view and Meta-Analysis. Front. Med. 2021, 8, 719472. [Google Scholar] [CrossRef] [PubMed]
- Chawla, L.S.; Eggers, P.W.; Star, R.A.; Kimmel, P.L. Acute kidney injury and chronic kidney disease as interconnected syn-dromes. N. Engl. J. Med. 2014, 371, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Ferenbach, D.A.; Bonventre, J.V. Mechanisms of maladaptive repair after AKI leading to accelerated kidney ageing and CKD. Nat. Rev. Nephrol. 2015, 11, 264–276. [Google Scholar]
- Coca, S.G.; Singanamala, S.; Parikh, C.R. Chronic kidney disease after acute kidney injury: A systematic review and me-ta-analysis. Kidney Int. 2012, 81, 442–448. [Google Scholar] [CrossRef]
- Karimi, Z.; Masjedi, F.; Malekmakan, L.; Doostkam, A.; Roozbeh, J.; Ghahramani, N. Potential Mechanisms of the SARS-CoV-2-induced AKI Progression to CKD: A Forward-Looking Perspective. Iran. J. Kidney Dis. 2021, 15, 243–255. [Google Scholar]
- Tanaka, S.; Tanaka, T.; Nangaku, M. Hypoxia as a key player in the AKI-to-CKD transition. Am. J. Physiol. Physiol. 2014, 307, F1187–F1195. [Google Scholar]
- Newsome, B.B.; Warnock, D.G.; McClellan, W.M.; Herzog, C.A.; Kiefe, C.I.; Eggers, P.W.; Allison, J.J. Long-term risk of mortality and end-stage renal disease among the elderly after small increases in serum creatinine level during hospitaliza-tion for acute myocardial infarction. Arch Intern. Med. 2008, 168, 609–616. [Google Scholar] [CrossRef]
- Coca, S.G.; Yusuf, B.; Shlipak, M.G.; Garg, A.X.; Parikh, C.R. Long-term Risk of Mortality and Other Adverse Outcomes After Acute Kidney Injury: A Systematic Review and Meta-analysis. Am. J. Kidney Dis. 2009, 53, 961–973. [Google Scholar] [CrossRef]
- Sifaat, M.; Patel, P.; Sheikh, R.; Ghaffar, D.; Vaishnav, H.; Nahar, L.; Rupani, S.; Quadri, S.J. Cardiorenal Disease in COVID-19 Patients. Renin Angiotensin Aldosterone Systtem 2022, 18, 4640788. [Google Scholar] [CrossRef] [PubMed]
- Aleksova, A.; Fluca, A.L.; Gagno, G.; Pierri, A.; Padoan, L.; Derin, A.; Moretti, R.; Noveska, E.A.; Azzalini, E.; D’Errico, S.; et al. Long-term effect of SARS-CoV-2 infection on cardiovascu-lar outcomes and all-cause mortality. Life Sci. 2022, 1, 121018. [Google Scholar] [CrossRef]
- Zheng, Y.-Y.; Ma, Y.-T.; Zhang, J.-Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 Novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Baral, R.; Tsampasian, V.; Debski, M.; Moran, B.; Garg, P.; Clark, A.; Vassiliou, V.S. Association between renin-angiotensin-aldosterone system inhibitors and clini-cal outcomes in patients with COVID-19: A systematic review and meta-analysis. JAMA Netw. Open 2021, 4, e213594. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Qiao, Y.; Yu, Z.; Huang, Y.; Yang, K.; He, T.; Zhao, J. T-Lymphocyte Subsets Alteration, Infection and Renal Outcome in Advanced Chronic Kidney Disease. Front Med. (Lausanne) 2021, 9, 742419. [Google Scholar] [CrossRef]
- Wang, R.; Liao, C.; He, H.; Hu, C.; Wei, Z.; Hong, Z.; Zhang, C.; Liao, M.; Shui, H. COVID-19 in Hemodialysis Patients: A Report of 5 Cases. Am. J. Kidney Dis. 2020, 76, 141–143. [Google Scholar] [CrossRef]
- Xiong, F.; Tang, H.; Liu, L.; Tu, C.; Tian, J.B.; Lei, C.T.; Liu, J.; Dong, J.W.; Chen, W.L.; Wang, X.H. Clinical characteristics of and medical interventions for COVID-19 in hemodialysis pa-tients in wuhan, China. J. Am. Soc. Nephrol. 2020, 31, 1387. [Google Scholar] [CrossRef]
- Clarke, C.; Prendecki, M.; Dhutia, A.; Ali, M.A.; Sajjad, H.; Shivakumar, O.; Lightstone, L.; Kelleher, P.; Pickering, M.C.; Thomas, D.; et al. High Prevalence of Asymptomatic COVID-19 Infection in Hemodialysis Patients Detected Using Serologic Screening. J. Am. Soc. Nephrol. 2020, 31, 1969–1975. [Google Scholar] [CrossRef]
- Boulanger, H.; Saksi, S.A.; Achiche, J.; Batusanski, F.; Stawiarski, N.; Diddaoui, A.; Fromentin, L.; Chawki, M. SARS-CoV-2 Antibodies in Hemodialysis Patients Six Months after Infection Compared to Healthcare Workers. Int. J. Nephrol. 2021, 2021, 4747221. [Google Scholar] [CrossRef]
- Cohen, D.E.; Sibbel, S.; Marlowe, G.; Bludorn, K.; Miller, D.; Kelley, T.; Connaire, J.; Young, A.; Tentori, F.; Brunelli, S.M. Antibody status, disease history, and incidence of SARS-CoV-2 infection among patients on chronic dialysis. J. Am. Soc. Nephrol. 2021, 32, 1880–1886. [Google Scholar] [CrossRef]
- Ma, Y.; Diao, B.; Lv, X.; Zhu, J.; Liang, W.; Liu, L.; Bu, W.; Cheng, H.; Zhang, S.; Yang, L.; et al. 2019 novel coronavirus disease in hemodialysis (HD) patients: Report from one HD center in Wuhan, China. medRxiv 2020. [Google Scholar] [CrossRef]
- Hsu, C.M.; Weiner, D.E. COVID-19 in dialysis patients: Outlasting and outsmarting a pandemic. Kidney Int. 2020, 98, 1402–1404. [Google Scholar] [CrossRef]
- Jiang, H.J.; Tang, H.; Xiong, F.; Chen, W.L.; Tian, J.B.; Sun, J.; Dong, J.W.; Wang, X.H.; Jin, X.F.; Ding, Y.Q.; et al. COVID-19 in peritoneal dialysis patients. Clin. J. Am. Soc. Nephrol. 2020, 31, 121–123. [Google Scholar] [CrossRef] [PubMed]
- Jeloka, T.; Gupta, A.; Prasad, N.; Varughese, S.; Mahajan, S.; Nayak, K.S.; Agarwal, S.K.; Abraham, G. COVID-19 Working Group of Indian Society of Nephrology. Indian J. Nephrol. 2020, 30, 171–173. [Google Scholar]
- Sachdeva, M.; Uppal, N.N.; Hirsch, J.S.; Ng, J.H.; Malieckal, D.; Fishbane, S.; Jhaveri, K.D. Northwell COVID-19 Research Consortium and the Northwell Nephrology COVID-19 Research Consortium. COVID-19 in Hospitalized Patients on Chronic Peritoneal Dialysis: A Case Series. Am. J. Nephrol. 2020, 51, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, S.; Gursu, M.; Arici, M.; Sahin, I.; Eren, N.; Yilmaz, M.; Koyuncu, S.; Karahisar Sirali, S. Evaluation of Out-comes of Peritoneal Dialysis Patients in the Post-COVID-19 Period: A National Multicenter Case-Control Study from Turkey. Nephron 2023, 147, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Toapanta, N.; Torres, I.B.; Sellarés, J.; Chamoun, B.; Serón, D.; Moreso, F. Kidney transplantation and COVID-19 renal and patient prognosis. Clin. Kidney J. 2021, 14 (Suppl. S1), i21–i29. [Google Scholar] [CrossRef]
- Mahalingasivam, V.; Craik, A.; Tomlinson, L.A.; Ge, L.; Hou, L.; Wang, Q.; Yang, K.; Fogarty, D.G.; Keenan, C. A systematic review of COVID-19 and kidney transplantation. Kidney Int. Rep. 2021, 6, 24–45. [Google Scholar] [CrossRef]
- Hilbrands, L.B.; Duivenvoorden, R.; Vart, P.; Franssen, C.F.M.; Hemmelder, M.H.; Jager, K.J.; Kieneker, L.M. COVID-19-related mortality in kidney transplant and dialysis patients: Results of the ERACODA collaboration. Nephrol. Dial. Transplant 2020, 35, 1973–1983. [Google Scholar] [CrossRef]
- Gandolfini, I.; Crespo, M.; Hellemans, R.; Maggiore, U.; Mariat, C.; Mjoen, G.; Oniscu, G.C.; Peruzzi, L.; Sever, M.S.; Watschinger, B.; et al. Issues regarding COVID-19 in kidney transplantation in the ERA of the Omicron variant: A commentary by the ERA Descartes Working Group. Nephrol. Dial. Transplant 2022, 22, 1824–1829. [Google Scholar] [CrossRef] [PubMed]
- Maggiore, U.; Abramowicz, D.; Crespo, M.; Mariat, C.; Mjoen, G.; Peruzzi, L.; Sever, M.S.; Oniscu, G.C.; Hilbrands, L.; Watschinger, B. How should I manage immunosuppression in a kidney transplant patient with COVID-19? An ERA-EDTA DESCARTES expert opinion. Nephrol. Dial. Transplant. 2020, 35, 899–904. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.; Montez-Rath, M.E.; Han, J.; Garcia, P.; Cadden, L.; Hunsader, P.; Kerschmann, R.; Beyer, P.; Dittrich, M.; Block, G.A.; et al. Antibody Response to COVID-19 Vaccination in Patients Receiving Dialysis. J. Am. Soc. Nephrol. 2021, 32, 2435–2438. [Google Scholar] [CrossRef]
- Hsu, C.M.; Weiner, D.E.; Manley, H.J.; Aweh, G.N.; Ladik, V.; Frament, J.; Miskulin, D.; Argyropoulos, C.; Abreo, K.; Chin, A.; et al. Seroresponse to SARS-CoV-2 Vaccines among Maintenance Dialysis Patients over 6 Months. Clin. J. Am. Soc. Nephrol. 2022, 17, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Peiyao, R.; Mengjie, Y.; Xiaogang, S.; Wenfang, H.; Danna, Z.; Yuqun, Z.; Juan, J.; Qiang, H. Immunogenicity and safety of SARS-CoV-2 vaccine in hemodialysis patients: A systematic review and meta-analysis. Front. Public Health 2022, 10, 951096. [Google Scholar] [CrossRef]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef]
- Chenchula, S.; Karunakaran, P.; Sharma, S.; Chavan, M. Current evidence on efficacy of COVID-19 booster dose vaccination against the Omicron variant: A systematic review. J. Med. Virol. 2022, 94, 2969–2976. [Google Scholar] [CrossRef]
- Zhou, Z.; Zhu, Y.; Chu, M. Role of COVID-19 Vaccines in SARS-CoV-2 Variants. Front. Immunol. 2022, 13, 898192. [Google Scholar] [CrossRef]
- Zheng, Q.; Wang, M.; Cheng, Y.; Liu, J.; Feng, Z.; Ye, L. Antibody response and safety of COVID-19 vaccine in peritoneal dialysis patients. J. Infect. 2022, 85, e167–e171. [Google Scholar] [CrossRef]
- Panizo, N.; Albert, E.; Giménez-Civera, E.; Puchades, M.J.; D’Marco, L.; Gandía-Salmerón, L.; Giménez, E.; Torre, I.; Sancho, A.; Gavela, E.; et al. Dynamics of SARS-CoV-2-Spike-reactive antibody and T-cell responses in chronic kidney disease patients within 3 months after COVID-19 full vaccination. Clin. Kidney J. 2022, 15, 1562–1573. [Google Scholar] [CrossRef]
- ElSawi, H.A.; Elborollosy, A. Immune-mediated adverse events post-COVID vaccination and types of vaccines: A systematic review and meta-analysis. Egypt. J. Intern. Med. 2022, 34, 1–11. [Google Scholar] [CrossRef]
- Klomjit, N.; Zand, L.; Cornell, L.D.; Alexander, M.P. COVID-19 and Glomerular Diseases. Kidney Int. Rep. 2023, 8, 1137–1150. [Google Scholar] [CrossRef]
- Diebold, M.; Locher, E.; Boide, P.; Enzler-Tschudy, A.; Faivre, A.; Fischer, I.; Helmchen, B.; Hopfer, H.; Kim, M.J.; Moll, S.; et al. Incidence of new onset glomerulonephritis after SARS-CoV-2 mRNA vaccination is not increased. Kidney Int. 2022, 102, 1409–1419. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month conse-quences of COVID-19 in patients discharged from hospital: A cohort study. Lancet. 2023, 401, e21–e33. [Google Scholar] [CrossRef] [PubMed]
- Nugent, J.; Aklilu, A.; Yamamoto, Y.; Simonov, M.; Li, F.; Biswas, A.; Ghazi, L.; Greenberg, H.; Mansour, G.; Moledina, G.; et al. Assessment of Acute Kidney Injury and Longitudinal Kidney Function After Hospital Discharge Among Patients with and Without COVID-19. JAMA Netw. Open 2021, 4, e211095. [Google Scholar] [CrossRef] [PubMed]
- Bowe, B.; Xie, Y.; Xu, E.; Al-Aly, Z. Kidney Outcomes in Long COVID. J. Am. Soc. Nephrol. 2021, 32, 2851–2862. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Huang, L.; Cui, D.; Wang, Y.; Wang, Y.; Xu, J.; Shang, L.; Fan, G.; Cao, B. Association of acute kidney injury with 1-year outcome of kidney function in hospital survivors with COVID-19: A cohort study. Ebiomedicine 2022, 76, 103817. [Google Scholar] [CrossRef]
- Schiffl, H.; Lang, S.M. Long-term interplay between COVID-19 and chronic kidney disease. Int. Urol. Nephrol. 2023, 55, 1977–1984. [Google Scholar] [CrossRef]


{kind=link}
| Antiviral Drugs |
|---|
| (1) Intravenous |
| Remdesevir: no renal dosage adjustment is needed but not recommended in e-GFR ≤ 30 mL/min |
| (2) Oral |
| Molnupiravir: no renal dosage adjustement |
| Nirmatrelvir + Ritonavir : renal dosage adjustement |
| Monoclonal Antibodies |
| Sotrovimab: no renal dosage adjustement |
| Casirivimab + imdevimaband: no renal dosage adjustement |
| Bamlanivimab + etesevimab: no renal dosage adjustement |
| Bebtelovimab: no renal dosage adjustement |
| Tixagevimab-cilgavimab: no renal dosage adjustement |
| Baricitinib: renal dosage adjustement |
| Tofacitinib: renal dosage adjustement |
| Anakinra: not recommended in e-GFR ≤ 30 mL/min |
| Vilobelimab: no data in CKD patients |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dousdampanis, P.; Mouzaki, A.; Trigka, K.; Stefanidis, I.; Galanopoulos, K.-E.; Siavelis, I.-S.; Stathopoulou, D.; Assimakopoulos, S.F. Kidney Issues Associated with COVID-19 Disease. Encyclopedia 2023, 3, 1085-1104. https://doi.org/10.3390/encyclopedia3030079
Dousdampanis P, Mouzaki A, Trigka K, Stefanidis I, Galanopoulos K-E, Siavelis I-S, Stathopoulou D, Assimakopoulos SF. Kidney Issues Associated with COVID-19 Disease. Encyclopedia. 2023; 3(3):1085-1104. https://doi.org/10.3390/encyclopedia3030079
Chicago/Turabian StyleDousdampanis, Periklis, Athanasia Mouzaki, Konstantina Trigka, Ioannis Stefanidis, Konstantinos-Eugenios Galanopoulos, Ioannis-Santo Siavelis, Dionysia Stathopoulou, and Stelios F. Assimakopoulos. 2023. "Kidney Issues Associated with COVID-19 Disease" Encyclopedia 3, no. 3: 1085-1104. https://doi.org/10.3390/encyclopedia3030079