
Trace Elements and Their Management in Dialysis Patients—Pathophysiology and Clinical Manifestations
Abstract
:1. Introduction
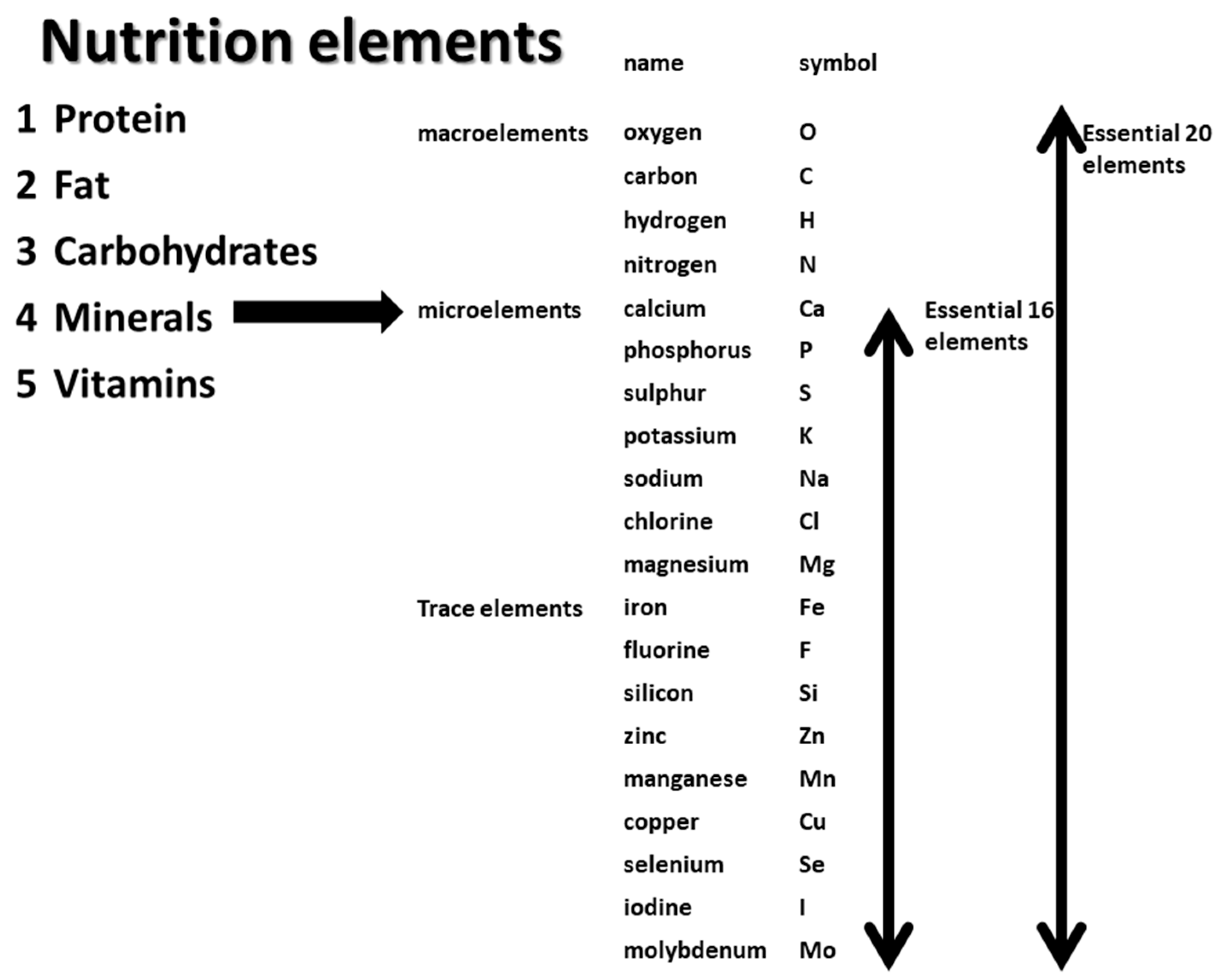
2. What Are Trace Elements?
3. Deficiency of Trace Elements
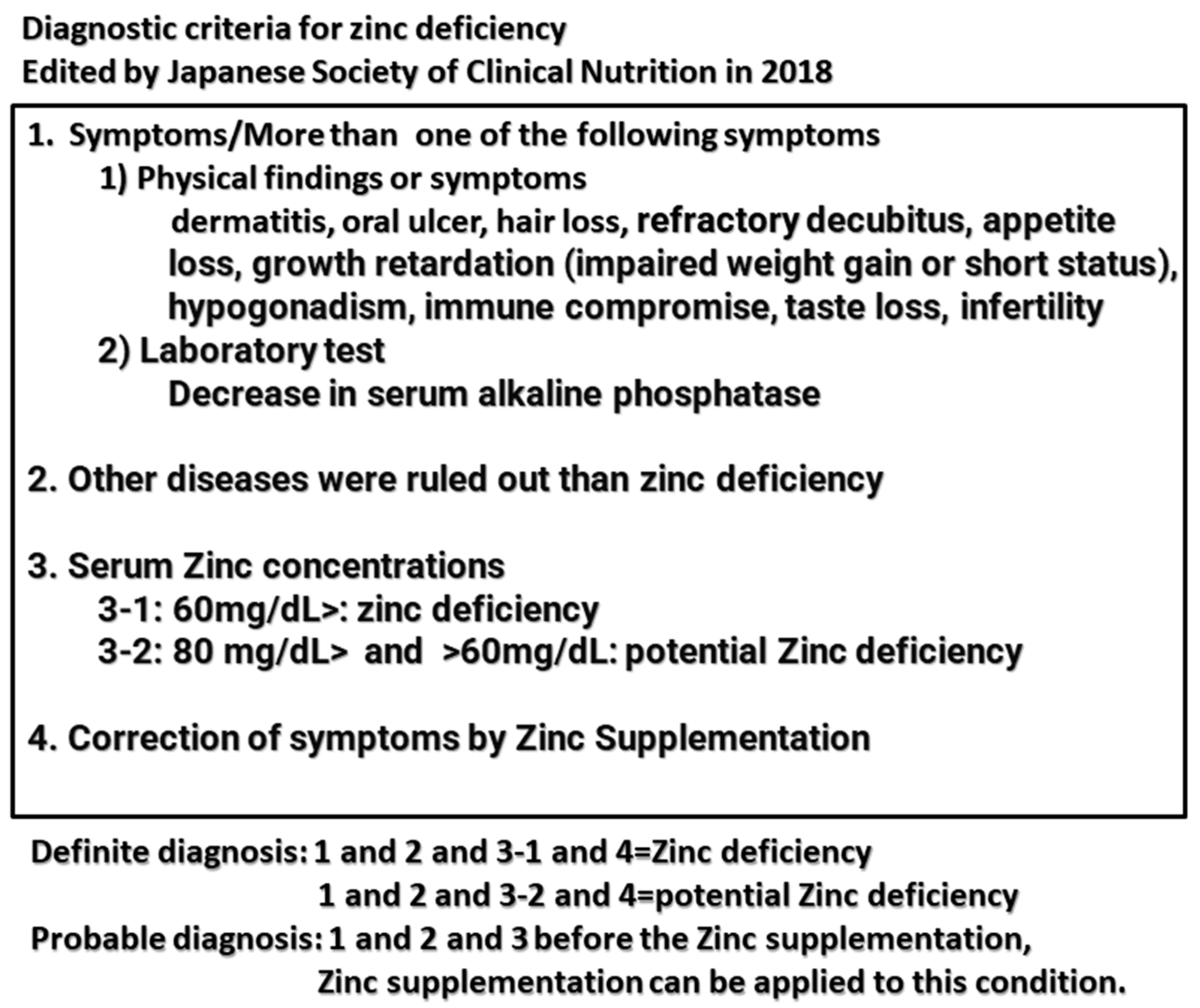
4. Zinc Deficiency in Dialysis Patients
4.1. Zinc and Zinc Deficiency
4.2. Zinc Deficiency in Dialysis Patients
4.3. Treatment of Zinc Deficiency
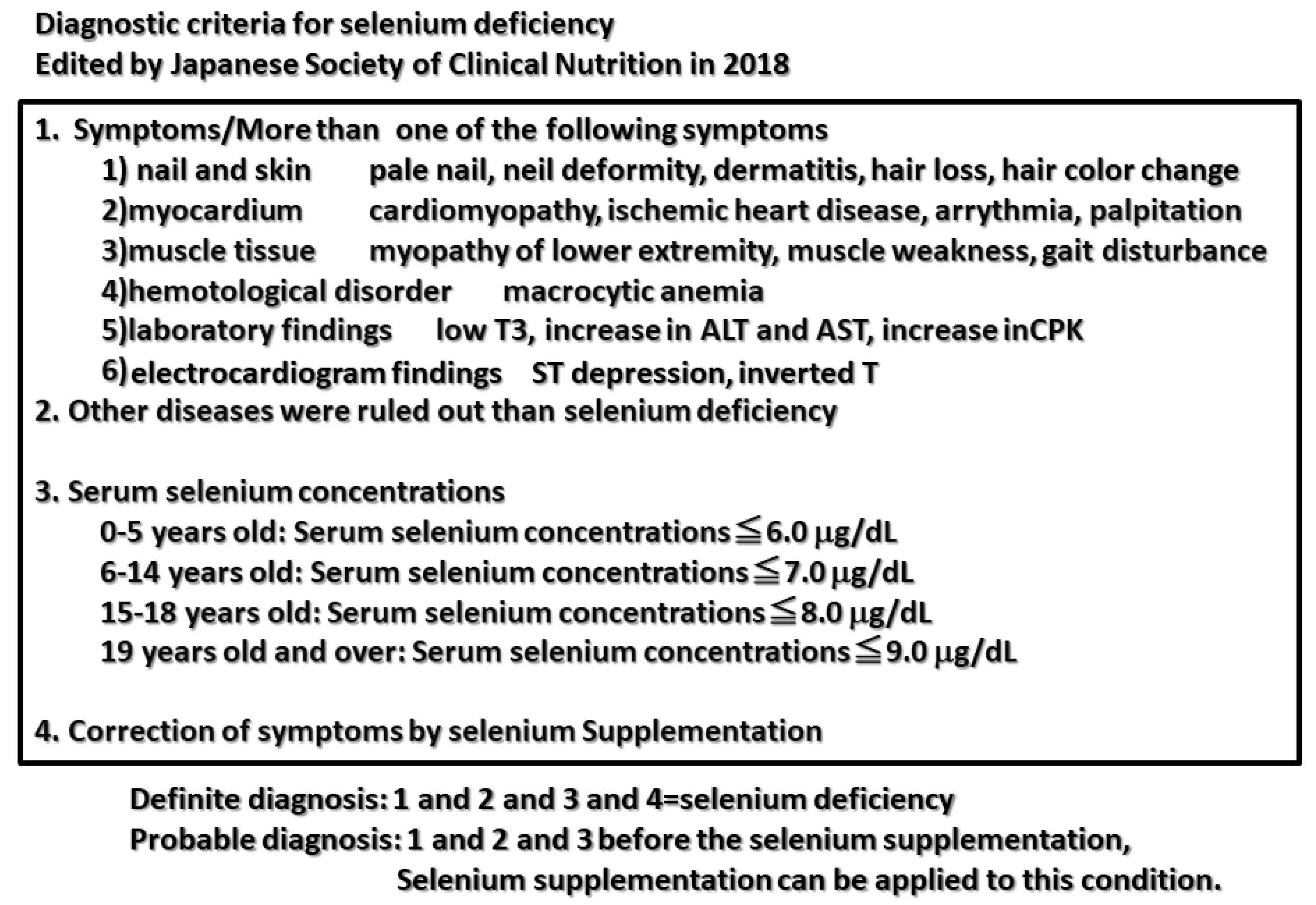
5. Selenium and Selenium Deficiency
5.1. Selenium and Selenium Deficiency
5.2. Selenium Deficiency in Dialysis Patients
5.3. Treatment of Selenium Deficiency in Dialysis Patients
5.4. Several Controversies about Selenium Supplementation
5.4.1. Optimal Serum Concentration of Selenium
5.4.2. The Tissue Distribution of Selenium
5.4.3. Gene Polymorphism of Selenoprotein
5.4.4. The Unique Bioavailability of Selenium
6. Copper
7. Chromium
8. Manganese
9. Lead
10. Arsenic
11. Other Trace Elements
12. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kodama, H.; Itakura, H.; Omori, H.; Sasaki, M.; Sando, K.; Kamura, T.; Fuse, Y.; Hosoi, T.; Yoshida, H. Clinical guidelines for zinc deficiency. J. Jpn. Soc. Clin. Nutr. 2018, 40, 120–167. [Google Scholar]
- Fukushima, T.; Horike, H.; Fujiki, S.; Kitada, S.; Sasaki, T.; Kashihara, N. Zinc deficiency anemia and effects of zinc therapy in maintenance hemodialysis patients. Ther. Apher. Dial. 2009, 13, 213–219. [Google Scholar] [CrossRef]
- Kobayashi, H.; Abe, M.; Okada, K.; Tei, R.; Maruyama, N.; Kikuchi, F.; Higuchi, T.; Soma, M. Oral zinc supplementation reduces the erythropoietin responsiveness index in patients on hemodialysis. Nutrients 2015, 7, 3783–3795. [Google Scholar] [CrossRef]
- Najafabadi, M.M.; Faghihi, G.; Emami, A.; Monghad, M.; Moeenzadeh, F.; Sharif, N.; Jazi, A.H.D. Zinc sulfate for relief of pruritus in patients on maintenance hemodialysis. Ther. Apher. Dial. 2012, 16, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Mapar, M.A.; Pazyar, N.; Siahpoosh, A.; Latifi, S.M.; SS, B.M.; Khazanee, A. Comparison of the efficacy and safety of zinc sulfate vs.placebo in the treatment of pruritus of hemodialytic patients: A pilot randomized, triple-blind study. G Ital. Dermatol. Venereol. 2015, 150, 351–355. [Google Scholar]
- Amerian, M.; Nezakati, E.; Ebrahimi, H.; Zolfaghari, P.; Yarmohammadi, M.; Sohrabi, M.B. Comparative effects of zinc sulfate and hydroxyzine in decreasing pruritus among hemodialysis patients: A cross-over clinical trial. J. Maz. Univ. Med. Sci. 2019, 29, 81–90. [Google Scholar]
- Atkin-Thor, E.; Goddard, B.W.; O’Nion, J.; Stephen, R.L.; Kolff, W.J. Hypogeusia and zinc depletion in chronic dialysis patients. Am. J. Clin. Nutr. 1978, 31, 1948–1951. [Google Scholar] [CrossRef] [PubMed]
- Sprenger, K.B.; Bundschu, D.; Lewis, K.; Spohn, B.; Schmitz, J.; Franz, H.E. Improvement of uremic neuropathy and hypogeusia by dialysate zinc supplementation by dialysate zinc supplementation: A double-blind study. Kidney Int. Suppl. 1983, 16, S315–S318. [Google Scholar]
- Kim, S.M.; Kim, M.; Lee, E.K.; Kim, S.B.; Chang, J.W.; Kim, H.W. The effect of zinc deficiency on salt taste acuity, preference, and dietary sodium intake in hemodialysis patients. Hemodial. Int. 2016, 20, 441–446. [Google Scholar] [CrossRef]
- Momen-Heravi, M.; Barahimi, E.; Razzaghi, R.; Bahmani, F.; Gilasi, H.R.; Asemi, Z. The effects of zinc supplementation on wound healing and metabolic status in patients with diabetic foot ulcer: A randomized, double-blind, placebo-controlled trial. Wound Repair Regen. 2017, 25, 512–520. [Google Scholar] [CrossRef]
- Koyama, A.; Tsuruoka, T.; Fujii, T.; Sugimoto, M.; Banno, H.; Komori, K. Zinc Deficiency and Clinical Outcome After Infrainguinal Bypass Grafting for Critical Limb Ischemia. Circ. Rep. 2020, 2, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-Y.; Wu, M.-L.; Chou, Y.-Y.; Li, S.-Y.; Deng, J.-F.; Yang, W.-C.; Ng, Y.-Y. Essential trace element status and clinical outcomes in long-term dialysis patients: A two-year prospective observational cohort study. Clin. Nutr. 2012, 31, 630–636. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.-J.; Wang, M.-Q.; Hu, R.; Yang, Y.; Huang, Y.-S.; Xian, S.-X.; Lu, L. Effect of Zinc Supplementation on Maintenance Hemodialysis Patients: A Systematic Review and Meta-Analysis of 15 Randomized Controlled Trials. BioMed. Res. Int. 2017, 2017, 1024769. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.M.; Djafarian, K.; Mojtahed, A.; Varkaneh, H.K.; Shab-Bidar, S. The effect of zinc supplementation on plasma C-reactive protein concentrations: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Pharmacol. 2018, 834, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, R.; Montazerifar, F.; Shahraki, E.; Karajibani, M.; Mokhtari, A.M.; Dashipour, A.R.; Ferns, G.A.; Jalali, M. The Effects of Zinc Sulfate Supplementation on Serum Copeptin, C-Reactive Protein and Metabolic Markers in Zinc-Deficient Diabetic Patients on Hemodialysis: A Randomized, Double-Blind, Placebo-Controlled Trial. Biol. Trace Elem. Res. 2022, 200, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Brodersen, H.-P.; Holtkamp, W.; Larbig, D.; Beckers, B.; Thiery, J.; Lautenschläger, J.; Probst, H.-J.; Ropertz, S.; Yavari, A. Zinc supplementation and hepatitis B vaccination in chronic haemodialysis patients: A multicentre study. Nephrol. Dial. Transpl. 1995, 10, 1780. [Google Scholar]
- Jern, N.A.; Vanbeber, A.D.; Gorman, M.A.; Weber, C.G.; Liepa, G.U.; Cochran, C.C. The effects of zinc supplementation on serum zinc concentration and protein catabolic rate in hemodialysis patients. J. Ren. Nutr. 2000, 10, 148–153. [Google Scholar] [CrossRef]
- Candan, F.; Gültekin, F.; Candan, F. Effect of vitamin C and zinc on osmotic fragility and lipid peroxidation in zinc-deficient haemodialysis patients. Cell Biochem. Funct. 2002, 20, 95–98. [Google Scholar] [CrossRef]
- Chevalier, C.A.; Liepa, G.; Murphy, M.D.; Suneson, J.; VanBeber, A.D.; Gorman, M.A.; Cochran, C. The effects of zinc supplementation on serum zinc and cholesterol concentrations in hemodialysis patients. J. Ren. Nutr. 2002, 12, 183–189. [Google Scholar] [CrossRef]
- Rashidi, A.A.; Salehi, M.; Piroozmand, A.; Sagheb, M.M. Effects of zinc supplementation on serum zinc and C-reactive protein concentrations in hemodialysis patients. J. Ren. Nutr. 2009, 19, 475–478. [Google Scholar] [CrossRef]
- Roozbeh, J.; Hedayati, P.; Sagheb, M.M.; Sharifian, M.; Jahromi, A.H.; Shaabani, S.; Jalaeian, H.; Raeisjalali, G.A.; Behzadi, S. Effect of zinc supplementation on triglyceride, cholesterol, LDL, and HDL levels in zinc-deficient hemodialysis patients. Ren. Fail. 2009, 31, 798–801. [Google Scholar] [CrossRef] [PubMed]
- Rahimi-Ardabili, B.; Argani, H.; Ghorbanihaghjo, A.; Rashtchizadeh, N.; Naghavi-Behzad, M.; Ghorashi, S.; Nezami, N. Paraoxonase enzyme activity is enhanced bey zinc supplementation in hemodialysis patients. Ren. Fail. 2012, 34, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Pakfetrat, M.; Shahroodi, J.R.; Zolgadr, A.A.; Larie, H.A.; Nikoo, M.H.; Malekmakan, L. Effects of zinc supplement on plasma homocysteine level in end-stage renal disease patients: A double-blind randomized clinical trial. Biol. Trace Elem. Res. 2013, 153, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Mazani, M.; Argani, H.; Rashtchizadeh, N.; Ghorbanihaghjo, A.; Hamdi, A.; Estiar, M.A.; Nezami, N. Effects of zinc supplementation on antioxidant status and lipid peroxidation in hemodialysis patients. J. Ren. Nutr. 2013, 23, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.H.; Wang, C.L. Effects of zinc supplementation on plasma copper/zinc ratios, oxidative stress, and immunological status in hemodialysis patients. Int. J. Med. Sci. 2013, 10, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Argani, H.; Mahdavi, R.; Ghorbani-Haghjo, A.; Razzaghi, R.; Nikniaz, L.; Gaemmaghami, S.J. Effects of zinc supplementation on serum zinc and leptin levels, BMI, and body composition in hemodialysis patients. J. Trace Elem. Med. Biol. 2014, 28, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Sherbini, N.S.; El-Shazly, A.N.; Elhady, S.A.; El-Mashad, G.M.; Sabry, J.H. Effect of zinc supplementation on body mass index and serum levels of zinc and leptin in pediatric hemodialysis patients. Int. J. Nephrol. Renov. Dis. 2015, 8, 159–163. [Google Scholar] [CrossRef]
- Sato, E.; Sato, S.; Degawa, M.; Ono, T.; Lu, H.; Matsumura, D.; Nomura, M.; Moriyama, N.; Amaha, M.; Nakamura, T. Effects of Zinc Acetate Hydrate Supplementation on Renal Anemia with Hypozincemia in Hemodialysis Patients. Toxins 2022, 14, 746. [Google Scholar] [CrossRef]
- Kodama, H.; Asagiri, M.; Etani, Y.; Koyama, H.; Soh, H.; Ida, S.; Tanaka, Y.; Takayanagi, M.; Funakoshi, M.; Yoshida, M. Clinical guidelines for selenium deficiency. J. Jpn. Soc. Clin. Nutr. 2019, 40, 239–283. [Google Scholar]
- Mochizuki, H.; Yokota, S.; Kaneko, K.; Koh, H.; Ishi, J.; Katsuta, M. A case of SEP complicated with dilated cardiomyopathy probably due to selenium deficiency. J. Jpn. Soc. Dial. Ther. 2001, 34, 1095–1099. [Google Scholar] [CrossRef]
- Nishida, H.; Abe, H.; Iida, Y.; Toriyama, C. A case of left ventricular hypofunction due to selenium-arginine depletion associated with short bowel syndrome and dialysis. Jpn. J. Intern. Med. 2016, 106, 828–833. [Google Scholar]
- Fujishima, Y.; Ohsawa, M.; Itai, K.; Kato, K.; Tanno, K.; Turin, T.C.; Onoda, T.; Endo, S.; Okayama, A.; Fujioka, T. Serum selenium levels are inversely associated with death risk among hemodialysis patients. Transplant 2011, 26, 3331–3338. [Google Scholar] [CrossRef] [PubMed]
- Fujishima, Y.; Ohsawa, M.; Itai, K.; Kato, K.; Tanno, K.; Turin, T.C.; Onoda, T.; Endo, S.; Okayama, A.; Fujioka, T. Serum selenium levels in hemodialysis patients are significantly lower than those in healthy controls. Blood Purif. 2011, 32, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, M.; Wiebe, N.; Bello, A.; Field, C.J.; Gill, J.S.; Hemmelgarn, B.R.; Holmes, D.T.; Jindal, K.; Klarenbach, S.W.; Manns, B.J.; et al. Concentrations of Trace Elements and Clinical Outcomes in Hemodialysis Patients: A Prospective Cohort Study. Clin. J. Am. Soc. Nephrol. 2018, 13, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, A.A.; Jiménez, E.M.; Bermejo-Barrera, P.; Lozano, R.; Seijas, V.M.-E. Selenium and All-cause Mortality in End-Stage Renal Disease. Retrospective Observational Cohort Study. J. Ren. Nutr. 2020, 30, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Taylor, E.W.; Bennett, K.; Saad, R.; Rayman, M.P. Association between regional selenium status and reported outcome of COVID-19 cases in China. Am. J. Clin. Nutr. 2020, 111, 1297–1299. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Tang, T.; Guo, P.; Zou, Q.; Ao, X.; Hu, L.; Tan, L. A meta-analysis of randomized controlled trials: Efficacy of selenium treatment for sepsis. Medicine 2019, 98, e14733. [Google Scholar] [CrossRef] [PubMed]
- Saint-Georges, M.D.; Bonnefont, D.J.; Bourely, B.A.; Jaudon, M.C.; Cereze, P.; Chaumeil, P.; Gard, C.; D’Auzac, C.L. Correction of selenium deficiency in hemodialyzed patients. Kidney Int. Suppl. 1989, 27, S274–S277. [Google Scholar]
- Atakan, A.; Macunluoglu, B.; Kaya, Y.; Ari, E.; Demir, H.; Asicioglu, E.; Kaspar, C. Decreased serum selenium levels are correlated with diminished coronary flow reserve among hemodialysis patients. Biol. Trace Elem. Res. 2013, 155, 333–338. [Google Scholar] [CrossRef]
- Yasukawa, M.; Arai, S.; Nagura, M.; Kido, R.; Asakawa, S.; Hirohama, D.; Yamazaki, O.; Tamura, Y.; Fujimaki, M.; Kobayashi, S.; et al. Selenium Associates with Response to Erythropoiesis-Stimulating Agents in Hemodialysis Patients. Kidney Int. Rep. 2022, 7, 1565–1574. [Google Scholar] [CrossRef]
- Xu, S.; Zou, D.; Tang, R.; Li, S.; Chen, W.; Wen, L.; Liu, Y.; Liu, Y.; Zhong, X. Levels of trace blood elements associated with severe sleep disturbance in maintenance hemodialysis patients. Sleep Breath 2021, 25, 2007–2013. [Google Scholar] [CrossRef]
- Richard, M.J.; Ducros, V.; Forêt, M.; Arnaud, J.; Coudray, C.; Fusselier, M.; Favier, A. Reversal of selenium and zinc deficiencies in chronic hemodialysis patients by intravenous sodium selenite and zinc gluconate supplementation. Biol. Trace Elem. Res. 1993, 39, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, G.; Bonomini, M.; Bomba, G.; Bucci, I.; Todisco, V.; Albertazzi, A.; Monaco, F. Thyroid function and plasma selenium in chronic uremic patients on hemodialysis treatment. Biol. Trace Elem. Res. 1996, 55, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Koenig, J.; Fischer, M.; Bulant, E.; Tiran, B.; Elmadfa, I.; Druml, W. Antioxidant status in patients on chronic hemodialysis therapy: Impact of parenteral selenium supplementation. Wien. Klin. Wochenschr. 1997, 109, 13–19. [Google Scholar] [PubMed]
- Temple, K.A.; Smith, A.M.; Cockram, D.B. Selenate-supplemented nutritional formula increases plasma selenium in hemodialysis patients. J. Ren. Nutr. 2000, 10, 16–23. [Google Scholar] [CrossRef]
- Zachara, B.A.; Koterska, D.; Manitius, J.; Sadowski, L.; Dziedziczko, A.; Salak, A.; Wasowicz, W. Selenium supplementation on plasma glutathione peroxidase activity in patients with end-stage chronic renal failure. Biol. Trace Elem. Res. 2004, 97, 15–30. [Google Scholar] [CrossRef]
- Salehi, M.; Sohrabi, Z.; Ekramzadeh, M.; Fallahzadeh, M.K.; Ayatollahi, M.; Geramizadeh, B.; Hassanzadeh, J.; Sagheb, M.M. Selenium supplementation improves the nutritional status of hemodialysis patients: A randomized, double-blind, placebo-controlled trial. Nephrol. Dial. Transpl. 2013, 28, 716–721. [Google Scholar] [CrossRef]
- Tonelli, M.; Network, F.T.A.K.D.; Wiebe, N.; Thompson, S.; Kinniburgh, D.; Klarenbach, S.W.; Walsh, M.; Bello, A.K.; Faruque, L.; Field, C.; et al. Alberta Kidney Disease Network. Trace element supplementation in hemodialysis patients: A randomized controlled trial. BMC Nephrol. 2015, 16, 52. [Google Scholar] [CrossRef]
- Shahreki, E.; Kaykhaei, M.A.; Mosallanezhad, Z.; Adineh, Z.; Mokhtari, A.M.; Mohammadi, M.; Hosseini, R.; Bazi, A. Effects of Selenium and/or N-Acetyl-Cysteine Supplementation on Nonthyroidal Illness Syndrome in Hemodialysis Patients: A Factorial Randomized Controlled Trial. Pharmacology 2022, 107, 480–485. [Google Scholar] [CrossRef]
- Salimian, M.; Soleimani, A.; Bahmani, F.; Tabatabaei, S.M.H.; Asemi, Z.; Talari, H.R. The effects of selenium administration on carotid intima-media thickness and metabolic status in diabetic hemodialysis patients: A randomized, double-blind, placebo-controlled trial. Clin. Nutr. ESPEN 2022, 47, 58–62. [Google Scholar] [CrossRef]
- Atapour, A.; Vahdat, S.; Hosseini, M.; Mohamadian, H. Effect of Selenium on Triglyceride and Total Cholesterol, Weight Gain, and Physical Activity on Hemodialysis Patients: A Randomized Double-Blinded Controlled Trial. Int. J. Prev. Med. 2022, 13, 63. [Google Scholar] [PubMed]
- Hurst, R.; Armah, C.N.; Dainty, J.R.; Hart, D.J.; Teucher, B.; Goldson, A.J.; Broadley, M.R.; Motley, A.K.; Fairweather-Tait, S.J. Establishing optimal selenium status: Results of a randomized, double-blind, placebo-controlled trial. Am. J. Clin. Nutr. 2010, 91, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, A. Role of Zinc and Copper in Erythropoiesis in Patients on Hemodialysis. J. Ren. Nutr. 2022, 32, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, T.; Matsukawa, Y.; Okada, K.; Oikawa, O.; Yamazaki, T.; Ohnishi, Y.; Fujita, T.; Fukuda, N.; Soma, M.; Matsumoto, K. Correction of copper deficiency improves erythropoietin unresponsiveness in hemodialysis patients with anemia. Intern. Med. 2006, 45, 271–273. [Google Scholar] [CrossRef] [PubMed]
- Gaetke, L.M.; Chow-Johnson, H.S.; Chow, C.K. Copper: Toxicological relevance and mechanisms. Arch. Toxicol. 2014, 88, 1929–1938. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.-H.; Chen, P.-C.; Yeh, M.-S.; Hsiung, D.-Y.; Wang, C.-L. Cu/Zn ratios are associated with nutritional status, oxidative stress, inflammation, and immune abnormalities in patients on peritoneal dialysis. Clin. Biochem. 2011, 44, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Feldman, L.; Beberashvili, I.; Hamad, R.A.; Yakov-Hai, I.; Abramov, E.; Wasser, W.; Gorelik, O.; Rozenberg, R.; Efrati, S. Serum Chromium Levels Are Higher in Peritoneal Dialysis than in Hemodialysis Patients. Perit. Dial. Int. 2019, 39, 330–334. [Google Scholar] [CrossRef]
- Jomova, K.; Valko, M. Advances in metal-induced oxidative stress and human disease. Toxicology 2011, 283, 65–87. [Google Scholar] [CrossRef]
- Hsu, C.-W.; Weng, C.-H.; Lee, C.-C.; Yen, T.-H.; Huang, W.-H. Association of serum chromium levels with malnutrition in hemodialysis patients. BMC Nephrol. 2019, 20, 302. [Google Scholar] [CrossRef]
- Tonelli, M.; Wiebe, N.; Hemmelgarn, B.; Klarenbach, S.; Field, C.; Manns, B.; Thadhani, R.; Gill, J. Alberta Kidney Disease Network. Trace elements in hemodialysis patients: A systematic review and meta-analysis. BMC Med. 2009, 7, 25. [Google Scholar] [CrossRef]
- Aschner, J.L.; Aschner, M. Nutritional aspects of manganese homeostasis. Mol. Aspects Med. 2005, 26, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Keen, C.; Zidenburg-Cherr, S. Encyclopedia of Food Science, Food Technology, and Nutrition; Academic Press: London, UK, 1993. [Google Scholar]
- Tonelli, M.; Wiebe, N.; Bello, A.; Field, C.J.; Gill, J.S.; Hemmelgarn, B.R.; Holmes, D.T.; Jindal, K.; Klarenbach, S.W.; Manns, B.J.; et al. Alberta Kidney Disease Network. Concentrations of Trace Elements in Hemodialysis Patients: A Prospective Cohort Study. Am. J. Kidney Dis. 2017, 70, 696–704. [Google Scholar] [CrossRef]
- Gómez de Oña, C.; Martínez-Morillo, E.; Gago González, E.; Vidau Argüelles, P.; Fernández Merayo, C.; Álvarez Menéndez, F.V. Variation of trace element concentrations in patients undergoing hemodialysis in the north of Spain. Scand. J. Clin. Lab. Invest. 2016, 76, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Hu, J.; Tang, R.; Guo, H.; Chen, Q.; Qiu, J.; Liu, Y.; Tan, R.; Zhong, X. Association between the blood manganese (Mn) and hemoglobin in patients undergoing maintenance hemodialysis. J. Trace Elem. Med. Biol. 2022, 71, 126947. [Google Scholar] [CrossRef]
- Vignoli, A.; Tenori, L.; Luchinat, C. An omics approach to study trace metals in sera of hemodialysis patients treated with erythropoiesis stimulating agents. Metallomics 2022, 14, mfac028. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Peng, H.; Zhang, K.; Xiao, L.; Yuan, Z.; Chen, J.; Wang, Z.; Wang, J.; Huang, H. The insufficiency intake of dietary micronutrients associated with malnutrition-inflammation score in hemodialysis population. PLoS ONE 2013, 8, e66841. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.L.; Lin-Tan, D.T.; Hsu, C.W.; Yen, T.H.; Chen, K.H.; Hsu, H.H.; Ho, T.C.; Hsu, K.H. Association of blood lead levels with mortality in patients on maintenance hemodialysis. Am. J. Med. 2011, 124, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.L.; Lin-Tan, D.T.; Chen, K.H.; Hsu, C.W.; Yen, T.H.; Huang, W.H.; Huang, Y.L. Blood lead levels association with 18-month all-cause mortality in patients with chronic peritoneal dialysis. Nephrol. Dial. Transplant. 2010, 25, 1627–1633. [Google Scholar] [CrossRef]
- Feldman, R.G. Urban lead mining: Lead intoxication among deleaders. N. Engl. J. Med. 1978, 298, 1143–1145. [Google Scholar] [CrossRef]
- Thomson, R.M.; Parry, G.J. Neuropathies associated with excessive exposure to lead. Muscle Nerve 2006, 33, 732–741. [Google Scholar] [CrossRef]
- Huang, W.H.; Hu, C.C.; Yen, T.H.; Hsu, C.W.; Weng, C.H. Blood lead level: An overlooked risk of carpal tunnel syndrome in hemodialysis patients. Ren. Fail. 2019, 41, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Danziger, J.; Mukamal, K.J.; Weinhandl, E. Associations of Community Water Lead Concentrations with Hemoglobin Concentrations and Erythropoietin-Stimulating Agent Use among Patients with Advanced CKD. J. Am. Soc. Nephrol. 2021, 32, 2425–2434. [Google Scholar] [CrossRef]
- Lu, K.C.; Wu, C.C.; Ma, W.Y.; Chen, C.C.; Wu, H.C.; Chu, P. Decreased blood lead levels after calcitriol treatment in hemodialysis patients with secondary hyperparathyroidism. Bone 2011, 49, 1306–1310. [Google Scholar] [CrossRef] [PubMed]
- Ford, M.; Goldfrank, L.; Flomenbaum, N.; Lewin, N.; Howland, M.; Hoffman, R.; Nelson, L. (Eds.) Arsenic. In Goldfrank’s Toxicological Emergencies; McGraw-Hill: New York, NY, USA, 2002; pp. 1183–1199. [Google Scholar]
- Schoen, A.; Beck, B.; Sharma, R.; Dube, E. Arsenic toxicity at low doses: Epidemiological and mode of action considerations. Toxicol, Appl, Pharmacol. 2004, 198, 253–267. [Google Scholar] [CrossRef] [PubMed]
- Morton, W.E.; Caron, G.A. Encephalopathy: An uncommon manifestation of workplace arsenic poisoning? Am. J. Ind. Med. 1989, 15, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Xiang, S.; Jin, Q.; Xu, F.; Yao, Y.; Liang, W.; Zuo, X.; Ye, T.; Ying, C. High serum arsenic and cardiovascular risk factors in patients undergoing continuous ambulatory peritoneal dialysis. J. Trace Elem. Med. Biol. 2019, 52, 1–5. [Google Scholar] [CrossRef]
- Ochi, A.; Ishimura, E.; Tsujimoto, Y.; Kakiya, R.; Tabata, T.; Mori, K.; Shoji, T.; Yasuda, H.; Nishizawa, Y.; Inaba, M. Trace elements in the hair of hemodialysis patients. Biol. Trace Elem. Res. 2011, 143, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Navarro, J.A.; Granadillo, V.A.; Salgado, O.; Rodríguez-Iturbe, B.; García, R.; Delling, G.; Romero, R.A. Bone metal content in patients with chronic renal failure. Clin. Chim. Acta 1992, 211, 133–142. [Google Scholar] [CrossRef]
- Oruc, M.; Mercan, S.; Bakan, S.; Kose, S.; Ikitimur, B.; Trabulus, S.; Altiparmak, M.R. Do trace elements play a role in coronary artery calcification in hemodialysis patients? Int. Urol. Nephrol. 2023, 55, 173–182. [Google Scholar] [CrossRef]
- Katko, M.; Kiss, I.; Karpati, I.; Kadar, A.; Matyus, J.; Csongradi, E.; Posta, J.; Paragh, G.; Balla, J.; Kovacs, B.; et al. Relationship between serum nickel and homocysteine concentration in hemodialysis patients. Biol. Trace. Elem. Res. 2008, 124, 195–205. [Google Scholar] [CrossRef]
- Schrooten, I.; Elseviers, M.M.; Lamberts, L.V.; De Broe, M.E.; D’Haese, P.C. Increased serum strontium levels in dialysis patients: An epidemiological survey. Kidney Int. 1999, 56, 1886–1892. [Google Scholar] [CrossRef]
- D’Haese, P.C.; Schrooten, I.; Goodman, W.G.; Cabrera, W.E.; Lamberts, L.V.; Elseviers, M.M.; Couttenye, M.M.; De Broe, M.E. Increased bone strontium levels in hemodialysis patients with osteomalacia. Kidney Int. 2000, 57, 1107–1114. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Trace Element | Normal Range | Predialysis | Hemodialysis | Peritoneal Dialysis | Deficiency Symptoms |
|---|---|---|---|---|---|
| Zinc (Zn) | 60–121 mg/dL | ↓ | ↓ | ↓ | Growth retardation, wound-healing delay, taste disorder, and sexual dysfunction |
| Manganese (Mn) | 0.31–1.04 mg/dL | ↓ | ↓ or → | → | Anemia and glucose intolerance |
| Selenium (Se) | 18–40 mg/mL | ↓ | ↓ | ↓ | Cardiac dysfunction, immune disorders, and carcinogenesis |
| Copper (Cu) | 68–128 mg/dL | → | → or ↑ | → | Hemolysis, leukocytosis, and metabolic acidosis |
| Cobalt (Co) | 0.04–0.40 mg/L | → | ↑ | ↑ | Cardiac dysfunction and impairment of gluconeogenesis |
| Chromium (Cr) | 0.04–0.35 mg/dL | ↑ | ↑ | ↑ | Liver dysfunction, renal dysfunction, and carcinogenesis |
| Molybdenum (Mo) | 0.27–1.17 mg/L | → | ↑ | ? | Amino acid metabolism disorder, arthropathy, and hypercalcemia |
| Vanadium (V) | 0.10–1.0 mg/L | → | ↑ | ? | Bone disease, dyslipidemia, anemia, and hypertension |
| Silicon (Si) | 0.14–0.20 mg/L | ↑ | ↑ | ↑ | Erythema, bone disease, neuropathy, and Wegener granulomatosis |
| Nickel (Ni) | 0.2–0.8 mg/dL | ↑ | ↑ | ↑ | Cardiac ischemia, anemia, and bone disease |
| Strontium (Sr) | 15–30 mg/L | → | ↑ | ↑ | Osteomalacia |
| Bromine (Br) | 2.19–5.00 mg/L | → | ↑ | ↑ | Sleep disorders |
| Cadmium (Cd) | 2.19–5.00 mg/L | ↑ | ↑ | ↑ | Growth defects, hypertension, and hyperparathyroidism |
| Rubidium (Rb) | 0.095–0.272 mg/L | → | ↑ | → | Depression and central nervous system dysfunction |
| Mode | Number | Treatment Route | Combination | Evaluation | Se Concentration | Outcome | Ref. |
|---|---|---|---|---|---|---|---|
| HD | 40 dialysis HBV non-responder Zn: n = 28 Control: n = 12 | 60 mg zinc aspartate after each dialysis session for 8 weeks | None | HBV antibody formation Titer of HVB antibody | Zn group: 77 ± 2.4 μg/dL Control group: 63 ± 2.1 μg/dL | HBV antibody formation Zn: 6 out of 28 patients Control: 2 out of 12 patients Antibody titer Zn: 0–2364 IE/L Control: 0–1110 IE/L | [16] |
| HD | Randomized, double-blind, before–after trial n = 20 (15 women, 5 men) | Zn: 7.7 pmol zinc sulfate (2200 μg) daily Control: cornstarch placebo capsule daily 90 days | None | Serum Zn concentration PCR (protein catabolic rate) | 12.2 μmol/L (80 μg/dL) on day 0 to 15.3 μmol/L (100 μg/dL) on day 90 | A significant positive correlation (r = 0.61) between PCR and serum zinc concentrations | [17] |
| HD | Zn group: 34 zinc-deficient HD patients. Control group: 16 sex- and age-matched normal volunteers | Zn: zinc (20 mg/day) Control: placebo 3 months | None | Levels of Zn malondialdehyde (MDA) osmotic fragility of red blood cells | Zn: 12.5 ± 1.0 to 18.8 ± 3.0 μmol/L Control: from 12.3 ± 1.0 to 12.1 ± 1.4 μmol/L | Increase in Zn concentration; Improvement of osmotic fragility; Decrease in the level of MDA | [18] |
| HD | Randomized, double-blind, before–after trial | Supplementation of Zn: 7.7 μmol zinc sulfate/day (50 mg elemental zinc/day) Control: cornstarch placebo capsule 90 days | None | Serum zinc, dietary intake, HDL, LDL, and TC | Zn: 0.79 μg/mL to 0.96 μg/mL | Increase in serum total cholesterol and LDL; No change in HDL; Increase in reported energy intake; No change in dietary intake of zinc, cholesterol, total fat, or saturated fat | [19] |
| HD | n = 55 hemodialysis patients (32 men and 23 women) | Zinc supplementation group (n = 28): 220 mg zinc sulfate capsule Control group (n = 27): placebo capsule (220 mg corn starch) 42 days | None | Serum zinc C-reactive protein levels | Zn group: 57.4 ± 2.4 μg/dL to 88.4 ± 4.8 μg/dL | Decrease in serum C-reactive protein: 13.5 ± 3.8 mg/L to 10.5 +/− 3.5 mg/L | [20] |
| HD | Double-blind zinc-deficient HD subjects Total: n = 53 (25 female and 28 male) | Zn group (n = 27): 220 mg zinc sulfate (50 mg elemental zinc) Control group (n = 26): starch placebo 42 days | None | Serum concentration of zinc, total cholesterol, HDL and LDL cholesterol, and triglycerides | Zn group: 0.53 ± 0.36 μg/mL to 0.86 μg/mL ± 0.42 μg/mL Control group: 0.52 ± 0.25 μg/mL to 0.64 ± 0.29 μg/mL | Increase in serum total cholesterol, serum LDL, and HDL cholesterol serum triglyceride | [21] |
| HD | Double-blind, randomized, controlled trial Total: n = 60 | Zn group (n = 30): 100 mg/day zinc Control group (n = 30): placebo 2 months | None | Paraoxonase (PON) enzyme activity Lipid profile apolipoprotein AI (Apo-AI) and B (Apo-B) levels | Not measured | No change in serum levels of TC, TG, or LDL or Apo-B levels Increase in serum levels of HDL, Apo-AI, and PON activity | [22] |
| HD | Double-blind, randomized, clinical trial Total: n = 97 ESRD patients with Zn deficiency | Zn group (n = 50): 50 mg/day Zn Control group (n = 47): placebo 6 weeks | None | Seum Zn Homocysteine (hCys) level | Zn group: 56.9 ± 13.9 to 120.8 ± 26 μg/dL Control group: 60.9 ± 9.8 to 63.9 ± 13.2 μg/dL | Decrease in serum hCys | [23] |
| HD | Double-blind, randomized, controlled trial 65 HD patients | Group A: placebo Group B: zinc (100 mg/day) 2 months. | None | Serum Zn concentration, total antioxidant capacity (TAC), whole blood glutathione peroxidase (GSH) level, superoxide dismutase (SOD) activity, and malondialdehyde (MDA) level | The levels of serum zinc were increased | Increase in TAC, GSH, and SOD activity Decrease in MDA | [24] |
| HD | Long-term HD patients with low plasma Zn concentrations (<80 mg/dL) | Zn group (n = 40): daily oral Zn No supplements (n = 25) Control (n = 38): age- and sex-matched healthy individuals 8 weeks | None | Plasma concentrations of Zn and Cu, Cu/Zn ratios, oxidative stress, and proinflammatory cytokines percentages of CD4 and CD19 lymphocytes CD4/CD8 ratios | The levels of serum Zn were increased | Decrease in Cu, Cu/Zn ratios, oxidative stress status, and inflammatory responses Increase in percentages of CD4 and CD19 lymphocytes and CD4/CD8 ratios | [25] |
| HD | Randomized, double-blind, and placebo-controlled trial 60 HD patients | Supplemented group (n = 30; male/female: 19/11): 100 mg/day elemental Zn Control group (n = 30; male/female: 17/13): placebo 60 days | None | serum zinc serum Leptin anthropometric measurements | Supplemented group: male, 81.7 ± 11 μg/dL to 105.5 ± 18 μg/dL; female, 75.5 ± 11 μg/dL to 106.3 ± 16 μg/dL Control group: male, 85.8 ± 16 μg/dL to 83.6 ± 9.6 μg/dL; female, 80.7 ± 18.8 μg/dL to 86.5 ± 12.7 μg/dL | Decrease in leptin in women; Increase in BMI and body weight in men; Increase in albumin and Hb; Negative association between serum zinc and leptin levels | [26] |
| HD | Prospective clinical trial study Pediatric HD patients between 5 and 18 years old Total: n = 60 | Group I (n = 40): 50–100 mg zinc sulfate (equivalent to 11–22 mg elemental zinc) Group II (n = 20): placebo (cornstarch) twice daily 90 days | None | serum zinc serum leptin anthropometric measurements | Group I: 53.2 ± 8.15 μg/dL to 90.75 ± 12.2 μg/dL Group II: 55.45 ± 9.1 μg/dL to 55.35 ± 9.15 μg/dL | Decrease in leptin; Increase in BMI and body weight; Negative association between serum zinc and leptin levels | [27] |
| HD | Patients on HD with low serum zinc levels (<65 μg/dL) Total: n = 70 | Polaprezinc group (n = 35): polaprezinc, 34 mg/day of zinc Control group (n = 35): no supplementation 12 months | Epoetin alph | ERI (erythropoietin responsiveness index); Weekly ESA dose (units)/dry weight (kg)/hemoglobin (g/dL) | Polaprezinc group: 53 ± 6 μg/dL to 80 ± 18 μg/dL Control group: 55 ± 5 μg/dL to 56 ± 10 μg/dL | Decrease in ESA dosage and ERI; No changes in Hb; No Change in serum iron or TSAT; Decrease in ferritin; Decrease in copper | [3] |
| HD | RCT Zn-deficient diabetic HD patients Total: n = 46 | Zn supplement group (n = 21): 220 mg/day Zn sulfate capsule (containing 50 mg Zn) Control group (n = 25): placebo capsule (220 mg corn starch) 8 weeks | None | serum levels of copeptin, high-sensitive C-reactive protein (hs-CRP) glycemic control anthropometric parameters renal function | Zn supplement group: 55.9 ± 8.0 μg/dL to 90.6 ± 15.7 μg/dL Control group: 68.26 ± 6.2 μg/dL to 68.5 ± 6.5 μg/dL | Decrease in serum copeptin, hs-CRP, BUN, Cr, and FBG levels; Increase in BMI and body weight; No change in QUICKI (quantitative insulin sensitivity check index), HOMA-IR (homeostasis model assessment—insulin resistance), or serum insulin | [15] |
| HD | Before–after trial Patients with serum Zn < 60 μg/dL Total: n = 21 | Zinc acetate hydrate 50 mg 6 months | None | erythropoietin resistance index (ERI) ERI = dose (IU) of erythropoiesis-stimulating agent (ESA)/week/body weight (kg)/hemoglobin content (g/dL) | 52.4 ± 7.6 μg/dL to 84.1 ± 16.3 μg/dL | Decrease in ERI and ESA dose; No change in Hb | [28] |
| Glutathione peroxidase (GPx) | GPx1 | The biochemical function of glutathione peroxidase (GPx) is to reduce lipid hydroperoxides to their corresponding alcohols and to reduce free hydrogen peroxide to water. |
| Gpx2 | ||
| GPx3 | ||
| Gpx4 | ||
| Gpx6 | ||
| Thioredoxin reductases (Txnrd) | TrxR1 | Thioredoxin reductases (TrxR) are the enzymes that catalyze the reduction of thioredoxin; hence, they are a central component in the thioredoxin system. Together with thioredoxin (Trx) and NADPH, this system’s most general description is as a system for reducing disulfide bonds in cells. They contribute to the antioxidant effects. |
| TrxR2 | ||
| TrxR3 | ||
| Iodothyronine deiodinase (DIO) | DIO1 | Iodothyronine deiodinase (DIO) an important enzyme in the activation and deactivation of thyroid hormones. Thyroxine (T4), the precursor of 3,5,3′-triiodothyronine (T3), is transformed into T3 by deiodinase activity. |
| DIO2 | ||
| DIO3 | ||
| Selenoprotein | SelH | Selenoproteins (Sels) are composed of 13 proteins that contain selenium in the molecule. Selenoprotein P is the most common selenoprotein found in the plasma. It is unusual because in humans, it contains 10 s residues. |
| SelI | ||
| SelK | ||
| SelM | ||
| Sel15 | ||
| SelN | ||
| SelO | ||
| SelP | ||
| SelR | ||
| SelS | ||
| SelT | ||
| SelV | ||
| SelW |
| Subject | Number | Treatment Route | Combination | Evaluation | Se Concentration | Outcome | Ref. |
|---|---|---|---|---|---|---|---|
| HD | Se group: n = 39 Control group: n = 15 | 500 μg oral administration for 3 months and 200 μg for the next 2 months | None | Serum GPx, GPx in RBC, and muscle volume IVS in echocardiogram | 3.83 μg/dL to 9.0–8.0 μg/dL | Increase in serum GPx and GPx in RBC; Increase in muscle volume; Decrease in IVS | [38] |
| HD | Se group: n = 6 | 50 μg intravenous administration for 5 weeks and 100 μg for the next 15 weeks | Intravenous Zn gluconate for 20 weeks | Serum GPx, GPx in RBC, serum TBARs, and serum Zn | 0.45 μmol/L to 0.89 μmol/L | Increase in serum GPx and GPx in RBC; Decrease in serum TBARS; No change in serum Zn | [42] |
| HD | Se group: n = 10 Placebo group: n = 5 | 500 μg oral administration for 3 months and 200 μg for the next 3 months | None | Serum Se fT3 and TSH | Se group: 7.68 μg/dL Placebo group: 5.30 μg/L | Increase in serum Se; Increase in fT3; Decrease in TSH | [43] |
| HD | Se group: n = 12 | 400 mg Intravenous sodium selenite after HD for 8 weeks | None | Serum Se and α-tocopherol, Se and α-tocopherol in RBC Serum ascorbic acid, serum retinol, serum glutathione, GPx, SOD activity in RBC, and serum MDA | Serum Se: increased to 8.37 μg/dL 4 weeks after the treatment Se in RBC: increased to 15.9 μg/dL 4 weeks after the treatment | GPx activity: increase in serum levels and no change in RBC; Decrease in MDA; No change in CAT or SOD activity | [44] |
| HD | Total: n = 793 Divided into 3 groups Three-affiliation prospective, randomized, single-blind study | Oral selenite Se 28 μg, Oral selenate Se 28 μg Control oral Se 7 μg 14 days | Energy intake of 35 kcal/kg/day | Serum GPx, GPx in RBC, and Se in RBC | Selenite group: 1.4 μmol/L Selenate group: 1.5 μmol/L Control group: 1.2 μmol/L | No differences in serum GPx, GPx in RBC, or Se in RBC | [45] |
| HD | 4 groups n = 15 in each group | Erythropoietin (EPO) 2000 × 3/week Se-rich yeast 300 μg × 3/week |
| Serum GPx and GPx activity in RBC | Increased to 120, 110, and 150 ng/mL in Se concentration in serum, blood, and RBC. Se concentration in serum and blood plateaued. Se in RBC increased to 200–250 ng/mL. | Increase in GPx activity in RBC in groups 3 and 4; No change in serum GPx | [46] |
| HD | Total: n = 80 Se group: n = 29 Placebo group: n = 36 Randomized, double-blind, placebo-controlled study | 200 μg/day oral administration for 12 weeks | None | Primary; SGA Secondary: MDA, IL-6, high-sensitivity CRP, homocysteine, transferrin, ferritin, MIS, and Hb | Not measured | Decrease in SGA and MIS; Decrease in MDA; No change in IL-6, high-sensitivity CRP, homocysteine, transferrin, ferritin, or Hb | [47] |
| HD | Total: n = 150 Three groups n = 50 in each group Randomized, double-blind, active-control study | Se capsule 1. standard supplementation (SS) (vitamins) 2. Low supplementation (LS) SS + vitamin E 250 IU + Zn 25 mg + Se 5 μg 3. Moderate supplementation (MS) SS + vitamin E 250 IU +Zn 50 mg + Se 75 μg | Standard supplementation; biotin 300 μg, folic acid 1 mg, nicotinamide 20 mg, thiamine 1.5 mg Cyanocobalamin 6 μg, riboflavin 1.7 mg, pyrydoxine 10 mg, ascorbic acid 100 mg | Primary: incidence of low Se and low Zn after 90 days Secondary: incidence of low Se and low Zn after 180 days Low Zn: Zn < 815 μg/L Low Se: Se < 121 μg/L | Day 90: SS: Se, 13.1 μg/dL LS: Se, 14.0 μg/dL MS: Se, 14.6 μg/dL Day 180: SS: Se, 13.5 μg/dL LS: Se, 13.5 μg/dL MS: Se, 13.0 μg/dL | Primary and secondary outcomes: No difference among three groups; No difference in sodium sensitivity or intradialytic body weight gain | [48] |
| HD | Total: n = 68 Se and NAC (N-acetylcysteine) treatment 4 groups each n = 17 12 weeks | Group A:placebo Group B: NAC 600 μg/day Group C: Se 200 μg/day Group D: Se 200 μg/day+ NAC 600 μg/day | NAC N-acetylcysteine | Free tri-iodothyronine (FT3), free thyroxine (FT4), thyroid-stimulating hormone (TSH), and reverse T3 (rT3) | Not measured | Decrease in rT3 levels in groups B, C, and D; No change in FT3, FT4, and TSH between the groups; Good effects on nonthyroidal illness syndrome (NTIS) | [49] |
| HD | 53 diabetic HD patients Randomized, double-blind, placebo-controlled trial | Selenium group (n = 26): 200 μg selenium per day Placebo group (n = 27) for 24 weeks | None | Carotid intima-media thickness, FPG, insulin, HOMA-IR, QUICKI, triglycerides, VLDL-C, total-C, LDL-C, HDL-C, CRP, total nitrites, TAC, GSH (total glutathione), and MDA | Not measured | Decrease in serum insulin levels, insulin resistance, total cholesterol, LDL cholesterol, and CRP; Increase in insulin sensitivity, HDL cholesterol, and GSH; No change in carotid intima-media thickness | [50] |
| HD | Total: n = 78 Intervention: n = 40 Placebo: n = 38 Double-blind clinical trial | 400 μg Oral selenium vs. placebo tablets three times after each hemodialysis session for 3 months | None | Blood Se levels, serum triglyceride, total cholesterol, weight, and physical activities (five times sit to stand test) | Intervention: 40 to 65 µg/L Placebo: 45 to 42 µg/L | Increase in Se concentration and physical activity in intervention group; No change in triglycerides, total cholesterol, or body weight in either group | [51] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wakino, S. Trace Elements and Their Management in Dialysis Patients—Pathophysiology and Clinical Manifestations. Kidney Dial. 2023, 3, 274-296. https://doi.org/10.3390/kidneydial3030025
Wakino S. Trace Elements and Their Management in Dialysis Patients—Pathophysiology and Clinical Manifestations. Kidney and Dialysis. 2023; 3(3):274-296. https://doi.org/10.3390/kidneydial3030025
Chicago/Turabian StyleWakino, Shu. 2023. "Trace Elements and Their Management in Dialysis Patients—Pathophysiology and Clinical Manifestations" Kidney and Dialysis 3, no. 3: 274-296. https://doi.org/10.3390/kidneydial3030025