
Differential Diagnosis in the Management of Acute Respiratory Infections through Point-of-Care Rapid Testing in a Post-Pandemic Scenario in Latin America: Special Focus on COVID-19, Influenza, and Respiratory Syncytial Virus
 , , , , , and
, , , , , and
Abstract
:1. Scope and Methodology
- Multidimensional impact of ARIs in the region and focus countries.
- Opportunities and challenges for the management of ARIs in a COVID-19 post-pandemic scenario.
- Scientific perspectives and positions on the role and value of testing, POC rapid testing, and differential diagnosis for the management of ARIs.
- The current international guidelines and recommendations regarding testing for ARIs, including POC rapid testing regionally and in focus countries.
- Key policies, frameworks, and recommendations for the management of ARIs regionally and in focus countries.
2. Background and Introduction

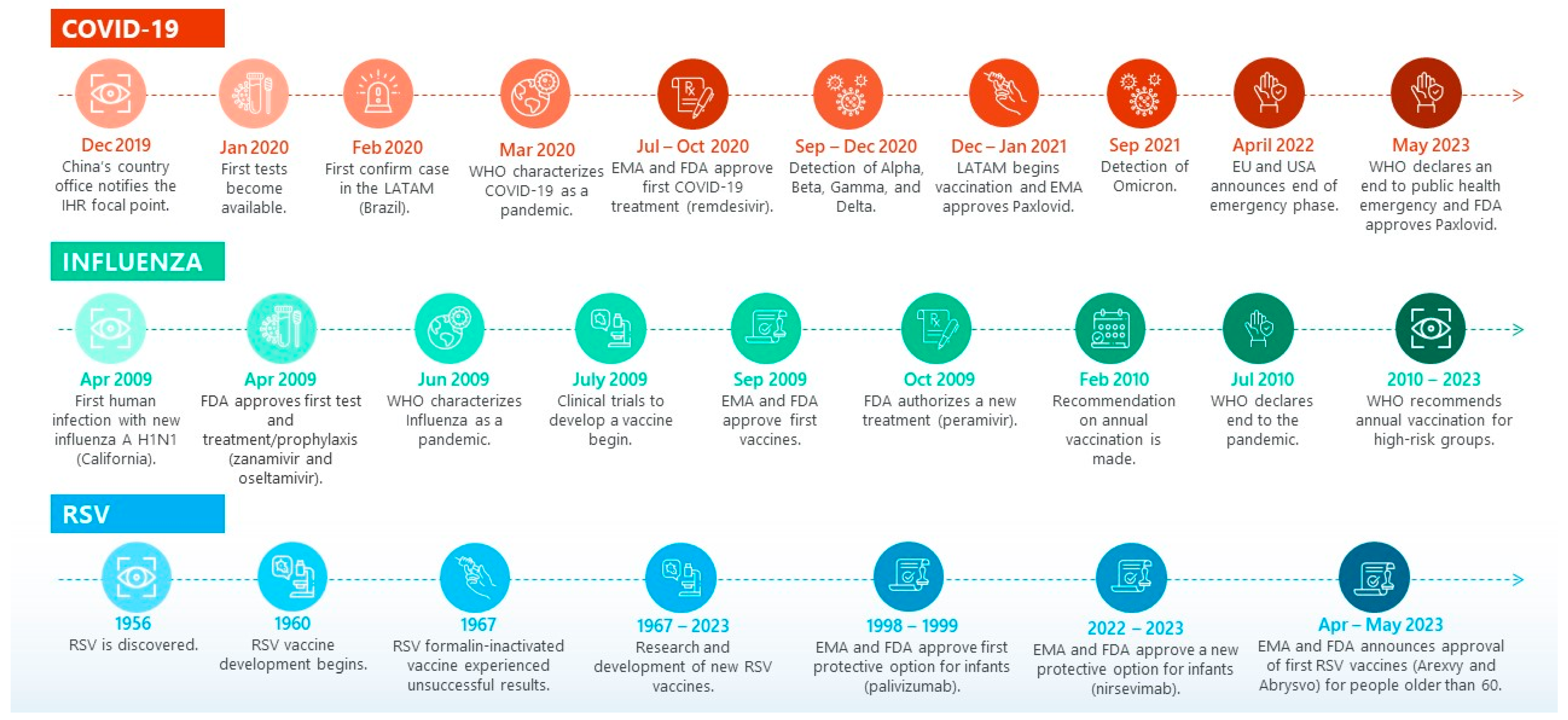
2.1. Vaccines and Treatments Available and in the Pipeline for ARIs
2.2. Misdiagnosis of ARIs and Its Impact on Drug Resistance
3. Impact of ARIs and COVID-19 in LATAM
4. Overview of Testing Options Available for ARIs
4.1. Types of Tests Available for Detecting COVID-19
4.2. Types of Tests Available for Detecting Influenza
4.3. Types of Tests Available for Detecting RSV
4.4. Types of Tests Eligible for POC Rapid Testing
5. What Is POC Rapid Testing?
- Disease identification: facilitates identifying the disease in a quick manner, allowing decisions to be made regarding adequate treatment and care, which in turn can reduce hospital follow-up visits.
- Disease monitoring: allows monitoring of the disease, including aspects such as the response to medicines.
- Behavior modification: contributes to patients’ capacity to modify behaviors to avoid further transmission swiftly and to improve the patient’s outcome.
- Reduced barriers to care: can also help reduce disparities in access to diagnosis in remote settings.
6. The Role and Value of POC Rapid Testing in the Diagnosis and Management of ARIs in a Post-Pandemic Scenario
- National policy, guidelines, and implementation plans.
- Strong governance and consultation.
- Champions from government, community, and health services.
- Shared responsibilities between the POC program and jurisdictional stakeholders.
- Staggered roll-out to learn lessons from the first tier of sites.
- Transparent but strict inclusion criteria due to limited test supply.
- Funding for diagnostics and personal protective equipment.
- Local supply of quality control and external quality assurance materials.
- Robust quality-control development, overcoming cold-chain barriers.
- Use of platforms already in place by a subset of health services.
- Reactive supply chain systems.
- Program website for rapid dissemination of program resources.
- Flexible connectivity systems.
- Referral pathways with accredited pathology providers.
- Capacity-building for health-care workers through a comprehensive set of procedures, posters, and other resources.
- Training and competency assessments delivered virtually, meaning no face-to-face contact is required.
- Monitoring and evaluation systems, including a real-time dashboard to enable management of stock and monitoring of the implementation progress.
- Flexibility in the implementation model to meet different jurisdictional and health service needs.
7. Current Recommendations on the Use of POC Rapid Testing for the Diagnosis and Management of ARIs

{kind=link}
| Country | National Health Plan Includes Respiratory Illnesses | National Policy Program for RSV | National Policy Program for Influenza | National Policy for Respiratory Illnesses (NPRI) | NPRI Integrates COVID-19, Influenza, and RSV a | Current Preferred Diagnostic Method for COVID-19 | Purpose of COVID-19 Rapid Testing | Current Recommendations Relevant to ARI Multiplex Testing | Are Multiplex Tests Available in the Market? b |
|---|---|---|---|---|---|---|---|---|---|
| Argentina | Yes [244] | No | Yes [244] | Yes [244] | Yes [244] | Antigen test [244] | Diagnosis, clinical management, surveillance, and control [244] | Recommended for pediatrics (less than 5 years old) and hospitalized patients [244] | Yes [263,264] |
| Brazil | Yes [265] | No | Yes [266,267] | Yes [268] | Partial c [259] | Antigen test [245,246] | Diagnosis, surveillance, and control [245,246] | No mention of multiplex tests in the national guidelines [245,246] | Yes [269] |
| Chile | Yes [270] | No | Yes [271] | Yes [272] | Yes [260] | Antigen test [247] | Diagnosis, surveillance, and control [247,273] | No mention of multiplex tests in the national guidelines | Yes [274] |
| Colombia | Yes [275] | No | Yes [276,277] | Yes [278,279] | Yes d [261] | Antigen and PCR tests [248] | Diagnosis and surveillance [248] | Recommended for hospitalized patients with a negative PCR for COVID-19 [261] | Yes [280] |
| Costa Rica | Yes e [281] | No | Yes [282] | Yes [282] | No | Antigen test [249] | Diagnosis and surveillance [249] | No mention of multiplex tests in the national guidelines [249] | Yes f [283] |
| Mexico | Yes [284] | No | Yes [285] | Yes [85] | Yes [85,262] | Antigen and PCR test [85,286] | Diagnosis and surveillance [85,262] | Recommended in serious cases and deaths covering only 10% of cases [85] | Yes [287] |
| Peru | Yes [288] | No | Yes [289] | Yes [290] | No [250,290] | Antigen test [250] | Diagnosis Surveillance [250] | No mention of multiplex tests in the national guidelines [250] | Yes [291] |
8. Challenges and Barriers to POC Rapid Testing of ARIs in a Post-Pandemic Scenario
8.1. Challenges and Barriers Related to Intrinsic Tests Limitations and Characteristics
8.2. Challenges and Barriers Regarding the Availability of Tests and Capacity to Implement POC Rapid Testing Strategies
8.3. Challenges and Barriers Regarding the Capacity to Make Adequate Use of POC Rapid Testing Results for Surveillance Purposes
8.4. Challenges and Barriers Related to Policies and Regulations for POC Rapid Testing
9. Policy Recommendations
9.1. Actions to Develop Evidence and Resolve Knowledge Gaps
- (a)
- There is a need to continue developing evidence on the cost-effectiveness of ARI POC rapid testing. Research institutes and the academic community, coordinated and motivated by governments, should undertake further studies that can provide insights into the value of differential diagnostics for respiratory infections. These studies could focus on generating evidence on the different POC rapid testing methods and their value for clinical management, prognosis, and surveillance.
- (b)
- Governments should commit to and implement measures and policies to actively identify the causing agents of ARI cases in the region, providing a more complete picture of the challenges and priorities that need to be addressed through POC testing, including the use of rapid tests and multiplex tests.
- (c)
- Governments should promote and conduct longitudinal and multicenter studies to overcome the knowledge gaps for the cost-effective use of multiplex tests at POC. Regional collaboration, under the leadership of flagship research centers, might help overcome logistical, resource, and capacity challenges to run such studies individually. As a result, recommendations should be made to enhance the adequate use of these tests for case management, surveillance activities, and public health policy decision-making. Studies should explore the potential benefits of using multiplex tests at POC in terms of costs saved by the health system, including costs associated with the course of the diseases (e.g., hospitalization, multiple interactions with healthcare providers, etc.).
- (d)
- Efforts to resolve knowledge gaps to understand the value of differential diagnostics at POC should pay particular attention to the multidimensional socio-economic impact of ARIs. Studies should also ensure that measures are taken to enhance the comparability of data across countries, allowing evidence to be shared across the region. Countries that have the capacity, ability, and resources to implement studies to develop knowledge and resolve gaps should collaborate with countries that require support, to share knowledge and evidence that can be extrapolated to inform policy decision-making.
- (e)
- Funding the research and development of new tests should be prioritized as new ARI virus variants will continue to emerge that might impact the accuracy of existing tests. Research and development strategies should consider performance verification and validation against potential future variants.
- (f)
- Test innovation efforts should consider the multiple uses of these technologies, including those beyond diagnostic (e.g., tests that are able to provide a prognosis). Tests should be accompanied by detailed guidelines to ensure their adequate use and interpretation.
9.2. Actions to Strengthen Capacity to Implement POC Rapid Testing
- (a)
- The use of antigen or molecular rapid tests for POC differential diagnosis should be considered according to the health systems’ capacity (including laboratory and technical capacity), resources, and costs. Given persistent financial constraints in the health sector in many LATAM countries and the advantages outlined by antigen rapid tests, they profile as the more suitable alternative for POC testing in the region.
- (b)
- Decisions regarding the use of antigen or molecular rapid tests for differential diagnosis need to balance and consider the use of the information provided by such tests, their cost-effectiveness, and other considerations, such as budget impact, feasibility of its implementation in actual practice, testing demand, laboratory capacity, tests accuracy, and testing turnaround times. Using a combination of both for different purposes and contexts might be considered (e.g., using molecular tests for sentinel surveillance purposes and antigen tests for POC diagnostics and case management, or using antigen tests for initial screening and molecular tests in case of negative results).
- (c)
- Governments should allocate dedicated resources to implement an ARI POC diagnostic strategy, addressing aspects of health workforce capacity-building, regulation and procurement of quality diagnostic tests, accessibility, and research and development. In context with limited financial resources, governments might benefit from building public-private partnerships to support addressing capacity-building concerns.
- (d)
- Governments should install and promote a training strategy on POC testing to guarantee that healthcare providers have the necessary skills and knowledge to guarantee the proper use, implementation, and interpretation of POC rapid tests. Training opportunities should be provided at different levels of care and with a particular focus on primary health care.
- (e)
- Governments should prioritize strengthening local capacities and mechanisms for genomic and metagenomic surveillance to be able to timely identify new pathogens associated with respiratory disease outbreaks. This may require investment in infrastructure, laboratory capacity, and technology.
- (f)
- Governments and international organizations should ensure the integration of ARI surveillance systems, both at national and international levels, promoting the interconnectivity between the different surveillance agencies in the LATAM region. Surveillance systems should capture and associate variants with severity, comorbidities, and age groups, among other risk factors.
- (g)
- Governments should ensure that the information collected through POC rapid testing is integrated with a broader health information platform, enhancing the opportunity to continue learning about the risk factors and health impact of COVID-19 and other ARIs.
9.3. Actions to Ensure Adequate Means of Implementation
- (a)
- International organizations (e.g., the PAHO and Southern Common Market) and professional societies should provide guidance and support to national decision-makers on the use of POC rapid tests across different settings and conditions.
- (b)
- International organizations and Ministries of Foreign Relations should align and provide guidelines to regulatory agencies in the region to ensure that approval procedures guarantee high-quality tests are available in the territories. Approval processes should be standardized across the region and ensure tests include information about the conditions and limitations of each methodology.
- (c)
- Policymakers, payers, medical societies, and healthcare providers should form a cross-functional partnership to collaborate on the ongoing development of knowledge related to the diagnosis of respiratory infections.
- (d)
- There should be a multistakeholder strategy for healthcare system strengthening, improved market sustainability, and integration of differential diagnostics into existing epidemic and pandemic response and preparedness plans. This strategy should be informed and supported by governments, medical societies, academic communities, and universities, among others.
9.4. Actions for the Inclusion of POC Rapid Testing in Respiratory Policies
- (a)
- Governments should consider using POC rapid testing to support case management. The differential diagnosis of ARIs at POC might positively impact the clinical management of high-risk patients and the management of disease in the general population when treatments are available, as well as reducing unnecessary or prolonged antibiotic courses (improved antimicrobial stewardship) and hospital admissions.
- (b)
- Given the risks of long COVID and COVID-19-related sequels, as well as sequels from other ARIs, the use of POC rapid testing should be prioritized to promote the early diagnosis of cases and prevent the further spread of infections.
- (c)
- Governments should consider using POC rapid testing to support the monitoring of infections and diseases as well as surveillance efforts. Evidence generated through POC rapid testing can be used for policy decision-making purposes. Evidence collected through POC testing can help monitor the burden of disease over time, control transmission, and prevent and control future outbreaks.
- (d)
- Governments should provide regulatory standards for POC rapid testing considering the conditions for approval, implementation, and the information registry. Regulatory standards will contribute to guaranteeing the quality of the tests (including sensitivity) and proper implementation, contributing to the accuracy of the results. Regulatory standards should be the norm in both the public and private sectors.
- (e)
- Creating a consistent regulatory framework for the standardized approval of COVID-19 rapid tests across LATAM countries might be beneficial. This could include collaborating to establish a regional body similar to EMA for harmonizing the approval process; developing standardized technical requirements for the validation and registration of tests (including sensitivity, specificity, sample type, and testing conditions); creating a common technical dossier format for test manufacturers to submit; establishing and strengthening mutual recognition agreements between countries; and developing comprehensive regulatory guidelines that detail the approval process, including pre-market evaluation, quality control, post-market surveillance, and transparent decision-making, among others.
- (f)
- Governments should consider including POC rapid tests in their national Essential Diagnostic Lists, based on the recognition of the value of diagnosis and disease monitoring and surveillance. Civil societies and patient advocacy groups could advocate for this inclusion.
- (g)
- Governments should include clear guidelines regarding POC rapid testing in relevant respiratory infections policies. Guidelines should specify which test to use, and in what setting, considering test characteristics of sensitivity, accuracy, accessibility, affordability, and the test result turnaround time. The guidelines should also address strategies to reduce access inequalities in the territories.
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Archived: WHO Timeline—COVID-19. 27 April 2020. Available online: https://www.who.int/news/item/27-04-2020-who-timeline---covid-19 (accessed on 13 August 2023).
- U.S. Food & Drug Administration. FDA Approves First Treatment for COVID-19. 2020. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-covid-19 (accessed on 13 August 2023).
- European Medicines Agency. COVID-19 Treatments: Authorized. 2023. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/treatments-vaccines/treatments-covid-19/covid-19-treatments-authorised (accessed on 3 May 2023).
- United Nations. WHO Chief Declares End to COVID-19 as a Global Health Emergency. UN News, 5 May 2023. Available online: https://news.un.org/en/story/2023/05/1136367(accessed on 13 August 2023).
- U.S. Food and Drug Administration (FDA). Authorizations of Emergency Use of Certain Antiviral Drugs-Zanamivir and Oseltamivir Phosphate; Availability. 2009. Available online: https://www.federalregister.gov/documents/2009/08/04/E9-18568/authorizations-of-emergency-use-of-certain-antiviral-drugs-zanamivir-and-oseltamivir-phosphate (accessed on 12 August 2023).
- Centers for Disease Control and Prevention (CDC). Influenza Historic Timeline. 2019. Available online: https://www.cdc.gov/flu/pandemic-resources/pandemic-timeline-1930-and-beyond.htm (accessed on 10 August 2023).
- European Centre for Disease Prevention and Control (ECDC). Timeline on the Pandemic (H1N1) 2009. August 2010. Available online: https://www.ecdc.europa.eu/en/seasonal-influenza/2009-influenza-h1n1-timeiline (accessed on 10 August 2023).
- Yu, Y.; Garg, S.; Yu, P.A.; Kim, H.-J.; Patel, A.; Merlin, T.; Redd, S.; Uyeki, T.M. Peramivir Use for Treatment of Hospitalized Patients With Influenza A(H1N1)Pdm09 Under Emergency Use Authorization, October 2009–June 2010. Clin. Infect. Dis. 2012, 55, 8–15. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). Coronavirus Disease 2019 (COVID-19) Pandemic: Increased Transmission in the EU/EEA and the UK—Seventh Update; ECDC: Stockholm, Sweden, 2020. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/RRA-seventh-update-Outbreak-of-coronavirus-disease-COVID-19.pdf (accessed on 10 August 2023).
- Pabbaraju, K.; Wong, A.A.; Douesnard, M.; Ma, R.; Gill, K.; Dieu, P.; Fonseca, K.; Zelyas, N.; Tipples, G.A. A Public Health Laboratory Response to the Pandemic. J. Clin. Microbiol. 2020, 58, e01110-20. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Ten Years of Gains: A Look Back at Progress Since the 2009 H1N1 Pandemic. 2019. Available online: https://www.cdc.gov/flu/spotlights/2018-2019/decade-since-h1n1-pandemic.html (accessed on 12 August 2023).
- Chow, E.J.; Uyeki, T.M.; Chu, H.Y. The Effects of the COVID-19 Pandemic on Community Respiratory Virus Activity. Nat. Rev. Microbiol. 2022, 21, 195–210. [Google Scholar] [CrossRef]
- Bish, D.R.; Bish, E.K.; El-Hajj, H.; Aprahamian, H. A Robust Pooled Testing Approach to Expand COVID-19 Screening Capacity. PLoS ONE 2021, 16, e0246285. [Google Scholar] [CrossRef] [PubMed]
- Hills, T.; Kearns, N.; Kearns, C.; Beasley, R. Influenza Control during the COVID-19 Pandemic. Lancet 2020, 396, 1633–1634. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization (PAHO). Guidance for the Implementation of the Influenza and SARS-CoV-2 Multiplex RT-PCR Assay into the Influenza and COVID-19 Integrated Surveillance. 2021 May. Available online: https://www.paho.org/en/documents/guidance-implementation-influenza-and-sars-cov-2-multiplex-rt-pcr-assay-influenza-and (accessed on 10 August 2023).
- European Centre for Disease Prevention and Control (ECDC). SARS-CoV-2 Variants of Concern as of 10 August 2023. 2023. Available online: https://www.ecdc.europa.eu/en/covid-19/variants-concern (accessed on 10 August 2023).
- European Commission. COVID-19: Commission Calls on Member States to Step Up Preparedness for the Next Pandemic Phase. 2022. Available online: https://ec.europa.eu/commission/presscorner/detail/en/ip_22_2646 (accessed on 10 August 2023).
- World Health Organization (WHO). Influenza (Seasonal). 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal) (accessed on 13 August 2023).
- Centers for Disease Control and Prevention (CDC). Respiratory Syncytial Virus Infection (RSV). For Healthcare Providers. 2023. Available online: https://www.cdc.gov/rsv/clinical/index.html#clinical%20 (accessed on 10 August 2023).
- Acosta, P.L.; Caballero, M.T.; Polack, F.P. Brief History and Characterization of Enhanced Respiratory Syncytial Virus Disease. Clin. Vaccine Immunol. 2016, 23, 189–195. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Respiratory Syncytial Virus (RSV) Disease. Available online: https://www.who.int/teams/health-product-policy-and-standards/standards-and-specifications/vaccine-standardization/respiratory-syncytial-virus-disease (accessed on 13 August 2023).
- European Medicines Agency (EMA). New Medicine to Protect Babies and Infants from Respiratory Syncytial Virus (RSV) Infection. 2022. Available online: https://www.ema.europa.eu/en/news/new-medicine-protect-babies-infants-respiratory-syncytial-virus-rsv-infection (accessed on 10 August 2023).
- European Medicines Agency (EMA). First Vaccine to Protect Older Adults from Respiratory Syncytial Virus (RSV) Infection. 2023. Available online: https://www.ema.europa.eu/en/news/first-vaccine-protect-older-adults-respiratory-syncytial-virus-rsv-infection#:~:text=EMA%20has%20recommended%20a%20marketing,respiratory%20syncytial%20virus%20(RSV) (accessed on 10 August 2023).
- U.S. Food and Drug Administration (FDA). FDA Approves First Respiratory Syncytial Virus (RSV) Vaccine. 2023. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-respiratory-syncytial-virus-rsv-vaccine (accessed on 12 August 2023).
- U.S. Food and Drug Administration (FDA). FDA Approves First Oral Antiviral for Treatment of COVID-19 in Adults. 2023. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-oral-antiviral-treatment-covid-19-adults#:~:text=Today%2C%20the%20U.S.%20Food%20and,19%2C%20including%20hospitalization%20or%20death (accessed on 12 August 2023).
- European Medicine Agency (EMA). Paxlovid Received Conditional Marketing Authorization. 2023. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/paxlovid#:~:text=Paxlovid%20received%20a%20conditional%20marketing,authorisation%20on%2024%20February%202023 (accessed on 10 August 2023).
- U.S. Food and Drug Administration (FDA). BLA Approval-ABRYSVO. Collegeville. May 2023. Available online: https://www.fda.gov/media/168890/download (accessed on 12 August 2023).
- U.S. Food and Drug Administration (FDA). Frequently Asked Questions on the Emergency Use Authorization for Paxlovid for Treatment of COVID-19. July 2023. Available online: https://www.fda.gov/media/155052/download (accessed on 12 August 2023).
- LaRotta, J.; Escobar, O.; Ávila-Aguero, M.L.; Torres, J.P.; Sini de Almeida, R.; del Carmen Morales, G.; Srivastava, A. COVID-19 in Latin America: A Snapshot in Time and the Road Ahead. Infect. Dis. Ther. 2023, 12, 389–410. [Google Scholar] [CrossRef]
- Public Health England. PHE Novel Coronavirus Diagnostic Test Rolled Out across UK. Government UK. 2020. Available online: https://www.gov.uk/government/news/phe-novel-coronavirus-diagnostic-test-rolled-out-across-uk (accessed on 13 August 2023).
- European Medicines Agency (EMA). Pandemic Influenza A(H1N1)v Vaccines Authorised via the Core Dossier Procedure Explanatory Note on Scientific Considerations Regarding the Licensing of Pandemic A(H1N1)v Vaccines; EMA: London, UK, 2009. Available online: https://www.ema.europa.eu/en/documents/medicine-qa/explanatory-note-scientific-considerations-regarding-licensing-pandemic-ah1n1v-vaccines_en.pdf (accessed on 10 August 2023).
- Simoes, E.A.F.; Groothius, J.R. Respiratory Syncytial Virus Prophylaxis—The Story so Far. Respir. Med. 2002, 96, S15–S24. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug Administration. FDA Approves New Drug to Prevent RSV in Babies and Toddlers. 2023. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-prevent-rsv-babies-and-toddlers (accessed on 10 August 2023).
- Malik, B.; Ghatol, A. Understanding How Monoclonal Antibodies Work. 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK572118/ (accessed on 13 August 2023).
- Mejias, A.; Rodríguez-Fernández, R.; Oliva, S.; Peeples, M.E.; Ramilo, O. The Journey to a Respiratory Syncytial Virus Vaccine. Ann. Allergy Asthma Immunol. 2020, 125, 36–46. [Google Scholar] [CrossRef]
- United Nations. COVID-19: With Booster Doses, Tests and Preparation, We Could End the Pandemic This Year (Translated from Spanish: COVID-19: Con Dosis de Refuerzo, Pruebas y Preparación, Podemos Poner Fin a La Pandemia Este Año). UN News. 2022. Available online: https://news.un.org/es/story/2022/09/1515191 (accessed on 13 August 2023).
- Klobucista, C.; Ferragamo, M. When Will COVID-19 Become Endemic? Council on Foreign Relations. 2023. Available online: https://www.cfr.org/in-brief/when-will-covid-19-become-endemic (accessed on 10 August 2023).
- Carabelli, A.M.; Peacock, T.P.; Thorne, L.G.; Harvey, W.T.; Hughes, J.; de Silva, T.I.; Peacock, S.J.; Barclay, W.S.; de Silva, T.I.; Towers, G.J.; et al. SARS-CoV-2 Variant Biology: Immune Escape, Transmission and Fitness. Nat. Rev. Microbiol. 2023, 21, 162–177. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Introduction to Epidemiology. 2018. Available online: https://www.cdc.gov/training/publichealth101/epidemiology.html (accessed on 10 August 2023).
- Antia, R.; Halloran, M.E. Transition to Endemicity: Understanding COVID-19. Immunity 2021, 54, 2172–2176. [Google Scholar] [CrossRef]
- Siggins, M.K.; Thwaites, R.S.; Openshaw, P.J.M. Durability of Immunity to SARS-CoV-2 and Other Respiratory Viruses. Trends Microbiol. 2021, 29, 648–662. [Google Scholar] [CrossRef]
- Mendoza, R.U.; Hartigan-Go, K.Y.; Brillantes, A.B.; Ruiz, K.E.V.; Baysic, I.S.; Valenzuela, S.A. Public Policy (Not the Coronavirus) Should Shape What Endemic Means. J. Glob. Health 2022, 12, 03050. [Google Scholar] [CrossRef] [PubMed]
- Biancolella, M.; Colona, V.L.; Mehrian-Shai, R.; Watt, J.L.; Luzzatto, L.; Novelli, G.; Reichardt, J.K.V. COVID-19 2022 Update: Transition of the Pandemic to the Endemic Phase. Hum. Genom. 2022, 16, 19. [Google Scholar] [CrossRef] [PubMed]
- Potter, S. When COVID-19 Is Endemic, What’s the Role of Testing? PBS Wisconsin, 2022. Available online: https://pbswisconsin.org/news-item/when-covid-19-is-endemic-whats-the-role-of-testing/(accessed on 13 August 2023).
- Centers for Disease Control and Prevention (CDC). Overview of COVID-19 Vaccines. 2023. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/overview-COVID-19-vaccines.html (accessed on 10 August 2023).
- European Medicines Agency (EMA). COVID-19 Medicines. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/covid-19-medicines (accessed on 10 August 2023).
- U.S. Food and Drug Administration (FDA). Coronavirus Treatment Acceleration Program (CTAP). 2023. Available online: https://www.fda.gov/drugs/coronavirus-covid-19-drugs/coronavirus-treatment-acceleration-program-ctap (accessed on 12 August 2023).
- Administration for Strategic Preparedness & Response (ASPR). What Are the Possible Treatment Options for COVID 19? US Department of Health and Human Services. Available online: https://aspr.hhs.gov/COVID-19/Treatments/Pages/Possible-Treatment-Options-for-COVID19.aspx#oral-antivirals (accessed on 13 August 2023).
- U.S. Food & Drug Administration (FDA). Coronavirus (COVID-19)|Drugs. 2023. Available online: https://www.fda.gov/drugs/emergency-preparedness-drugs/coronavirus-covid-19-drugs (accessed on 13 August 2023).
- Centers for Disease Control and Prevention (CDC). COVID-19 Treatments and Medications. 2023. Available online: https://www.cdc.gov/coronavirus/2019-ncov/your-health/treatments-for-severe-illness.html (accessed on 13 August 2023).
- European Medicines Agency (EMA). COVID-19 Medicines under Evaluation. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/covid-19-medicines/covid-19-medicines-under-evaluation (accessed on 13 August 2023).
- Centers for Disease Control and Prevention (CDC). Seasonal Flu Vaccines. 2022. Available online: https://www.cdc.gov/flu/prevent/flushot.htm#:~:text=Several%20different%20brands%20of%20standard,(muscle)%20with%20a%20needle (accessed on 13 August 2023).
- European Medicines Agency (EMA). Pandemic Influenza. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/pandemic-influenza (accessed on 10 August 2023).
- European Medicines Agency (EMA). Antiviral Medicines for Pandemic Influenza. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/pandemic-influenza/antiviral-medicines-pandemic-influenza (accessed on 10 August 2023).
- Pizzorno, A.; Padey, B.; Terrier, O.; Rosa-Calatrava, M. Drug Repurposing Approaches for the Treatment of Influenza Viral Infection: Reviving Old Drugs to Fight Against a Long-Lived Enemy. Front. Immunol. 2019, 10, 531. [Google Scholar] [CrossRef] [PubMed]
- Sarker, A.; Gu, Z.; Mao, L.; Ge, Y.; Hou, D.; Fang, J.; Wei, Z.; Wang, Z. Influenza-Existing Drugs and Treatment Prospects. Eur. J. Med. Chem. 2022, 232, 114189. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration (FDA). Influenza (Flu) Antiviral Drugs and Related Information. 2022. Available online: https://www.fda.gov/drugs/information-drug-class/influenza-flu-antiviral-drugs-and-related-information#:~:text=There%20are%20four%20FDA%2Dapproved,against%20recently%20circulating%20influenza%20viruses.&text=Two%20older%20drugs%2C%20amantadine%20(generic,of%20influenza%20A%20virus%20infection (accessed on 12 August 2023).
- Centers for Disease Control and Prevention (CDC). Influenza Antiviral Drug Resistance. Available online: https://www.cdc.gov/flu/treatment/antiviralresistance.htm (accessed on 10 August 2023).
- Lampejo, T. Influenza and Antiviral Resistance: An Overview. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1201–1208. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency (EMA). Abrysvo. 2023. Available online: https://www.ema.europa.eu/en/medicines/human/summaries-opinion/abrysvo (accessed on 12 August 2023).
- Tin, A. First RSV Vaccine to Protect Infants Wins Backing of FDA Panel. CBS News, 2023. Available online: https://www.cbsnews.com/news/fda-rsv-vaccine-to-protect-infants-pfizer/(accessed on 12 August 2023).
- World Health Organization (WHO). Annex 2 Guidelines on the Quality, Safety and Efficacy of Respiratory Syncytial virus Vaccines. 2020. Available online: https://cdn.who.int/media/docs/default-source/biologicals/vaccine-standardization/respiratory-syncytial-virus-(rsv)-vaccines/annex_2_rsv_vaccines_trs_1024.pdf?sfvrsn=5d7aefa7_3&download=true (accessed on 13 August 2023).
- PATH. RSV Vaccine and mAb Snapshot. 2023. Available online: https://www.path.org/resources/rsv-vaccine-and-mab-snapshot/ (accessed on 13 August 2023).
- Smyk, J.M.; Szydłowska, N.; Szulc, W.; Majewska, A. Evolution of Influenza Viruses—Drug Resistance, Treatment Options, and Prospects. Int. J. Mol. Sci. 2022, 23, 12244. [Google Scholar] [CrossRef] [PubMed]
- Hernández-González, D.G.; Rodríguez-Muñoz, L.; Solórzano-Santos, F. Impact of the Use of Multiplex PCR on Etiological Diagnosis and Treatment of Acute Respiratory Infections in a Private Hospital of the North of the Country. Gac. Med. Mex. 2021, 157, 160–165. [Google Scholar] [CrossRef]
- Havers, F.P.; Hicks, L.A.; Chung, J.R.; Gaglani, M.; Murthy, K.; Zimmerman, R.K.; Jackson, L.A.; Petrie, J.G.; McLean, H.Q.; Nowalk, M.P.; et al. Outpatient Antibiotic Prescribing for Acute Respiratory Infections During Influenza Seasons. JAMA Netw. Open 2018, 1, e180243. [Google Scholar] [CrossRef]
- Tonkin-Crine, S.; Yardley, L.; Little, P. Antibiotic Prescribing for Acute Respiratory Tract Infections in Primary Care: A Systematic Review and Meta-Ethnography. J. Antimicrob. Chemother. 2011, 66, 2215–2223. [Google Scholar] [CrossRef]
- Obolski, U.; Kassem, E.; Na’amnih, W.; Tannous, S.; Kagan, V.; Muhsen, K. Unnecessary Antibiotic Treatment of Children Hospitalised with Respiratory Syncytial Virus (RSV) Bronchiolitis: Risk Factors and Prescription Patterns. J. Glob. Antimicrob. Resist. 2021, 27, 303–308. [Google Scholar] [CrossRef]
- Allen, K.E.; Beekmann, S.E.; Polgreen, P.; Poser, S.; St. Pierre, J.; Santibañez, S.; Gerber, S.I.; Kim, L. Survey of Diagnostic Testing for Respiratory Syncytial Virus (RSV) in Adults: Infectious Disease Physician Practices and Implications for Burden Estimates. Diagn. Microbiol. Infect. Dis. 2018, 92, 206–209. [Google Scholar] [CrossRef] [PubMed]
- Egilmezer, E.; Walker, G.J.; Bakthavathsalam, P.; Peterson, J.R.; Gooding, J.J.; Rawlinson, W.; Stelzer-Braid, S. Systematic Review of the Impact of Point-of-Care Testing for Influenza on the Outcomes of Patients with Acute Respiratory Tract Infection. Rev. Med. Virol. 2018, 28, e1995. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. 2023. Available online: https://data.who.int/dashboards/covid19/deaths?n=c (accessed on 22 November 2023).
- Gamba, M.R.; LeBlanc, T.T.; Vázquez, D.; dos Santos, E.P.; Franco, O.H. Health Emergency Preparedness and Response Capacity in Latin America and the Caribbean. Am. J. Public Health 2022, 112, S572. [Google Scholar] [CrossRef] [PubMed]
- Our World in Data. Coronavirus (COVID-19) Deaths-Cumulative Confirmed COVID-19 Cases per Million People. 2023. Available online: https://ourworldindata.org/covid-deaths#explore-the-global-data-on-confirmed-covid-19-deaths (accessed on 24 November 2023).
- Organisation for Economic Cooperation and Development; The World Bank. Health at a Glance: Latin America and the Caribbean; OECD Publishing: Paris, France, 2023. [Google Scholar] [CrossRef]
- Pan American Health Organization (PAHO). PAHO Biweekly COVID-19 Epidemiological Update—31st May 2023; PAHO: Washington, DC, USA, 2023; Available online: https://www.paho.org/en/documents/paho-biweekly-covid-19-epidemiological-update-31st-may-2023 (accessed on 13 August 2023).
- Our World in Data. Cumulative COVID-19 Tests per 1000 People. 2023. Available online: https://ourworldindata.org/covid-deaths#explore-the-global-data-on-confirmed-covid-19-deaths (accessed on 24 November 2023).
- Our World in Data. Tests Conducted per Confirmed Case of COVID-19, 7-Day Rolling Average. 2023. Available online: https://ourworldindata.org/coronavirus-testing (accessed on 24 November 2023).
- Our World in Data. Excess Mortality: Cumulative Deaths from All Causes Compared to Projection Based on Previous Years. 2023. Available online: https://ourworldindata.org/covid-deaths#explore-the-global-data-on-confirmed-covid-19-deaths (accessed on 24 November 2023).
- Our World in Data. The Our World in Data COVID-19 Testing Dataset: Source Information Country by Country. 2023. Available online: https://ourworldindata.org/coronavirus-testing (accessed on 24 November 2023).
- Garcia, J.; Torres, C.; Castro, A.; Rousset Yepez, B. The Registration of COVID-19 Associated Deaths: Who Is Included in the Statistics? ALAP (Asociación Latinoamericana de Población): Rio de Janeiro, Brazil, 2021; Available online: https://archined.ined.fr/view/AX3H6p8-Qw0312HDrH9d (accessed on 13 August 2023).
- Binstock, G.; Nathan, M.; Pardo, I.; Peláez, E. Challegens for the Advance of the 2030 Agenda in the Latin America and the Caribbean in the Gramework of COVID-19 (Translated from Spanish: Desafíos Para El Avance de La Agenda 2030 En América Latina y El Caribe En El Marco de La COVID-19); ALAP (Asociación Latinoamericana de Población): Rio de Janeiro, Brazil, 2021; Available online: https://lac.unfpa.org/es/publications/desaf%C3%ADos-para-el-avance-de-la-agenda-2030-en-am%C3%A9rica-latina-y-el-caribe-en-el-marco-de (accessed on 13 August 2023).
- Pan American Health Organization (PAHO). International Guideline for the Certification and Classification (Coding) of COVID-19 as a Cause of Death, April 20th, 2020. (Translated from Spanish: Orientación Internacional Para La Certificación y Clasificación (Codificación) del COVID-19 Como Causa de Muerte, 20 de Abril de 2020); PAHO: Washington, DC, USA, 2020; Available online: https://iris.paho.org/handle/10665.2/52848 (accessed on 13 August 2023).
- National Health Institute (INS) Colombia. ABC of the Mortality Registry by COVID in Colombia (Translated from Spanish: ABECÉ del Registro de Mortalidad Por COVID En Colombia); National Health Institute (INS) Colombia: Bogota, Colombia, 2023. Available online: https://www.ins.gov.co/BibliotecaDigital/abece-Registro-mortalidad-Covid.pdf (accessed on 12 August 2023).
- Ministry of Health Argentina. COVID-19 Disease. Guide for the Codification of Death Causes. (Translated from Spanish: Enfermedad Por COVID-19 Guía para la Codificación de Las Causas de Muerte); Ministry of Health Argentina: Buenos Aires, Argentina, 2020. Available online: https://www.argentina.gob.ar/sites/default/files/certifdef_covid19_cace_2.pdf (accessed on 13 August 2023).
- Health Secretariat Mexico. Standarized Guideline for the Epidemiological and Laboratory Surveillance of Viral Respiratory Disease (Translated from Spanish: Lineamiento Estandarizado Para La Vigilancia Epidemiológica y Por Laboratorio de La Enfermedad Respiratoria Viral); Health Secretariat Mexico: Mexico City, Mexico, 2022. Available online: https://www.gob.mx/cms/uploads/attachment/file/715444/Lineamiento_VE_y_Lab_Enf_Viral_05042022.pdf (accessed on 13 August 2023).
- Advisory Council COVID-19 Ministry of Health Chile. Surveillance, Registry and Death Certificates during the COVID-19 Pandemic (Translated from Spanish: Vigilancia, Registro y Certificación de Defunciones Durante La Pandemia de COVID-19); Advisory Council COVID-19 Ministry of Health Chile: Santiago, Chile, 2020; Available online: https://ciperchile.cl/wp-content/uploads/Minuta-Vigilancia-y-registro-de-defunciones-durante-la-pandemia-de-COVID-19_12-Junio.pdf (accessed on 13 August 2023).
- Brazil Civil Registry. Deaths with Suspicion or Confirmation of COVID-19 by Sex and Age (Translated from Portuguese: Óbitos com Suspeita ou Confirmação de COVID-19 por Sexo e Faixa etária). Transparency Portal Brazil. 2020. Available online: https://transparencia.registrocivil.org.br/especial-covid (accessed on 13 August 2023).
- Bonacina, F.; Boëlle, P.-Y.; Colizza, V.; Lopez, O.; Thomas, M.; Poletto, C. Global Patterns and Drivers of Influenza Decline during the COVID-19 Pandemic. Int. J. Infect. Dis. 2023, 128, 132–139. [Google Scholar] [CrossRef]
- Achangwa, C.; Park, H.; Ryu, S.; Lee, M.-S. Collateral Impact of Public Health and Social Measures on Respiratory Virus Activity during the COVID-19 Pandemic 2020–2021. Viruses 2022, 14, 1071. [Google Scholar] [CrossRef] [PubMed]
- Olsen, S.J.; Azziz-Baumgartner, E.; Budd, A.P.; Brammer, L.; Sullivan, S.; Pineda, R.F.; Cohen, C.; Fry, A.M. Decreased Influenza Activity During the COVID-19 Pandemic—United States, Australia, Chile, and South Africa, 2020. MMWR Morb. Mortal. Wkly Rep. 2020, 69, 1305–1309. [Google Scholar] [CrossRef]
- Chuang, Y.-C.; Lin, K.-P.; Wang, L.-A.; Yeh, T.-K.; Liu, P.-Y. The Impact of the COVID-19 Pandemic on Respiratory Syncytial Virus Infection: A Narrative Review. Infect. Drug Resist. 2023, 16, 661–675. [Google Scholar] [CrossRef]
- Sabeena, S.; Ravishankar, N.; Robin, S. The Impact of COVID-19 Pandemic on Influenza Surveillance: A Systematic Review and Meta-Analysis. Indian J. Public Health 2022, 66, 458. [Google Scholar] [CrossRef]
- Bermúdez Barrezueta, L.; Gutiérrez Zamorano, M.; López-Casillas, P.; Brezmes-Raposo, M.; Sanz Fernández, I.; Pino Vázquez, M.d.l.A. Influence of the COVID-19 Pandemic on the Epidemiology of Acute Bronchiolitis. Enferm. Infecc. Microbiol. Clin. 2023, 41, 348–351. [Google Scholar] [CrossRef]
- Nickbakhsh, S.; Mair, C.; Matthews, L.; Reeve, R.; Johnson, P.C.D.; Thorburn, F.; von Wissmann, B.; Reynolds, A.; McMenamin, J.; Gunson, R.N.; et al. Virus–Virus Interactions Impact the Population Dynamics of Influenza and the Common Cold. Proc. Natl. Acad. Sci. USA 2019, 116, 27142–27150. [Google Scholar] [CrossRef] [PubMed]
- Savy, V.; Ciapponi, A.; Bardach, A.; Glujovsky, D.; Aruj, P.; Mazzoni, A.; Gibbons, L.; Ortega-Barría, E.; Colindres, R.E. Burden of Influenza in Latin America and the Caribbean: A Systematic Review and Meta-Analysis. Influenza Other Respir. Viruses 2013, 7, 1017–1032. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Lopardo, G.; Scarpellini, B.; Stein, R.T.; Ribeiro, D. Systematic Review on Respiratory Syncytial Virus Epidemiology in Adults and the Elderly in Latin America. Int. J. Infect. Dis. 2020, 90, 170–180. [Google Scholar] [CrossRef] [PubMed]
- Bardach, A.; Rey-Ares, L.; Cafferata, M.L.; Cormick, G.; Romano, M.; Ruvinsky, S.; Savy, V. Systematic Review and Meta-Analysis of Respiratory Syncytial Virus Infection Epidemiology in Latin America. Rev. Med. Virol. 2014, 24, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Gupta, T.; Gupta, N. Global Respiratory Virus Surveillance: Strengths, Gaps, and Way Forward. Int. J. Infect. Dis. 2022, 121, 184–189. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). History of the Influenza Vaccine. Available online: https://www.who.int/news-room/spotlight/history-of-vaccination/history-of-influenza-vaccination (accessed on 12 August 2023).
- World Health Organization (WHO). Global Influenza Surveillance and Response System (GISRS). 2023. Available online: https://www.who.int/initiatives/global-influenza-surveillance-and-response-system (accessed on 13 August 2023).
- Barberis, I.; Martini, M.; Iavarone, F.; Orsi, A. Available Influenza Vaccines: Immunization Strategies, History and New Tools for Fighting the Disease. J. Prev. Med. Hyg. 2016, 57, E41–E46. [Google Scholar] [PubMed]
- Pebody, R.; Moyes, J.; Hirve, S.; Campbell, H.; Jackson, S.; Moen, A.; Nair, H.; Simões, E.A.F.; Smith, P.G.; Wairagkar, N.; et al. Approaches to Use the WHO Respiratory Syncytial Virus Surveillance Platform to Estimate Disease Burden. Influenza Other Respir. Viruses 2020, 14, 615–621. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Influenza Programme-WHO Launches Phase II of the Global Respiratory Syncytial Virus Surveillance; WHO: Geneva, Switzerland, 2022; Available online: https://www.who.int/teams/global-influenza-programme/global-respiratory-syncytial-virus-surveillance#:~:text=WHO%20launches%20phase%20II%20of%20the%20Global%20Respiratory%20Syncytial%20Virus%20Surveillance&text=(d)%20generate%20a%20robust%20understanding,representation%20in%20all%20WHO%20Regions (accessed on 13 August 2023).
- Pan American Health Organization (PAHO). Influenza and Other Respiratory Viruses: Surveillance in the Americas 2021; PAHO: Washington, DC, USA, 2022; Available online: https://iris.paho.org/bitstream/handle/10665.2/56544/9789275124994_eng.pdf?sequence=3&isAllowed=y (accessed on 13 August 2023).
- Broor, S.; Campbell, H.; Hirve, S.; Hague, S.; Jackson, S.; Moen, A.; Nair, H.; Palekar, R.; Rajatonirina, S.; Smith, P.G.; et al. Leveraging the Global Influenza Surveillance and Response System for Global Respiratory Syncytial Virus Surveillance—Opportunities and Challenges. Influenza Other Respir. Viruses 2020, 14, 622–629. [Google Scholar] [CrossRef]
- Sah, R.; Zaman, K.; Mohanty, A.; Al-Ahdal, T.; Awad, H.; Padhi, B.K.; Bhargava, A. Respiratory Syncytial Virus with Ongoing COVID-19: Is It an Emerging Threat? Ann. Med. Surg. 2023, 85, 67–70. [Google Scholar] [CrossRef]
- Pan American Health Organization (PAHO). FluNet Home Page 2010–2023. 2023. Available online: https://ais.paho.org/phip/viz/ed_flu.asp (accessed on 13 August 2023).
- Institute for health and metrics and evaluation (IHME). Global Disease Burden-Respiratory Infections. 2019. Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 12 August 2023).
- Pan American Health Organization (PAHO) FluNet. Cumulative Percent Positivity for Flu, RSV, and SARS-CoV-2, for 2022 by Country. 2023. Available online: https://ais.paho.org/phip/viz/ed_flu.asp (accessed on 13 August 2023).
- Dowdy, D.; D’Souza, G. COVID-19 Testing: Understanding the “Percent Positive”. Available online: https://publichealth.jhu.edu/2020/covid-19-testing-understanding-the-percent-positive#:~:text=The%20percent%20positive%20will%20be,haven’t%20been%20tested%20yet (accessed on 12 August 2023).
- Centers for Disease Control and Prevention (CDC). About Multisystem Inflammatory Syndrome (MIS). 2023. Available online: https://www.cdc.gov/mis/about.html (accessed on 10 August 2023).
- Sakhamuri, S.M.; Jankie, S.; Pinto Pereira, L.M. Calling on Latin America and the Caribbean Countries to Recognise the Disability from Long COVID. Lancet Reg. Health-Am. 2022, 15, 100362. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Moreno, C.A.; Pineda, J.; Bareño, A.; Espitia, R.; Rengifo, P. Long COVID-19 in Latin America: Low Prevalence, High Resilience or Low Surveillance and Difficulties Accessing Health Care? Travel Med. Infect. Dis. 2023, 51, 102492. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Lopez-Echeverri, M.C.; Perez-Raga, M.F.; Quintero-Romero, V.; Valencia-Gallego, V.; Galindo-Herrera, N.; López-Alzate, S.; Sánchez-Vinasco, J.D.; Gutiérrez-Vargas, J.J.; Mayta-Tristan, P.; et al. The Global Challenges of the Long COVID-19 in Adults and Children. Travel Med. Infect. Dis. 2023, 54, 102606. [Google Scholar] [CrossRef] [PubMed]
- The World Bank Group, United Nations Development Programme (UNDP). Long COVID: The Extended Effects of the Pandemic on Labor Markets in Latin America and the Caribbean. 2022. Available online: https://documents1.worldbank.org/curated/en/099900007072289098/pdf/P1758390cd83e707b0845f0450936b8882b.pdf (accessed on 13 August 2023).
- Angarita-Fonseca, A.; Torres-Castro, R.; Benavides-Cordoba, V.; Chero, S.; Morales-Satán, M.; Hernández-López, B.; Salazar-Pérez, R.; Larrateguy, S.; Sanchez-Ramirez, D.C. Exploring Long COVID Condition in Latin America: Its Impact on Patients’ Activities and Associated Healthcare Use. Front. Med. 2023, 10, 1168628. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, E.; Bonadies, L.; Manzoni, P. Evidence on the Link between Respiratory Syncytial Virus Infection in Early Life and Chronic Obstructive Lung Diseases. Am. J. Perinatol. 2020, 37, S26–S30. [Google Scholar] [CrossRef]
- Verwey, C.; Nunes, M.C.; Dangor, Z.; Madhi, S.A. Pulmonary Function Sequelae after Respiratory Syncytial Virus Lower Respiratory Tract Infection in Children: A Systematic Review. Pediatr. Pulmonol. 2020, 55, 1567–1583. [Google Scholar] [CrossRef]
- The World Bank COVID-19. (Coronavirus) Response-The World Bank in Latin America and the Caribbean. Available online: https://www.worldbank.org/en/region/lac/coronavirus (accessed on 13 August 2023).
- Congressional Research Service. Latin America and the Caribbean: Impact of COVID-19; Congressional Research Service: Washington, DC, USA, 2022. Available online: https://sgp.fas.org/crs/row/IF11581.pdf (accessed on 10 August 2023).
- Organisation for Economic Co-Operation and Development (OECD). OECD Policy Responses to Coronavirus (COVID-19) COVID-19 in Latin America and the Caribbean: Regional Socio-Economic Implications and Policy Priorities; OECD: Paris, France, 2020; Available online: https://www.oecd.org/coronavirus/policy-responses/covid-19-in-latin-america-and-the-caribbean-regional-socio-economic-implications-and-policy-priorities-93a64fde/ (accessed on 13 August 2023).
- Economic Commission for Latin America and the Caribbean (ECLAC). The Sociodemographic Impacts of the COVID-19 Pandemic in Latin America and the Caribbean; ECLAC: Santiago, Chile, 2022; Available online: https://www.cepal.org/en/publications/47923-sociodemographic-impacts-covid-19-pandemic-latin-america-and-caribbean (accessed on 13 August 2023).
- Mosegui, G.B.G.; Antoñanzas, F.; de Mello Vianna, C.M. Cost of Lost Productivity from Acute Respiratory Infections in South America. Rev. Panam. De Salud Pública 2023, 47, 1. [Google Scholar] [CrossRef]
- Economic Commission for Latin America and the Caribbean (ECLAC). Preliminary Evaluation of the Impact of the Influenza H1N1-Document Developed by the Team of ECLAC-PAHO-WHO, as a Request and with the Support of the Government of Mexico (Translated from Spanish: Evaluación Preliminar Del Impacto En México de La Influenza AH1N1, Documento Elaborado Por El Equipo Conjunto CEPAL/OPS-OMS a Solicitud y Con El Apoyo Del Gobierno de México; ECLAC: Santiago, Chile, 2010; Available online: https://www.cepal.org/pt-br/node/19750 (accessed on 13 August 2023).
- Sachs, J.D.; Karim, S.S.A.; Aknin, L.; Allen, J.; Brosbøl, K.; Colombo, F.; Barron, G.C.; Espinosa, M.F.; Gaspar, V.; Gaviria, A.; et al. The Lancet Commission on Lessons for the Future from the COVID-19 Pandemic. Lancet 2022, 400, 1224–1280. [Google Scholar] [CrossRef] [PubMed]
- Cid, C.; Marinho, M.L. Two Years of the COVID-19 Pandemic in Latin America and the Caribbean (Translated from Spanish: Dos Años de Pandemia de COVID-19 En América Latina y El Caribe); Comisión Económica para América Latina y el Caribe: Santiago, Chile, 2022; Available online: https://www.cepal.org/es/publicaciones/47914-anos-pandemia-covid-19-america-latina-caribe-reflexiones-avanzar-sistemas-salud (accessed on 13 August 2023).
- Fisher, D.; Suri, S.; Carson, G. What Comes next in the COVID-19 Pandemic? Lancet 2022, 399, 1691–1692. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization (PAHO). Advancing towards Universal Health in Latin America and the Caribbean: Lessons from the COVID-19 Pandemic. 2022. Available online: https://www.paho.org/en/stories/advancing-towards-universal-health-latin-america-and-caribbean-lessons-covid-19-pandemic (accessed on 13 August 2023).
- Kruse, M.H.; Durstine, A.; Evans, D.P. Effect of COVID-19 on Patient Access to Health Services for Noncommunicable Diseases in Latin America: A Perspective from Patient Advocacy Organizations. Int. J. Equity Health 2022, 21, 45. [Google Scholar] [CrossRef]
- United Nations. Development Programme (UNDP); World Bank an Inequal Recovery: Taking Pulse of Latin America and the Caribbean after the Pandemic (Translated from Spanish: Una Recuperación Desigual: Tomando El Pulso de América Latina y El Caribe Después de La Pandemia). Available online: https://www.undp.org/sites/g/files/zskgke326/files/migration/latinamerica/55c219b7a3249badb633859cc85fd94f4b2c7be80af62137d5be4d22a9a3378f.pdf (accessed on 13 August 2023).
- Gallegos, M.; Consoli, A.; Ferrari, I.F.; Cervigni, M.; de Castro, V.; Martino, P.; Caycho, T.; Razumovskiy, A. COVID-19: Psychosocial Impact and Mental Health in Latin America. Fractal (Niterói) 2022, 33, 226–232. [Google Scholar] [CrossRef]
- Zhang, S.X.; Batra, K.; Xu, W.; Liu, T.; Dong, R.K.; Yin, A.; Delios, A.Y.; Chen, B.Z.; Chen, R.Z.; Miller, S.; et al. Mental Disorder Symptoms during the COVID-19 Pandemic in Latin America—A Systematic Review and Meta-Analysis. Epidemiol. Psychiatr. Sci. 2022, 31, e23. [Google Scholar] [CrossRef] [PubMed]
- Otoo, J.A.; Schlappi, T.S. REASSURED Multiplex Diagnostics: A Critical Review and Forecast. Biosensors 2022, 12, 124. [Google Scholar] [CrossRef] [PubMed]
- Domnich, A.; Bruzzone, B.; Trombetta, C.-S.; De Pace, V.; Ricucci, V.; Varesano, S.; Garzillo, G.; Ogliastro, M.; Orsi, A.; Icardi, G. Rapid Differential Diagnosis of SARS-CoV-2, Influenza A/B and Respiratory Syncytial Viruses: Validation of a Novel RT-PCR Assay. J. Clin. Virol. 2023, 161, 105402. [Google Scholar] [CrossRef] [PubMed]
- Khorramdelazad, H.; Kazemi, M.H.; Najafi, A.; Keykhaee, M.; Zolfaghari Emameh, R.; Falak, R. Immunopathological Similarities between COVID-19 and Influenza: Investigating the Consequences of Co-Infection. Microb. Pathog. 2021, 152, 104554. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Testing for SARS-CoV-2 Infection and Immunity. 2021. Available online: https://www.who.int/docs/default-source/coronaviruse/1_diagnostic-testing_a40858ba4cdeb844218acf06d5cffffa8b.pdf?sfvrsn=8b8894bf_1 (accessed on 13 August 2023).
- Centers for Disease Control and Prevention (CDC). Nucleic Acid Amplification Tests (NAATs). 2023. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/naats.html (accessed on 10 August 2023).
- Yilmaz Gulec, E.; Cesur, N.P.; Yesilyurt Fazlioğlu, G.; Kazezoğlu, C. Effect of Different Storage Conditions on COVID-19 RT-PCR Results. J. Med. Virol. 2021, 93, 6575–6581. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, M.W.; Walsh, T.J. PCR Methodology and Applications for the Detection of Human Fungal Pathogens. Expert. Rev. Mol. Diagn. 2016, 16, 1025–1036. [Google Scholar] [CrossRef] [PubMed]
- Tabatabaei, M.S.; Islam, R.; Ahmed, M. Applications of Gold Nanoparticles in ELISA, PCR, and Immuno-PCR Assays: A Review. Anal. Chim. Acta 2021, 1143, 250–266. [Google Scholar] [CrossRef]
- Fakruddin, M.; Mannan, K.B.; Chowdhury, A.; Mazumdar, R.; Hossain, M.; Islam, S.; Chowdhury, M. Nucleic Acid Amplification: Alternative Methods of Polymerase Chain Reaction. J. Pharm. Bioallied Sci. 2013, 5, 245. [Google Scholar] [CrossRef]
- Obande, G.A.; Banga Singh, K.K. Current and Future Perspectives on Isothermal Nucleic Acid Amplification Technologies for Diagnosing Infections. Infect. Drug Resist. 2020, 13, 455–483. [Google Scholar] [CrossRef]
- Cao, S.; Tang, X.; Chen, T.; Chen, G. Types and Applications of Nicking Enzyme-Combined Isothermal Amplification. Int. J. Mol. Sci. 2022, 23, 4620. [Google Scholar] [CrossRef]
- Thompson, D.; Lei, Y. Mini Review: Recent Progress in RT-LAMP Enabled COVID-19 Detection. Sens. Actuators Rep. 2020, 2, 100017. [Google Scholar] [CrossRef]
- Amaral, C.; Antunes, W.; Moe, E.; Duarte, A.G.; Lima, L.M.P.; Santos, C.; Gomes, I.L.; Afonso, G.S.; Vieira, R.; Teles, H.S.S.; et al. A Molecular Test Based on RT-LAMP for Rapid, Sensitive and Inexpensive Colorimetric Detection of SARS-CoV-2 in Clinical Samples. Sci. Rep. 2021, 11, 16430. [Google Scholar] [CrossRef] [PubMed]
- Khan, P.; Aufdembrink, L.M.; Engelhart, A.E. Isothermal SARS-CoV-2 Diagnostics: Tools for Enabling Distributed Pandemic Testing as a Means of Supporting Safe Reopenings. ACS Synth. Biol. 2020, 9, 2861–2880. [Google Scholar] [CrossRef] [PubMed]
- Choi, G.; Moehling, T.J.; Meagher, R.J. Advances in RT-LAMP for COVID-19 Testing and Diagnosis. Expert. Rev. Mol. Diagn. 2023, 23, 9–28. [Google Scholar] [CrossRef]
- Huang, X.; Tang, G.; Ismail, N.; Wang, X. Developing RT-LAMP Assays for Rapid Diagnosis of SARS-CoV-2 in Saliva. EBioMedicine 2022, 75, 103736. [Google Scholar] [CrossRef]
- Yang, Q.; Meyerson, N.R.; Clark, S.K.; Paige, C.L.; Fattor, W.T.; Gilchrist, A.R.; Barbachano-Guerrero, A.; Healy, B.G.; Worden-Sapper, E.R.; Wu, S.S.; et al. Saliva TwoStep for Rapid Detection of Asymptomatic SARS-CoV-2 Carriers. medRxiv 2021. [Google Scholar] [CrossRef]
- Uribe-Alvarez, C.; Lam, Q.; Baldwin, D.A.; Chernoff, J. Low Saliva PH Can Yield False Positives Results in Simple RT-LAMP-Based SARS-CoV-2 Diagnostic Tests. PLoS ONE 2021, 16, e0250202. [Google Scholar] [CrossRef]
- Dao Thi, V.L.; Herbst, K.; Boerner, K.; Meurer, M.; Kremer, L.P.; Kirrmaier, D.; Freistaedter, A.; Papagiannidis, D.; Galmozzi, C.; Stanifer, M.L.; et al. A Colorimetric RT-LAMP Assay and LAMP-Sequencing for Detecting SARS-CoV-2 RNA in Clinical Samples. Sci. Transl. Med. 2020, 12, eabc7075. [Google Scholar] [CrossRef] [PubMed]
- Kellner, M.J.; Ross, J.J.; Schnabl, J.; Dekens, M.P.S.; Matl, M.; Heinen, R.; Grishkovskaya, I.; Bauer, B.; Stadlmann, J.; Menéndez-Arias, L.; et al. A Rapid, Highly Sensitive and Open-Access SARS-CoV-2 Detection Assay for Laboratory and Home Testing. Front. Mol. Biosci. 2022, 9, 801309. [Google Scholar] [CrossRef]
- Haque, M.F.U.; Bukhari, S.S.; Ejaz, R.; Zaman, F.U.; Sreejith, K.R.; Rashid, N.; Umer, M.; Shahzad, N. A Novel RdRp-Based Colorimetric RT-LAMP Assay for Rapid and Sensitive Detection of SARS-CoV-2 in Clinical and Sewage Samples from Pakistan. Virus Res. 2021, 302, 198484. [Google Scholar] [CrossRef]
- He, Y.; Xie, T.; Tong, Y. Rapid and Highly Sensitive One-Tube Colorimetric RT-LAMP Assay for Visual Detection of SARS-CoV-2 RNA. Biosens. Bioelectron. 2021, 187, 113330. [Google Scholar] [CrossRef] [PubMed]
- Nie, S.; Roth, R.B.; Stiles, J.; Mikhlina, A.; Lu, X.; Tang, Y.-W.; Babady, N.E. Evaluation of Alere i Influenza A and B for Rapid Detection of Influenza Viruses A and B. J. Clin. Microbiol. 2014, 52, 3339–3344. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.-N.; Jiang, D.; Wang, X.; Liu, Y.; Wei, D. Recent Progress on Rapid Diagnosis of COVID-19 by Point-of-Care Testing Platforms. Chin. Chem. Lett. 2023, 108688. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Huang, Z.; Zhu, J.; Li, C.; Fang, Z.; Chen, K.; Zhang, Y. An Updated Review of SARS-CoV-2 Detection Methods in the Context of a Novel Coronavirus Pandemic. Bioeng. Transl. Med. 2023, 8, e10356. [Google Scholar] [CrossRef] [PubMed]
- James, A.; Alawneh, J. COVID-19 Infection Diagnosis: Potential Impact of Isothermal Amplification Technology to Reduce Community Transmission of SARS-CoV-2. Diagnostics 2020, 10, 399. [Google Scholar] [CrossRef] [PubMed]
- Rhoads, D.D.; Cherian, S.S.; Roman, K.; Stempak, L.M.; Schmotzer, C.L.; Sadri, N. Comparison of Abbott ID Now, DiaSorin Simplexa, and CDC FDA Emergency Use Authorization Methods for the Detection of SARS-CoV-2 from Nasopharyngeal and Nasal Swabs from Individuals Diagnosed with COVID-19. J. Clin. Microbiol. 2020, 58, e00760-20. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Zinger, T.; Inglima, K.; Woo, K.; Atie, O.; Yurasits, L.; See, B.; Aguero-Rosenfeld, M.E. Performance of Abbott ID Now COVID-19 Rapid Nucleic Acid Amplification Test Using Nasopharyngeal Swabs Transported in Viral Transport Media and Dry Nasal Swabs in a New York City Academic Institution. J. Clin. Microbiol. 2020, 58, e01136-20. [Google Scholar] [CrossRef]
- Roumani, F.; Azinheiro, S.; Sousa, H.; Sousa, A.; Timóteo, M.; Varandas, T.; Fonseca-Silva, D.; Baldaque, I.; Carvalho, J.; Prado, M.; et al. Optimization and Clinical Evaluation of a Multi-Target Loop-Mediated Isothermal Amplification Assay for the Detection of SARS-CoV-2 in Nasopharyngeal Samples. Viruses 2021, 13, 940. [Google Scholar] [CrossRef]
- Smithgall, M.C.; Scherberkova, I.; Whittier, S.; Green, D.A. Comparison of Cepheid Xpert Xpress and Abbott ID Now to Roche Cobas for the Rapid Detection of SARS-CoV-2. J. Clin. Virol. 2020, 128, 104428. [Google Scholar] [CrossRef]
- Chen, C.-C.; Chen, S.-Y.; Fang, S.-B.; Lu, S.-C.; Bai, C.-H.; Wang, Y.-H. Diagnostic Accuracy of SARS-CoV-2 Antigen Test in the Pediatric Population: A Systematic Review and Meta-Analysis. Pediatr. Neonatol. 2023, 64, 247–255. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection. Interim Guidance. 6 October 2021. Available online: https://apps.who.int/iris/rest/bitstreams/1376869/retrieve (accessed on 13 August 2023).
- Korenkov, M.; Poopalasingam, N.; Madler, M.; Vanshylla, K.; Eggeling, R.; Wirtz, M.; Fish, I.; Dewald, F.; Gieselmann, L.; Lehmann, C.; et al. Evaluation of a Rapid Antigen Test To Detect SARS-CoV-2 Infection and Identify Potentially Infectious Individuals. J. Clin. Microbiol. 2021, 59. [Google Scholar] [CrossRef]
- Dinnes, J.; Deeks, J.J.; Adriano, A.; Berhane, S.; Davenport, C.; Dittrich, S.; Emperador, D.; Takwoingi, Y.; Cunningham, J.; Beese, S.; et al. Rapid, Point-of-Care Antigen and Molecular-Based Tests for Diagnosis of SARS-CoV-2 Infection. Cochrane Database Syst. Rev. 2020, 8, CD013705. [Google Scholar] [CrossRef] [PubMed]
- Bekliz, M.; Adea, K.; Essaidi-Laziosi, M.; Sacks, J.A.; Escadafal, C.; Kaiser, L.; Eckerle, I. SARS-CoV-2 Rapid Diagnostic Tests for Emerging Variants. Lancet Microbe 2021, 2, e351. [Google Scholar] [CrossRef]
- Bekliz, M.; Adea, K.; Puhach, O.; Perez-Rodriguez, F.; Marques Melancia, S.; Baggio, S.; Corvaglia, A.-R.; Jacquerioz, F.; Alvarez, C.; Essaidi-Laziosi, M.; et al. Analytical Sensitivity of Eight Different SARS-CoV-2 Antigen-Detecting Rapid Tests for Omicron-BA.1 Variant. Microbiol. Spectr. 2022, 10, e00853-22. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Haage, V.C.; Bleicker, T.; Schmidt, M.L.; Mühlemann, B.; Zuchowski, M.; Jo, W.K.; Tscheak, P.; Möncke-Buchner, E.; Müller, M.A.; et al. Comparison of Seven Commercial SARS-CoV-2 Rapid Point-of-Care Antigen Tests: A Single-Centre Laboratory Evaluation Study. Lancet Microbe 2021, 2, e311–e319. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug Administration. SARS-CoV-2 Viral Mutations: Impact on COVID-19. Tests. Available online: https://www.fda.gov/medical-devices/coronavirus-covid-19-and-medical-devices/sars-cov-2-viral-mutations-impact-covid-19-tests (accessed on 28 January 2024).
- Stanley, S.; Hamel, D.J.; Wolf, I.D.; Riedel, S.; Dutta, S.; Contreras, E.; Callahan, C.J.; Cheng, A.; Arnaout, R.; Kirby, J.E.; et al. Limit of Detection for Rapid Antigen Testing of the SARS-CoV-2 Omicron and Delta Variants of Concern Using Live-Virus Culture. J. Clin. Microbiol. 2022, 60, e00140-22. [Google Scholar] [CrossRef]
- World Health Organization. Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection. Interim Guidance. Available online: https://www.who.int/publications/i/item/antigen-detection-in-the-diagnosis-of-sars-cov-2infection-using-rapid-immunoassays (accessed on 28 January 2024).
- Nasrallah, G.K.; Ali, F.; Younes, S.; Al Khatib, H.A.; Al-Thani, A.A.; Yassine, H.M. Enhancing the Sensitivity of Rapid Antigen Detection Test (RADT) of Different SARS-CoV-2 Variants and Lineages Using Fluorescence-Labeled Antibodies and a Fluorescent Meter. Heliyon 2023, 9, e17179. [Google Scholar] [CrossRef]
- Urusov, A.E.; Zherdev, A.V.; Dzantiev, B.B. Towards Lateral Flow Quantitative Assays: Detection Approaches. Biosensors 2019, 9, 89. [Google Scholar] [CrossRef]
- Lee, J.; Song, J.-U.; Shim, S.R. Comparing the Diagnostic Accuracy of Rapid Antigen Detection Tests to Real Time Polymerase Chain Reaction in the Diagnosis of SARS-CoV-2 Infection: A Systematic Review and Meta-Analysis. J. Clin. Virol. 2021, 144, 104985. [Google Scholar] [CrossRef]
- Platten, M.; Hoffmann, D.; Grosser, R.; Wisplinghoff, F.; Wisplinghoff, H.; Wiesmüller, G.; Schildgen, O.; Schildgen, V. SARS-CoV-2, CT-Values, and Infectivity—Conclusions to Be Drawn from Side Observations. Viruses 2021, 13, 1459. [Google Scholar] [CrossRef]
- Paul, G.; Plecko, T.; Sethi, S.; Schilling, T.; Wienand, O.; Jürgensen, J.S.; Menzel, C.U. Klinische Performance Eines Neuen SARS-CoV-2-Antigen-Tests in Der Notaufnahme Eines Maximalversorgers. Epidemiol. Bull. 2021, 3, 10–15. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Ending Isolation and Precautions for People with COVID-19: Interim Guidance. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/duration-isolation.html (accessed on 28 January 2024).
- Nicollete, D.R.P.; Benedetti, R.; Valença, B.A.; Kuniyoshi, K.K.; de Jesus, T.C.S.; Gevaerd, A.; Santiago, E.B.; de Almeida, B.M.M.; Júnior, S.R.R.; Figueredo, M.V.M. Enhancing a SARS-CoV-2 Nucleocapsid Antigen Test Sensitivity with Cost Efficient Strategy through a Cotton Intermembrane Insertion. Sci. Rep. 2023, 13, 4690. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Coronavirus Disease (COVID-19): Serology, Antibodies and Immunity. 2020. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-covid-19-serology (accessed on 13 August 2023).
- World Health Organization (WHO). “Solidarity II” Global Serologic Study for COVID-19. 2021. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/global-research-on-novel-coronavirus-2019-ncov/solidarity-2-global-serologic-study-for-covid-19 (accessed on 13 August 2023).
- World Health Organization (WHO). Population-Based Age-Stratified Seroepidemiological Investigation Protocol for COVID-19 Virus Infection; WHO: Geneva, Switzerland, 2020; Available online: https://apps.who.int/iris/bitstream/handle/10665/331656/WHO-2019-nCoV-Seroepidemiology-2020.1-eng.pdf?sequence=1&isAllowed=y (accessed on 13 August 2023).
- World Health Organization (WHO). Guidelines for the Clinical Management of Severe Illness from Influenza Virus Infections; WHO: Geneva, Switzerland, 2022; Available online: https://apps.who.int/iris/handle/10665/352453 (accessed on 13 August 2023).
- Centers for Disease Control and Prevention (CDC). Overview of Influenza Testing Methods. 2020. Available online: https://www.cdc.gov/flu/professionals/diagnosis/overview-testing-methods.htm (accessed on 10 August 2023).
- Vemula, S.; Zhao, J.; Liu, J.; Wang, X.; Biswas, S.; Hewlett, I. Current Approaches for Diagnosis of Influenza Virus Infections in Humans. Viruses 2016, 8, 96. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Recommendations Announced for Influenza Vaccine Composition for the 2023–2024 Northern Hemisphere Influenza Season. 2023. Available online: https://www.who.int/news/item/24-02-2023-recommendations-announced-for-influenza-vaccine-composition-for-the-2023-2024-northern-hemisphere-influenza-season (accessed on 13 August 2023).
- Testing. Respiratory Syncytial Virus (RSV) Testing. Testing. 2020. Available online: https://www.testing.com/tests/respiratory-syncytial-virus-rsv-testing/ (accessed on 13 August 2023).
- Shi, T.; McAllister, D.A.; O’Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, Regional, and National Disease Burden Estimates of Acute Lower Respiratory Infections Due to Respiratory Syncytial Virus in Young Children in 2015: A Systematic Review and Modelling Study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef]
- Ackerson, B.; Tseng, H.F.; Sy, L.S.; Solano, Z.; Slezak, J.; Luo, Y.; Fischetti, C.A.; Shinde, V. Severe Morbidity and Mortality Associated With Respiratory Syncytial Virus Versus Influenza Infection in Hospitalized Older Adults. Clin. Infect. Dis. 2019, 69, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Binder, W.; Thorsen, J.; Borczuk, P. RSV in Adult ED Patients: Do Emergency Providers Consider RSV as an Admission Diagnosis? Am. J. Emerg. Med. 2017, 35, 1162–1165. [Google Scholar] [CrossRef] [PubMed]
- Branche, A.R.; Falsey, A.R. Respiratory Syncytial Virus Infection in Older Adults: An Under-Recognized Problem. Drugs Aging 2015, 32, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.; Rha, B.; Abramson, J.S.; Anderson, L.J.; Byington, C.L.; Chen, G.L.; DeVincenzo, J.; Edwards, K.M.; Englund, J.A.; Falsey, A.R.; et al. Identifying Gaps in Respiratory Syncytial Virus Disease Epidemiology in the United States Prior to the Introduction of Vaccines. Clin. Infect. Dis. 2017, 65, 1020–1025. [Google Scholar] [CrossRef] [PubMed]
- Tran, P.T.; Nduaguba, S.O.; Diaby, V.; Choi, Y.; Winterstein, A.G. RSV Testing Practice and Positivity by Patient Demographics in the United States: Integrated Analyses of MarketScan and NREVSS Databases. BMC Infect. Dis. 2022, 22, 681. [Google Scholar] [CrossRef] [PubMed]
- Rha, B.; Curns, A.T.; Lively, J.Y.; Campbell, A.P.; Englund, J.A.; Boom, J.A.; Azimi, P.H.; Weinberg, G.A.; Staat, M.A.; Selvarangan, R.; et al. Respiratory Syncytial Virus–Associated Hospitalizations Among Young Children: 2015–2016. Pediatrics 2020, 146, e20193611. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Guidance for SARS-CoV-2 Rapid Testing Performed in Point-of-Care Settings. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/point-of-care-testing.html (accessed on 10 August 2023).
- Infectious Diseases Society of America (IDSA); Centers for Disease Control and Prevention (CDC). Diagnostics- Rapid Testing. 2023. Available online: https://www.idsociety.org/covid-19-real-time-learning-network/diagnostics/#/+/0/publishedDate_na_dt/desc/ (accessed on 12 August 2023).
- Peeling, R.W.; Heymann, D.L.; Teo, Y.-Y.; Garcia, P.J. Diagnostics for COVID-19: Moving from Pandemic Response to Control. Lancet 2022, 399, 757–768. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Rapid Influenza Diagnostic Tests. 2016. Available online: https://www.cdc.gov/flu/professionals/diagnosis/clinician_guidance_ridt.htm (accessed on 10 August 2023).
- Yin, N.; Van Nuffelen, M.; Bartiaux, M.; Préseau, T.; Roggen, I.; Delaunoy, S.; Mahadeb, B.; Dahma, H.; Busson, L.; Vandenberg, O.; et al. Clinical Impact of the Rapid Molecular Detection of RSV and Influenza A and B Viruses in the Emergency Department. PLoS ONE 2022, 17, e0274222. [Google Scholar] [CrossRef] [PubMed]
- Favresse, J.; Douxfils, J.; Henry, B.; Lippi, G.; Plebani, M. Clinical Chemistry and Laboratory Medicine Celebrates 60 Years—Narrative Review Devoted to the Contribution of the Journal to the Diagnosis of SARS-CoV-2. Clin. Chem. Lab. Med. (CCLM) 2023, 61, 811–821. [Google Scholar] [CrossRef] [PubMed]
- Girdwood, S.J.; Carmona, S.; Hannay, E.; Nichols, B. Cost-Effectiveness of SARS-CoV-2 Rapid Antigen Testing in Lowresource Settings. Top. Antivir. Med. 2021, 29, 269. [Google Scholar]
- Cedro, V.Q.M.; de Lima Gomes, S.; Simões, A.C.C.D.; do Valle Lovato Sverzut, T.; Bertti, K.C.X.; Tristão, M.T.; Cavalcanti, Y.W.; Câmara, J.V.F.; Pereira, A.C. Cost-Effectiveness Analysis of COVID-19 Tests in the Unified Health System. Cost. Eff. Resour. Alloc. 2023, 21, 64. [Google Scholar] [CrossRef] [PubMed]
- de Araújo, E.S.A.; Condursi, J.R.; Garmatter, L.P.L. Análise Econômica Da Incorporação Do Teste Rápido de Antígeno Para Covid-19 versus RT-PCR Como Estratégia de Diagnóstico de Pacientes Sintomáticos No Pronto Atendimento de Uma Operadora de Saúde Do Brasil. Braz. J. Infect. Dis. 2022, 26, 101781. [Google Scholar] [CrossRef]
- Diel, R.; Nienhaus, A. Point-of-Care COVID-19 Antigen Testing in German Emergency Rooms—A Cost-Benefit Analysis. Pulmonology 2022, 28, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Pighi, L.; Henry, B.M.; Mattiuzzi, C.; De Nitto, S.; Salvagno, G.L.; Lippi, G. Cost-Effectiveness Analysis of Different COVID-19 Screening Strategies Based on Rapid or Laboratory-Based SARS-CoV-2 Antigen Testing. Clin. Chem. Lab. Med. (CCLM) 2023, 61, e168–e171. [Google Scholar] [CrossRef]
- Bonnet, G.; Bimba, J.; Chavula, C.; Chifamba, H.N.; Divala, T.; Lescano, A.G.; Majam, M.; Mbo, D.; Suwantika, A.A.; Tovar, M.A.; et al. “We Usually See a Lot of Delay in Terms of Coming for or Seeking Care”: An Expert Consultation on COVID Testing and Care Pathways in Seven Low- and Middle-Income Countries. BMC Health Serv. Res. 2023, 23, 1288. [Google Scholar] [CrossRef]
- Bertram, M.Y.; Lauer, J.A.; De Joncheere, K.; Edejer, T.; Hutubessy, R.; Kieny, M.-P.; Hill, S.R. Cost–Effectiveness Thresholds: Pros and Cons. Bull. World Health Organ. 2016, 94, 925–930. [Google Scholar] [CrossRef]
- Stolberg-Stolberg, J.; Jacob, E.; Kuehn, J.; Hennies, M.; Hafezi, W.; Freistuehler, M.; Koeppe, J.; Friedrich, A.W.; Katthagen, J.C.; Raschke, M.J. COVID-19 Rapid Molecular Point-of-Care Testing Is Effective and Cost-Beneficial for the Acute Care of Trauma Patients. Eur. J. Trauma Emerg. Surg. 2023, 49, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Diel, R.; Nienhaus, A. Cost–Benefit of Real-Time Multiplex PCR Testing of SARS-CoV-2 in German Hospitals. Int. J. Env. Res. Public Health 2023, 20, 3447. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Li, H.; Tang, Y.; Yu, F.; Ma, C.; Zhang, H.; Pang, L.; Zhao, H.; Wang, L. Multiplex Tests for Respiratory Tract Infections: The Direct Utility of the FilmArray Respiratory Panel in Emergency Department. Can. Respir. J. 2020, 2020, 6014563. [Google Scholar] [CrossRef] [PubMed]
- El-Nawawy, A.A.; Antonios, M.A.; Tawfik, M.E.; Meheissen, M.A. Comparison of a Point-of-Care FilmArray Test to Standard-of-Care Microbiology Test in Diagnosis of Healthcare Associated Infections in a Tertiary Care Pediatric Intensive Care Unit. Antibiotics 2022, 11, 453. [Google Scholar] [CrossRef] [PubMed]
- Dincer, C.; Bruch, R.; Kling, A.; Dittrich, P.S.; Urban, G.A. Multiplexed Point-of-Care Testing—XPOCT. Trends Biotechnol. 2017, 35, 728–742. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Table 4. Multiplex Assays Authorized for Simultaneous Detection of Influenza Viruses and SARS-CoV-2 by FDA. 2020. Available online: https://www.cdc.gov/flu/professionals/diagnosis/table-flu-covid19-detection.html (accessed on 10 August 2023).
- Clark, T.W.; Lindsley, K.; Wigmosta, T.B.; Bhagat, A.; Hemmert, R.B.; Uyei, J.; Timbrook, T.T. Rapid Multiplex PCR for Respiratory Viruses Reduces Time to Result and Improves Clinical Care: Results of a Systematic Review and Meta-Analysis. J. Infect. 2023, 86, 462–475. [Google Scholar] [CrossRef] [PubMed]
- Boukli, N.; Flamand, C.; Chea, K.L.; Heng, L.; Keo, S.; Sour, K.; In, S.; Chhim, P.; Chhor, B.; Kruy, L.; et al. One Assay to Test Them All: Comparing Multiplex Assays for Expansion of Respiratory Virus Surveillance. Medrxiv 2023. [Google Scholar] [CrossRef]
- Kang, T.; Hyun Cha, J.; Kim, J.; Kim, K.J.; Nam, M.; Nam, M.H.; Kim, D.W.; Cho, Y.; Kyu Lee, C.; Gyu Yun, S. Evaluation of Multiplex Rapid Antigen Test for the Detection of SARS-CoV-2 and Influenza A/B in Respiratory Samples. 2023. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4351273 (accessed on 12 August 2023). [CrossRef]
- Nichols, J.H. Point-of-Care Testing. In Contemporary Practice in Clinical Chemistry; Elsevier: Amsterdam, The Netherlands, 2020; pp. 323–336. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Biological Risk Management for Point-of-Care Testing Sites. Available online: https://www.cdc.gov/csels/dls/point-of-care-testing.html (accessed on 13 August 2023).
- Valera, E.; Jankelow, A.; Lim, J.; Kindratenko, V.; Ganguli, A.; White, K.; Kumar, J.; Bashir, R. COVID-19 Point-of-Care Diagnostics: Present and Future. ACS Nano 2021, 15, 7899–7906. [Google Scholar] [CrossRef]
- Izadi, R.; Hatam, N.; Baberi, F.; Yousefzadeh, S.; Jafari, A. Economic Evaluation of Strategies against Coronavirus: A Systematic Review. Health Econ. Rev. 2023, 13, 18. [Google Scholar] [CrossRef]
- National Community Pharmacist Association (NCPA). Point-of-Care Testing (POCT). 2023. Available online: https://ncpa.org/point-care-testing-poct (accessed on 13 August 2023).
- American Society for Microbiology. Making Sense of Respiratory Viral Panel Results. 2020. Available online: https://asm.org/Articles/2020/March/Making-Sense-of-Respiratory-Viral-Panel-Results (accessed on 10 August 2023).
- Hanson, K.E.; Azar, M.M.; Banerjee, R.; Chou, A.; Colgrove, R.C.; Ginocchio, C.C.; Hayden, M.K.; Holodiny, M.; Jain, S.; Koo, S.; et al. Molecular Testing for Acute Respiratory Tract Infections: Clinical and Diagnostic Recommendations From the IDSA’s Diagnostics Committee. Clin. Infect. Dis. 2020, 71, 2744–2751. [Google Scholar] [CrossRef]
- Gentilotti, E.; De Nardo, P.; Cremonini, E.; Górska, A.; Mazzaferri, F.; Canziani, L.M.; Hellou, M.M.; Olchowski, Y.; Poran, I.; Leeflang, M.; et al. Diagnostic Accuracy of Point-of-Care Tests in Acute Community-Acquired Lower Respiratory Tract Infections. A Systematic Review and Meta-Analysis. Clin. Microbiol. Infect. 2022, 28, 13–22. [Google Scholar] [CrossRef]
- Antoñanzas, F.; Juárez-Castelló, C.A.; Rodríguez-Ibeas, R. Using Point-of-Care Diagnostic Testing for Improved Antibiotic Prescription: An Economic Model. Health Econ. Rev. 2021, 11, 29. [Google Scholar] [CrossRef]
- Hengel, B.; Causer, L.; Matthews, S.; Smith, K.; Andrewartha, K.; Badman, S.; Spaeth, B.; Tangey, A.; Cunningham, P.; Saha, A.; et al. A Decentralised Point-of-Care Testing Model to Address Inequities in the COVID-19 Response. Lancet Infect. Dis. 2021, 21, e183–e190. [Google Scholar] [CrossRef]
- Bouzid, D.; Casalino, E.; Mullaert, J.; Laurent, O.; Duval, X.; Lescure, F.X.; Peiffer Smadja, N.; Tubiana, S.; Armand Lefèvre, L.; Descamps, D.; et al. Added Value of Rapid Respiratory Syndromic Testing at Point of Care versus Central Laboratory Testing: A Controlled Clinical Trial. J. Antimicrob. Chemother. 2021, 76, iii20–iii27. [Google Scholar] [CrossRef] [PubMed]
- Levin-Reisman, I.; Brauner, A.; Ronin, I.; Balaban, N.Q. Epistasis between Antibiotic Tolerance, Persistence, and Resistance Mutations. Proc. Natl. Acad. Sci. USA 2019, 116, 14734–14739. [Google Scholar] [CrossRef] [PubMed]
- Fiore, A.; Fry, A.; Shay, D.; Gubareva, L.; Bresee, J.; Uyeki, T.; Centers for Disease Control and Prevention (CDC). Antiviral Agents for the Treatment and Chemoprophylaxis of Influenza—Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm. Rep. 2011, 60, 1–24. [Google Scholar] [PubMed]
- Randomised Trial of Efficacy and Safety of Inhaled Zanamivir in Treatment of Influenza A and B Virus Infections. The MIST (Management of Influenza in the Southern Hemisphere Trialists) Study Group. Lancet 1998, 352, 1877–1881. [Google Scholar]
- Treanor, J.J.; Hayden, F.G.; Vrooman, P.S.; Barbarash, R.; Bettis, R.; Riff, D.; Singh, S.; Kinnersley, N.; Ward, P.; Mills, R.G.; et al. Efficacy and Safety of the Oral Neuraminidase Inhibitor Oseltamivir in Treating Acute Influenza. JAMA 2000, 283, 1016. [Google Scholar] [CrossRef]
- Brendish, N.J.; Malachira, A.K.; Armstrong, L.; Houghton, R.; Aitken, S.; Nyimbili, E.; Ewings, S.; Lillie, P.J.; Clark, T.W. Routine Molecular Point-of-Care Testing for Respiratory Viruses in Adults Presenting to Hospital with Acute Respiratory Illness (ResPOC): A Pragmatic, Open-Label, Randomised Controlled Trial. Lancet Respir. Med. 2017, 5, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Li-Kim-Moy, J.; Dastouri, F.; Rashid, H.; Khandaker, G.; Kesson, A.; McCaskill, M.; Wood, N.; Jones, C.; Zurynski, Y.; Macartney, K.; et al. Utility of Early Influenza Diagnosis through Point-of-Care Testing in Children Presenting to an Emergency Department. J. Paediatr. Child. Health 2016, 52, 422–429. [Google Scholar] [CrossRef]
- Andrews, D.; Chetty, Y.; Cooper, B.S.; Virk, M.; Glass, S.K.; Letters, A.; Kelly, P.A.; Sudhanva, M.; Jeyaratnam, D. Multiplex PCR Point of Care Testing versus Routine, Laboratory-Based Testing in the Treatment of Adults with Respiratory Tract Infections: A Quasi-Randomised Study Assessing Impact on Length of Stay and Antimicrobial Use. BMC Infect. Dis. 2017, 17, 671. [Google Scholar] [CrossRef]
- Drain, P.K. Rapid Diagnostic Testing for SARS-CoV-2. N. Engl. J. Med. 2022, 386, 264–272. [Google Scholar] [CrossRef]
- PATH. Decentralizing Testing for COVID-19 and Beyond. 2021. Available online: https://www.path.org/articles/decentralizing-testing-covid-19-and-beyond/ (accessed on 13 August 2023).
- Groseclose, S.L.; Buckeridge, D.L. Public Health Surveillance Systems: Recent Advances in Their Use and Evaluation. Annu. Rev. Public Health 2017, 38, 57–79. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization (PAHO). Final Report Ad Hoc Expert Consultation in the Region of the Americas: Challenges, Gaps and next Steps in COVID 19 Surveillance and Its Integration in to Influenza and Other Respiratory Viruses Surveillance; PAHO: Washington, DC, USA, 2022; Available online: https://www.paho.org/en/documents/final-report-ad-hoc-expert-consultation-region-americas-challenges-gaps-and-next-steps (accessed on 13 August 2023).
- World Health Organization (WHO). End-to-End Integration of SARS-CoV-2 and Influenza Sentinel Surveillance: Revised Interim Guidance. January 2022. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Integrated_sentinel_surveillance-2022.1 (accessed on 13 August 2023).
- Fernandes, R.S.; de Oliveira Silva, J.; Gomes, K.B.; Azevedo, R.B.; Townsend, D.M.; de Paula Sabino, A.; Branco de Barros, A.L. Recent Advances in Point of Care Testing for COVID-19 Detection. Biomed. Pharmacother. 2022, 153, 113538. [Google Scholar] [CrossRef] [PubMed]
- de Lusignan, S.; Hoang, U.; Liyanage, H.; Tripathy, M.; Sherlock, J.; Joy, M.; Ferreira, F.; Diez-Domingo, J.; Clark, T. Using Point of Care Testing to Estimate Influenza Vaccine Effectiveness in the English Primary Care Sentinel Surveillance Network. PLoS ONE 2021, 16, e0248123. [Google Scholar] [CrossRef] [PubMed]
- Sakthivel, D.; Delgado-Diaz, D.; McArthur, L.; Hopper, W.; Richards, J.S.; Narh, C.A. Point-of-Care Diagnostic Tools for Surveillance of SARS-CoV-2 Infections. Front. Public Health 2021, 9, 766871. [Google Scholar] [CrossRef] [PubMed]
- Iliescu, F.S.; Ionescu, A.M.; Gogianu, L.; Simion, M.; Dediu, V.; Chifiriuc, M.C.; Pircalabioru, G.G.; Iliescu, C. Point-of-Care Testing—The Key in the Battle against SARS-CoV-2 Pandemic. Micromachines 2021, 12, 1464. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Argentina. Guide for the Epidemiological Surveillance and Recommendations for the Prevention and Control of Acute Respiratory Infections 2023 (Translated from Spanish: Guía Para La Vigilancia Epidemiológica y Recomendaciones Para La Prevención y Control de Las Infecciones Respiratorias Agudas 2023); Ministry of Health Argentina: Buenos Aires, Argentina, 2023. Available online: https://bancos.salud.gob.ar/sites/default/files/2023-05/guia-vigilancia-ira_2023.pdf (accessed on 13 August 2023).
- Ministry of Health Brazil. National Plan for the Testing Expansion for COVID-19 (Translated from Portuguese: Plano Nacional Da Expansão Da Testagem Para COVID-19); Ministry of Health Brazil: Brasilia, Brazil, 2022. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/cartilhas/2021/plano-nacional-de-expansao-da-testagem-para-covid-19.pdf/@@download/file (accessed on 13 August 2023).
- Ministry of Health Brazil. 14th Technical Report National Plan for the Testing Expansion for COVID-19 (Translated from Portuguese: 14° Informe Técnico Plano Nacional Da Expansão Da Testagem Para COVID-19); Ministry of Health Brazil: Brasilia, Brazil, 2022. Available online: https://www.gov.br/saude/pt-br/coronavirus/distribuicao-de-testes/pautas-de-distribuicao/14o-informe-tecnico-do-plano-nacional-de-expansao-da-testagem-para-covid-19-14a-pauta-de-distribuicao (accessed on 13 August 2023).
- Ministry of Health Chile. Testing, Tracing and Isolation Strategy (Translated from Spanish: Estrategio Testeo, Trazabilidad y Aislamiento); Ministry of Health Chile: Santiago, Chile, 2021. Available online: https://www.minsal.cl/wp-content/uploads/2021/03/GUIA_ESTRATEGIA_TTA.pdf (accessed on 13 August 2023).
- Ministry of Health and Social Protection Colombia. Guidelines for the Use of SARS-CoV-2 Diagnostic Tests in Colombia (Translated from Spanish: Lineamientos Para El Uso de Pruebas Diagnósticas Para SARS-CoV-2-En Colombia); Ministry of Health and Social Protection Colombia: Bogota, Colombia, 2022. Available online: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/PP/ET/gips21-lineamientos-uso-pruebas-diagnosticas-sars-cov-2-covid19-2021.pdf (accessed on 13 August 2023).
- Ministry of Health Costa Rica. LS-SS-012. Guidelines for the Use of the Alternative Tests (Antigen, and Isothermic Molecular Tests) from the Gold Standard (RTPCR) for the COVID-19 Diagnosis (Translated from Spanish: LS-SS-012. Lineamientos Generales Para El Uso de Pruebas Alternativas (Antígeno, Pruebas Moleculares Isotérmicas) al Estándar de Oro (RTPCR) Para El Diagnóstico de COVID-19); Ministry of Health Costa Rica: San José, Costa Rica, 2023. Available online: https://www.ministeriodesalud.go.cr/index.php/biblioteca-de-archivos-left/documentos-ministerio-de-salud/vigilancia-de-la-salud/normas-protocolos-guias-y-lineamientos/situacion-nacional-covid-19/lineamientos-especificos-covid-19/lineamientos-de-servicios-de-salud/5399-version-7-03-marzo-2022-lineamientos-generales-para-el-uso-de-pruebas-alternativas-antigeno-pruebas-moleculares-isotermicas-al-estandar-de-oro-rtpcr-para-el-diagnostico-de-covid-19/file (accessed on 12 August 2023).
- Ministry of Health Peru. Technical Document: Prevention, Diagnosis, and Treatment of People Affected by COVID-19 in Peru. (Translated from Spanish: Documento Técnico Prevención, Diagnóstico, y Tratamiento de Personas Afectadas Por COVID-19 En El Perú); Ministry of Health Peru: Lima, Peru, 2020. Available online: https://cdn.www.gob.pe/uploads/document/file/582567/Prevencio%CC%81n__Diagno%CC%81stico_y_Tratamiento_de_personas_afectadas_por_COVID-19_en_el_Peru%CC%81_.PDF?v=1588182165 (accessed on 13 August 2023).
- Freire-Paspuel, B.; Garcia-Bereguiain, M.A. Low Clinical Performance of the Isopollo COVID-19 Detection Kit (M Monitor, South Korea) for RT-LAMP SARS-CoV-2 Diagnosis: A Call for Action against Low Quality Products for Developing Countries. Int. J. Infect. Dis. 2021, 104, 303–305. [Google Scholar] [CrossRef] [PubMed]
- Morales-Jadan, D.; Castro-Rodriguez, B.; Viteri-Dávila, C.; Orlando, S.A.; Bruno, A.; Perez, F.; Garcia-Bereguiain, M.A. The Quality of Commercial SARS-CoV-2 Nucleic Acid Tests in Ecuador: Lessons from COVID-19 Pandemic for Advancing Social Equity through Microbiology. Front. Cell. Infect. Microbiol. 2023, 13, 1179786. [Google Scholar] [CrossRef]
- Hernández, C.; Florez, C.; Castañeda, S.; Ballesteros, N.; Martínez, D.; Castillo, A.; Muñoz, M.; Gomez, S.; Rico, A.; Pardo, L.; et al. Evaluation of the Diagnostic Performance of Nine Commercial RT-PCR Kits for the Detection of SARS-CoV-2 in Colombia. J. Med. Virol. 2021, 93, 5618–5622. [Google Scholar] [CrossRef]
- World Health Organization (WHO). From Emergency Response to Long-Term COVID-19 Disease Management: Sustaining Gains Made during the COVID-19 Pandemic. 2023. Available online: https://www.who.int/publications/i/item/WHO-WHE-SPP-2023.1 (accessed on 13 August 2023).
- World Health Organization (WHO). Recommendations for National SARS-CoV-2 Testing Strategies and Diagnostic Capacities Interim Guidance. 25 June 2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/342002/WHO-2019-nCoV-lab-testing-2021.1-eng.pdf?sequence=1&isAllowed=y (accessed on 13 August 2023).
- Centers for Disease Control and Prevention (CDC). Similarities and Differences between Flu and COVID-19. Available online: https://www.cdc.gov/flu/symptoms/flu-vs-covid19.htm (accessed on 13 August 2023).
- World Health Organization (WHO). WHO Policy Brief: COVID-19 Testing 14 September 2022; WHO: Geneva, Switzerland, 2022; Available online: https://apps.who.int/iris/rest/bitstreams/1465979/retrieve (accessed on 13 August 2023).
- Centers for Disease Control and Prevention (CDC). CDC’s Influenza SARS-CoV-2 Multiplex Assay. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/multiplex.html (accessed on 13 August 2023).
- Ministry of Health Brazil. Guide for Epidemiological Surveillance- Public Health National Emergency by Coronavirus 2019-Disease: Surveillance of Acute Respiratory Syndromes (Translated from Portuguese: Guia de Vigilância Epidemiologica—Emergênciacia de Saúde Pública de Importância Nacional Pela Doença Pelo Coronavírus 2019: Vigilância de Síndromes Respiratorias Agudas); Ministry of Health Brazil: Brasilia, Brazil, 2022. Available online: https://www.gov.br/saude/pt-br/coronavirus/publicacoes-tecnicas/guias-e-planos/guia-de-vigilancia-epidemiologica-covid-19/@@download/file (accessed on 13 August 2023).
- Public Health Institute Ministry of Health Chile. Respiratory virus Surveillance (Translated from Spanish: Vigilancia de Virus Respiratorios). 2023. Available online: https://www.ispch.gob.cl/virusrespiratorios/ (accessed on 13 August 2023).
- National Health Institute (INS) Colombia. Protocol for Acute Respiratory Infection Surveillance (Translated from Spanish: Protocolo de Vigilancia de Infección Respiratoria Aguda (IRA)); National Health Institute (INS) Colombia: Bogota, Colombia, 2022. Available online: https://www.ins.gov.co/buscador-eventos/Lineamientos/PRO_IRA.pdf (accessed on 13 August 2023).
- Health Secretariat Mexico. Guideline for the Surveillance by Laboratory of Respiratory Viruses (Translated from Spanish: Lineamientos para la Vigilancia por Laboratorios de Virus Respiratorios); Health Secretariat Mexico: Mexico City, Mexico, 2022. Available online: https://www.gob.mx/cms/uploads/attachment/file/727495/LVL_Virus_respiratorios__Mayo_2022_.pdf (accessed on 13 August 2023).
- National Administration of Drugs F and MD (ANMAT) A. PanbioTM COVID-19/Flu A&B Rapid Panel 62FK10 (Nasopharyngeal)-Abbott. Orlaweg. November 2023. Available online: https://helena.anmat.gob.ar/uploads/pdfs/IF-2023-06015124-APN-INPM%20ANMAT.pdf?rnd=61674e08-dd23-4ed7-970e-381ba820af8e (accessed on 13 August 2023).
- National Administration of Drugs F and MD (ANMAT) A. Accordance Declaration 1252-177 (Translated from Spanish: Declaración de conformidad-1252-177). Argentina. 2020. Available online: https://helena.anmat.gob.ar/uploads/pdfs/dc_24138_30638975994_2516.pdf?rnd=a71b0beb-2e4c-4868-b085-c0ea280087f4 (accessed on 13 August 2023).
- Ministry of Health Brazil. National Health Plan 2020-2023 (Translated from Portuguese: Plano Nacional de Saúde 2020–2023); Ministry of Health Brazil: Brasilia, Brazil, 2020. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/plano_nacional_saude_2020_2023.pdf (accessed on 13 August 2023).
- Ministry of Health Brazil. Guide for the Laboratory Network of Influenza Surveillance in Brazil (Translated from Portuguese: Guia para a Rede Laboratorial de Vigilância de Influenza no Brasil); Ministry of Health Brazil: Brasilia, Brazil, 2016. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/guia_laboratorial_influenza_vigilancia_influenza_brasil.pdf (accessed on 13 August 2023).
- Ministry of Health Brazil. Influenza Treatment Protocol: 2017 (Translated from Portuguese: Protocolo de Tratamento de Influenza: 2017); Ministry of Health Brazil: Brasilia, Brazil, 2018. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/protocolo_tratamento_influenza_2017.pdf (accessed on 13 August 2023).
- Federal District Government Brazil. Plan for the Confrontation of Childhood Respiratory Diseases in the Federal District (Translated from Portuguese: Plano de Enfrentamento para as Doencas Respiratorias da Infancia no Distrito Federal); Federal District Government Brazil: Brasilia, Brazil, 2023. Available online: https://www.saude.df.gov.br/documents/37101/0/SEI_GDF+-+107165154+-+Plano+de+A%C3%A7%C3%A3o.pdf/26544adc-aec5-af5c-2080-d9015b894b62?t=1679598372243 (accessed on 13 August 2023).
- Brazilian Health Regulatory Agency (Anvisa). Consultation of Health Products- Coronavirus Brazilian Health Regulatory Agency- ANVISA (Translated from Portuguese: Consultas Produtos para Saúde-Coronavirus ANVISA—Agencia Nacional de Vigilancia Sanitaria). 2023. Available online: https://consultas.anvisa.gov.br/#/saude/q/?nomeTecnico=coronav%C3%ADru (accessed on 13 August 2023).
- Ministry of Health Chile. National Health Strategy for the Health Obectives 2030 (Translated from Spanish: Estrategia Nacional de Salud para los Objetivos Sanitarios al 2030). 2022. Available online: https://www.minsal.cl/wp-content/uploads/2022/03/Estrategia-Nacional-de-Salud-2022-MINSAL-V8.pdf (accessed on 13 August 2023).
- Ministry of Health Chile. Clinical Practice Guideline for the Prevention, Diagnosis, and Clinical Management of Influenza Cases (Translated from Spanish: Guía de Práctica Clinica Prevención, Diagnóstico, y Manejo Clínico de Casos de Influenza). 2014. Available online: https://diprece.minsal.cl/wrdprss_minsal/wp-content/uploads/2015/02/GUIA-CLINICA-INFLUENZA-2014.pdf (accessed on 13 August 2023).
- Ministry of Health Chile. Acute Respiratory Infections (Translated from Spanish: Enfermedades Respiratorias Agudas). 2023. Available online: https://diprece.minsal.cl/programas-de-salud/programas-enfermedades-transmisibles/enfermedades-respiratorias/ (accessed on 13 August 2023).
- Ministry of Health Chile. Update of the Operational Definitions for COVID-19 Surveillance in the Framework of the Plan “We Keep Taking Care of Ourselves” (Translated from Spanish: Actualización de las definiciones operativas para la vigilancia de COVID-19 en el marco del Plan “Seguimos Cuidandónos”; Ministry of Health Chile: Santiago, Chile, 2022. Available online: https://www.minsal.cl/wp-content/uploads/2022/11/ORD-4915-19-10-2022.pdf (accessed on 13 August 2023).
- Public Health Institute, C. List of tests for detection of antigens SARS-CoV-2 of the National Regulatory Authorities from the International Forum of Medical Devices Regulators (Translated from Spanish: Listado de tests para detección de antígenos SARS-CoV-2 de la Autoridades Reguladoras Nacionales pertenecientes al Foro Internacional de Reguladores de Dispositivos Médicos). 2021. Available online: https://www.ispch.cl/wp-content/uploads/2021/12/Lista-Test-Antigenos-Covid-al-28.12.21.pdf (accessed on 13 August 2023).
- Ministry of Health and Social Protection. Public Health Decennial Plan 2022-2031 (Translated from Spanish: Plan Decenal Salud Pública 2022–2031). 2023. Available online: https://www.minsalud.gov.co/plandecenal/Paginas/PDSP-2022-2031.aspx (accessed on 13 August 2023).
- Ministry of Health and Social Protection Colombia. Guidelines for the Prevention, Diagnosis, Management and Control of Influenza Cases. (Translated from Spanish: Lineamientos para la Prevención, Diagnóstico, Manejo y Control de casos de Influenza). 2018. Available online: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/PP/lineamientos-prevencion-diagnostico-manejo-control-casos-influenza.pdf (accessed on 13 August 2023).
- Ministry of Health and Social Protection Colombia. Influenza Antipandemic Plan (Plan Antipandemia Influenza). 2010. Available online: https://www.minsalud.gov.co/salud/Paginas/PlanAntipandemiadeInfluenza.aspx (accessed on 13 August 2023).
- National Health Institute (INS) Colombia. Guidelines for Laboratory Surveillance of Respiratory Viruses (Translated from Spanish: Lineamientos para la Vigilancia por Laboratorio de Virus Respiratorios); National Health Institute (INS) Colombia: Bogota, Colombia, 2021. Available online: https://www.ins.gov.co/buscador-eventos/Informacin%20de%20laboratorio/Lineamientos%20para%20la%20vigilancia%20por%20Laboratorio%20de%20virus%20respiratorios.pdf (accessed on 13 August 2023).
- National Health Institute (INS) Colombia. Guide for the laboratory surveillance of influenza and other respiratory viruses (Translated from Spanish: Guía para la vigilancia por laboratorio del virus de la influenza y otros virus respiratorios) [Internet]; National Health Institute (INS) Colombia: Bogota, Colombia, 2017. Available online: https://www.ins.gov.co/buscador/Informacin%20de%20laboratorio/Guia%20para%20la%20Vigilancia%20por%20Laboratorio%20de%20Virus%20Respiratorios.pdf (accessed on 13 August 2023).
- National Food and Drug Surveillance Institute (INVIMA) Colombia. Nucleic Acid Tests- Diagnosis Reactives and RUO (Translated from Spanish: Pruebas de Ácidos Núcleicos- Reactivos de Diagnóstico y RUO). Available online: https://www.invima.gov.co/documents/20143/4061863/Reactivos+de+Diagno%CC%81stico+y+RUO+%28Pruebas+PCR%2C+Kit+de+Extraccio%CC%81n%2C+Kit+de+Purificacio%CC%81n%2C+etc%29_mayo-2021.pdf/ (accessed on 13 August 2023).
- Ministry of Health Costa Rica, Government of Costa Rica. National Health Plan 2016–2020 (Translated from Spanish: Plan Nacional de Salud Costa Rica). 2016. Available online: https://www.ministeriodesalud.go.cr/index.php/biblioteca-de-archivos-left/documentos-ministerio-de-salud/ministerio-de-salud/planes-y-politicas-institucionales/planes-institucionales/planes-planes-institucionales/709-plan-nacional-de-salud-2016-2020/file (accessed on 13 August 2023).
- Ministry of Health Costa Rica; Costa Rica’s Institute for Research and Teaching in Health and Nutrition (INCIENSA); Costa Rica Social Security. National Protocol for the Surveillance of People with Influenza and other Respiratory Viruses (Translated from Spanish: Protocolo Nacional para la Vigilancia de Personas con Influenza y Otras Viruses Respiratorias). 2018. Available online: https://www.ministeriodesalud.go.cr/index.php/biblioteca-de-archivos-left/documentos-ministerio-de-salud/vigilancia-de-la-salud/normas-protocolos-guias-y-lineamientos/inmunoprevenibles/1828-protocolo-nacional-para-la-vigilancia-de-personas-con-influenza-y-otras-virosis-respiratorias/file (accessed on 13 August 2023).
- Ministry of Health Costa Rica. Laboratories with Authorization for the Use of Antigen SARS-CoV-2 Tests (Translated from Spanish: Laboratorios con Aval de Salud para Realizar Pruebas de Antígeno de SARS-CoV-2). 2021. Available online: https://www.ministeriodesalud.go.cr/index.php/prensa/43-noticias-2021/839-laboratorios-con-aval-de-salud-para-realizar-pruebas-de-antigeno-de-sars-cov-2 (accessed on 13 August 2023).
- Health Secretariat Mexico. Health Secretariat Sector Program Derived from the National Development Plan of Development 2019–2024 (Translated from Spanish: Programa Sectorial derivado del Plan Nacional de Desarrollo 2019–2024). 2020. Available online: https://dof.gob.mx/nota_detalle.php?codigo=5598474&fecha=17/08/2020#gsc.tab=0 (accessed on 13 August 2023).
- Health Secretariat Mexico. National Plan for the Preparation and Response towards the Stational Influenza Increase or towards an Influenza Pandemic (Translated from Spanish: Plan Nacional para la Preparación y Respuesta Ante la Intensificación de la Influenza Estacional o Ante una Pandemia de Influenza). 2013. Available online: http://www.cenaprece.salud.gob.mx/programas/interior/emergencias/descargas/pdf/Plan_Nacional_Influenza.pdf (accessed on 13 August 2023).
- Government of Mexico. COVID Tests (Translated from Spanish: Pruebas COVID). 2021. Available online: https://www.gob.mx/profeco/es/articulos/pruebas-covid?idiom=es (accessed on 13 August 2023).
- Health Secretariat Mexico. List of Molecular Tests RT-PCR Multiplex, Useful for the Diagnosis of SARS-CoV-2 during the COVID-19 Contingency in Mexico (Translated from Spanish: Listado de Pruebas Moleculares RT-PCR Multiplexado, Útiles para el Diagnóstico de SARS-CoV-2 Durante la Contingencia de COVID-19 en Mexico). 2022. Available online: https://www.gob.mx/cms/uploads/attachment/file/785143/Listado_de_pruebas_moleculares_por_RT-PCR_Multiplexado_evaluadas_para_el_diagn_stico_de_SARS-CoV-2.pdf (accessed on 13 August 2023).
- Ministry of Health Peru. National Multisector Health Policy 2030 (Translated from Spanish: Política Nacional Multisectorial de Salud al 2030). Lima. Available online: https://cdn.www.gob.pe/uploads/document/file/1272348/Pol%C3%ADtica%20Nacional%20Multisectorial%20de%20Salud%20al%202030.pdf (accessed on 13 August 2023).
- Ministry of Health Peru. National Plan for the Preparation and Response towards a Potential Influenza and Other Emerging Respiratory virus Pandemic and an Stational Influenza Increase 2014–2015 (Translated from Spanish: Plan Nacional de Preparación y Respuesta Frente a una Potencial Pandemia de Influenza u otros Virus Respiratorios Emergentes e Incremento Estacional de Influenza); Ministry of Health Peru: Lima, Peru, 2014. Available online: http://www.dge.gob.pe/portal/docs/tools/flu/RM747_2014.pdf (accessed on 13 August 2023).
- Ministry of Health Peru. Health Directive N061- MINSA/DGE V.01 for the Epidemiological Surveillance of the Acute Respiratory Infections (ARI) (Translated from Spanish: Directiva Sanitaria N061-MINSA/DGE V.01 para la Vigilancia Epidemiológica de las Infecciones Respiratorias Agudas (IRA). 2015. Available online: http://bvs.minsa.gob.pe/local/MINSA/3266.pdf (accessed on 13 August 2023).
- General Directorate of Medicines S and D (DIGEMID), P. Rapid Tests with Specificity and Sensitivity Authorized with Sanitary Registry 31/03/2023 (Translated from Spanish: Pruebas Rapidas con Especificidad y Sensibilidad Autorizadas con Registro Sanitario 31/03/2023). 2023. Available online: https://www.digemid.minsa.gob.pe/Archivos/PortalWeb/Informativo/Covid19/AutorizacionesExcepcionales/AE_PRUEBAS_RAPIDAS_.xlsx (accessed on 13 August 2023).
- Ministry of Health Costa Rica. Health Regulation-Bioequivalency (Translated from Spanish: Regulación de la Salud-Bioequivalencia). 2022. Available online: https://www.ministeriodesalud.go.cr/index.php/regulacion-de-la-salud/20-regulacion-de-la-salud/60-bioequivalencia-2 (accessed on 13 August 2023).
- Centers for Disease Control and Prevention (CDC). Information on Rapid Molecular Assays, RT-PCR, and other Molecular Assays for Diagnosis of Influenza Virus Infection. 2019. Available online: https://www.cdc.gov/flu/professionals/diagnosis/molecular-assays.htm (accessed on 13 August 2023).
- Ritchey, M.D.; Rosenblum, H.G.; Del Guercio, K.; Humbard, M.; Santos, S.; Hall, J.; Chaitram, J.; Salerno, R.M. COVID-19 Self-Test Data: Challenges and Opportunities—United States, 31 October 2021–11 June 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1005–1010. [Google Scholar] [CrossRef]
- Hay, J.A.; Kennedy-Shaffer, L.; Kanjilal, S.; Lennon, N.J.; Gabriel, S.B.; Lipsitch, M.; Mina, M.J. Estimating Epidemiologic Dynamics from Cross-Sectional Viral Load Distributions. Science 2021, 373, eabh0635. [Google Scholar] [CrossRef]
- World Health Organization (WHO). COVID-19 Diagnostic Testing in the Context of International Travel-16 December 2020-19: Scientific Briefs. 2020. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Sci_Brief-international_travel_testing-2020.1 (accessed on 13 August 2023).
- U.S. Food and Drug Administration (FDA). Antibody (Serology) Testing for COVID-19: Information for Patients and Consumers. 2023. Available online: https://www.fda.gov/medical-devices/coronavirus-covid-19-and-medical-devices/antibody-serology-testing-covid-19-information-patients-and-consumers (accessed on 13 August 2023).
- Kundu, D.; Gautam, P.; Dayanand, D.; Gunasekaran, K.; Manesh, A.; Sebastian, M.; Abhilash, K.P.P.; Zachariah, A.; George, T.; Sathyendra, S.; et al. The Role and Diagnostic Accuracy of Serology for COVID-19. BMC Infect. Dis. 2022, 22, 390. [Google Scholar] [CrossRef]
- Lai, C.K.C.; Lam, W. Laboratory Testing for the Diagnosis of COVID-19. Biochem. Biophys. Res. Commun. 2021, 538, 226–230. [Google Scholar] [CrossRef]
- Mitra, P.; Sharma, P. POCT in Developing Countries. EJIFCC 2021, 32, 195–199. [Google Scholar]
- Yadav, H.; Shah, D.; Sayed, S.; Horton, S.; Schroeder, L.F. Availability of Essential Diagnostics in Ten Low-Income and Middle-Income Countries: Results from National Health Facility Surveys. Lancet Glob. Health 2021, 9, e1553–e1560. [Google Scholar] [CrossRef]
- The World Bank. Current Health Expenditure (% of GDP)—Latin America & Caribbean. Available online: https://data.worldbank.org/indicator/SH.XPD.CHEX.GD.ZS?locations=ZJ&name_desc=true (accessed on 28 January 2024).
- Ortiz-Prado, E.; Henriquez-Trujillo, A.R.; Rivera-Olivero, I.A.; Freire-Paspuel, B.; Vallejo-Janeta, A.P.; Lozada, T.; Garcia-Bereguiain, M.A. Massive SARS-CoV-2 RT-PCR Testing on Rural Communities in Manabi Province (Ecuador) Reveals Severe COVID-19 Outbreaks. Am. J. Trop. Med. Hyg. 2021, 104, 1493–1494. [Google Scholar] [CrossRef] [PubMed]
- Nichols, J.H. Utilizing Point-of-Care Testing to Optimize Patient Care. EJIFCC 2021, 32, 140–144. [Google Scholar] [PubMed]
- Ibrahim, N.K. Epidemiologic Surveillance for Controlling Covid-19 Pandemic: Types, Challenges and Implications. J. Infect. Public Health 2020, 13, 1630–1638. [Google Scholar] [CrossRef] [PubMed]
| Country/ Region | Cumulative Cases per Million Inhabitants (As of 18 November 2023) [73] | Cumulative Deaths per Million Inhabitants (As of 18 November 2023) [73] | Excess Mortality (As of 31 December 2021) a [78] | Tests per Confirmed Case b [77] | Tests Applied per 1000 Inhabitants [76] | Type of Tests Reported c [79] | Vaccination Rate (As of 24 November 2023) d [71] |
|---|---|---|---|---|---|---|---|
| LATAM e | NA: 207,377.11 SA: 157,588.76 | NA: 2689.55 SA: 3105.43 | Not available by region | Not available by region | Not available by region | PCR tests Antigen test Selection of serology tests | 71.21 f |
| Argentina | 220,929.56 | 2866.87 | 19.24% | 3.50 (4 June 2022) | 809.77 (4 June 2022) | - | 83.73 |
| Brazil | 175,194.53 | 3272.71 | 22.34% | Not available | 330.91 (11 March 2022) | PCR tests Antigen test Selection of serology tests | 80.66 |
| Chile | 269,794.54 | 3143.13 | 18.54% | 6.70 (22 June 2022) | 2040.37 (22 June 2022) | PCR tests Antigen test | 92.68 |
| Colombia | 123,068.00 | 2755.56 | 28.70% | 11.80 (16 June 2022) | 684.08 (16 June 2022) | PCR tests Antigen test | 72.76 |
| Costa Rica | 239,128.20 | 1819.78 | 11.49% | 5.70 (29 May 2022) | 713.53 (29 May 2022) | PCR tests | 85.57 |
| Mexico | 60,336.25 | 2625.69 | 34.35% | 2.00 (18 June 2022) | 122.88 (18 June 2022) | PCR tests Antigen test | 63.09 |
| Peru | 132,820.23 | 6511.89 | 45.50% | 111.10 (5 April 2022) | 859.28 (5 April 2022) | PCR tests Antigen test Serology test | 86.91 |
| Country/Region | Prevalence Lower Respiratory Infections (Rate; 2019) [108] | Prevalence Upper Respiratory Infections (Rate; 2019) [108] | Incidence Lower Respiratory Infections (Rate; 2019) [108] | Incidence Upper Respiratory Infections (Rate; 2019) [108] | Cumulative Percent Positivity Influenza (2022) [109] | Cumulative Percent Positivity RSV (2022) [109] |
|---|---|---|---|---|---|---|
| LATAM | 149.99 | 3751.78 | 6862.71 | 272,487.36 | 6% | 3% |
| Argentina | 123.31 | 3782.42 | 5612.97 | 274,577.70 | 11% | 7% |
| Brazil a | 190.22 | 4204.29 | 8738.58 | 305,180.61 | Fiocruz: 2% Adolfo Lutz: 6% Evandro Chagas: 18% | Fiocruz: 0% Adolfo Lutz: 4% Evandro Chagas: 1% |
| Chile | 87.05 | 3715.18 | 4066.10 | 269,742.74 | 11% | 7% |
| Colombia | 120.14 | 4115.23 | 5597.67 | 299,095.86 | 1% | 4% |
| Costa Rica | 143.72 | 3194.20 | 6629.07 | 232,100.73 | 6% | 5% |
| Mexico | 102.01 | 3442.71 | 4616.49 | 250,202.90 | 34% | 4% |
| Peru | 210.70 | 3754.46 | 9628.63 | 272,846.31 | 11% | 1% |
| ARI | Types of POC Rapid Tests | Advantages of Rapid Antigen Test | Disadvantages of Rapid Antigen Tests |
| COVID-19 |
| ||
| Influenza |
| ||
| RSV |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alvarez-Moreno, C.A.; de Araújo, E.S.A.; Baumeister, E.; Nogales Crespo, K.A.; Kalergis, A.M.; Muñoz Medina, J.E.; Tsukayama, P.; Ugarte-Gil, C. Differential Diagnosis in the Management of Acute Respiratory Infections through Point-of-Care Rapid Testing in a Post-Pandemic Scenario in Latin America: Special Focus on COVID-19, Influenza, and Respiratory Syncytial Virus. COVID 2024, 4, 221-260. https://doi.org/10.3390/covid4020017
Alvarez-Moreno CA, de Araújo ESA, Baumeister E, Nogales Crespo KA, Kalergis AM, Muñoz Medina JE, Tsukayama P, Ugarte-Gil C. Differential Diagnosis in the Management of Acute Respiratory Infections through Point-of-Care Rapid Testing in a Post-Pandemic Scenario in Latin America: Special Focus on COVID-19, Influenza, and Respiratory Syncytial Virus. COVID. 2024; 4(2):221-260. https://doi.org/10.3390/covid4020017
Chicago/Turabian StyleAlvarez-Moreno, Carlos Arturo, Evaldo Stanislau Affonso de Araújo, Elsa Baumeister, Katya A. Nogales Crespo, Alexis M. Kalergis, José Esteban Muñoz Medina, Pablo Tsukayama, and Cesar Ugarte-Gil. 2024. "Differential Diagnosis in the Management of Acute Respiratory Infections through Point-of-Care Rapid Testing in a Post-Pandemic Scenario in Latin America: Special Focus on COVID-19, Influenza, and Respiratory Syncytial Virus" COVID 4, no. 2: 221-260. https://doi.org/10.3390/covid4020017