
Patient-Perceived Impact of the COVID-19 Pandemic on Medication Adherence and Access to Care for Long-Term Diseases: A Cross-Sectional Online Survey
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
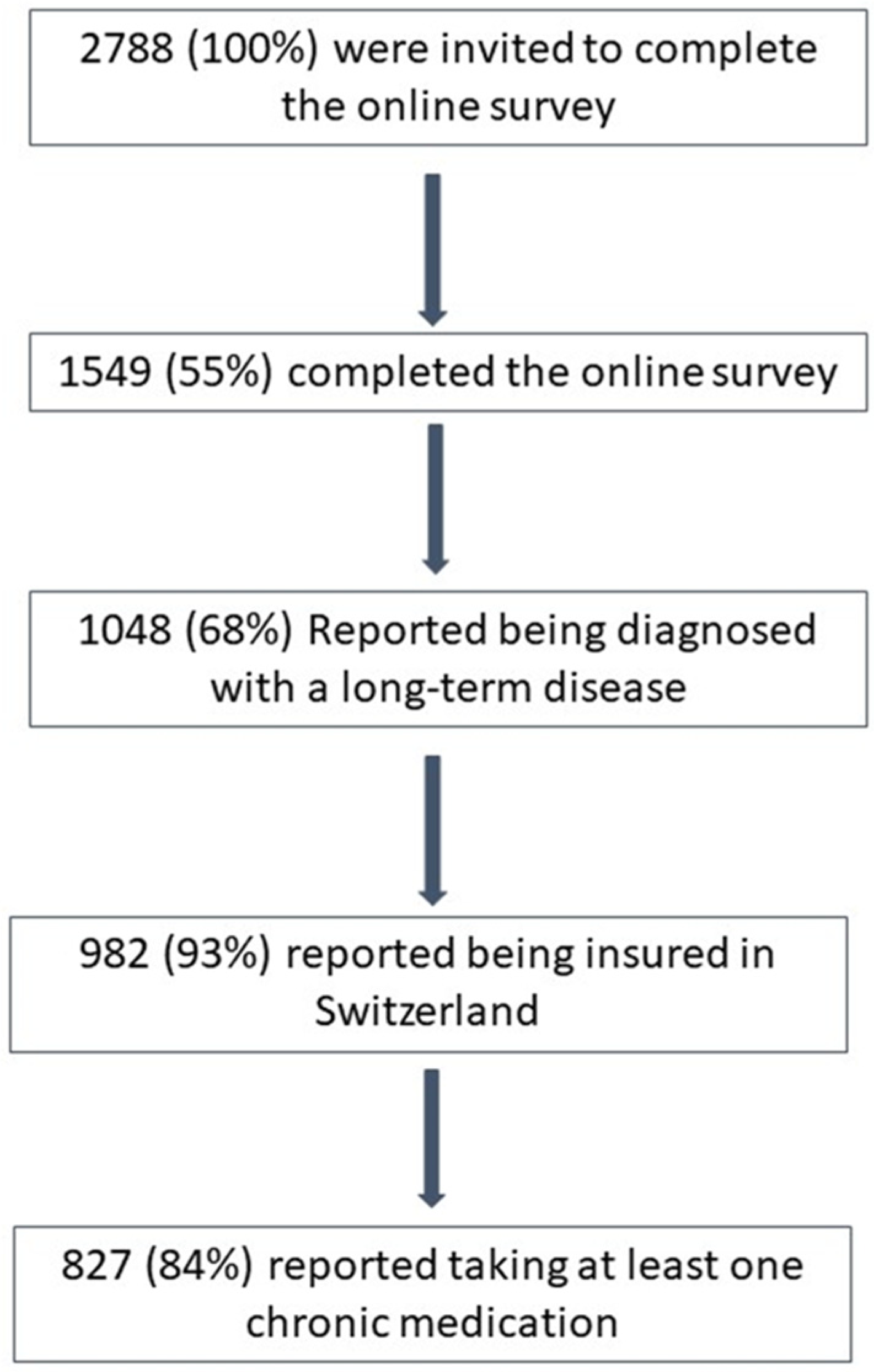
2.1. Study Design and Patients’ Eligibility
2.2. Study Variables and Measurements
2.3. Data Management and Statistical Analysis
3. Results
3.1. Impact of the Pandemic on Adherence to Long-Term Medications and Motivation to Take Medications
3.2. Impact of the Pandemic on Access to Medications, Medical Appointments, Exams and Overall Medical Care
3.3. Impact on Diet and Physical Activity Programs, Participation in Therapeutic Support Groups and Home Care
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burkhart, P.V.; Sabaté, E. Adherence to long-term therapies: Evidence for action. J. Nurs. Sch. 2003, 35, 207. [Google Scholar] [CrossRef]
- Maldonado, D.; Tu, E.; Mahmood, S.N.; Wahezi, D.M.; Darapaneni, R.; Sima, N.; Curiel-Duran, L.; Pattison, L.M.; Gabbay, V.; Bauman, L.J.; et al. Association of Medication Access Difficulty and COVID-19-Related Distress With Disease Flares in Rheumatology Patients During the COVID-19 Pandemic. Arthritis Care Res. 2021, 73, 1162–1170. [Google Scholar] [CrossRef]
- Menon, S.; Sander, J.W. Effects of the COVID-19 pandemic on medication adherence: In the case of antiseizure medications, A scoping review. Seizure 2021, 93, 81–87. [Google Scholar] [CrossRef]
- Olmastroni, E.; Galimberti, F.; Tragni, E.; Catapano, A.L.; Casula, M. Impact of COVID-19 Pandemic on Adherence to Chronic Therapies: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 3825. [Google Scholar] [CrossRef]
- Gasteiger, N.; Vedhara, K.; Massey, A.; Jia, R.; Ayling, K.; Chalder, T.; Coupland, C.; Broadbent, E. Depression, anxiety and stress during the COVID-19 pandemic: Results from a New Zealand cohort study on mental well-being. BMJ Open 2021, 11, e045325. [Google Scholar] [CrossRef] [PubMed]
- Refaie, E.; García Mateo, S.; Martínez Domínguez, S.J.; Gargallo-Puyuelo, C.J.; Lario Quilez, L.; Carrera-Lasfuentes, P.; Arroyo Villarino, M.T.; Gomollón García, F. Impact of the lockdown period due to the COVID-19 pandemic in patients with inflammatory bowel disease. Gastroenterol. Hepatol. 2022, 45, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Patel, D.; Xie, D.; Pernes, T.; Lewis, J.; Yang, Y.X. Adherence of Infusible Biologics During the Time of COVID-19 Among Patients With Inflammatory Bowel Disease: A Nationwide Veterans Affairs Cohort Study. Gastroenterology 2020, 159, 1592–1594.e1. [Google Scholar] [CrossRef] [PubMed]
- Tilotta, G.; Pistone, G.; Caruso, P.; Gurreri, R.; Castelli, E.; Curiale, S.; Caputo, V.; Bongiorno, M.R. Adherence to biological therapy in dermatological patients during the COVID-19 pandemic in Western Sicily. Int. J. Dermatol. 2021, 60, 248–249. [Google Scholar] [CrossRef]
- Zhang, Y.; Staker, E.; Cutter, G.; Krieger, S.; Miller, A.E. Perceptions of risk and adherence to care in MS patients during the COVID-19 pandemic: A cross-sectional study. Mult. Scler. Relat. Disord. 2021, 50, 102856. [Google Scholar] [CrossRef]
- Konak, H.E.; Armağan, B.; Güven, S.C.; Atalar, E.; Karakaş, Ö.; Esmer, S.; Eksin, M.A.; Polat, B.; Apaydin, H.; Gök, K.; et al. Intravenous treatment adherence of patients with chronic inflammatory rheumatic diseases during the COVID-19 pandemic: Experience of a single center. Rom. J. Intern. Med. 2022, 60, 173–181. [Google Scholar] [CrossRef]
- WHO. The Impact of the COVID-19 Pandemic on Noncommunicable Disease Resources and Services: Results of a Rapid Assessment. 2020. Available online: https://iris.who.int/handle/10665/334136 (accessed on 6 February 2024).
- Esposti, L.D.; Buda, S.; Nappi, C.; Paoli, D.; Perrone, V. Implications of COVID-19 infection on medication adherence with chronic therapies in italy: A proposed observational investigation by the fail-to-refill project. Risk Manag. Healthc. Policy 2020, 13, 3179–3185. [Google Scholar] [CrossRef]
- Michaud, K.; Wipfler, K.; Shaw, Y.; Simon, T.A.; Cornish, A.; England, B.R.; Ogdie, A.; Katz, P. Experiences of Patients With Rheumatic Diseases in the United States during Early Days of the COVID-19 Pandemic. ACR Open Rheumatol. 2020, 2, 335–343. [Google Scholar] [CrossRef]
- Coman, C.; Bularca, M.C.; Repanovici, A.; Rogozea, L. Misinformation about medication during the COVID- 19 pandemic: A perspective of medical staff. PLoS ONE 2022, 17, e0276693. [Google Scholar] [CrossRef] [PubMed]
- Baysson, H.; Pennachio, F.; Wisniak, A.; Zabella, M.E.; Pullen, N.; Collombet, P.; Lorthe, E.; Joost, S.; Balavoine, J.F.; Bachmann, D.; et al. Specchio-COVID19 cohort study: A longitudinal follow-up of SARS-CoV-2 serosurvey participants in the canton of Geneva, Switzerland. BMJ Open 2022, 12, e055515. [Google Scholar] [CrossRef]
- Baysson, H.; Pennacchio, F.; Wisniak, A.; Zaballa, M.-E.; Pullen, N.; Collombet, P.; Lorthe, E.; Joost, S.; Balavoine, J.-F.; Bachmann, D.; et al. The Specchio-COVID19 cohort study: A longitudinal follow-up of SARS-CoV-2 serosurvey participants in the canton of Geneva, Switzerland (Study protocol). medRxiv 2021. [Google Scholar] [CrossRef]
- Vrijens, B.; De Geest, S.; Hughes, D.A.; Przemyslaw, K.; Demonceau, J.; Ruppar, T.; Dobbels, F.; Fargher, E.; Morrison, V.; Lewek, P.; et al. A new taxonomy for describing and defining adherence to medications. Br. J. Clin. Pharmacol. 2012, 73, 691–705. [Google Scholar] [CrossRef]
- WHO. International Classification of Diseases 11th Revision. Available online: https://icd.who.int/en (accessed on 6 February 2024).
- WHO. Anatomical Therapeutic Chemical Classification System/Defined Daily Dose (ATC/DDD) Index 2021. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 6 February 2024).
- Farina, M.P.; Ailshire, J.A. Sociodemographic and health status differences in delaying medical care during the COVID-19 pandemic among older adults: Findings from the Health and Retirement Study. BMC Public Health 2022, 22, 1720. [Google Scholar] [CrossRef] [PubMed]
- Larsen, J.; Stovring, H.; Kragstrup, J.; Hansen, D.G. Can differences in medical drug compliance between European countries be explained by social factors: Analyses based on data from the European Social Survey, round 2. BMC Public Health 2009, 9, 145. [Google Scholar] [CrossRef] [PubMed]
- Wuyts, J.; Maesschalck, J.; De Wulf, I.; De Lepeleire, J.; Foulon, V. Studying the impact of a medication use evaluation by the community pharmacist (Simenon): Patient-reported outcome measures. Res. Soc. Adm. Pharm. 2020, 16, 1760–1767. [Google Scholar] [CrossRef]
- Jarab, A.S.; Mukattash, T.L. Exploring variables associated with medication non-adherence in patients with COPD. Int. J. Clin. Pharm. 2019, 41, 1202–1209. [Google Scholar] [CrossRef] [PubMed]
- Al-Qerem, W.; Jarab, A.S.; Badinjki, M.; Hyassat, D.; Qarqaz, R. Exploring variables associated with medication non-adherence in patients with type 2 diabetes mellitus. PLoS ONE 2021, 16, e0256666. [Google Scholar] [CrossRef] [PubMed]
- Kardas, P.; Lewek, P.; Matyjaszczyk, M. Determinants of patient adherence: A review of systematic reviews. Front. Pharmacol. 2013, 4, 91. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Du, J.; Li, Z.; Xu, Z.; Wu, Y.; Duan, W.; Wang, W.; Zhang, T.; Xu, J.; Wu, H.; et al. It is time to improve the acceptance of COVID-19 vaccines among people with chronic diseases: A systematic review and meta-analysis. J. Med. Virol. 2023, 95, e28509. [Google Scholar] [CrossRef] [PubMed]
- Sunjaya, A.P.; Allida, S.M.; Di Tanna, G.L.; Jenkins, C.R. Asthma and COVID-19 risk: A systematic review and meta-analysis. Eur. Respir. J. Mar. 2022, 59, 2101209. [Google Scholar] [CrossRef] [PubMed]
- Shcherbakova, N.; Shepherd, M. Community pharmacists, Internet and social media: An empirical investigation. Res. Soc. Adm. Pharm. 2014, 10, e75–e85. [Google Scholar] [CrossRef]
- Ismail, H.; Marshall, V.D.; Patel, M.; Tariq, M.; Mohammad, R.A. The impact of the COVID-19 pandemic on medical conditions and medication adherence in people with chronic diseases. J. Am. Pharm. Assoc. 2022, 62, 834–839.e1. [Google Scholar] [CrossRef]
- Clement, J.; Jacobi, M.; Greenwood, B.N. Patient access to chronic medications during the COVID-19 pandemic: Evidence from a comprehensive dataset of US insurance claims. PLoS ONE 2021, 16, e0249453. [Google Scholar] [CrossRef]
- Boulin, M.; Cransac-Miet, A.; Maynadié, M.; Volot, F.; Creuzot-Garcher, C.; Eicher, J.C.; Chagué, F.; Ksiazek, E.; Beltramo, G.; Bonniaud, P.; et al. COVID-19 Lockdown in Patients with Chronic Diseases: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 3957. [Google Scholar] [CrossRef]
- Romagnoli, A.; Santoleri, F.; Costantini, A. The impact of COVID-19 on chronic therapies: The Pescara (ASL) local health authority experience in Italy. Curr. Med. Res. Opin. 2022, 38, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Mueller, T.M.; Kostev, K.; Gollwitzer, S.; Lang, J.D.; Stritzelberger, J.; Westermayer, V.; Reindl, C.; Hamer, H.M. The impact of the coronavirus disease (COVID-19) pandemic on outpatient epilepsy care: An analysis of physician practices in Germany. Epilepsy Behav. 2021, 117, 107833. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, F.; Polymeris, A.A.; Verbeek, M.; Engelter, S.T.; Hersberger, K.E.; Schaedelin, S.; Arnet, I.; Lyrer, P.A. Impact of the COVID-19 lockdown on the adherence of stroke patients to direct oral anticoagulants: A secondary analysis from the MAAESTRO study. J. Neurol. 2022, 269, 19–25. [Google Scholar] [CrossRef]
- Cransac-Miet, A.; Zeller, M.; Chagué, F.; Faure, A.S.; Bichat, F.; Danchin, N.; Boulin, M.; Cottin, Y. Impact of COVID-19 lockdown on lifestyle adherence in stay-at-home patients with chronic coronary syndromes: Towards a time bomb. Int. J. Cardiol. 2021, 323, 285–287. [Google Scholar] [CrossRef] [PubMed]
- Midão, L.; Almada, M.; Carrilho, J.; Sampaio, R.; Costa, E. Pharmacological Adherence Behavior Changes during COVID-19 Outbreak in a Portugal Patient Cohort. Int. J. Environ. Res. Public Health 2022, 19, 1135. [Google Scholar] [CrossRef] [PubMed]
- Di Novi, C.; Leporatti, L.; Levaggi, R.; Montefiori, M. Adherence during COVID-19: The role of aging and socio-economics status in shaping drug utilization. J. Econ. Behav. Organ. 2022, 204, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Kaye, L.; Theye, B.; Smeenk, I.; Gondalia, R.; Barrett, M.A.; Stempel, D.A. Changes in medication adherence among patients with asthma and COPD during the COVID-19 pandemic. J. Allergy Clin. Immunol. Pr. 2020, 8, 2384–2385. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Yang-Huang, J.; Franse, C.B.; Rukavina, T.; Vasiljev, V.; Mattace-Raso, F.; Verma, A.; Borrás, T.A.; Rentoumis, T.; Raat, H. Factors associated with polypharmacy and the high risk of medication-related problems among older community-dwelling adults in European countries: A longitudinal study. BMC Geriatr. 2022, 22, 841. [Google Scholar] [CrossRef] [PubMed]
- Ruksakulpiwat, S.; Zhou, W.; Niyomyart, A.; Wang, T.; Kudlowitz, A. How does the COVID-19 pandemic impact medication adherence of patients with chronic disease? A systematic review. Chronic Illn. 2022, 19, 495–513. [Google Scholar] [CrossRef] [PubMed]
- Fox, E.R.; Stolbach, A.I.; Mazer-Amirshahi, M. The Landscape of Prescription Drug Shortages During the COVID-19 Pandemic. J. Med. Toxicol. 2020, 16, 311–313. [Google Scholar] [CrossRef]
- Cameron, E.E.; Bushell, M.-J.A. Analysis of drug shortages across two countries during pre-pandemic and pandemic times. Res. Soc. Adm. Pharm. 2021, 17, 1570–1573. [Google Scholar] [CrossRef]
- Akour, A.; Elayeh, E.; Tubeileh, R.; Hammad, A.; Ya’Acoub, R.; Al-Tammemi, A.B. Role of community pharmacists in medication management during COVID-19 lockdown. Pathog. Glob. Health 2021, 115, 168–177. [Google Scholar] [CrossRef]
- Han, E.; Tan, M.M.J.; Turk, E.; Sridhar, D.; Leung, G.M.; Shibuya, K.; Asgari, N.; Oh, J.; García-Basteiro, A.L.; Hanefeld, J.; et al. Lessons learnt from easing COVID-19 restrictions: An analysis of countries and regions in Asia Pacific and Europe. Lancet 2020, 396, 1525–1534. [Google Scholar] [CrossRef] [PubMed]
- FOPH. Simplified Supply of Medicinal Products Subject to Prescription. Available online: https://www.bag.admin.ch/bag/en/home/medizin-und-forschung/heilmittel/abgabe-von-arzneimitteln.html (accessed on 6 February 2024).
- Bandiera, C.; Pasquier, J.; Locatelli, I.; Niquille, A.; Wuerzner, G.; Dotta-Celio, J.; Hachfeld, A.; Wandeler, G.; Wagner, A.D.; Csajka, C.; et al. Medication Adherence Evaluated Through Electronic Monitors During the 2020 COVID-19 Pandemic Lockdown in Switzerland: A Longitudinal Analysis. Patient Prefer Adherence 2022, 16, 2313–2320. [Google Scholar] [CrossRef]
- Bell, J.S.; Reynolds, L.; Freeman, C.; Jackson, J.K. Strategies to promote access to medications during the COVID-19 pandemic. Aust. J. Gen. Pract. 2020, 49, 530–532. [Google Scholar] [CrossRef] [PubMed]
- Wilson, G.; Windner, Z.; Bidwell, S.; Currie, O.; Dowell, A.; Halim, A.A.; Toop, L.; Savage, R.; Ranaweera, U.; Beadel, H.; et al. ‘Here to stay’: Changes to prescribing medication in general practice during the COVID-19 pandemic in New Zealand. J. Prim. Health Care 2021, 13, 222–230. [Google Scholar] [CrossRef]
- Parajuli, D.R.; Khanal, S.; Wechkunanukul, K.H.; Ghimire, S.; Poudel, A. Pharmacy practice in emergency response during the COVID-19 pandemic: Lessons from Australia. Res. Soc. Adm. Pharm. 2022, 18, 3453–3462. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishnan, M.; Poojari, P.G.; Rashid, M.; Nair, S.; Pulikkel Chandran, V.; Thunga, G. Impact of COVID-19 pandemic on medicine supply chain for patients with chronic diseases: Experiences of the community pharmacists. Clin. Epidemiol. Glob. Health 2023, 20, 101243. [Google Scholar] [CrossRef]
- Chatterji, P.; Li, Y. Effects of the COVID-19 Pandemic on Outpatient Providers in the United States. Med. Care 2021, 59, 58–61. [Google Scholar] [CrossRef]
- Zhang, Y.N.; Chen, Y.; Wang, Y.; Li, F.; Pender, M.; Wang, N.; Yan, F.; Ying, X.H.; Tang, S.L.; Fu, C.W. Reduction in healthcare services during the COVID-19 pandemic in China. BMJ Glob. Health 2020, 5, e003421. [Google Scholar] [CrossRef]
- Shadmi, E. Disparities in multiple chronic conditions within populations. J. Comorb. 2013, 3, 45–50. [Google Scholar] [CrossRef]
- Michel, J.; Schmid, S.; Aebersold, E.R.; Mettler, A.; Sauter, T.C. Did the pandemic influence telehealth use among Swiss emergency department patients? A sequential explanatory study. BMJ Open 2023, 13, e070046. [Google Scholar] [CrossRef]
- Stamenova, V.; Chu, C.; Pang, A.; Fang, J.; Shakeri, A.; Cram, P.; Bhattacharyya, O.; Bhatia, R.S.; Tadrous, M. Virtual care use during the COVID-19 pandemic and its impact on healthcare utilization in patients with chronic disease: A population-based repeated cross-sectional study. PLoS ONE 2022, 17, e0267218. [Google Scholar] [CrossRef]
- Singer, A.; Kosowan, L.; LaBine, L.; Shenoda, D.; Katz, A.; Abrams, E.M.; Halas, G.; Wong, S.T.; Talpade, S.; Kirby, S.; et al. Characterizing the use of virtual care in primary care settings during the COVID-19 pandemic: A retrospective cohort study. BMC Prim. Care 2022, 23, 320. [Google Scholar] [CrossRef] [PubMed]
- Hardcastle, L.; Ogbogu, U. Virtual care: Enhancing access or harming care? Healthc. Manag. Forum 2020, 33, 288–292. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Pasion, R.; Paiva, T.O.; Fernandes, C.; Barbosa, F. The AGE Effect on Protective Behaviors During the COVID-19 Outbreak: Sociodemographic, Perceptions and Psychological Accounts. Front. Psychol. 2020, 11, 561785. [Google Scholar] [CrossRef]
- Poroes, C.; Henchoz, Y.; Seematter-Bagnoud, L. Government recommendations during the COVID-19 epidemic in Switzerland: Clarity, compliance and impact on the daily life of seniors in a population-based cohort. Swiss Med. Wkly. 2022, 152, w30161. [Google Scholar] [CrossRef]
- FOPH. Coronavirus: Measures and Ordinances. Available online: https://www.bag.admin.ch/bag/en/home/krankheiten/ausbrueche-epidemien-pandemien/aktuelle-ausbrueche-epidemien/novel-cov/massnahmen-des-bundes.html (accessed on 6 February 2024).
- Jones, A.; Maclagan, L.C.; Schumacher, C.; Wang, X.; Jaakkimainen, R.L.; Guan, J.; Swartz, R.H.; Bronskill, S.E. Impact of the COVID-19 Pandemic on Home Care Services Among Community-Dwelling Adults With Dementia. J. Am. Med. Dir. Assoc. 2021, 22, 2258–2262.e1. [Google Scholar] [CrossRef]
- Sterling, M.R.; Tseng, E.; Poon, A.; Cho, J.; Avgar, A.C.; Kern, L.M.; Ankuda, C.K.; Dell, N. Experiences of Home Health Care Workers in New York City During the Coronavirus Disease 2019 Pandemic: A Qualitative Analysis. JAMA Intern. Med. 2020, 180, 1453–1459. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Boyland, E.; Chisholm, A.; Harrold, J.; Maloney, N.G.; Marty, L.; Mead, B.R.; Noonan, R.; Hardman, C.A. Obesity, eating behavior and physical activity during COVID-19 lockdown: A study of UK adults. Appetite 2021, 156, 104853. [Google Scholar] [CrossRef]
- Sakur, F.; Ward, K.; Khatri, N.N.; Lau, A.Y.S. Self-care Behaviors and Technology Used During COVID-19: Systematic Review. JMIR Hum. Factors 2022, 9, e35173. [Google Scholar] [CrossRef]
- Bevilacqua, G.; D’Angelo, S.; Linaker, C.; Paul, A.; Bloom, I.; Zhang, J.; Laskou, F.; Cooper, C.; Ward, K.A.; Walker-Bone, K.; et al. Physical Activity and Diet in a Global Pandemic: An Investigation of the Impact of COVID-19 on Factors Relevant for Musculoskeletal Health at Two Different Stages of the Lifecourse. Front. Endocrinol. 2022, 13, 882399. [Google Scholar] [CrossRef]
- Park, A.H.; Zhong, S.; Yang, H.; Jeong, J.; Lee, C. Impact of COVID-19 on physical activity: A rapid review. J. Glob. Health 2022, 12, 05003. [Google Scholar] [CrossRef]
- Lallukka, T.; Pietiläinen, O.; Jäppinen, S.; Laaksonen, M.; Lahti, J.; Rahkonen, O. Factors associated with health survey response among young employees: A register-based study using online, mailed and telephone interview data collection methods. BMC Public Health 2020, 20, 184. [Google Scholar] [CrossRef] [PubMed]
- Kelfve, S.; Kivi, M.; Johansson, B.; Lindwall, M. Going web or staying paper? The use of web-surveys among older people. BMC Med. Res. Methodol. 2020, 20, 252. [Google Scholar] [CrossRef] [PubMed]
- Stirratt, M.J.; Dunbar-Jacob, J.; Crane, H.M.; Simoni, J.M.; Czajkowski, S.; Hilliard, M.E.; Aikens, J.E.; Hunter, C.M.; Velligan, D.I.; Huntley, K.; et al. Self-report measures of medication adherence behavior: Recommendations on optimal use. Transl. Behav. Med. 2015, 5, 470–482. [Google Scholar] [CrossRef] [PubMed]
- Pizzoli, S.F.M.; Renzi, C.; Arnaboldi, P.; Russell-Edu, W.; Pravettoni, G. From life-threatening to chronic disease: Is this the case of cancers? A systematic review. Cogent Psychol. 2019, 6, 1577593. [Google Scholar] [CrossRef]
- Puspitasari, I.M.; Garnisa, I.T.; Sinuraya, R.K.; Witriani, W. Perceptions, Knowledge, and Attitude Toward Mental Health Disorders and Their Treatment Among Students in an Indonesian University. Psychol. Res. Behav. Manag. 2020, 13, 845–854. [Google Scholar] [CrossRef]


{kind=link}
| Sociodemographic Data | N (%) |
|---|---|
| Age range (yrs) (n = 982; min 18; max 97; missing data = 0;) | |
| 18–40 | 127 (13%) |
| 41–60 | 482 (49%) |
| 61–80 | 356 (36%) |
| ≥ 81 | 17 (2%) |
| Gender (n= 982; other = 4; missing data = 0) | |
| Female | 596 (61%) |
| Nationality (n = 982; missing data = 0) | |
| Swiss | 831 (85%) |
| European | 101 (10%) |
| Extra-European | 50 (5%) |
| Native language (n = 982; missing data = 0) | |
| French | 697 (71%) |
| Highest education level (n = 977; missing data = 5) | |
| Primary (obligatory schooling) | 41 (4%) |
| Secondary (middle school, high school, apprenticeship) | 432 (44%) |
| Tertiary (university, professional college) | 504 (51%) |
| Living as (n= 982; missing data= 0) | |
| Couple, no children | 341 (35%) |
| Couple with children | 333 (34%) |
| Alone | 210 (21%) |
| Together with other adults (cohabitation) | 46 (5%) |
| Single parent | 52 (5%) |
| Working situation (n = 982; missing data = 0) | |
| Employed | 528 (54%) |
| Retired | 286 (29%) |
| Independent | 70 (7%) |
| Disabled (disability insurance) | 25 (3%) |
| In the household | 34 (3%) |
| Unemployed | 25 (3%) |
| Student | 14 (1%) |
| Financial difficulties (n = 982; missing data = 0) | |
| No (never) | 534 (54%) |
| Yes, in the past (not anymore) | 300 (31%) |
| Yes, I have been for many years | 55 (6%) |
| Yes, for a year or less | 30 (3%) |
| I do not wish to answer | 63 (6%) |
| Clinical and Health-Related Data | N (%) |
|---|---|
| Chronic diseases (n = 2548; missing data = 0) | |
| Heart diseases | 483 (19%) |
| Metabolic diseases | 367 (14%) |
| Osteoarticular diseases | 328 (13%) |
| Respiratory diseases | 247 (10%) |
| Digestive diseases | 173 (7%) |
| Psychological/mental diseases | 172 (7%) |
| Neurological diseases | 148 (6%) |
| Urinary tract diseases | 126 (5%) |
| Dermatological diseases | 121 (5%) |
| Immunological diseases | 109 (4%) |
| Cancers | 97 (4%) |
| Others (eyes, infectious diseases, blood and others non-classified) | 177 (7%) |
| Number of medications taken (n = 917; missing data = 65) | |
| 0 | 90 (9%) |
| 1 | 317 (32%) |
| 2 | 184 (19%) |
| 3 | 135 (14%) |
| >3 | 191 (19%) |
| Types of chronic medications (n = 1878; missing data/unclassified = 23) | |
| Cardiovascular system | 538 (29%) |
| Alimentary tract and metabolism | 316 (17%) |
| Nervous system | 270 (14%) |
| Respiratory system | 154 (8%) |
| Blood and blood-forming organs | 138 (7%) |
| Musculoskeletal system | 117 (6%) |
| Systemic hormonal preparations (sex hormones and insulin excluded) | 114 (6%) |
| Others (antineoplastic/immunomodulating agents; genito-urinary system and sex hormones; anti-infectives and antiparasitic agents for systemic use; sensory organs; dermatologicals; various) | 208 (11%) |
| COVID-19 vaccination status (n = 891; missing data = 91) | |
| Two doses | 627 (64%) |
| One dose | 115 (12%) |
| None | 149 (15%) |
| Perceived risk of COVID-19 infection due to own chronic diseases (n = 981, missing data = 1) | |
| Yes, I am at risk | 103 (10%) |
| No, I am not at risk | 315 (32%) |
| No, I am not at risk because I am vaccinated | 519 (53%) |
| I do not know | 44 (4%) |
| Perceived general health (n = 982; missing data = 0) | |
| Very good | 124 (13%) |
| Good | 551 (56%) |
| Average | 267 (27%) |
| Poor | 38 (4%) |
| Very poor | 2 (0%) |
| Perceived mental health (n = 982; missing data = 0) | |
| Very good | 242 (25%) |
| Good | 528 (54%) |
| Average | 184 (19%) |
| Poor | 25 (3%) |
| Very poor | 3 (0%) |
| Participants currently reporting … (moderate to incapacitating) (n = 982, missing data = 0) | |
| Pain/discomfort | 234 (24%) |
| Anxiety/depression | 143 (15%) |
| Performance of current activities | 85 (9%) |
| Issues with mobility | 71 (7%) |
| Issues with autonomy | 10 (1%) |
| Medication Adherence OR (CI 95%) | |||||||
|---|---|---|---|---|---|---|---|
| Average to Extreme Impact on Motivation to Take Medication (vs. Limited or No Impact) Sample Size: 708 HL Goodness of Fit (p-Val): 0.21 | Change in Medication Intake Regularity (More or Less Regularly vs. No Change) Sample Size: 691 HL Goodness of Fit (p-Val): 0.95 | Change in Medication Dosage (Increase or Decrease vs. No Change) Sample Size: 696 HL Goodness of Fit (p-Val): 0.82 | Medication Interruption or Delay Sample Size: 703 HL Goodness of Fit (p-Val): 0.73 | ||||
| Female (vs. male) | 0.96 (0.51–1.82) | 1.46 (0.76–2.80) | 1.74 (0.93–3.26) | 1.23 (0.62–2.44) | |||
| Age (continuous) | 0.97 (0.94–0.99) * | 0.96 (0.94–0.98) ** | 0.98 (0.95–1.00) * | 0.96 (0.94–0.99) * | |||
| More regular | Less regular | Increase | Decrease | Interruption | Delay | ||
| Sample size = 795 HL Goodness of fit (p-val):0.11 | Sample size: 797 HL Goodness of fit (p-val): 0.87 | Sample size: 811 HL Goodness of fit (p-val): 0.54 | |||||
| 0.99 (0.96–1.01) | 0.93 (0.89–0.96) ** | 0.98 (0.96–1.01) | 0.95 (0.92–0.98) ** | 0.94 (0.91–0.97) ** | 0.99 (0.96–1.02) | ||
| Tertiary education (vs. primary and secondary) | 0.48 (0.26–0.89) ** | 0.61 (0.33–1.10) | 0.80 (0.46–1.39) | 1.51 (0.80–2.86) | |||
| Living as a single adult (vs. living with at least one adult) | 1.20 (0.59–2.44) | 1.13 (0.56–2.29) | 1.30 (0.68–2.47) | 1.22 (0.59–2.55) | |||
| Poor to very poor general health (vs. average to very good) | 1.30 (0.42–4.07) | 0.58 (0.12–2.85) | 1.65 (0.48–5.65) | 2.64 (0.82–8.50) | |||
| Interruption | Delay | ||||||
| Sample size: 811 HL Goodness of fit (p-val): 0.54 | |||||||
| 1.94 (0.42–8.99) | 3.54 (0.99–12.60) | ||||||
| Not vaccinated against COVID-19 (vs. 1 or 2 doses) | 1.27 (0.61–2.67) | 0.50 (0.21–1.20) | 0.85 (0.40–1.82) | 1.56 (0.71–3.41) | |||
| Perceived risk of COVID-19 due to chronic disease (vs. no perceived risk) | 2.69 (1.29–5.64) * | 0.94 (0.37–2.38) | 1.03 (0.45–2.37) | 1.32 (0.56–3.16) | |||
| Taking > 3 chronic medications (vs. 3 or less) | 2.55 (1.28–5.05) ** | 1.76 (0.87–3.58) | 0.89 (0.42–1.89) | 1.51 (0.70–3.28) | |||
| Medication for the respiratory system (vs. all other medications) | 2.12 (1.04–4.32) * | 2.92 (1.49–5.72) ** | 2.33 (1.20–4.55) * | 0.67 (0.26–1.72) | |||
| More regular | Less regular | Increase | Decrease | ||||
| Sample size = 795 HL Goodness of fit (p-val):0.11 | Sample size: 797 HL Goodness of fit (p-val): 0.87 | ||||||
| 4.27 (2.11–8.63) ** | 1.09 (0.34–3.47) | 3.21 (1.63–6.32) ** | 0.72 (0.21–2.55) | ||||
| Overall Medical Care and Access to Physicians and Medication OR (CI 95%) | ||||
|---|---|---|---|---|
| Strong to Extreme Impact on Overall Medical Care (vs. Limited or No Impact) Sample Size: 695 HL Goodness of Fit (p-Val): 0.22 | Average Impact on Overall Medical Care (vs. Limited or No Impact) Sample Size: 695 HL Goodness of Fit (p-Val): 0.22 | Physician Appointments Postponed, Canceled or Conducted Less Frequently (vs. No Impact) Sample Size: 665 HL Goodness of Fit (p-Val): 0.14 | Need for Stockpiling Medications for More Than 3 Months (vs. Always Accessing Medications) Sample Size: 693 HL Goodness of Fit (p-Val): 0.38 | |
| Female (vs. male) | 0.82 (0.39–1.74) | 1.95 (1.11–3.42) * | 1.35 (0.86–2.12) | 1.50 (0.78–2.87) |
| Age (continuous) | 0.96 (0.93–0.99) ** | 0.97 (0.95–0.99) ** | 0.96 (0.95–0.98) ** | 0.97 (0.94–0.99) ** |
| Tertiary education (vs. primary and secondary) | 1.20 (0.59–2.47) | 0.66 (0.40–1.09) | 1.91 (1.23–2.96) ** | 0.96 (0.53–1.72) |
| Living as only adult (vs. living with at least one adult) | 3.73 (1.80–7.73) ** | 0.97 (0.52–1.80) | 1.46 (0.88–2.42) | 1.28 (0.65–2.54) |
| Poor to very poor general health (vs. average to very good) | 3.73 (1.11–12.52) * | 4.19 (1.55–11.35) ** | 4.10 (1.60–10.46) ** | 0.53 (0.13–2.07) |
| Not vaccinated against COVID-19 (vs. 1 or 2 doses) | 0.99 (0.37–2.62) | 0.75 (0.37–1.51) | 0.90 (0.49–1.64) | 0.76 (0.33–1.74) |
| Perceived risk of COVID-19 due to chronic disease (vs. no perceived risk) | 2.81 (1.16–6.78) * | 1.38 (0.67–2.86) | 1.75 (0.96–3.19) | 2.38 (1.13–5.02) * |
| Taking more than 3 chronic medications (vs. 3 or less) | 3.41 (1.56–7.43) ** | 2.32 (1.29–4.15) ** | 1.97 (1.16–3.35) * | 2.92 (1.50–5.64) ** |
| Medication for the respiratory system (vs. all other medications) | 1.75 (0.71–4.33) | 1.73 (0.89–3.33) | 1.29 (0.71–2.33) | 1.27 (0.58-2.75) |
| Diet OR (CI 95%) (Average to Extreme Impact) Sample Size: 380 HL Goodness of Fit (p-Val): 0.42 | Physical Activity OR (CI 95%) (Average to Extreme Impact) Sample Size: 422 HL Goodness of Fit (p-Val): 0.94 | Participation in Therapeutic Education/Patient Association Activities OR (CI 95%) Sample Size: 205 HL Goodness of Fit (p-Val): 0.94 | |
|---|---|---|---|
| Female (vs. male) | 1.04 (0.60–1.79) | 1.44 (0.95–2.18) | 1.31 (0.66–2.63) |
| Age (continuous) | 0.95 (0.93–0.97) ** | 0.97 (0.97–0.99) ** | 0.99 (0.97–1.02) |
| Tertiary education (vs. primary and secondary) | 1.31 (0.78–2.20) | 1.15 (0.76–1.73) | 0.89 (0.45–1.76) |
| Living as only adult (vs. living with at least one adult) | 0.90 (0.47–1.72) | 0.93 (0.56–1.52) | 1.06 (0.50–2.28) |
| Perceiving financial difficulties | 1.92 (0.91–4.06) | 1.48 (0.76–2.90) | 1.33 (0.45–3.95) |
| Poor to very poor general health (vs. average to very good) | 1.01 (0.30–3.43) | 3.24 (0.82–1.87) | 2.78 (0.74–10.48) |
| Not vaccinated against COVID-19 (vs. 1 or 2 doses) | 0.90 (0.42–1.91) | 0.72 (0.39–1.34) | 1.24 (0.47–3.27) |
| Perceived risk of COVID-19 due to chronic disease (vs. no perceived risk) | 2.32 (1.99–4.47) * | 1.64 (0.90–2.96) | 0.77 (0.28–2.17) |
| Taking more than 3 chronic medications (vs. 3 or less) | 1.93 (1.03–3.60) * | 1.17 (0.90–2.96) | 3.04 (1.50–6.16) ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, B.; Boulaguiem, Y.; Baysson, H.; Pullen, N.; Guessous, I.; Guerrier, S.; Stringhini, S.; Schneider, M.P. Patient-Perceived Impact of the COVID-19 Pandemic on Medication Adherence and Access to Care for Long-Term Diseases: A Cross-Sectional Online Survey. COVID 2024, 4, 191-207. https://doi.org/10.3390/covid4020015
Santos B, Boulaguiem Y, Baysson H, Pullen N, Guessous I, Guerrier S, Stringhini S, Schneider MP. Patient-Perceived Impact of the COVID-19 Pandemic on Medication Adherence and Access to Care for Long-Term Diseases: A Cross-Sectional Online Survey. COVID. 2024; 4(2):191-207. https://doi.org/10.3390/covid4020015
Chicago/Turabian StyleSantos, Beatriz, Younes Boulaguiem, Helene Baysson, Nick Pullen, Idris Guessous, Stephane Guerrier, Silvia Stringhini, and Marie P. Schneider. 2024. "Patient-Perceived Impact of the COVID-19 Pandemic on Medication Adherence and Access to Care for Long-Term Diseases: A Cross-Sectional Online Survey" COVID 4, no. 2: 191-207. https://doi.org/10.3390/covid4020015