

Extraction-Free RT-PCR Surveillance Testing and Reporting for SARS-CoV-2
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
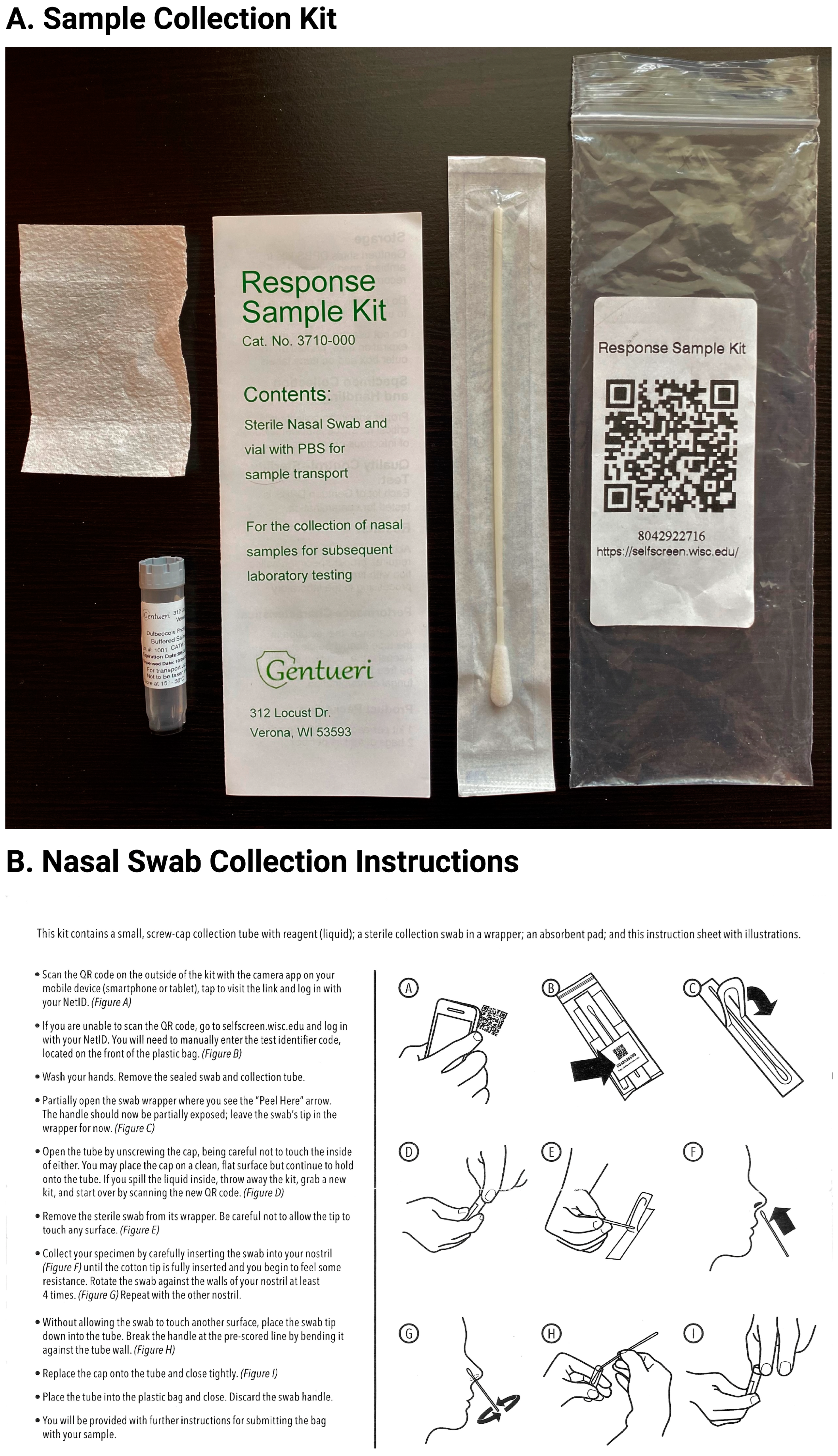
2.1. Sample Collection and Inactivation
2.2. One-Step RT-PCR
2.3. Data Analysis
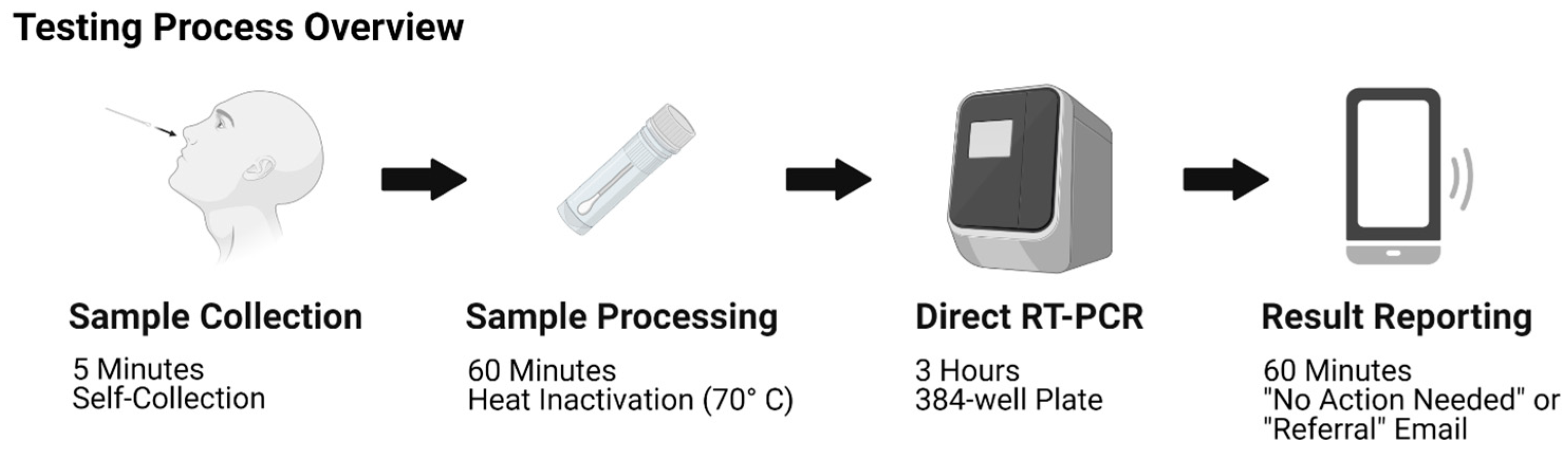
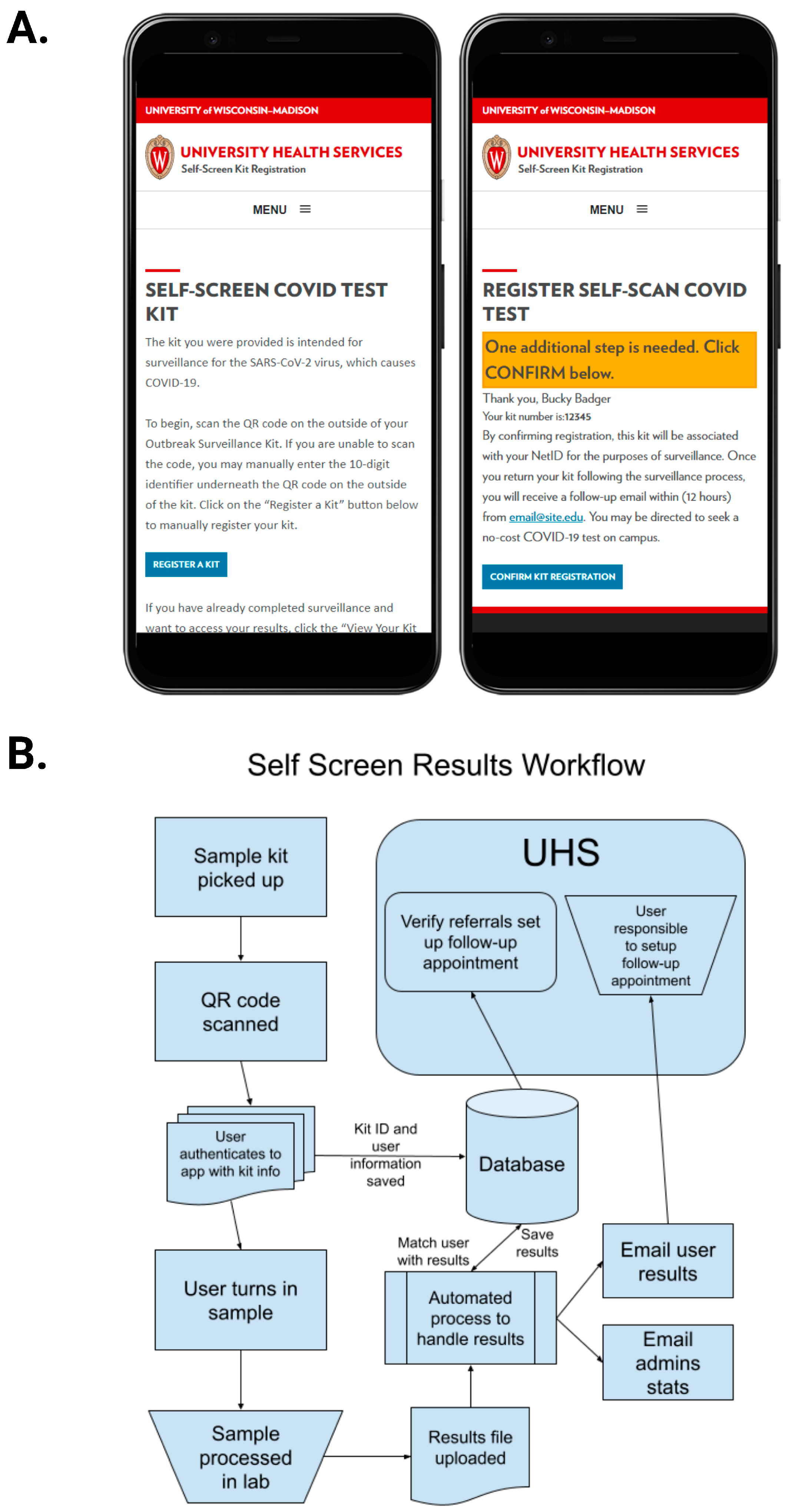
2.4. Test Kits and Testing Pipeline
3. Results
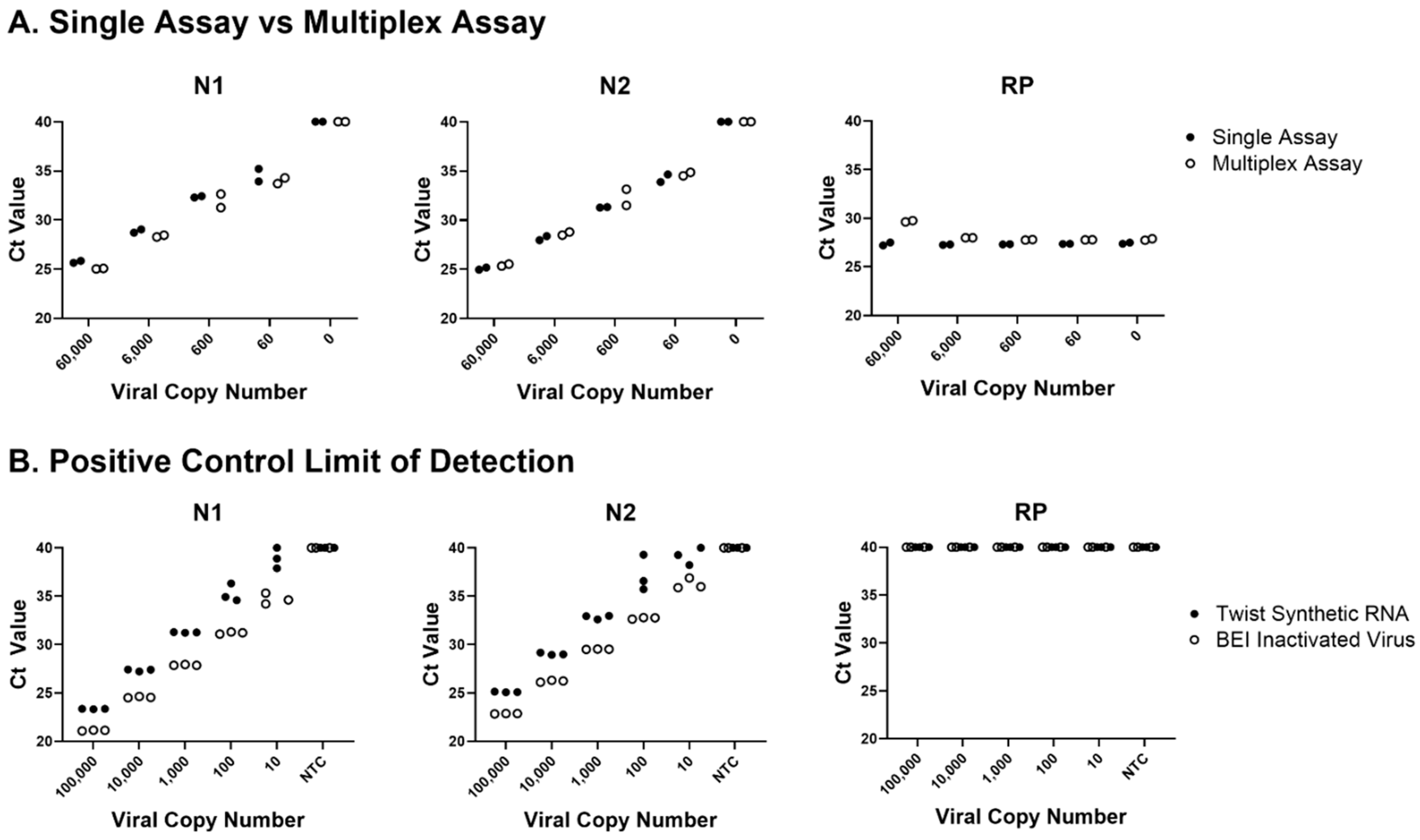
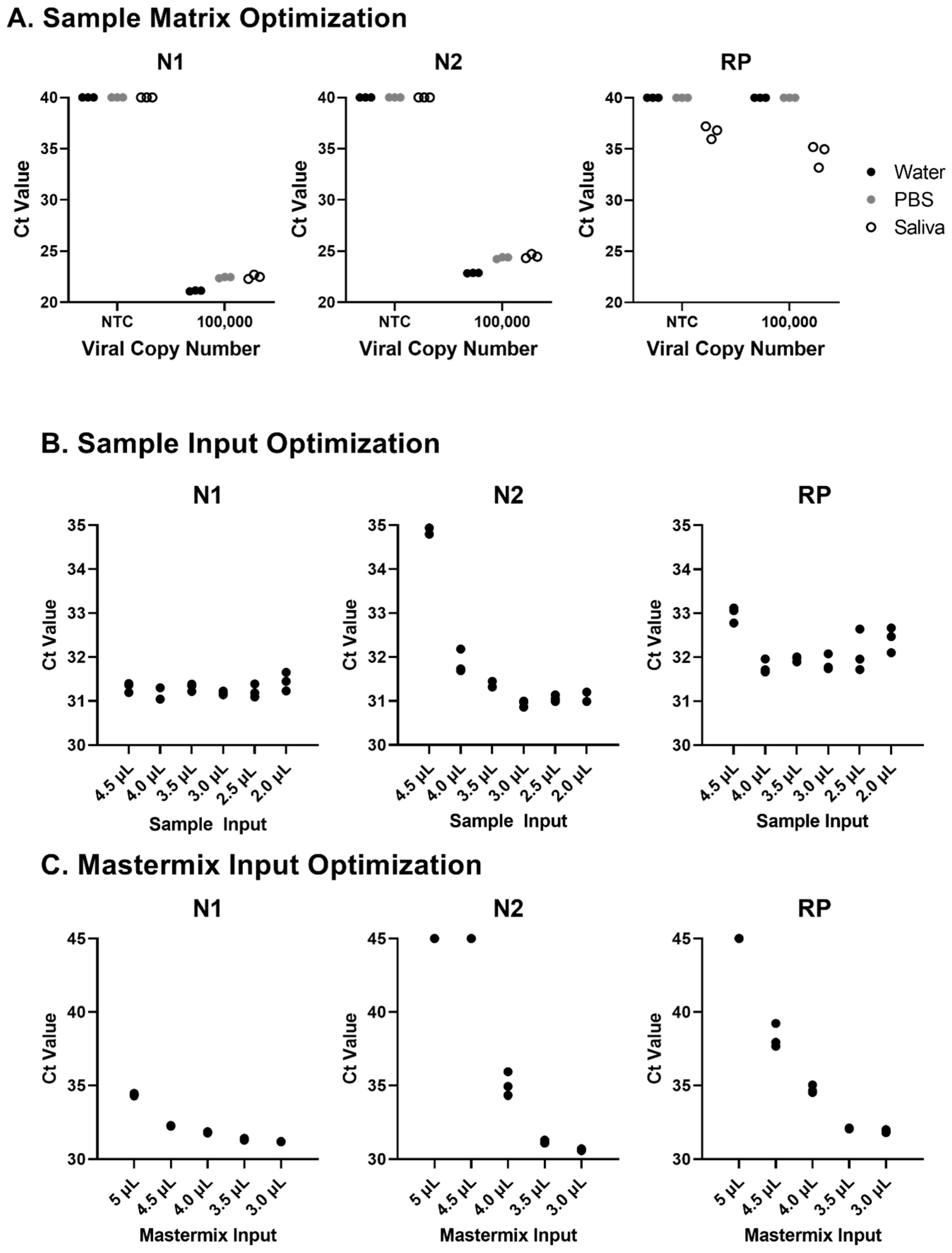
3.1. Development of a Multiplex SARS-CoV-2 qPCR Assay
3.2. Testing of Direct RT-PCR from a Nasal Swab in PBS Medium
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Naming the Coronavirus Disease (COVID-19) and the Virus That Causes It. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 21 April 2021).
- CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel. Available online: https://www.fda.gov/media/134922/download (accessed on 21 April 2021).
- Lübke, N.; Senff, T.; Scherger, S.; Hauka, S.; Andrée, M.; Adams, O.; Timm, J.; Walker, A. Extraction-free SARS-CoV-2 detection by rapid RT-qPCR universal for all primary respiratory materials. J. Clin. Virol. 2020, 130, 104579. [Google Scholar] [CrossRef] [PubMed]
- E Dumm, R.; Elkan, M.; Fink, J.; Richard-Greenblatt, M.; E Obstfeld, A.; Harris, R.M. Implementation of an Extraction-Free COVID Real-Time PCR Workflow in a Pediatric Hospital Setting. J. Appl. Lab. Med. 2021, 6, 1441–1451. [Google Scholar] [CrossRef] [PubMed]
- Smyrlaki, I.; Ekman, M.; Lentini, A.; De Sousa, N.R.; Papanicolaou, N.; Vondracek, M.; Aarum, J.; Safari, H.; Muradrasoli, S.; Rothfuchs, A.G.; et al. Massive and rapid COVID-19 testing is feasible by extraction-free SARS-CoV-2 RT-PCR. Nat. Commun. 2020, 11, 4812. [Google Scholar] [CrossRef] [PubMed]
- Srivatsan, S.; Heidl, S.; Pfau, B.; Martin, B.K.; Han, P.D.; Zhong, W.; van Raay, K.; McDermot, E.; Opsahl, J.; Gamboa, L.; et al. SwabExpress: An End-to-End Protocol for Extraction-Free COVID-19 Testing. Clin. Chem. 2021, 68, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Rödel, J.; Egerer, R.; Suleyman, A.; Sommer-Schmid, B.; Baier, M.; Henke, A.; Edel, B.; Löffler, B. Use of the variplexTM SARS-CoV-2 RT-LAMP as a rapid molecular assay to complement RT-PCR for COVID-19 diagnosis. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2020, 132, 104616. [Google Scholar] [CrossRef]
- Mohon, A.N.; Oberding, L.; Hundt, J.; van Marle, G.; Pabbaraju, K.; Berenger, B.M.; Lisboa, L.; Griener, T.; Czub, M.; Doolan, C.; et al. Optimization and clinical validation of dual-target RT-LAMP for SARS-CoV-2. J. Virol. Methods 2020, 286, 113972. [Google Scholar] [CrossRef] [PubMed]
- Thi, V.L.D.; Herbst, K.; Boerner, K.; Meurer, M.; Kremer, L.P.; Kirrmaier, D.; Freistaedter, A.; Papagiannidis, D.; Galmozzi, C.; Stanifer, M.L.; et al. A colorimetric RT-LAMP assay and LAMP-sequencing for detecting SARS-CoV-2 RNA in clinical samples. Sci. Transl. Med. 2020, 12, eabc7075. [Google Scholar] [CrossRef]
- Chen, L.; Zhang, G.; Liu, L.; Li, Z. Emerging biosensing technologies for improved diagnostics of COVID-19 and future pandemics. Talanta 2021, 225, 121986. [Google Scholar] [CrossRef] [PubMed]
- Maricic, T.; Nickel, O.; Aximu-Petri, A.; Essel, E.; Gansauge, M.; Kanis, P.; Macak, D.; Richter, J.; Riesenberg, S.; Bokelmann, L.; et al. A direct RT-qPCR approach to test large numbers of individuals for SARS-CoV-2. PLoS ONE 2020, 15, e0244824. [Google Scholar] [CrossRef] [PubMed]
- Nyaruaba, R.; Li, C.; Mwaliko, C.; Mwau, M.; Odiwuor, N.; Muturi, E.; Muema, C.; Xiong, J.; Li, J.; Yu, J.; et al. Developing multiplex ddPCR assays for SARS-CoV-2 detection based on probe mix and amplitude based multiplexing. Expert Rev. Mol. Diagn. 2021, 21, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Perez, V.P.; Pessoa, W.F.B.; Galvão, B.H.A.; Sousa, E.S.S.; Dejani, N.N.; Campana, E.H.; Cavalcanti, M.G.D.S.; Cantarelli, V.V. Evaluation of alternative RNA extraction methods for detection of SARS-CoV-2 in nasopharyngeal samples using the recommended CDC primer-probe set. J. Clin. Virol. Plus 2021, 1, 100032. [Google Scholar] [CrossRef] [PubMed]
- Dhakad, M.S.; Gogoi, S.; Kumari, A.; Singh, A.K.; Jais, M.B.; Prakash, A.; Pangtey, G.; Kaur, R. Comparative evaluation of cost effective extraction free molecular technique for detection of SARS-CoV-2 with reference to standard VTM based RT-qPCR method. Iran. J. Microbiol. 2021, 13, 748–756. [Google Scholar] [CrossRef] [PubMed]
- Stanton, J.-A.L.; O’Brien, R.; Hall, R.J.; Chernyavtseva, A.; Ha, H.J.; Jelley, L.; Mace, P.D.; Klenov, A.; Treece, J.M.; Fraser, J.D.; et al. Uncoupling Molecular Testing for SARS-CoV-2 From International Supply Chains. Front. Public Health 2022, 9, 808751. [Google Scholar] [CrossRef] [PubMed]
- Das, N.N.; Kumar, N.; Kaur, M.; Kumar, V.; Singh, D. Automated Deep Transfer Learning-Based Approach for Detection of COVID-19 Infection in Chest X-rays. Ing. Rech. Bioméd. 2022, 43, 114–119. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primer/Probe Name | Sequence (5′→3′) |
|---|---|
| 2019-nCoV_N1-FWD | GACCCCAAAATCAGCGAAAT |
| 2019-nCoV_N1-REV | TCTGGTTACTGCCAGTTGAATCTG |
| 2019-nCoV_N1-ABY | ABY-ACCCCGCATTACGTTTGGTGGACC-QSY |
| 2019-nCoV_N2-FWD | TTACAAACATTGGCCGCAAA |
| 2019-nCoV_N2-REV | GCGCGACATTCCGAAGAA |
| 2019-nCoV_N2-FAM | FAM-ACAATTTGCCCCCAGCGCTTCAG-QSY |
| RP-FWD | AGATTTGGACCTGCGAGCG |
| RP-FEV | GAGCGGCTGTCTCCACAAGT |
| RP-VIC | VIC-TTCTGACCTGAAGGCTCTGCGCG-QSY |
| Presence Targets | Absence Targets | Call | Assessment |
|---|---|---|---|
| N1, N2, RP | Presence | Referral | |
| N1 | N2, RP | Presence | Referral |
| N2 | N1, RP | Presence | Referral |
| N1, RP | N2 | Presence | Referral |
| N2, RP | N1 | Presence | Referral |
| N1, N2 | RP | Presence | Referral |
| N1, N2, RP | Inconclusive | Referral | |
| RP | N1, N2 | Absence | No Action Needed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carney, P.R.; Duellman, T.; Chan, J.-Y.; Wells, L.; Tessmer, M.; Frater-Rubsam, L.; Zeller, M.; Field, M.; Speers, J.; Tyrrell, K.; et al. Extraction-Free RT-PCR Surveillance Testing and Reporting for SARS-CoV-2. COVID 2023, 3, 1031-1041. https://doi.org/10.3390/covid3070075
Carney PR, Duellman T, Chan J-Y, Wells L, Tessmer M, Frater-Rubsam L, Zeller M, Field M, Speers J, Tyrrell K, et al. Extraction-Free RT-PCR Surveillance Testing and Reporting for SARS-CoV-2. COVID. 2023; 3(7):1031-1041. https://doi.org/10.3390/covid3070075
Chicago/Turabian StyleCarney, Patrick R., Tyler Duellman, Jia-Yi Chan, Lauren Wells, Michael Tessmer, Leah Frater-Rubsam, Molly Zeller, Mark Field, James Speers, Kelly Tyrrell, and et al. 2023. "Extraction-Free RT-PCR Surveillance Testing and Reporting for SARS-CoV-2" COVID 3, no. 7: 1031-1041. https://doi.org/10.3390/covid3070075