
An Automated Approach to Instrumenting the Up-on-the-Toes Test(s)

Abstract
:1. Introduction
2. Methods
2.1. Participant Recruitment
2.2. Protocol
- Twenty seconds of stationary standing.
- a UTT-30. Here, participants were instructed to rise-UTT as high as comfortably possible and at a comfortable speed until indicated to stop (after 30 s), ensuring the heel contacted the ground between each movement. Note, all UTT movements were accepted for later analysis.
- Twenty seconds of stationary standing.
- a UTT-stand. Here, participants were instructed to rise-UTT as fast as comfortably possible and then hold this position until indicated to “return” to normal standing (after 5 s).
- Twenty seconds of stationary standing.
2.3. Data Collection
2.4. Data Treatment and Analysis
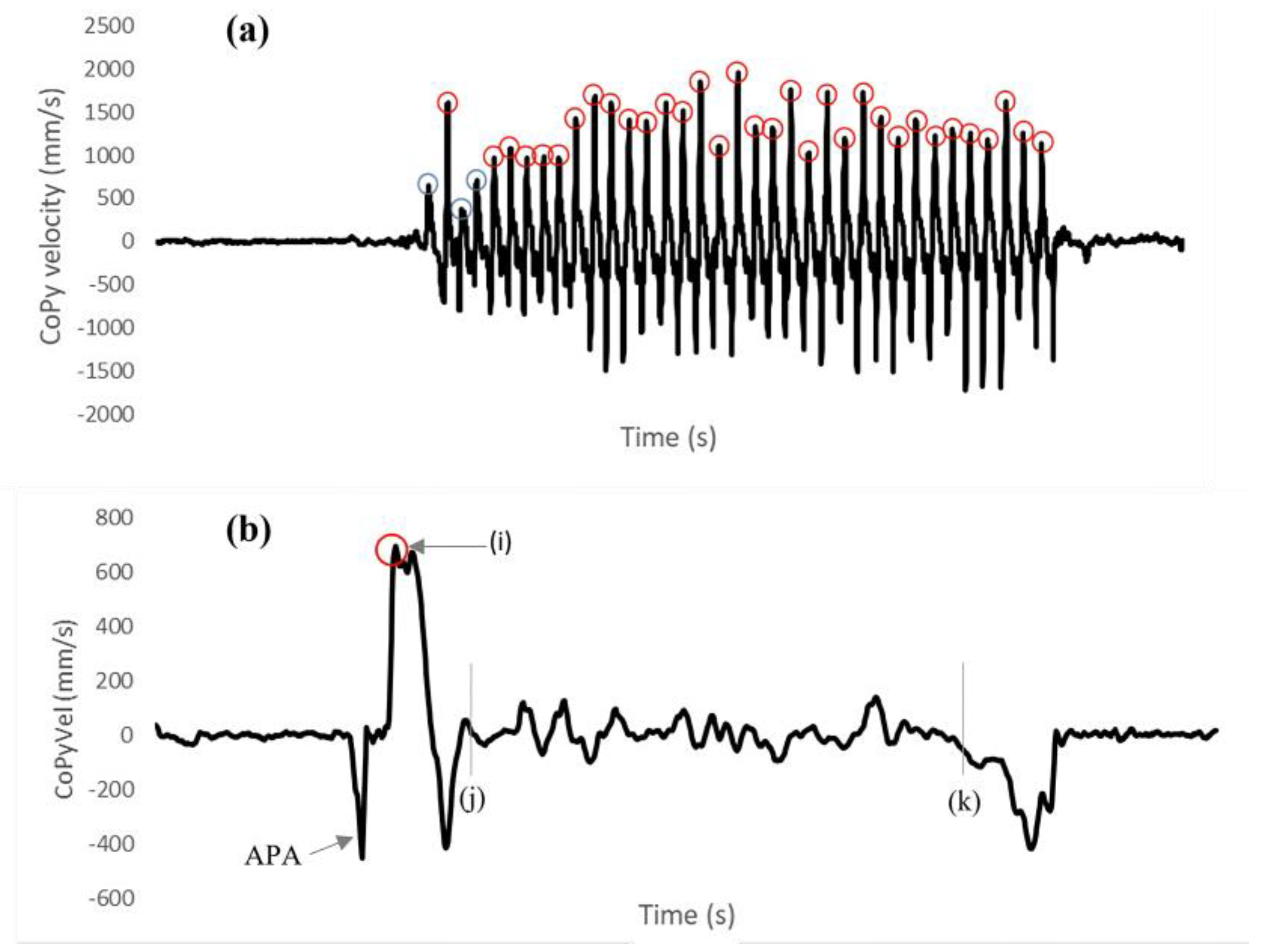
2.4.1. Forceplatform Data Analysis
UTT-30 (Figure 1a): Num. UTT Movements Completed, and Mean Peak CoPyVel
UTT-Stand (Figure 1b): Peak CoPyVel, and Peak CoPy Accel (Figure 1b)
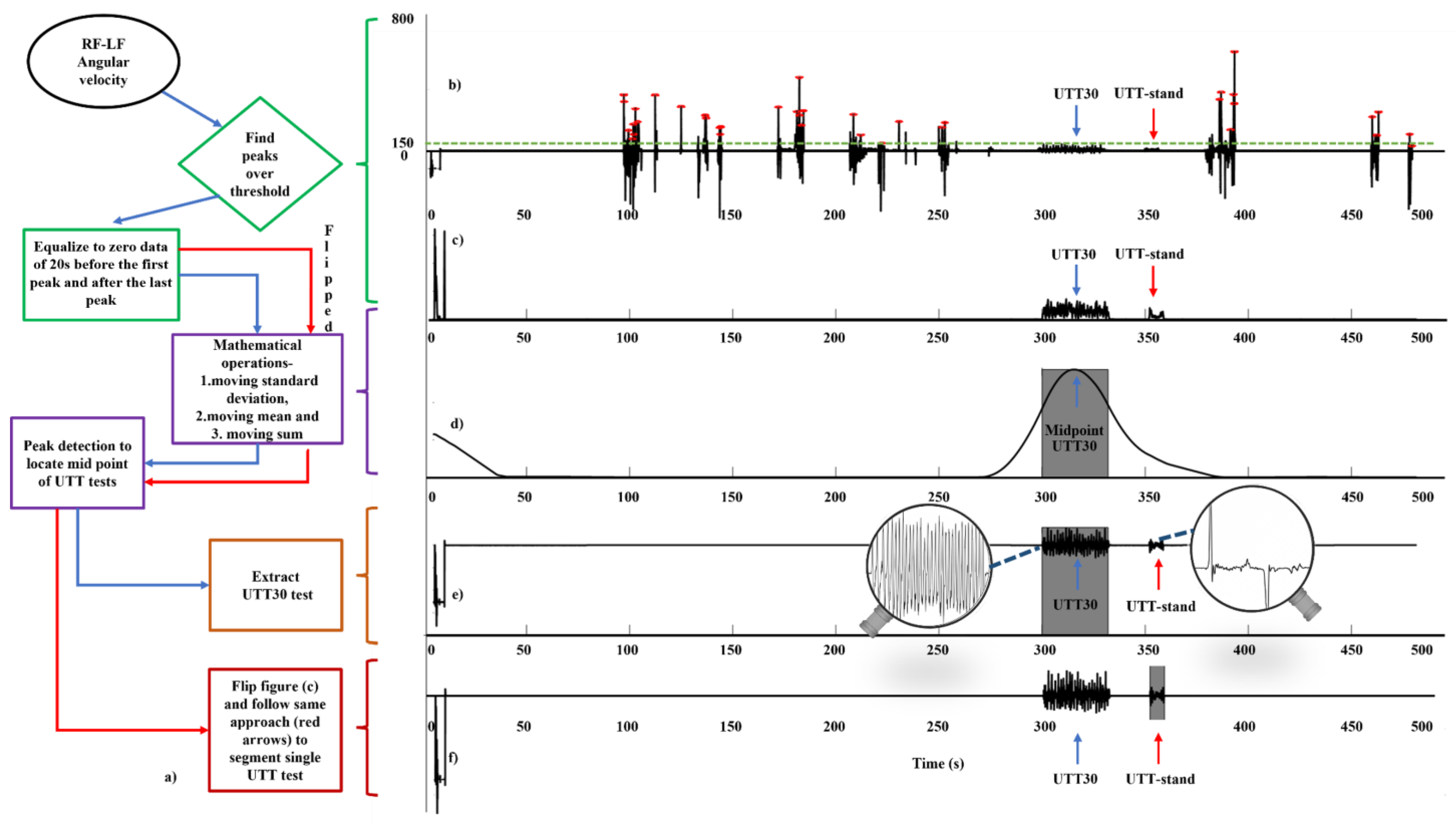
2.4.2. IMU Data Analysis
- A peak detection algorithm was used to detect the peaks (local maxima) above the 150°/s threshold.
- Data for the 20 s before the first peak and after the last peak was equalized/set to zero, i.e., the algorithm requires and makes use of periods of 20 s stationary standing before and after the UTT-30 (Figure 2c).
- Moving SD and moving mean operations with a 5 s sliding window were used to differentiate the UTT-30 from UTT-stand.
- Moving summing operations along with peak detection was used to detect the midpoint of the repeated UTT-30 (Figure 2d). The sliding window size of the moving sum operation was set to 30 s (i.e., the length of UTT-30).
- The UTT-30 was segmented considering 15 s before and after the calculated midpoint/peak location (Figure 2e).
- Once the UTT-30 was segmented, the signal was flipped in the time domain (MATLAB® ‘flipud’ function), reversing the chronological order of the data. This allowed the UTT-stand to be segmented using the same approach as described in step 3 above (e.g., moving SD, Figure 2f), with the sliding window size of the moving sum operation set to 5 s (i.e., length of a UTT-stand).
Number of Movements, and Mean Peak Foot Angular Velocity
Peak Plantarflexion Angular Velocity
Peak CoM (L5) Upwards Acceleration (When Rising to Toes)
Postural Stability Whilst Holding UTT Position
2.5. Analysis: Comparison between IMU and FP Outcomes
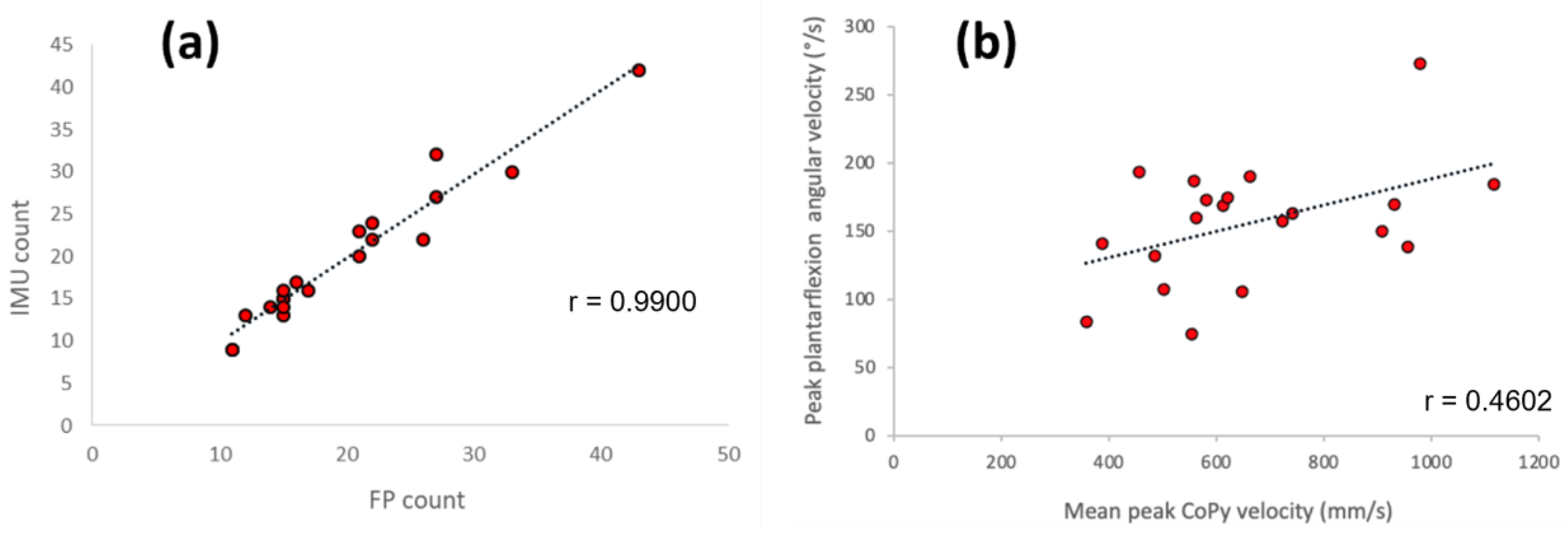
- number of fully completed UTT movements determined by IMU against number determined by FP (Figure 4a).
- the mean peak plantarflexion angular velocity against the mean peak CoPy velocity (Figure 4b).
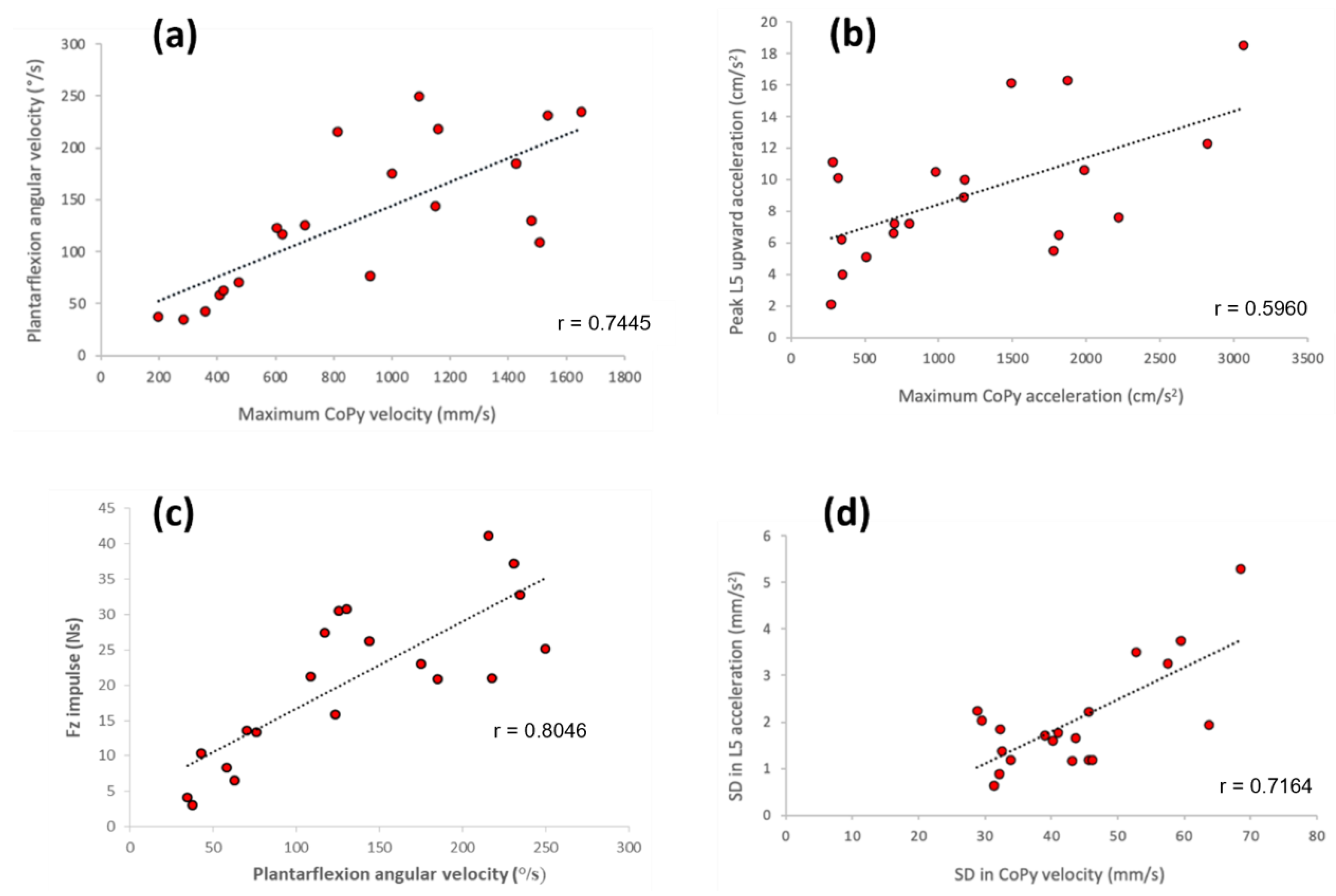
- for the period when moving UTT: peak plantarflexion angular velocity against the maximum CoPy velocity (Figure 5a); the peak L5 upward acceleration against the maximum CoPy acceleration (Figure 5b); and the peak plantarflexion angular velocity against the vertical (Fz) impulse (Figure 5c).
- for the period when holding the UTT position: the SD in L5 horizontal acceleration against the SD in CoPy velocity (Figure 5d).
3. Results
3.1. UTT-30
3.1.1. Number of Movements
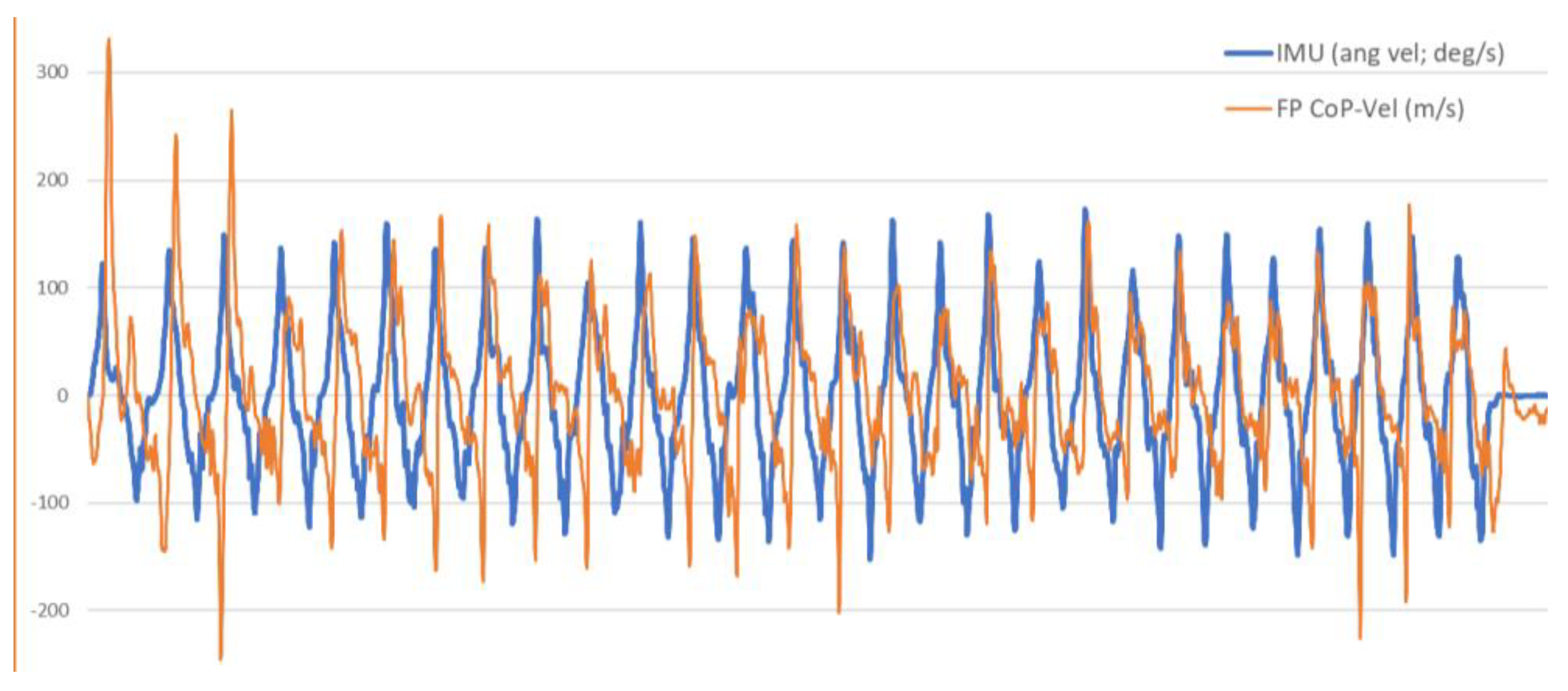
3.1.2. CoPy Velocity and Plantarflexion Angular Velocity
3.2. UTT-Stand
3.2.1. Period When Rising to the Toes
3.2.2. Period of Holding the UTT Position
4. Discussion
4.1. UTT-30
4.2. UTT-Stand
4.3. Limitations and Recommendations for Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pol, F.; Baharlouei, H.; Taheri, A.; Menz, H.B.; Forghany, S. Foot and ankle biomechanics during walking in older adults: A systematic review and meta-analysis of observational studies. Gait Posture 2021, 1, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Spink, M.J.; Fotoohabadi, M.R.; Wee, E.; Hill, K.D.; Lord, S.R.; Menz, H.B. Foot and ankle strength, range of motion, posture, and deformity are associated with balance and functional ability in older adults. Arch. Phys. Med. Rehabil. 2011, 1, 68–75. [Google Scholar] [CrossRef]
- Menz, H.B.; Morris, M.E.; Lord, S.R. Foot and Ankle Characteristics Associated with Impaired Balance and Functional Ability in Older People. J. Gerontol. Ser. A 2005, 60, 1546–1552. [Google Scholar] [CrossRef]
- Buckley, J.G.; Cooper, G.; Maganaris, C.N.; Reeves, N.D. Is stair descent in the elderly associated with periods of high centre of mass downward accelerations? Exp. Gerontol. 2013, 48, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Riener, R.; Rabuffetti, M.; Frigo, C. Stair ascent and descent at different inclinations. Gait Posture 2002, 15, 32–44. [Google Scholar] [CrossRef]
- André, H.I.; Carnide, F.; Borja, E.; Ramalho, F.; Santos-Rocha, R.; Veloso, A.P. Calf-raise senior: A new test for assessment of plantar flexor muscle strength in older adults: Protocol, validity, and reliability. Clin. Interv. Aging 2016, 11, 1661–1674. [Google Scholar] [CrossRef] [Green Version]
- Hébert-Losier, K.; Newsham-West, R.J.; Schneiders, A.G.; Sullivan, S.J. Raising the standards of the calf-raise test: A systematic review. J. Sci. Med. Sport 2009, 12, 594–602. [Google Scholar] [CrossRef] [Green Version]
- Jan, M.-H.; Chai, H.M.; Lin, Y.F.; Lin, J.C.; Tsai, L.Y.; Ou, Y.C.; Lin, D.H. Effects of age and sex on the results of an ankle plantar-flexor manual muscle test. Phys. Ther. 2005, 85, 1078–1084. [Google Scholar] [CrossRef] [Green Version]
- Lunsford, B.R.; Perry, J. The standing heel-rise test for ankle plantar flexion: Criterion for normal. Phys. Ther. 1995, 75, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Sman, A.D.; Hiller, C.E.; Imer, A.; Ocsing, A.; Burns, J.; Refshauge, K.M. Design and reliability of a novel heel rise test measuring device for plantarflexion endurance. BioMed Res. Int. 2014, 2014, 391646. [Google Scholar] [CrossRef]
- Zahid, S.A.; Celik, Y.; Godfrey, A.; Buckley, J.G. Use of ‘wearables’ to assess the Up-on-the-toes test. J. Biomech. 2022, 143, 111272. [Google Scholar] [CrossRef]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Ladha, C.; Jackson, D.; Ladha, K.; Nappey, T.; Olivier, P. Shaker table validation of OpenMovement AX3 accelerometer. In Proceedings of the Ahmerst (ICAMPAM 2013 AMHERST): 3rd International Conference on Ambulatory Monitoring of Physical Activity and Movement, Amherst, MA, USA, 17–19 June 2013. [Google Scholar]
- Github DigitalInteraction. AX3 GUI. Available online: https://github.com/digitalinteraction/openmovement/wiki/AX3-GUI (accessed on 2 December 2019).
- Taylor, R. Interpretation of the Correlation Coefficient: A Basic Review. J. Diagn. Med. Sonogr. 1990, 6, 35–39. [Google Scholar] [CrossRef]
- O’Brien, M.K.; Hidalgo-Araya, M.D.; Mummidisetty, C.K.; Vallery, H.; Ghaffari, R.; Rogers, J.A.; Lieber, R.; Jayaraman, A. Augmenting clinical outcome measures of gait and balance with a single inertial sensor in age-ranged healthy adults. Sensors 2019, 19, 4537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasegawa, N.; Maas, K.C.; Shah, V.V.; Carlson-Kuhta, P.; Nutt, J.G.; Horak, F.B.; Asaka, T.; Mancini, M. Functional limits of stability and standing balance in people with Parkinson’s disease with and without freezing of gait using wearable sensors. Gait Posture 2021, 87, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Kang, G.E.; Stout, A.; Waldon, K.; Kang, S.; Killeen, A.L.; Crisologo, P.A.; Siah, M.; Jupiter, D.; Najafi, B.; Vaziri, A.; et al. Digital Biomarkers of Gait and Balance in Diabetic Foot, Measurable by Wearable Inertial Measurement Units: A Mini Review. Sensors 2022, 22, 9278. [Google Scholar] [CrossRef] [PubMed]
- Noamani, A.; Nazarahari, M.; Lewicke, J.; Vette, A.H.; Rouhani, H. Validity of using wearable inertial sensors for assessing the dynamics of standing balance. Med. Eng. Phys. 2020, 77, 53–59. [Google Scholar] [CrossRef]
- Song, S.; Nordin, A.D. Balance Perturbations in Simulated Low-Gravity Modulate Human Premotor and Frontoparietal Electrocortical Theta, Alpha, and Beta Band Spectral Power. IEEE Open J. Eng. Med. Biol. 2023, 1–9. [Google Scholar] [CrossRef]
- Young, F.; Coulby, G.; Watson, I.; Downs, C.; Stuart, S.; Godfrey, A. Just Find It: The Mymo Approach to Recommend Running Shoes. IEEE Access 2020, 8, 109791–109800. [Google Scholar] [CrossRef]
- Celik, Y.; Powell, D.; Woo, W.L.; Stuart, S.; Godfrey, A. A feasibility study towards instrumentation of the Sport Concussion Assessment Tool (iSCAT). In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020. [Google Scholar]
- Furtado, S.; Godfrey, A.; Del Din, S.; Rochester, L.; Gerrand, C. Are Accelerometer-based Functional Outcome Assessments Feasible and Valid After Treatment for Lower Extremity Sarcomas? Clin. Orthop. Relat. Res. 2020, 478, 482–503. [Google Scholar] [CrossRef]
- Cattagni, T.; Scaglioni, G.; Laroche, D.; Grémeaux, V.; Martin, A. The involvement of ankle muscles in maintaining balance in the upright posture is higher in elderly fallers. Exp. Gerontol. 2016, 1, 38–45. [Google Scholar] [CrossRef]
- Menz, H.B.; Morris, M.E.; Lord, S.R. Foot and Ankle Risk Factors for Falls in Older People: A Prospective Study. J. Gerontol. Ser. A 2006, 61, 866–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cattagni, T.; Scaglioni, G.; Laroche, D.; Van Hoecke, J.; Gremeaux, V.; Martin, A. Ankle muscle strength discriminates fallers from non-fallers. Front. Aging Neurosci. 2014, 6, 336. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | No. UTT Counted by Observer | No of UTT Movements Detected | No of UTT Movements Detected | No. UTT Fully Completed | No. UTT Fully Completed | Mean Peak CoPyVel (mm/s) | Mean Peak p-f Angular Velocity (°/sec) |
|---|---|---|---|---|---|---|---|
| FP | IMU | FP | IMU | FP | IMU | ||
| 1 | 29 | 29 | 29 | 22 | 24 | 613.0 | 169.1 |
| 2 | 36 | 36 | 36 | 33 | 30 | 957.1 | 138.4 |
| 3 | 12 | 12 | 12 | 11 | 9 | 932.0 | 169.7 |
| 4 | 24 | 24 | 24 | 22 | 22 | 563.4 | 159.9 |
| 5 | 36 | 36 | 36 | 27 | 32 | 980.6 | 272.7 |
| 6 | 31 | 31 | 31 | 27 | 27 | 456.0 | 193.4 |
| 7 | 19 | 19 | 19 | 16 | 17 | 663.2 | 189.7 |
| 8 | 28 | 28 | 28 | 26 | 22 | 559.7 | 186.8 |
| 9 | 21 | 21 | 21 | 17 | 16 | 741.6 | 163.1 |
| 10 | 23 | 23 | 23 | 21 | 20 | 388.2 | 140.5 |
| 11 | 26 | 26 | 26 | 21 | 23 | 1116.6 | 183.9 |
| 12 | 18 | 18 | 18 | 15 | 15 | 581.7 | 172.4 |
| 13 | 17 | 17 | 17 | 14 | 14 | 647.3 | 105.5 |
| 14 | 12 | 12 | 12 | 11 | 9 | 358.5 | 83.1 |
| 15 | 18 | 18 | 18 | 15 | 15 | 485.6 | 131.5 |
| 16 | 15 | 15 | 15 | 12 | 13 | 503.0 | 106.9 |
| 17 | 18 | 18 | 18 | 15 | 16 | 724.0 | 157.1 |
| 18 | 17 | 17 | 16 | 15 | 13 | 555.4 | 74.3 |
| 19 | 19 | 19 | 19 | 15 | 14 | 908.5 | 149.9 |
| 20 | 52 | 52 | 52 | 43 | 42 | 621.9 | 174.7 |
| Mean ± SD | 23.6 ± 9.7 | 23.6 ± 9.7 | 23.5 ± 9.8 | 19.9 ± 8.1 | 19.7 ± 8.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zahid, S.A.; Celik, Y.; Godfrey, A.; Buckley, J.G. An Automated Approach to Instrumenting the Up-on-the-Toes Test(s). Biomechanics 2023, 3, 278-290. https://doi.org/10.3390/biomechanics3030024
Zahid SA, Celik Y, Godfrey A, Buckley JG. An Automated Approach to Instrumenting the Up-on-the-Toes Test(s). Biomechanics. 2023; 3(3):278-290. https://doi.org/10.3390/biomechanics3030024
Chicago/Turabian StyleZahid, Sarah Aruje, Yunus Celik, Alan Godfrey, and John G. Buckley. 2023. "An Automated Approach to Instrumenting the Up-on-the-Toes Test(s)" Biomechanics 3, no. 3: 278-290. https://doi.org/10.3390/biomechanics3030024