
Biobanks: Archives or Resources? Their Secondary Use for Forensic Purposes—A Systematic Review

Abstract
:1. Introduction
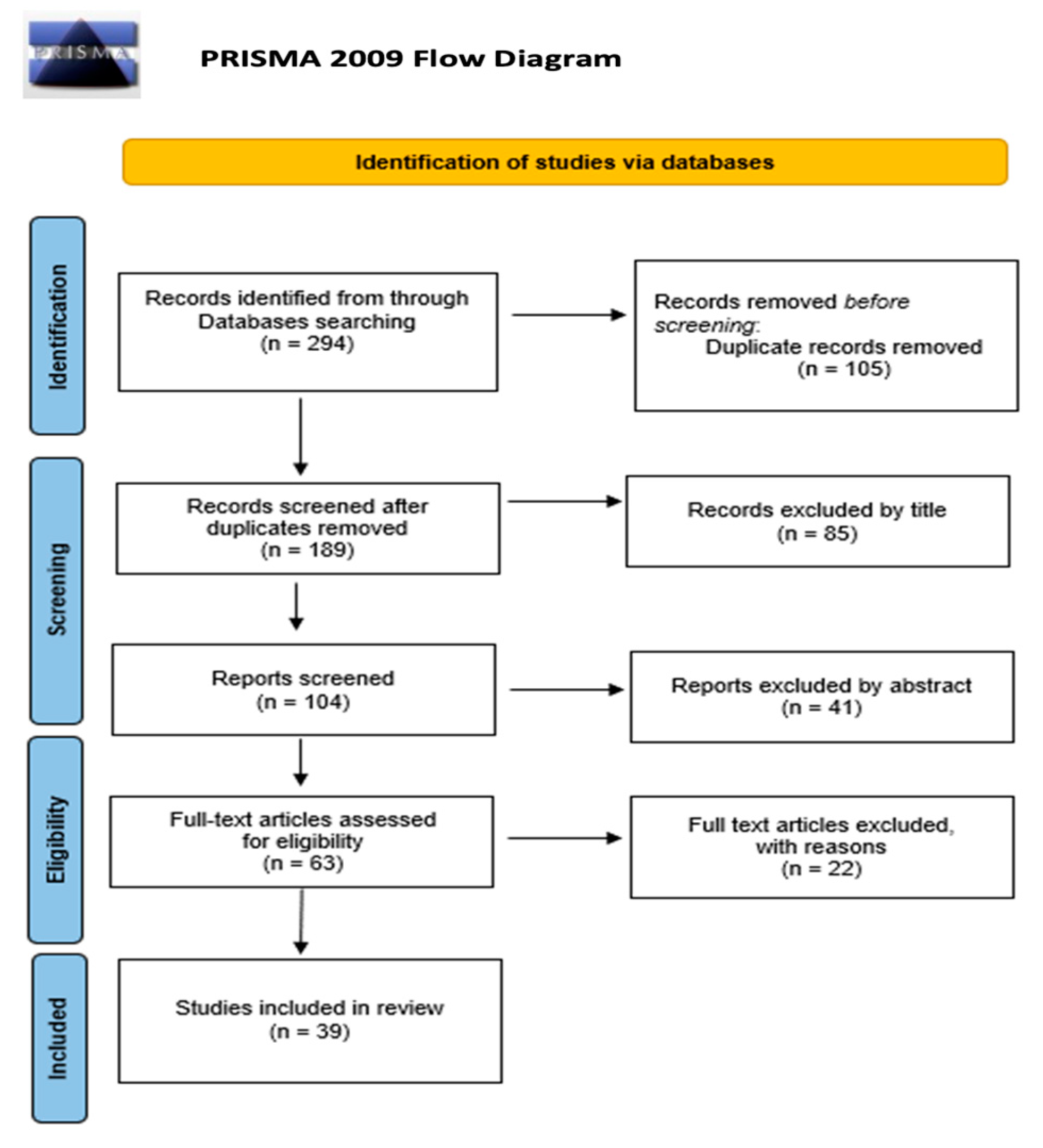
2. Materials and Methods
3. Results
3.1. Forensic Biobanks
- Forensic databases, totally separated from medical biobanks, where the biological material is gathered from suspects, convicted felons, victims, and other persons involved in the criminal investigation [10,11]. In the work of Machado and Silva in 2015, European countries are distinguished based on the criteria of inclusion of profiles in databases. The authors indicate countries with legislation having expansive effects (Austria, Denmark, Estonia, Finland, Latvia, Lithuania, Scotland, Slovakia, and England and Wales) and countries with legislation having restrictive effects (Belgium, France, Germany, Hungary, Ireland, Italy, Luxemburg, The Netherlands, Poland, Portugal, Romania, Spain, and Sweden). In the first group, the inclusion criteria allow samples to be taken from individuals suspected of any crime. In the second group, however, the condition generally imposed for the inclusion of profiles in databases is that an individual is suspected or convicted of a crime that involves a prison sentence or the crimes committed are considered serious [11];
- Forensic databases created by enlarging the area of application of existing medical biobanks. In this case, the biobank population is represented by all those who voluntarily agree to contribute to a sample [10];
- Forensic databases, as (2) previously stated, but containing also all the genetic information from newborns collected at birth for medical research purposes, with or without any explicit statement precluding forensic uses. Also, in this case, sample collection is voluntary, subject to the consent of parents or legal representatives [10].
3.2. Potential Use of Biobanks for Forensic and Research Purposes
3.3. Risks and Problems Related to Forensic Biobanks

{kind=link}
| Risks and Problems Related to Forensic Biobanks | |
|---|---|
| Discrimination against certain social groups | |
| Tozzo and Caenazzo, 2020 [6] Dhai and Mahomed, 2013 [9] Tamburrini, 2011 [10] Machado and Silva, 2015 [11] Bak et al., 2020 [39] Bathe and McGuire, 2009 [40] Cambon-Thomsen et al., 2007 [41] | Social risks include stigmatization and discrimination. Data might be associated with individual or group characteristics, criminal behavior, or medical conditions. Stored information turns into a registry of a particular social group since criminals often come from certain social categories. After all, when in a biobank, the percentage of patients is over-represented compared to that of healthy individuals, the access of the police to it can be targeted at patients. |
| Abuse of control and violation of privacy | |
| Paris, 2022 [3] Tozzo and Caenazzo, 2020 [6] Wiskott et al., 2022 [34] Norlin et al., 2012 [42] Tamburrini, 2011 [10] Machado and Silva, 2015 [11] Caenazzo and Tozzo, 2021 [13] Dranseika et al., 2016 [30] De Groot et al., 2021 [31] Bathe and McGuire, 2009 [40] Cambon-Thomsen et al., 2007 [41] Virani and Longstaff, 2015 [43] Kurihara et al., 2020 [44] | Nowadays, the concept of confidentiality extends to data privacy, data sharing and secondary use of samples, informed consent, sample ownership, and the benefit of sharing. This includes both the physical and psychological integrity of a person. Anonymization is proposed as a solution to privacy issues; although, this is never entirely possible. Plus, anonymization techniques significantly hinder the progress of scientific research. |
| Post-mortem use of biomaterial | |
| Moraia et al., 2014 [7] Dhai and Mahomed, 2013 [9] Tassé, 2011 [19] Wiskott et al., 2022 [34] De Groot et al., 2021 [31] Bak et al., 2020 [39] Hanold et al., 2017 [45] Tassé et al., 2010 [46] | The ethical question that governs biomedical research is addressed, also, when it involves participants’ deaths. Even if samples and data have been collected prior to the death of the participant with valid consent, this raises ethical and legal issues since genetic research has an impact, also, on family members. The authors questioned whether the post-mortem use and sharing of identifiable research data were ethically permissible at all. When consent from a deceased persons is missing, guidelines are not always clear for the research activity and do not consider the impact of a secondary use on the biological family of the deceased. |
| Informed consent open to biomaterials’ secondary uses | |
| Paris, 2022 [3] Tozzo et al., 2010 [4] Moraia et al., 2014 [7] Dhaia and Mohamed, 2013 [9] Tassé, 2010 [19] Jahns et al., 2019 [24] Machado and Silva, 2015 [11] De Groot et al., 2021 [31] Cambon-Thomsen et al., 2007 [41] Virani et al., 2015 [43] Kurihara et al., 2020 [44] Hanold et al., 2017 [45] Tassé et al., 2010 [46] Warner et al., 2018 [47] Caufield et al., Mungwira et al., 2015 [48] Chen et al., 2005 [49] Kondylakis et al., 2017 [50] Gefenas et al., 2022 [51] Moodley et al., 2014 [52] Staunton et al., 2013 [53] | Informed consent allows individuals to exercise their fundamental right to decide whether and how their body, body parts, and associated data will be used in research. Analyzing the various types of informed consent available to date, it is evident that well-drafted consent must consider: (a) the possibility of contacting the child upon reaching a legal mutual; (b) the death of the donor; and (c) the secondary use of samples and data. Since a study could be carried out several years after sample collection and it might use research topics and techniques that were unimaginable at the time, it should be determined in what way these can be considered in the consent given at the time of the first data collection. Also, restrictions to certain secondary uses should be shown and permitted to be chosen by the person involved. |
3.3.1. Discrimination against Certain Social Groups
3.3.2. Abuse of Control and Violation of Privacy
3.3.3. Post-Mortem Use of Biomaterial
3.3.4. Informed Consent Opens up the Secondary Use of Biobank Material for Forensic Research Purposes
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Park, A. Biobanks-10 Ideas Changing the World Right Now-Printout—TIME. 2009. Available online: https://content.time.com/time/specials/packages/printout/0,29239,1884779_1884782_1884766,00.html (accessed on 16 January 2024).
- Balanovska, E.V.; Zhabagin, M.K.; Agdzhoyan, A.T.; Chukhryaeva, M.I.; Markina, N.V.; Balaganskaya, O.A.; Skhalyakho, R.A.; Yusupov, Y.M.; Utevska, O.M.; Bogunov, Y.V.; et al. Population biobanks: Organizational models and prospects of application in gene geography and personalized medicine. Russ. J. Genet. 2016, 52, 1227–1243. [Google Scholar] [CrossRef]
- Paris, C. Biobanche di ricerca e banca dati nazionale del DNA: Un difficile bilanciamento tra interessi contrapposti. BioLaw J. 2022, 2022, 83–106. [Google Scholar]
- Tozzo, P.; Pegoraro, R.; Caenazzo, L. Biobanks for non-clinical purposes and the new law on forensic biobanks: Does the Italian context protect the rights of minors? J. Med. Ethics. 2010, 36, 775–778. [Google Scholar] [CrossRef] [PubMed]
- Haga, S.B.; Beskow, L.M. Ethical, Legal, and Social Implications of Biobanks for Genetics Research. Adv. Genet. 2008, 60, 505–544. [Google Scholar] [CrossRef] [PubMed]
- Tozzo, P.; Caenazzo, L. The skeleton in the closet: Faults and strengths of public versus private genetic biobanks. Biomolecules 2020, 1–9, 1273. [Google Scholar] [CrossRef] [PubMed]
- Moraia, L.B.; Kaye, J.; Tasse, A.M.; Knoppers, B.M.; Mitchell, C.; Soini, S.; Hoppe, N.; Wallace, S.E.; Øien, M. A comparative analysis of the requirements for the use of data in biobanks based in Finland, Germany, the Netherlands, Norway and the United Kingdom. Med. Law Int. 2014, 14, 187–212. [Google Scholar] [CrossRef]
- Vaught, J.; Kelly, A.; Hewitt, R. A Review of International Biobanks and Networks: Success Factors and Key Benchmarks. Biopreserv. Biobank. 2009, 7, 143. [Google Scholar] [CrossRef]
- Dhai, A.; Mahomed, S. Biobank research: Time for discussion and debate. S. Afr. Med. J. 2013, 103, 225–227. [Google Scholar] [CrossRef]
- Tamburrini, C. What’s Wrong with Forensic Uses of Biobanks? Int. Libr. Ethics Law Technol. 2011, 8, 127–140. [Google Scholar] [CrossRef]
- Machado, H.; Silva, S. Public participation in genetic databases: Crossing the boundaries between biobanks and forensic DNA databases through the principle of solidarity. Law Ethics Med. 2015, 41, 820–824. [Google Scholar] [CrossRef]
- Liu, A.; Pollard, K. Biobanking for personalized medicine. Biobanking 21st Century 2015, 864, 55–68. [Google Scholar] [CrossRef]
- Caenazzo, L.; Tozzo, P. Microbiome forensic biobanking: A step toward microbial profiling for forensic human identification. Healthcare 2021, 9, 1371. [Google Scholar] [CrossRef]
- Mahomed, S. Human Biobanking in Developed and Developing Countries: An Ethico-Legal Comparative Analysis of the Frameworks in the United Kingdom, Australia, Uganda, and South Africa. Camb. Q. Healthc. Ethics 2020, 30, 146–160. [Google Scholar] [CrossRef]
- International ethical guidelines for biomedical research involving human subjects. Bull. Med. Ethics 2002, 182, 17–23.
- WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects—WMA—The World Medical Association, (n.d.). Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 27 September 2023).
- Declaration of Taipei—WMA—The World Medical Association, (n.d.). Available online: https://www.wma.net/what-we-do/medical-ethics/declaration-of-taipei/ (accessed on 27 September 2023).
- International Declaration on Human Genetic Data|UNESCO, (n.d.). Available online: https://www.unesco.org/en/ethics-science-technology/human-genetic-data (accessed on 17 January 2024).
- Tassé, A.M. Biobanking and deceased persons. Hum. Genet. 2011, 130, 415–423. [Google Scholar] [CrossRef]
- Coppola, L.; Cianflone, A.; Grimaldi, A.M.; Incoronato, M.; Bevilacqua, P.; Messina, F.; Baselice, S.; Soricelli, A.; Mirabelli, P.; Salvatore, M. Biobanking in health care: Evolution and future directions. J. Transl. Med. 2019, 17, 172. [Google Scholar] [CrossRef]
- Caenazzo, L.; Tozzo, P. The Future of Biobanking: What Is Next? (n.d.). BioTech 2020, 9, 23. [Google Scholar] [CrossRef]
- Barnes, R.O.; Watson, P.H. Precision medicine: Driving the evolution of biobanking quality. Health Manag. Forum 2020, 33, 102–106. [Google Scholar] [CrossRef]
- Tozzo, P.; Angiola, F.; Caenazzo, L. Letter to the Editor. Progress in morgues: The time has come for a wide network of forensic research biobanks. Int. J. Legal Med. 2021, 135, 2135–2137. [Google Scholar] [CrossRef] [PubMed]
- Jahns, R.; Geiger, J.; Schlünder, I.; Strech, D.; Brumhard, M.; Von Kielmansegg, S.G. Broad donor consent for human biobanks in Germany and Europe: A strategy to facilitate cross-border sharing and exchange of human biological materials and related data. J. Lab. Med. 2019, 43, 291–299. [Google Scholar] [CrossRef]
- Toom, V. Cross-Border Exchange and Comparison of Forensic DNA Data in the Context of the Prüm Decision. Study of the Directorate General for Internal Policies. Policy Department for Citizens’ Rights and Constitutional Affaris. 2018. Available online: https://www.researchgate.net/profile/Victor-Toom/publication/327467541_Cross-border_exchange_and_comparison_of_forensic_DNA_data_in_the_context_of_the_Prum_Decision/links/5b90f298299bf114b7feb836/Cross-border-exchange-and-comparison-of-forensic-DNA-data-in-the-context-of-the-Pruem-Decision.pdf (accessed on 1 October 2023).
- Aaron, R.; Aaron, D.; Racine-Avila, J.; Menikoff, J. The use of human biospecimens for research. J. Orthop. Res. 2021, 39, 1603–1610. [Google Scholar] [CrossRef] [PubMed]
- Vaught, J. Biobanking Comes of Age: The Transition to Biospecimen Science Introduction: Origins of Biobanks. Annu. Rev. Pharmacol. Toxicol. 2016, 56, 211–239. [Google Scholar] [CrossRef] [PubMed]
- Schneider, P.M.; Martin, P.D. Criminal DNA databases: The European situation. Forensic Sci. Int. 2001, 119, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Bexelius, C.; Hoeyer, K.; Lynöe, N. Will forensic use of medical biobanks decrease public trust in healthcare services? Some empirical observations. Scand. J. Public Health 2007, 35, 442–444. [Google Scholar] [CrossRef] [PubMed]
- Dranseika, V.; Piasecki, J.; Waligora, M. Forensic uses of research biobanks: Should donors be informed? Med. Health Care Philos. 2016, 19, 141–146. [Google Scholar] [CrossRef] [PubMed]
- De Groot, N.F.; Van Beers, B.C.; Decock, L.; Meynen, G. Accessing medical biobanks to solve crimes: Ethical considerations. J. Med. Ethics 2021, 47, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Levitt, M. Forensic databases: Benefits and ethical and social costs. Br. Med. Bull. 2007, 83, 235–248. [Google Scholar] [CrossRef] [PubMed]
- Hartman, D.; Benton, L.; Morenos, L.; Beyer, J.; Spiden, M.; Stock, A. The importance of Guthrie cards and other medical samples for the direct matching of disaster victims using DNA profiling. Forensic Sci. Int. 2011, 205, 59–63. [Google Scholar] [CrossRef]
- Wiskott, K.; Gilardi, F.; Michaud, K.; Augsburger, M.; Castiglioni, C.; Carminati, A.; Grabherr, S.; Thomas, A.; Fracasso, T. Creation of a Forensic Pathology Biobank in Switzerland: Which issues and research opportunities? Int. J. Legal Med. 2022, 136, 919–922. [Google Scholar] [CrossRef]
- van Deventer, B.S.; Toit-Prinsloo, L.D.; van Niekerk, C. Practical tips to using formalin-fixed paraffin-embedded tissue archives for molecular diagnostics in a South African setting. Afr. J. Lab. Med. 2022, 11, 6. [Google Scholar] [CrossRef]
- Metcalf, J.L.; Xu, Z.Z.; Bouslimani, A.; Dorrestein, P.; Carter, D.O.; Knight, R. Microbiome Tools for Forensic Science. Trends Biotechnol. 2017, 35, 814–823. [Google Scholar] [CrossRef]
- Sguazzi, G.; Mickleburgh, H.L.; Ghignone, S.; Voyron, S.; Renò, F.; Migliario, M.; Sellitto, F.; Lovisolo, F.; Camurani, G.; Ogbanga, N.; et al. Microbial DNA in human nucleic acid extracts: Recoverability of the microbiome in DNA extracts stored frozen long-term and its potential and ethical implications for forensic investigation. Forensic Sci. Int. Genet. 2022, 59, 102686. [Google Scholar] [CrossRef]
- Lovisolo, F.; Ogbanga, N.; Sguazzi, G.; Renò, F.; Migliario, M.; Nelson, A.; Procopio, N.; Gino, S. Oral and Skin Microbiome as Potential Tools in Forensic Field. Forensic Sci. Int. Genet. Suppl. Ser. 2022, 8, 65–67. [Google Scholar] [CrossRef]
- Bak, M.A.R.; Ploem, M.C.; Ateşyürek, H.; Blom, M.T.; Tan, H.L.; Willems, D.L. Stakeholders’ perspectives on the post-mortem use of genetic and health-related data for research: A systematic review. Eur. J. Hum. Genet. 2020, 28, 403–416. [Google Scholar] [CrossRef]
- Bathe, O.F.; McGuire, A.L. The ethical use of existing samples for genome research. Genet. Med. 2009, 11, 712–715. [Google Scholar] [CrossRef]
- Cambon-Thomsen, A.; Rial-Sebbag, E.; Knoppers, B.M. Trends in ethical and legal frameworks for the use of human biobanks. Eur. Respir. J. 2007, 30, 373–382. [Google Scholar] [CrossRef]
- Norlin, L.; Fransson, M.; Eaker, S.; Elinder, G.; Litton, J.E. Adapting research to the 21st century—The Swedish Biobank Register. Nor. Epidemiol. 2012, 21, 149–153. [Google Scholar] [CrossRef]
- Virani, A.H.; Longstaff, H. Ethical Considerations in Biobanks: How a Public Health Ethics Perspective Sheds New Light on Old Controversies. J. Genet. Couns. 2015, 24, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Kurihara, C.; Baroutsou, V.; Becker, S.; Brun, J.; Franke-Bray, B.; Carlesi, R.; Chan, A.; Collia, L.F.; Kleist, P.; Laranjeira, L.F.; et al. Linking the Declarations of Helsinki and of Taipei: Critical Challenges of Future-Oriented Research Ethics. Front. Pharmacol. 2020, 11, 1692. [Google Scholar] [CrossRef] [PubMed]
- Hänold, S.; Forgó, N.; Kobeissi, D.; Nwankwo, I. Legal Perspectives on Post-mortem Use of Biomaterial and Data for Research: A Focus on the German Situation. Eur. J. Health Law 2017, 24, 311–327. [Google Scholar] [CrossRef]
- Tassé, A.M.; Budin-Ljøsne, I.; Knoppers, B.M.; Harris, J.R. Retrospective access to data: The ENGAGE consent experience. Eur. J. Hum. Genet. 2010, 18, 741–745. [Google Scholar] [CrossRef]
- Warner, T.D.; Weil, C.J.; Andry, C.; Degenholtz, H.B.; Parker, L.; Carithers, L.J.; Feige, M.; Wendler, D.; Pentz, R.D.; Warner, D. Broad Consent for Research on Biospecimens: The Views of Actual Donors at Four U.S. Medical Centers HHS Public Access. J. Empir. Res. Hum. Res. Ethics 2018, 13, 115–124. [Google Scholar] [CrossRef]
- Mungwira, R.G.; Nyangulu, W.; Misiri, J.; Iphani, S.; Ng’Ong’Ola, R.; Chirambo, C.M.; Masiye, F.; Mfutso-Bengo, J. Is it ethical to prevent secondary use of stored biological samples and data derived from consenting research participants? The case of Malawi Ethics in Public Health, medical law, and health policy. BMC Med. Ethics 2015, 16, 83. [Google Scholar] [CrossRef]
- Chen, D.T.; Rosenstein, D.L.; Muthappan, P.; Hilsenbeck, S.G.; Miller, F.G.; Emanuel, E.J.; Wendler, D. Research with Stored Biological Samples. Arch. Intern. Med. 2005, 165, 652. [Google Scholar] [CrossRef]
- Kondylakis, H.; Koumakis, L.; Hänold, S.; Nwankwo, I.; Forgó, N.; Marias, K.; Tsiknakis, M.; Graf, N. Donor’s support tool: Enabling informed secondary use of patient’s biomaterial and personal data. Int. J. Med. Inform. 2017, 97, 282–292. [Google Scholar] [CrossRef]
- Gefenas, E.; Lekstutiene, J.; Lukaseviciene, V.; Hartlev, M.; Mourby, M.; Cathaoir, K. Controversies between regulations of research ethics and protection of personal data: Informed consent at a cross-road. Med. Heal. Care Philos. 2022, 25, 23–30. [Google Scholar] [CrossRef]
- Moodley, K.; Sibanda, N.; February, K.; Rossouw, T. It’s my blood: Ethical complexities in the use, storage and export of biological samples: Perspectives from South African research participants. BMC Med. Ethics 2014, 15, 4. [Google Scholar] [CrossRef]
- Staunton, C.; Moodley, K. Challenges in biobank governance in Sub-Saharan Africa. BMC Med. Ethics 2013, 14, 35. [Google Scholar] [CrossRef] [PubMed]
- European Convention on Human Rights—ECHR Official Texts—ECHR-ECHR/CEDH, (n.d.). Available online: https://www.echr.coe.int/european-convention-on-human-rights (accessed on 27 September 2023).
- European Commission, Directorate-General for Research and Innovation,. Biobanks for Europe: A Challenge for Governance, Luxemboutg: Publications Office of the European Union 2012. Available online: https://data.europa.eu/doi/10.2777/68942 (accessed on 27 September 2023).
- Universal Declaration on the Human Genome and Human Rights|OHCHR, (n.d.). Available online: https://www.ohchr.org/en/instruments-mechanisms/instruments/universal-declaration-human-genome-and-human-rights (accessed on 3 October 2023).
- Laurie, G. Genetic databases: Assessing the benefits and the impact on human and patient rights—A WHO report. Eur. J. Health Law 2004, 11, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for Human Biobanks and Genetic Research Databases (HBGRDs)—OECD, (n.d.). Available online: https://www.oecd.org/sti/emerging-tech/guidelines-for-human-biobanks-and-genetic-research-databases.htm (accessed on 27 September 2023).
- Caulfield, T.; Upshur, R.E.G.; Daar, A. DNA databanks and consent: A suggested policy option involving an authorization model. BMC Med. Ethics 2003, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Gazzetta Ufficiale della Repubblica Italiana, DECRETO LEGISLATIVO 30 Giugno 2003, n.196 Recante il “Codice in Materia di Protezione dei Dati Personali,” (n.d.). Available online: https://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario?atto.dataPubblicazioneGazzetta=2003-07-29&atto.codiceRedazionale=003G0218 (accessed on 4 October 2023).
- Autorizzazione n. 9/2016—Autorizzazione Generale al Trattamento dei...-Garante Privacy, (n.d.). Available online: https://www.garanteprivacy.it/home/docweb/-/docweb-display/docweb/5805552 (accessed on 4 October 2023).
- GDPR—Regolamento Generale sulla Protezione dei dati, (n.d.). Available online: https://www.altalex.com/documents/codici-altalex/2018/03/05/regolamento-generale-sulla-protezione-dei-dati-gdpr (accessed on 4 October 2023).
- National Health Act 61 of 2003|South African Government, (n.d.). Available online: https://www.gov.za/documents/national-health-act (accessed on 1 October 2023).
- Goldenberg, A.J.; Maschke, K.J.; Joffe, S.; Botkin, J.R.; Rothwell, E.; Murray, T.H.; Anderson, R.; Deming, N.; Rosenthal, B.F.; Rivera, S.M. IRB practices and policies regarding the secondary research use of biospecimens Ethics in Biomedical Research. BMC Med. Ethics 2015, 16, 32. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, S.; Helgesson, G. Potential harms, anonymization, and the right to withdraw consent to biobank research. Eur. J. Hum. Genet. 2005, 13, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Penasa, S.; de Miguel Beriain, I.; Barbosa, C.; Białek, A.; Chortara, T.; Pereira, A.D.; Jiménez, P.N.; Sroka, T.; Tomasi, M. The EU general data protection regulation: How will it impact the regulation of research biobanks? Setting the legal frame in the Mediterranean and Eastern European area. Med. Law Int. 2018, 18, 241–255. [Google Scholar] [CrossRef]
- UK Biobank—UK Biobank, (n.d.). Available online: https://www.ukbiobank.ac.uk/ (accessed on 12 October 2023).
- Gazzetta Ufficiale della Repubblica Italiana, DECRETO LEGGE10 febbraio 2020, n. 10. Norme in materia di disposizione del proprio corpo e dei tessuti post mortem a fini di studio, di formazione e di ricerca scientifica. (n.d.). Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/04/20G00024/sg (accessed on 12 October 2023).
- Biobanca UPO|Struttura, Valori e Governance, (n.d.). Available online: https://biobank.uniupo.it/biobanca/ (accessed on 13 October 2023).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sguazzi, G.; Fasani, G.; Renò, F.; Gino, S. Biobanks: Archives or Resources? Their Secondary Use for Forensic Purposes—A Systematic Review. Forensic Sci. 2024, 4, 42-61. https://doi.org/10.3390/forensicsci4010004
Sguazzi G, Fasani G, Renò F, Gino S. Biobanks: Archives or Resources? Their Secondary Use for Forensic Purposes—A Systematic Review. Forensic Sciences. 2024; 4(1):42-61. https://doi.org/10.3390/forensicsci4010004
Chicago/Turabian StyleSguazzi, Giulia, Giulia Fasani, Filippo Renò, and Sarah Gino. 2024. "Biobanks: Archives or Resources? Their Secondary Use for Forensic Purposes—A Systematic Review" Forensic Sciences 4, no. 1: 42-61. https://doi.org/10.3390/forensicsci4010004