
Effectiveness of Passive Ultrasonic Irrigation Protocols in Simulated Complex Root Canal Cavities

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
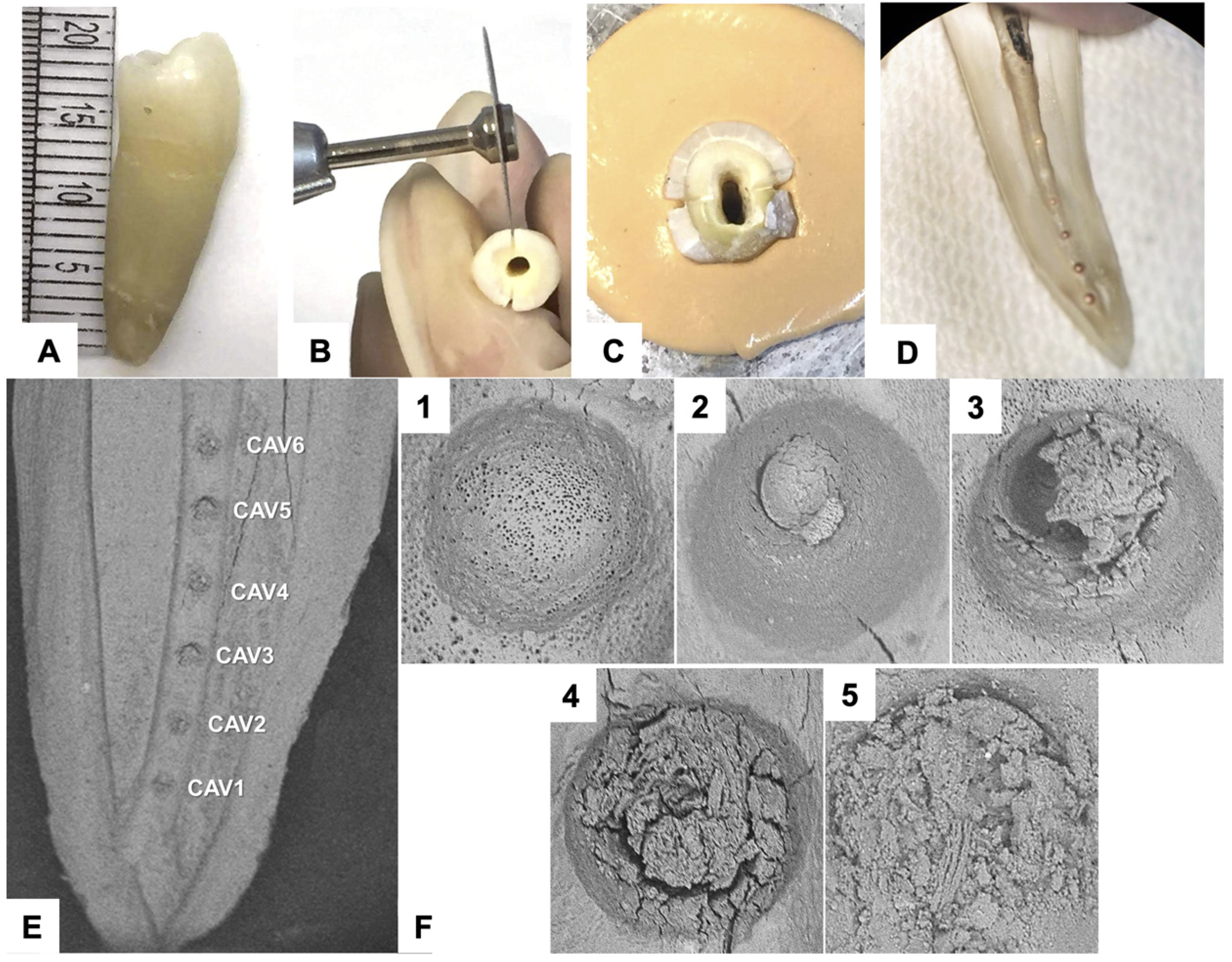
2.1. Specimens Selection and Preparation
2.2. Control and Experimental Group Design
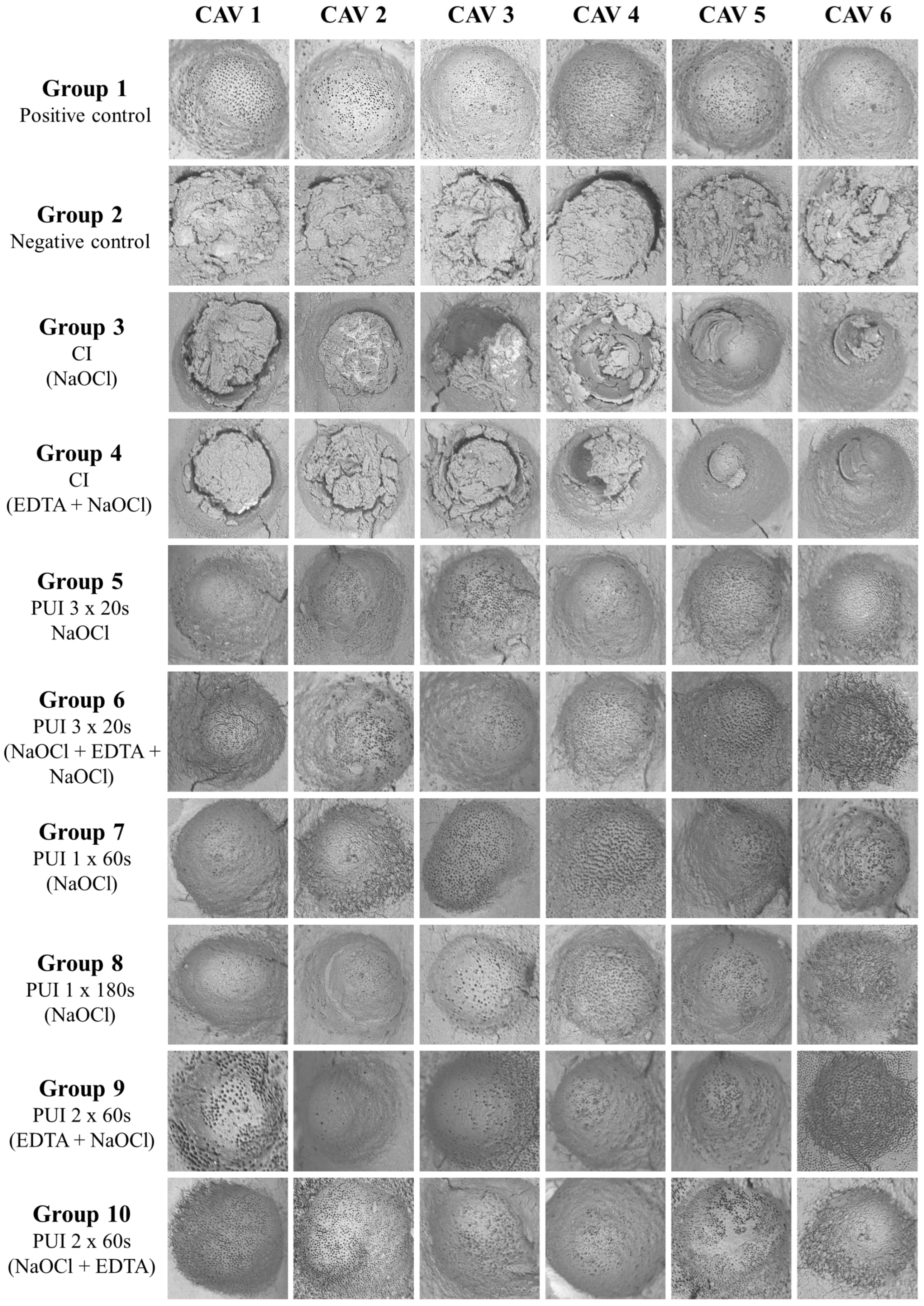
- Group 1—Positive control: Cavities were prepared as described above and kept debris-free. No irrigation protocol was carried out.
- Group 2—Negative control: The artificial cavities were filled with debris, and no irrigation protocol was performed.
- Group 3—CI with 15 mL of 2.5% NaOCl.
- Group 4—CI with 5 mL of NaOCl, 5 mL of 17% EDTA, and new 5 mL 2.5% NaOCl.
- Group 5—three cycles of PUI for 20 s using 2.5% NaOCl.
- Group 6—three cycles of PUI for 20 s using 2.5% NaOCl, 17% EDTA, and 2.5% NaOCl.
- Group 7—one PUI cycle for 60 s using 2.5% NaOCl.
- Group 8—one PUI cycle for 180 s using 2.5% NaOCl.
- Group 9—two PUI cycles for 60 s using 17% EDTA, and 2.5% NaOCl.
- Group 10—two PUI cycles for 60 s using 2.5% NaOCl, and 17% EDTA.
2.3. Statistical Analysis
3. Results
3.1. Protocols × Samples
3.2. Protocols × Cavities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Gregorio, C.; Estevez, R.; Cisneros, R.; Paranjpe, A.; Cohenca, N. Efficacy of different irrigation and activation systems on the penetration of sodium hypochlorite into simulated lateral canals and up to working length: An in vitro study. J. Endod. 2010, 36, 1216–1221. [Google Scholar] [CrossRef] [PubMed]
- Versiani, M.A.; De-Deus, G.; Vera, J.; Souza, E.; Steier, L.; Pécora, J.D.; Sousa-Neto, M.D. 3D mapping of the irrigated areas of the root canal space using micro-computed tomography. Clin. Oral Investig. 2015, 19, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.N. On the causes of persistent apical periodontitis: A review. Int. Endod. J. 2006, 39, 249–281. [Google Scholar] [CrossRef] [PubMed]
- Orlowski, N.B.; Schimdt, T.F.; Teixeira, C.D.S.; Garcia, L.; Savaris, J.M.; Tay, F.R.; Bortoluzzi, E.A. Smear Layer Removal Using Passive Ultrasonic Irrigation and Different Concentrations of Sodium Hypochlorite. J. Endod. 2020, 46, 1738–1744. [Google Scholar] [CrossRef]
- Agrawal, V.S.; Kapoor, S. An in vitro scanning electron microscopic study comparing the efficacy of passive ultrasonic and syringe irrigation methods using sodium hypochlorite in removal of debris from the root canal system. J. Ir. Dent. Assoc. 2012, 58, 156–161. [Google Scholar]
- Urban, K.; Donnermeyer, D.; Schäfer, E.; Bürklein, S. Canal cleanliness using different irrigation activation systems: A SEM evaluation. Clin. Oral Investig. 2017, 21, 2681–2687. [Google Scholar] [CrossRef]
- Castagna, F.; Rizzon, P.; da Rosa, R.A.; Santini, M.F.; Barreto, M.S.; Duarte, M.A.; Só, M.V. Effect of passive ultrassonic instrumentation as a final irrigation protocol on debris and smear layer removal--a SEM analysis. Microsc. Res. Tech. 2013, 76, 496–502. [Google Scholar] [CrossRef]
- Sahar-Helft, S.; Sarp, A.S.; Stabholtz, A.; Gutkin, V.; Redenski, I.; Steinberg, D. Comparison of positive-pressure, passive ultrasonic, and laser-activated irrigations on smear-layer removal from the root canal surface. Photomed. Laser Surg. 2015, 33, 129–135. [Google Scholar] [CrossRef]
- Jiang, L.M.; Verhaagen, B.; Versluis, M.; van der Sluis, L.W. Influence of the oscillation direction of an ultrasonic file on the cleaning efficacy of passive ultrasonic irrigation. J. Endod. 2010, 36, 1372–1376. [Google Scholar] [CrossRef]
- Leoni, G.B.; Versiani, M.A.; Silva-Sousa, Y.T.; Bruniera, J.F.; Pécora, J.D.; Sousa-Neto, M.D. Ex vivo evaluation of four final irrigation protocols on the removal of hard-tissue debris from the mesial root canal system of mandibular first molars. Int. Endod. J. 2017, 50, 398–406. [Google Scholar] [CrossRef]
- Lee, S.J.; Wu, M.K.; Wesselink, P.R. The effectiveness of syringe irrigation and ultrasonics to remove debris from simulated irregularities within prepared root canal walls. Int. Endod. J. 2004, 37, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Mancini, M.; Cerroni, L.; Iorio, L.; Armellin, E.; Conte, G.; Cianconi, L. Smear layer removal and canal cleanliness using different irrigation systems (EndoActivator, EndoVac, and passive ultrasonic irrigation): Field emission scanning electron microscopic evaluation in an in vitro study. J. Endod. 2013, 39, 1456–1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, R.B.; Marchesan, M.A.; Silva-Sousa, Y.T.; Sousa-Neto, M. Effectiveness of root canal debris removal using passive ultrasound irrigation with chlorhexidine digluconate or sodium hypochlorite individually or in combination as irrigants. J. Contemp. Dent. Pract. 2008, 9, 68–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalap, N.D.; Kokate, S.; Hegde, V. Ultrasonic versus sonic activation of the final irrigant in root canals instrumented with rotary/reciprocating files: An in-vitro scanning electron microscopy analysis. J. Conserv. Dent. 2016, 19, 368–372. [Google Scholar] [CrossRef] [PubMed]
- de Castro, F.P.; Pinheiro, S.L.; Duarte, M.A.; Duque, J.A.; Fernandes, S.L.; Anchieta, R.B.; da Silveira Bueno, C.E. Effect of time and ultrasonic activation on ethylenediaminetetraacetic acid on smear layer removal of the root canal. Microsc. Res. Tech. 2016, 79, 1062–1068. [Google Scholar] [CrossRef]
- Koçak, S.; Bağcı, N.; Çiçek, E.; Türker, S.A.; Can Sağlam, B.; Koçak, M.M. Influence of passive ultrasonic irrigation on the efficiency of various irrigation solutions in removing smear layer: A scanning electron microscope study. Microsc. Res. Tech. 2017, 80, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Martins Justo, A.; Abreu da Rosa, R.; Santini, M.F.; Cardoso Ferreira, M.B.; Pereira, J.R.; Hungaro Duarte, M.A.; Reis So, M.V. Effectiveness of final irrigant protocols for debris removal from simulated canal irregularities. J. Endod. 2014, 40, 2009–2014. [Google Scholar] [CrossRef]
- Andrabi, S.M.; Kumar, A.; Zia, A.; Iftekhar, H.; Alam, S.; Siddiqui, S. Effect of passive ultrasonic irrigation and manual dynamic irrigation on smear layer removal from root canals in a closed apex in vitro model. J. Investig. Clin. Dent. 2014, 5, 188–193. [Google Scholar] [CrossRef]
- Schneider, S.W. A comparison of canal preparations in straight and curved root canals. Oral Surg. Oral Med. Oral Pathol. 1971, 32, 271–275. [Google Scholar] [CrossRef]
- Kato, A.S.; Cunha, R.S.; da Silveira Bueno, C.E.; Pelegrine, R.A.; Fontana, C.E.; de Martin, A.S. Investigation of the Efficacy of Passive Ultrasonic Irrigation Versus Irrigation with Reciprocating Activation: An Environmental Scanning Electron Microscopic Study. J. Endod. 2016, 42, 659–663. [Google Scholar] [CrossRef]
- Rodig, T.; Bozkurt, M.; Konietschke, F.; Hulsmann, M. Comparison of the Vibringe system with syringe and passive ultrasonic irrigation in removing debris from simulated root canal irregularities. J. Endod. 2010, 36, 1410–1413. [Google Scholar] [CrossRef] [PubMed]
- Haapasalo, M.; Shen, Y.; Qian, W.; Gao, Y. Irrigation in endodontics. Dent. Clin. N. Am. 2010, 54, 291–312. [Google Scholar] [CrossRef] [PubMed]
- Boutsioukis, C.; Arias-Moliz, M.T.; Chávez de Paz, L.E. A critical analysis of research methods and experimental models to study irrigants and irrigation systems. Int. Endod. J. 2022, 55 (Suppl. S2), 295–329. [Google Scholar] [CrossRef] [PubMed]
- Rossi-Fedele, G.; Rödig, T. Effectiveness of root canal irrigation and dressing for the treatment of apical periodontitis: A systematic review and meta-analysis of clinical trials. Int. Endod. J. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Souza, C.C.; Bueno, C.E.; Kato, A.S.; Limoeiro, A.G.; Fontana, C.E.; Pelegrine, R.A. Efficacy of passive ultrasonic irrigation, continuous ultrasonic irrigation versus irrigation with reciprocating activation device in penetration into main and simulated lateral canals. J. Conserv. Dent. 2019, 22, 155–159. [Google Scholar] [CrossRef]
- Barbosa, A.F.A.; Lima, C.O.; Sassone, L.M.; Fares, R.D.; Fidalgo, T.; Silva, E. Effect of passive ultrasonic irrigation on hard tissue debris removal: A systematic review and meta-analysis. Braz. Oral. Res. 2021, 35, e123. [Google Scholar] [CrossRef]
- Kluge, M.; Trüschler, J.; Elamin, F.; Anderson, A.; Hellwig, E.; Altenburger, M.; Vach, K.; Wittmer, A.; Al-Ahmad, A. Improving the microbial sampling and analysis of secondary infected root canals by passive ultrasonic irrigation. Clin. Oral Investig. 2022, 26, 4575–4586. [Google Scholar] [CrossRef]
- Li, Q.; Zhang, Q.; Zou, X.; Yue, L. Evaluation of four final irrigation protocols for cleaning root canal walls. Int. J. Oral. Sci. 2020, 12, 29. [Google Scholar] [CrossRef]
- Ali, A.; Bhosale, A.; Pawar, S.; Kakti, A.; Bichpuriya, A.; Agwan, M.A. Current Trends in Root Canal Irrigation. Cureus 2022, 14, e24833. [Google Scholar] [CrossRef]
- Boutsioukis, C.; Arias-Moliz, M.T. Present status and future directions-irrigants and irrigation methods. Int. Endod. J. 2022, 55 (Suppl. S3), 588–612. [Google Scholar] [CrossRef]
- Cheung, A.W.T.; Lee, A.H.C.; Cheung, G.S.P. Clinical efficacy of activated irrigation in endodontics: A focused review. Restor. Dent. Endod. 2021, 46, e10. [Google Scholar] [CrossRef] [PubMed]
- Çapar, İ.D.; Aydinbelge, H.A. Effectiveness of various irrigation activation protocols and the self-adjusting file system on smear layer and debris removal. Scanning 2014, 36, 640–647. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Groups | Cleaning (Debris Removal) | Lower 95% CI of Mean | Upper 95% CI of Mean | Cleaning (Tubules Exposure) | Lower 95% CI of Mean | Upper 95% CI of Mean |
|---|---|---|---|---|---|---|
| 1- Positive Control | 1b | 0.97 | 1.12 | 1bc | 1 | 1.13 |
| 2- Negative Control | 4c | 4 | 4 | 2a | 2 | 2 |
| 3- CI NaOCl + NaOCl + NaOCl | 2a | 1.90 | 2.43 | 2a | 2 | 2 |
| 4- CI NaOCl + EDTA + NaOCl | 3a | 2.13 | 2.67 | 2a | 1.95 | 2 |
| 5- PUI 3 × 20 s NaOCl | 1b | 1.02 | 1.17 | 1b | 1.22 | 1.47 |
| 6- PUI 3 × 20 s NaOCl + EDTA + NaOCl | 1b | 0.97 | 1.12 | 1c | 0.99 | 1.10 |
| 7- PUI 1 × 60 s NaOCl | 1b | 0.96 | 1.10 | 1c | 0.98 | 1.05 |
| 8- PUI 1 × 180 s NaOCl | 1b | 0.98 | 1.08 | 1bc | 1.15 | 1.38 |
| 9- PUI 2 × 60 s EDTA + NaOCl | 1b | 0.98 | 1.08 | 1bc | 1.01 | 1.15 |
| 10- PUI two cycles 60 s NaOCl + EDTA | 1b | 0.98 | 1.05 | 1c | 0.99 | 1.10 |
| Groups | CAV1 | CAV2 | CAV3 | CAV4 | CAV5 | CAV6 |
|---|---|---|---|---|---|---|
| 1- Positive Control | 1Ab | 1Aa | 1Ab | 1Aa | 1Aa | 1Aa |
| 2- Negative Control | 4Ac | 4Ab | 4Aa | 4Ab | 4Ac | 4Ab |
| 3- IC NaOCl + NaOCl + NaOCl | 3Aac | 2.5Ababc | 2ABa | 2ABab | 1.5Bab | 1Ba |
| 4- IC NaOCl + EDTA + NaOCl | 3Aac | 3ABbc | 3ABa | 1Ba | 2Bbc | 1.5Ba |
| 5- PUI 3 × 20 s NaOCl | 1Aab | 1Aac | 1Ab | 1Aa | 1Aa | 1Aa |
| 6- PUI 3 × 20 s NaOCl + EDTA + NaOCl | 1Ab | 1Aa | 1Ab | 1Aa | 1Aa | 1Aa |
| 7- PUI 1 × 60 s NaOCl | 1Ab | 1Aa | 1Ab | 1Aa | 1Aab | 1Aa |
| 8- PUI 1 × 180 s NaOCl | 1Ab | 1Aa | 1Ab | 1Aa | 1Aa | 1Aa |
| 9- PUI 2 × 60 s EDTA + NaOCl | 1Ab | 1Aa | 1Ab | 1Aa | 1Aa | 1Aa |
| 10- PUI two cycles 60 s NaOCl + EDTA | 1Ab | 1Aa | 1Ab | 1Aa | 1Aa | 1Aa |
| Groups | CAV1 | CAV2 | CAV3 | CAV4 | CAV5 | CAV6 |
|---|---|---|---|---|---|---|
| 1- Positive Control | 1b | 1b | 1b | 1b | 1b | 1b |
| 2- Negative Control | 2a | 2a | 2a | 2a | 2a | 2a |
| 3- IC NaOCl + NaOCl + NaOCl | 2a | 2a | 2a | 2a | 2a | 2a |
| 4- IC NaOCl + EDTA + NaOCl | 2a | 2a | 2a | 2a | 2a | 2a |
| 5- PUI 3 × 20 s NaOCl | 1.5ab | 1ab | 1ab | 1ab | 1ab | 1ab |
| 6- PUI 3 × 20 s NaOCl + EDTA + NaOCl | 1b | 1b | 1b | 1b | 1b | 1b |
| 7- PUI 1 × 60 s NaOCl | 1b | 1b | 1b | 1b | 1b | 1b |
| 8- PUI 1 × 180 s NaOCl | 1ab | 1ab | 1b | 1ab | 1ab | 1b |
| 9- PUI 2 × 60 s EDTA + NaOCl | 1b | 1b | 1b | 1b | 1b | 1b |
| 10- PUI two cycles 60 s NaOCl + EDTA | 1b | 1b | 1b | 1b | 1b | 1b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plazza, F.A.; Dal-Fabbro, R.; Cosme-Silva, L.; Duarte, P.C.T.; Loureiro, C.; Custódio, V.Z.; Cintra, L.T.A.; Duarte, M.A.H.; Gomes-Filho, J.E. Effectiveness of Passive Ultrasonic Irrigation Protocols in Simulated Complex Root Canal Cavities. Oral 2023, 3, 1-10. https://doi.org/10.3390/oral3010001
Plazza FA, Dal-Fabbro R, Cosme-Silva L, Duarte PCT, Loureiro C, Custódio VZ, Cintra LTA, Duarte MAH, Gomes-Filho JE. Effectiveness of Passive Ultrasonic Irrigation Protocols in Simulated Complex Root Canal Cavities. Oral. 2023; 3(1):1-10. https://doi.org/10.3390/oral3010001
Chicago/Turabian StylePlazza, Flávia A., Renan Dal-Fabbro, Leopoldo Cosme-Silva, Paulo C. T. Duarte, Caroline Loureiro, Vitória Z. Custódio, Luciano T. A. Cintra, Marco A. H. Duarte, and João Eduardo Gomes-Filho. 2023. "Effectiveness of Passive Ultrasonic Irrigation Protocols in Simulated Complex Root Canal Cavities" Oral 3, no. 1: 1-10. https://doi.org/10.3390/oral3010001