
Dermal Melanocytic Disorders

 , , and
, , and
Abstract
:1. Introduction
2. Cases
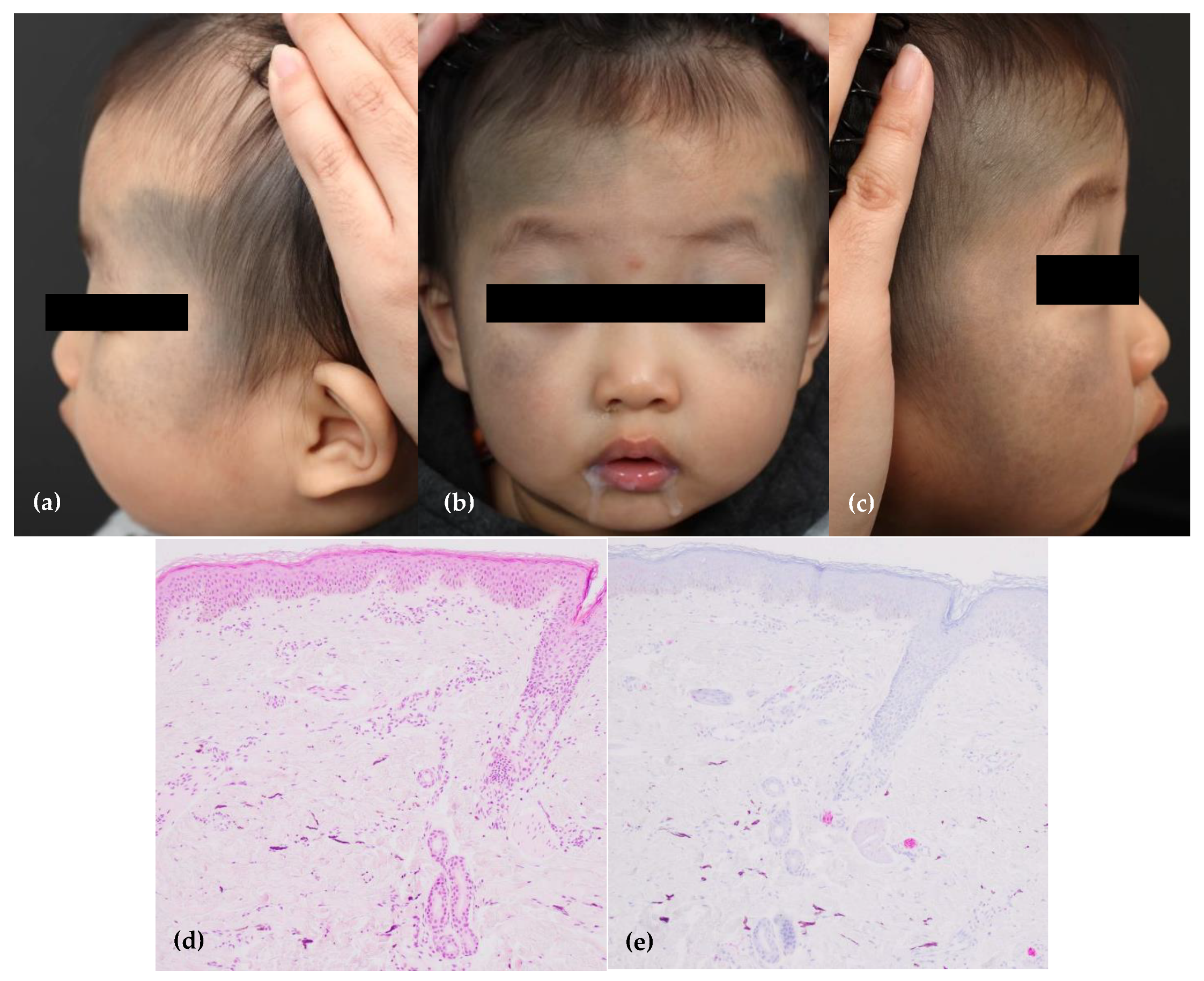
2.1. Case 1: Bilateral Nevus of Ota or Aberrant Mongolian Spot
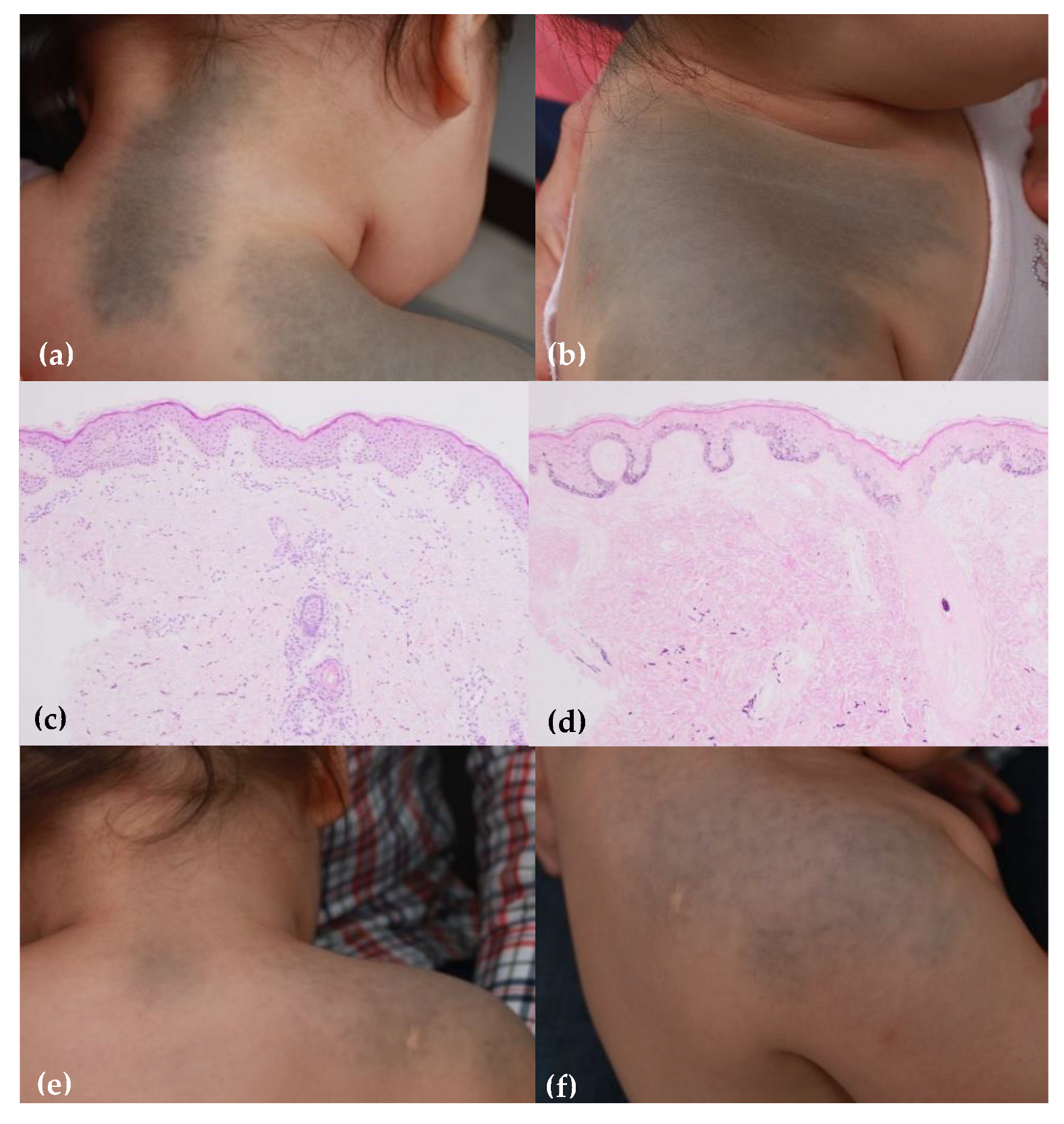
2.2. Case 2: Nevus of Ito or Aberrant Mongolian Spot
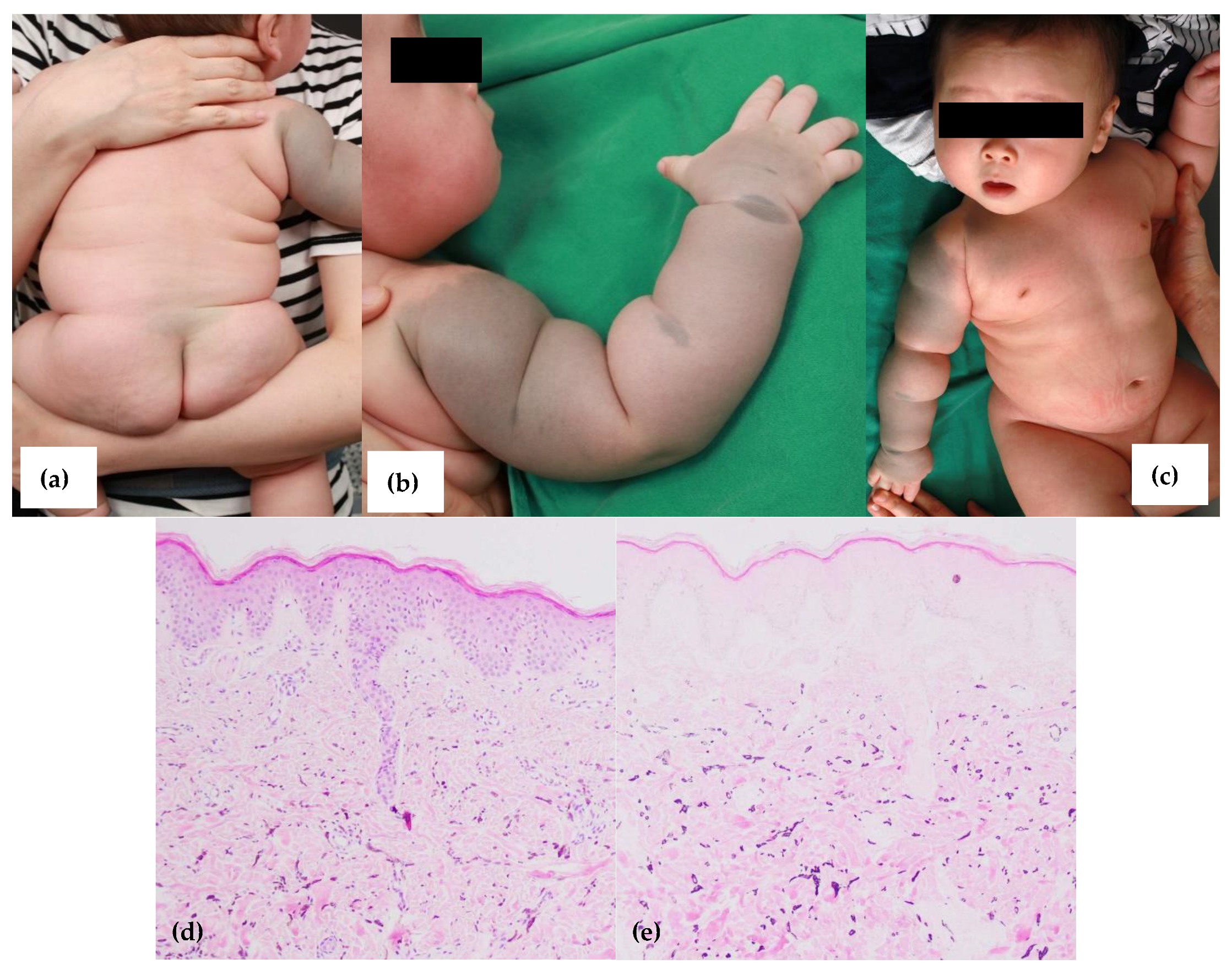
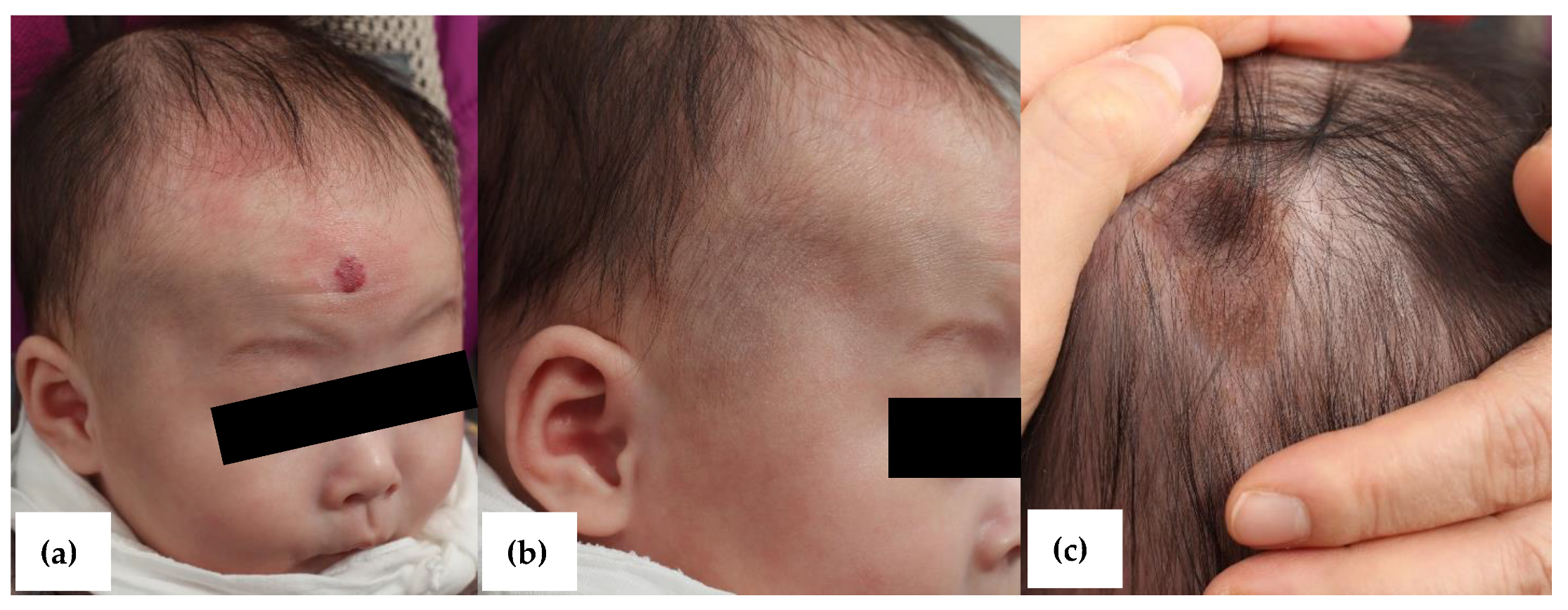
2.3. Case 3: Aberrant Mongolian Spot or Nevus of Ota with Co-Existing Congenital Melanocytic Nevus and Hemangioma
2.4. Case 4: Nevus of Ito or Aberrant Mongolian Spot
3. Discussion
3.1. Mongolian Spot and Aberrant Mongolian Spot
3.2. Nevus of Ota
3.3. Nevus of Ito
3.4. Discussion on Our Cases
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gupta, D.; Thappa, D.M. Mongolian Spots-A Prospective Study. Pediatric Dermatol. 2013, 30, 683–688. [Google Scholar] [CrossRef]
- Agarwal, P.; Patel, B.C. Nevus of Ota and Ito. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Cordova, A. The Mongolian spot: A study of ethnic differences and a literature review. Clin. Pediatrics 1981, 20, 714–719. [Google Scholar] [CrossRef]
- Kikuchi, I. What is a Mongolian spot? Int. J. Dermatol. 1982, 21, 131–133. [Google Scholar] [CrossRef] [PubMed]
- Egemen, A.; Ikizoğlu, T.; Ergör, S.; Asar, G.M.; Yilmaz, O. Frequency and characteristics of mongolian spots among Turkish children in Aegean region. Turk. J. Pediatrics 2006, 48, 232–236. [Google Scholar]
- Reza, A.M.; Farahnaz, G.Z.; Hamideh, S.; SeyedAlinaghi, S.; Saeed, Z.; Mostafa, H. Incidence of Mongolian Spots and its Common Sites at Two University Hospitals in Tehran, Iran. Pediatric Dermatol. 2010, 27, 397–398. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.K.C. Mongolian Spots in Chinese Children. Int. J. Dermatol. 1988, 27, 106–108. [Google Scholar] [CrossRef] [PubMed]
- Happle, R. Phacomatosis Pigmentovascularis Revisited and Reclassified. Arch. Dermatol. 2005, 141, 385–388. [Google Scholar] [CrossRef]
- Ochiai, T.; Suzuki, Y.; Kato, T.; Shichino, H.; Chin, M.; Mugishima, H.; Orii, T. Natural history of extensive Mongolian spots in mucopolysaccharidosis type II (Hunter syndrome): A survey among 52 Japanese patients. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 1082–1085. [Google Scholar] [CrossRef]
- Su, F.; Li, F.; Jin, H.-Z. Extensive Mongolian spots in a child with mucolipidosis II. Int. J. Dermatol. 2010, 49, 438–440. [Google Scholar] [CrossRef]
- Kagami, S.; Asahina, A.; Watanabe, R.; Mimura, Y.; Shirai, A.; Hattori, N.; Watanabe, T.; Tamaki, K. Laser treatment of 26 Japanese patients with Mongolian spots. Dermatol. Surg. 2008, 34, 1689–1694. [Google Scholar]
- Shirakawa, M.; Ozawa, T.; Ohasi, N.; Ishii, M.; Harada, T. Comparison of regional efficacy and complications in the treatment of aberrant Mongolian spots with the Q-switched ruby laser. J. Cosmet. Laser Ther. 2010, 12, 138–142. [Google Scholar] [CrossRef]
- Ota, M. Naevus fusco-caeruleus ophthalmo-maxillaris. Jpn. J. Dermatol. 1939, 46, 360. [Google Scholar]
- Ho, S.G.; Chan, H.H. The Asian dermatologic patient: Review of common pigmentary disorders and cutaneous diseases. Am. J. Clin. Dermatol. 2009, 10, 153–168. [Google Scholar] [CrossRef] [PubMed]
- Van Raamsdonk, C.D.; Bezrookove, V.; Green, G.; Bauer, J.; Gaugler, L.; O’Brien, J.M.; Simpson, E.M.; Barsh, G.S.; Bastian, B.C. Frequent somatic mutations of GNAQ in uveal melanoma and blue naevi. Nature 2009, 457, 599–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konstantinov, N.K.; Berry, T.M.; Elwood, H.R.; Zlotoff, B.J. Nevus of Ota associated with a primary uveal melanoma and intracranial melanoma metastasis. Cutis 2018, 102, E2–E4. [Google Scholar] [PubMed]
- Polder, K.D.; Landau, J.M.; Vergilis-Kalner, I.J.; Goldberg, L.H.; Friedman, P.M.; Bruce, S. Laser Eradication of Pigmented Lesions: A Review. Dermatol. Surg. 2011, 37, 572–595. [Google Scholar] [CrossRef]
- Sami, L.; Changzheng, H.; Yan, L. Factors affecting response, number of laser sessions and complications in nevus of Ota treated by Q-switched alexandrite laser: A retrospective study. G Ital. Dermatol. Venereol. 2015, 151, 160–168. [Google Scholar]
- Dekio, S.; Koike, S.; Jidoi, J. Nevus of ota with nevus of Ito—Report of a case with cataract. J. Dermatol. 1989, 16, 164–166. [Google Scholar] [CrossRef]
- Kumar, M.A. Nevus Ota associated with nevus of Ito. Indian J. Dermatol. Venereol. Leprol. 2004, 70, 112–113. [Google Scholar]
- Tse, J.Y.; Walls, B.E.; Pomerantz, H.; Yoon, C.H.; Buchbinder, E.I.; Werchniak, A.E.; Dong, F.; Lian, C.G.; Granter, S.R. Melanoma arising in a nevus of Ito: Novel genetic mutations and a review of the literature on cutaneous malignant transformation of dermal melanocytosis. J. Cutan. Pathol. 2015, 43, 57–63. [Google Scholar] [CrossRef]
- Yeh, I.; Mully, T.W.; Wiesner, T.; Vemula, S.S.; Mirza, S.A.; Sparatta, A.J.; McCalmont, T.H.; Bastian, B.; LeBoit, P.E. Ambiguous Melanocytic Tumors with Loss of 3p21. Am. J. Surg. Pathol. 2014, 38, 1088–1095. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.W.; Wang, J.B.; Liu, Y.H.; Zuo, Y.G.; Jin, H.Z.; Jiang, G.T.; Li, H.C.; Ma, D.L. Clinical efficacy of Q-switched Alexandrite laser for pigmentary skin diseases in 4656 patients. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 2006, 28, 202–205. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Mongolian Spot | Aberrant Mongolian Spot | Nevus of Ota | Nevus of Ito |
|---|---|---|---|---|
| Site of involvement | Sacrococcygeal area | Extrasacral area including face, extremities and trunk | Face and orbits in a unilateral trigeminal nerve distribution | Neck, supraclavicular and scapular area |
| Sclera involvement | - | Rare | In two-thirds | - |
| Onset | Congenital | Congenital | Congenital, early childhood or puberty | Congenital, early childhood or puberty |
| Epidemiology | Asian, African, and Hispanic population | Asian, African, and Hispanic population | Asian female | Asian female |
| Pathology | Diffusely spread spindle-shaped melanocytes in the lower dermis | Diffusely spread spindle-shaped melanocytes in the lower dermis | Evenly spread spindle-shaped melanocytes throughout the entire dermis | Evenly spread spindle-shaped melanocytes throughout the entire dermis |
| Melanocyte density | Sparsely found in the deeper dermis | Sparsely found in the deeper dermis | Increased in the epidermis; Scattered in the upper and mid dermis | Increased in the epidermis; Scattered in the upper and mid dermis |
| Course | Mostly regress during childhood | Often regress during childhood but may persist into adulthood | Persistent | Persistent |
| Malignant transformation | None | None | Rare | Rare |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, Y.; Lee, S.-H.; Cho, M.; Cho, S.-H.; Lee, J.-D.; Woo, Y.-R.; Kim, H.-S. Dermal Melanocytic Disorders. Dermato 2021, 1, 35-42. https://doi.org/10.3390/dermato1020006
Han Y, Lee S-H, Cho M, Cho S-H, Lee J-D, Woo Y-R, Kim H-S. Dermal Melanocytic Disorders. Dermato. 2021; 1(2):35-42. https://doi.org/10.3390/dermato1020006
Chicago/Turabian StyleHan, Yujin, Se-Hoon Lee, Minah Cho, Sang-Hyun Cho, Jeong-Deuk Lee, Yu-Ri Woo, and Hei-Sung Kim. 2021. "Dermal Melanocytic Disorders" Dermato 1, no. 2: 35-42. https://doi.org/10.3390/dermato1020006